
Redesigning Recruitment and Engagement Strategies for Virtual Culinary Medicine and Medical Nutrition Interventions in a Randomized Trial of Patients with Uncontrolled Type 2 Diabetes
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design
2.3. Study Eligibility
2.4. Recruitment Strategy
2.5. Participant Enrollment and Food Assistance
2.6. Development of Medical Nutrition Therapy Arm (MNT)
2.7. Development of Electronic Culinary Medicine Arm (eCM)
2.8. Initial Study Launch Review
3. Results
3.1. Study Recruitment and Enrollment Redesign
3.2. eCM Engagement and Redesign
3.3. Trial Recruitment Results
3.4. Randomization and Baseline Characteristics
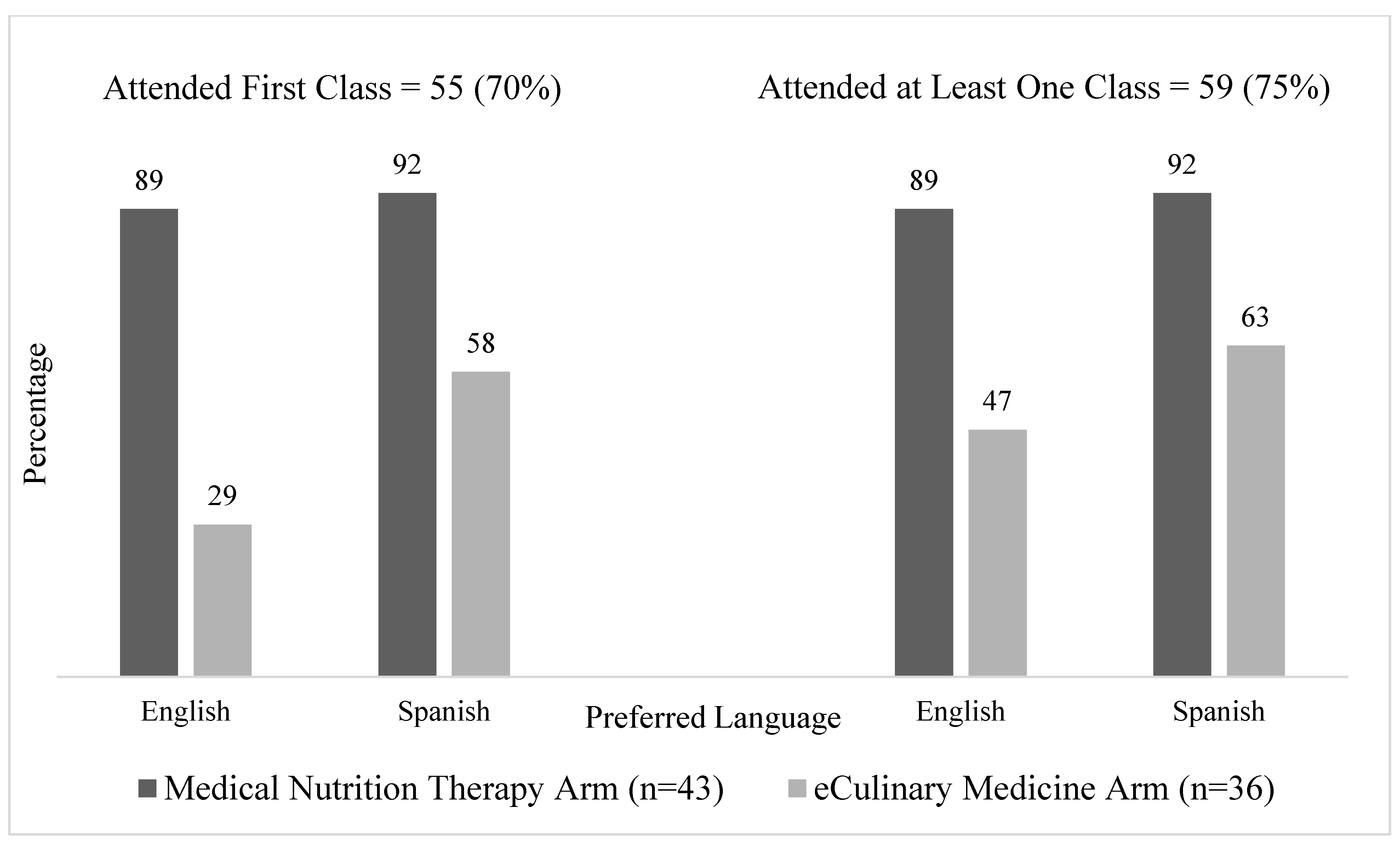
3.5. Participant Engagement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kolb, L. An Effective Model of Diabetes Care and Education: The ADCES7 Self-Care Behaviors™. Sci. Diabetes Self-Manag. Care 2021, 47, 30–53. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [PubMed]
- Medicine, I. The Role of Nutrition in Maintaining Health in the Nation’s Elderly: Evaluating Coverage of Nutrition Services for the Medicare Population; The National Academies Press: Washington, DC, USA, 2000; p. 382. [Google Scholar]
- Agee, M.D.; Gates, Z.; Irwin, P.M., Jr. Effect of Medical Nutrition Therapy for Patients With Type 2 Diabetes in a Low-/No-Cost Clinic: A Propensity Score-Matched Cohort Study. Diabetes Spectr. 2018, 31, 83–89. [Google Scholar] [CrossRef]
- Razaz, J.M.; Rahmani, J.; Varkaneh, H.K.; Thompson, J.; Clark, C.; Abdulazeem, H.M. The health effects of medical nutrition therapy by dietitians in patients with diabetes: A systematic review and meta-analysis: Nutrition therapy and diabetes. Prim. Care Diabetes 2019, 13, 399–408. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S60–S82. [Google Scholar] [CrossRef] [PubMed]
- Briggs Early, K.; Stanley, K. Position of the Academy of Nutrition and Dietetics: The Role of Medical Nutrition Therapy and Registered Dietitian Nutritionists in the Prevention and Treatment of Prediabetes and Type 2 Diabetes. J. Acad. Nutr. Diet. 2018, 118, 343–353. [Google Scholar] [CrossRef]
- DiSantis, K.I.; Grier, S.A.; Odoms-Young, A.; Baskin, M.L.; Carter-Edwards, L.; Young, D.R.; Lassiter, V.; Kumanyika, S.K. What "price" means when buying food: Insights from a multisite qualitative study with Black Americans. Am. J. Public Health 2013, 103, 516–522. [Google Scholar] [CrossRef]
- Marcy, T.R.; Britton, M.L.; Harrison, D. Identification of barriers to appropriate dietary behavior in low-income patients with type 2 diabetes mellitus. Diabetes Ther. 2011, 2, 9–19. [Google Scholar] [CrossRef]
- Farmer, N.; Touchton-Leonard, K.; Ross, A. Psychosocial Benefits of Cooking Interventions: A Systematic Review. Health Educ. Behav. 2018, 45, 167–180. [Google Scholar] [CrossRef]
- Lillquist, S.; Ruiz Barnecett, G.; Flexman, N.; Mikati, N. Recipes for Health: A Community-Based Nutrition and Culinary Intervention. Cureus 2022, 14, e32322. [Google Scholar] [CrossRef]
- Rees, J.; Fu, S.C.; Lo, J.; Sambell, R.; Lewis, J.R.; Christophersen, C.T.; Byrne, M.F.; Newton, R.U.; Boyle, S.; Devine, A. How a 7-Week Food Literacy Cooking Program Affects Cooking Confidence and Mental Health: Findings of a Quasi-Experimental Controlled Intervention Trial. Front. Nutr. 2022, 9, 802940. [Google Scholar] [CrossRef] [PubMed]
- Pooler, J.A.; Morgan, R.E.; Wong, K.; Wilkin, M.K.; Blitstein, J.L. Cooking Matters for Adults Improves Food Resource Management Skills and Self-confidence Among Low-Income Participants. J. Nutr. Educ. Behav. 2017, 49, 545–553.e541. [Google Scholar] [CrossRef] [PubMed]
- Wetherill, M.S.; Davis, G.C.; Kezbers, K.; Carter, V.; Wells, E.; Williams, M.B.; Ijams, S.D.; Monlezun, D.; Harlan, T.; Whelan, L.J. Development and Evaluation of a Nutrition-Centered Lifestyle Medicine Curriculum for Physician Assistant Students. Med. Sci. Educ. 2019, 29, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Bernardo, G.L.; Jomori, M.M.; Fernandes, A.C.; Colussi, C.F.; Condrasky, M.D.; Proença, R. Nutrition and Culinary in the Kitchen Program: A randomized controlled intervention to promote cooking skills and healthy eating in university students-study protocol. Nutr. J. 2017, 16, 83. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.; Yan, J.; Messiah, S.E.; Albin, J. Culinary Medicine as Innovative Nutrition Education for Medical Students: A Scoping Review. Acad. Med. 2023, 98, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Atamanchuk, L.; Rao, T.; Sato, K.; Crowley, J.; Ball, L. Exploring culinary medicine as a promising method of nutritional education in medical school: A scoping review. BMC Med. Educ. 2022, 22, 441. [Google Scholar] [CrossRef]
- Razavi, A.C.; Sapin, A.; Monlezun, D.J.; McCormack, I.G.; Latoff, A.; Pedroza, K.; McCullough, C.; Sarris, L.; Schlag, E.; Dyer, A.; et al. Effect of culinary education curriculum on Mediterranean diet adherence and food cost savings in families: A randomised controlled trial. Public Health Nutr. 2021, 24, 2297–2303. [Google Scholar] [CrossRef]
- Metcalfe, J.J.; Prescott, M.P.; Schumacher, M.; Kownacki, C.; McCaffrey, J. Community-based culinary and nutrition education intervention promotes fruit and vegetable consumption. Public Health Nutr. 2022, 25, 437–449. [Google Scholar] [CrossRef]
- Flint, K.L.; Davis, G.M.; Umpierrez, G.E. Emerging trends and the clinical impact of food insecurity in patients with diabetes. J. Diabetes 2020, 12, 187–196. [Google Scholar] [CrossRef]
- Sharma, S.V.; McWhorter, J.W.; Chow, J.; Danho, M.P.; Weston, S.R.; Chavez, F.; Moore, L.S.; Almohamad, M.; Gonzalez, J.; Liew, E.; et al. Impact of a Virtual Culinary Medicine Curriculum on Biometric Outcomes, Dietary Habits, and Related Psychosocial Factors among Patients with Diabetes Participating in a Food Prescription Program. Nutrients 2021, 13, 4492. [Google Scholar] [CrossRef]
- Silver, J.K.; Finkelstein, A.; Minezaki, K.; Parks, K.; Budd, M.A.; Tello, M.; Paganoni, S.; Tirosh, A.; Polak, R. The Impact of a Culinary Coaching Telemedicine Program on Home Cooking and Emotional Well-Being during the COVID-19 Pandemic. Nutrients 2021, 13, 2311. [Google Scholar] [CrossRef] [PubMed]
- Denton, J. Health meets Food™ Remotely As Culinary Medicine Course Moves Online. Available online: https://news.uthsc.edu/health-meets-food-remotely-as-culinary-medicine-course-moves-online/ (accessed on 3 June 2020).
- Economic Research Service (ERS). Food Access Research Atlas. Available online: https://www.ers.usda.gov/data-products/food-access-research-atlas/ (accessed on 25 August 2023).
- Centers for Disease Control and Prevention (CDC), PLACES. Available online: https://www.cdc.gov/places (accessed on 10 August 2023).
- Pickens, S.; Boumbulian, P.; Anderson, R.J.; Ross, S.; Phillips, S. Community-Oriented Primary Care in Action: A Dallas Story. Am. J. Public Health 2002, 92, 1728–1732. [Google Scholar] [CrossRef] [PubMed]
- Zoom Video Communications, Inc. Zoom Cloud Meetings, Version 5.13.11 (13424); Zoom Video Communications, Inc.: San Jose, CA, USA.
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)–A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. REDCap Consortium. The REDCap consortium: Building an international community of software partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Dave, J.M.; Thompson, D.I.; Svendsen-Sanchez, A.; Cullen, K.W. Perspectives on Barriers to Eating Healthy Among Food Pantry Clients. Health Equity 2017, 1, 28–34. [Google Scholar] [CrossRef]
- National Center for Health Statistics (NCHS), National Health and Nutrition Examination Survey Data 2021–2022. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/questionnaires.aspx?BeginYear=2021 (accessed on 10 August 2023).
- Blumberg, S.J.; Bialostosky, K.; Hamilton, W.L.; Briefel, R.R. The Effectiveness of a Short Form of the Household Food Security Scale. Am. J. Public Health 1999, 89, 1231–1234. [Google Scholar] [CrossRef]
- Board, C.M.S. Health Meets Food. Available online: https://culinarymedicine.org/ (accessed on 25 August 2023).
- Vindrola-Padros, C.; Johnson, G.A. Rapid Techniques in Qualitative Research: A Critical Review of the Literature. Qual. Health Res. 2020, 30, 1596–1604. [Google Scholar] [CrossRef]
- Yen, P.H.; Leasure, A.R. Use and Effectiveness of the Teach-Back Method in Patient Education and Health Outcomes. Fed. Pract. 2019, 36, 284–289. [Google Scholar]
- Thorpe, K.E.; Zwarenstein, M.; Oxman, A.D.; Treweek, S.; Furberg, C.D.; Altman, D.G.; Tunis, S.; Bergel, E.; Harvey, I.; Magid, D.J.; et al. A pragmatic-explanatory continuum indicator summary (PRECIS): A tool to help trial designers. J. Clin. Epidemiol. 2009, 62, 464–475. [Google Scholar] [CrossRef]
- Edge, I.; Greenberg, I.; Reilly, J.M.; Silva, W. Virtual, bilingual English-Spanish community nutrition and exercise classes: Barriers and opportunities. Health Educ. J. 2022, 81, 705–717. [Google Scholar] [CrossRef]
- T. Thomas, K.; Friedman, S.A.; J. Larson, M.; C. Jorgensen, T.; Sharma, S.; Smith, A.; S. Lavi, M. A cohort-based nutrition ECHO for community health workers. Health Educ. Res. 2023, 38, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Marshall, H.; Albin, J. Food as Medicine: A Pilot Nutrition and Cooking Curriculum for Children of Participants in a Community-Based Culinary Medicine Class. Matern. Child Health J. 2021, 25, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Nagy, A.; McMahon, A.; Tapsell, L.; Deane, F. The therapeutic relationship between a client and dietitian: A systematic integrative review of empirical literature. Nutr. Diet. 2022, 79, 303–348. [Google Scholar] [CrossRef] [PubMed]
- Endevelt, R.; Gesser-Edelsburg, A. A qualitative study of adherence to nutritional treatment: Perspectives of patients and dietitians. Patient Prefer. Adherence 2014, 2014, 147–154. [Google Scholar] [CrossRef]
- Saxe-Custack, A.; Egan, S. Flint Families Cook: A Virtual Cooking and Nutrition Program for Families. J. Nutr. Educ. Behav. 2022, 54, 359–363. [Google Scholar] [CrossRef]
- Herbert, J.; Flego, A.; Gibbs, L.; Waters, E.; Swinburn, B.; Reynolds, J.; Moodie, M. Wider impacts of a 10-week community cooking skills program--Jamie’s Ministry of Food, Australia. BMC Public Health 2014, 14, 1161. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Concept | eCulinary Medicine | Medical Nutrition Therapy |
|---|---|---|
| Facilitator Background | Lead Bilingual RDcm (Contractor), Assistant Bilingual facilitator with CM-specific training or RDcm | English-speaking RD Parkland provider, Spanish-speaking RD Parkland provider |
| Educational Approach | Experiential learning in a small, virtual group setting focused on practical meal planning and preparation, culinary skills building, and food presentation and discussion. Participants were given binders with recipes and handouts, and both a practical, “hands-on” cooking experience and a didactic lesson from the facilitator reinforced themes of a nourishing dietary pattern for health promotion. | Traditional diabetes education model tailored for patients with known diabetes. The session content generally followed a predetermined outline of six sessions but was adjusted for individual patient needs based on ADA standards of care nutrition consensus statements for diabetes and prediabetes. |
| Frequency | Sessions were held on a fixed monthly schedule on Tuesday evenings, with English one week and Spanish the following week. | Sessions were held monthly and scheduled during designated appointment slots based on RD’s schedule during their working hours. |
| Scheduling | Participants were given a class schedule at the beginning of the intervention and reminder messages prior to each class. All contact and attendance documentation occurred outside of the health record and their established healthcare practice. | Participants were scheduled per clinic workflow and by appointment. RD called the participants to schedule an appointment. If the participant “no-showed”, RDs reschedule. All contact and attendance documentation occurred in the electronic health record. |
| Setting/Timing | All participants simultaneously joined the 2-h class from their individual kitchens via Zoom with phone/device camera and microphones turned on. A study team member managed the Zoom chat and session controls. The facilitator had one camera on his face, and another on the demonstrative cutting board for the live demo. | 1:1 sessions with the language-specific RD lasted 45–60 min and were virtual or in-person in the RD clinic-based office, per patient preference. Language-specific group sessions lasted 60–90 min and took place in a conference room at the clinic. Virtual sessions took place via phone call. |
| Session Handouts and Educational Visuals | Recipes and educational handouts were selected based on the cultural representation of learners from the Diabetes and Carbohydrate Module of the Health Meets Food curriculum [33]. | Food models, measuring cups, various nutrition handouts, fact sheet handouts, sugar demo posters, exercise videos, and food labels were provided by the RDs. |
| Resources Issued to Subjects | Cooking equipment (frying pan, cutting board, measuring cups, cutlery), Recipe binders, grocery shopping lists, Zoom instructions, Pantry Pack (non-perishable foods, oils, and spices), Food Assistance Resource List, $10 Grocery stipend per class | Cooking equipment (frying pan, cutting board, measuring cups, cutlery) |
| Pre-Class Preparation | Participants were expected to review the shopping list and procure ingredients before the start of each class. | Participants were expected to find transportation to and from the clinic for the in-person meetings. |
| Session Focus | eCulinary Medicine | Medical Nutrition Therapy |
| Session 1 | Knife safety demonstration; kitchen orientation, temperature safety, and “danger zone” including cross-contamination; How to make your own vegetable stock and salad dressing; Common kitchen tools, common cooking abbreviations, appropriate knife cuts, and cooking terms; How to cut a yellow onion, a bell pepper. | 1:1 Virtual/In-Person Meeting: Medication adherence related to meal timing; Glucose monitoring and pattern management intro; Diet history review; Assess barriers; Make referrals; Carbohydrate awareness; Beverage recommendations (including alcohol); Discuss recent lab results; Exercise recommendations; Goal Setting |
| Session 2 | Caramelization of carbohydrates for flavor-building, balancing texture for palatability; Tips for cooking with whole grains; Alternative use and storage of leftovers. | 1:1 Virtual/In-Person Meeting: Meal composition and timing relative to medication and glucose log; Review carbohydrate awareness and consistency; Snack recommendations and options |
| Session 3 | Meal planning tips; Substitutions for oils and butters in baking and other dishes; Tips for shopping for and preparing/storing seafood/shellfish for best taste and safe handling. | Group In-Person Meeting: Meal planning tips; Sugar-containing beverages; fat content impact on Diabetes and Cardiovascular disease; Plate method principles with demonstration and participation; Food label review; Grocery shopping and cooking tips; exercise adherence tips |
| Session 4 | Discuss sofrito and flavor building, mirepoix, especially in vegan/vegetarian cooking, and strategies for flavor building when reducing red meat and saturated fat. | 1:1 Virtual/In-Person Meeting: Review food label reading using items from pantry/fridge |
| Session 5 | Review previous sessions, assess knowledge gaps, and address any deficits; Tips for adding more vegetables and whole grains into familiar dishes. | Group In-Person Meeting: Importance of weight loss/maintenance; Eating and preparing meals as a family; Heart Health- increasing fibers and healthy fats; Maintaining motivation and how to get back on track; Problem-solving when eating outside of the home, holidays, etc. |
| Session 6 | Tips for when to use which type of fat/oil; Education on smoke point. | 1:1 Virtual/In-Person Meeting: Review goals and progress |
| Original Recruitment Design | Interview/Observational Feedback | Description of Change |
|---|---|---|
| Study team schedules participants for pick up, conducts reminder calls, and coordinates with DBC * staff to meet participants during first DBC food distribution to complete baseline consent/survey | Study Staff Feedback
|
|
Participant Feedback
| ||
| Study team contacts patients to notify them of the study opportunity and randomization arm | Participant Feedback
|
|
| Study team asks patients about internet access prior to consent as a screening question | Study Staff Feedback
|
|
| Original Medical Nutrition Therapy | Interview/Observational Feedback | Description of Change |
| Study recruitment is completed by the study staff, and participants are transitioned into the MNT program | Study Staff Feedback
|
|
| MNT program run and coordinated by clinic-based RDs with experience in diabetes management within context of a clinic visit | Participant Feedback
|
|
| Original Culinary Medicine Design | Interview/Observational Feedback | Description of Change |
| Participants procure their ingredients and log in to join eCM class on Zoom from their own kitchen | Participant Feedback
|
|
| Participants receive a call from the study team the day prior to the class to remind them of the class time and what recipe will be prepared | Study Staff Feedback
|
|
| Participants receive recipe binders with cooking instructions, handouts, and shopping lists to prepare for each class | Study Staff Feedback
|
|
| Total n = 79 | Medical Nutrition Therapy Arm n = 43 | eCulinary Medicine Arm n = 36 | |
|---|---|---|---|
| Age (n, %) | 49.7, SD 11.26, range: 24–82 | 48.7 | 50.9 |
| 20–29 | 4 (5.1%) | 2 (4.7%) | 2 (5.6%) |
| 30–39 | 12 (15.2%) | 9 (20.9%) | 3 (8.3%) |
| 40–49 | 21 (26.6%) | 10 (23.3%) | 11 (30.6%) |
| 50–59 | 29 (36.7%) | 15 (34.9%) | 14 (38.9%) |
| 60–69 | 11 (13.9%) | 6 (14.0%) | 5 (13.9%) |
| 70–79 | 1 (1.3%) | 1 (2.3%) | 0 (0.0%) |
| 80–89 | 1 (1.3%) | 0 (0.0%) | 1 (2.8%) |
| Female (n, %) | 65 (82%) | 35 (81%) | 30 (83%) |
| Preferred language Spanish (n, %) | 44 (56%) | 25 (58%) | 19 (53%) |
| Less than high school education (n, %) * | 30 (38%) | 18 (42%) | 12 (33%) |
| Food Insecure (n, %) * | 34 (43%) | 16 (37%) | 18 (50%) |
| Using Food Assistance (n, %) * | 50 (63%) | 27 (63%) | 23 (64%) |
| Household Size (average number of people, including children) * | 3.8, SD 2.06, range: 1–12 | 4.1 | 3.6 |
| Baseline HbA1c Value (average mg/dL) | 9.4%, SD 1.84, range: 7.0–15.1% | 9.6% | 9.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGuire, M.F.; Chen, P.M.; Smith-Morris, C.; Albin, J.; Siler, M.D.; Lopez, M.A.; Pruitt, S.L.; Merrill, V.C.; Bowen, M.E. Redesigning Recruitment and Engagement Strategies for Virtual Culinary Medicine and Medical Nutrition Interventions in a Randomized Trial of Patients with Uncontrolled Type 2 Diabetes. Nutrients 2023, 15, 4124. https://doi.org/10.3390/nu15194124
McGuire MF, Chen PM, Smith-Morris C, Albin J, Siler MD, Lopez MA, Pruitt SL, Merrill VC, Bowen ME. Redesigning Recruitment and Engagement Strategies for Virtual Culinary Medicine and Medical Nutrition Interventions in a Randomized Trial of Patients with Uncontrolled Type 2 Diabetes. Nutrients. 2023; 15(19):4124. https://doi.org/10.3390/nu15194124
Chicago/Turabian StyleMcGuire, Molly F., Patricia M. Chen, Carolyn Smith-Morris, Jaclyn Albin, Milette D. Siler, Miguel Angel Lopez, Sandi L. Pruitt, Vincent C. Merrill, and Michael E. Bowen. 2023. "Redesigning Recruitment and Engagement Strategies for Virtual Culinary Medicine and Medical Nutrition Interventions in a Randomized Trial of Patients with Uncontrolled Type 2 Diabetes" Nutrients 15, no. 19: 4124. https://doi.org/10.3390/nu15194124