
Effect of a Multifaceted Intervention on Children’s Body Image and the Mediating Role of Body Image in Changes in Adiposity Indicators
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Description of Intervention
2.3. Measurements
2.4. Statistical Analyses
3. Results
3.1. General Characteristics
3.2. The Effect of Intervention on the Children’s Body Image
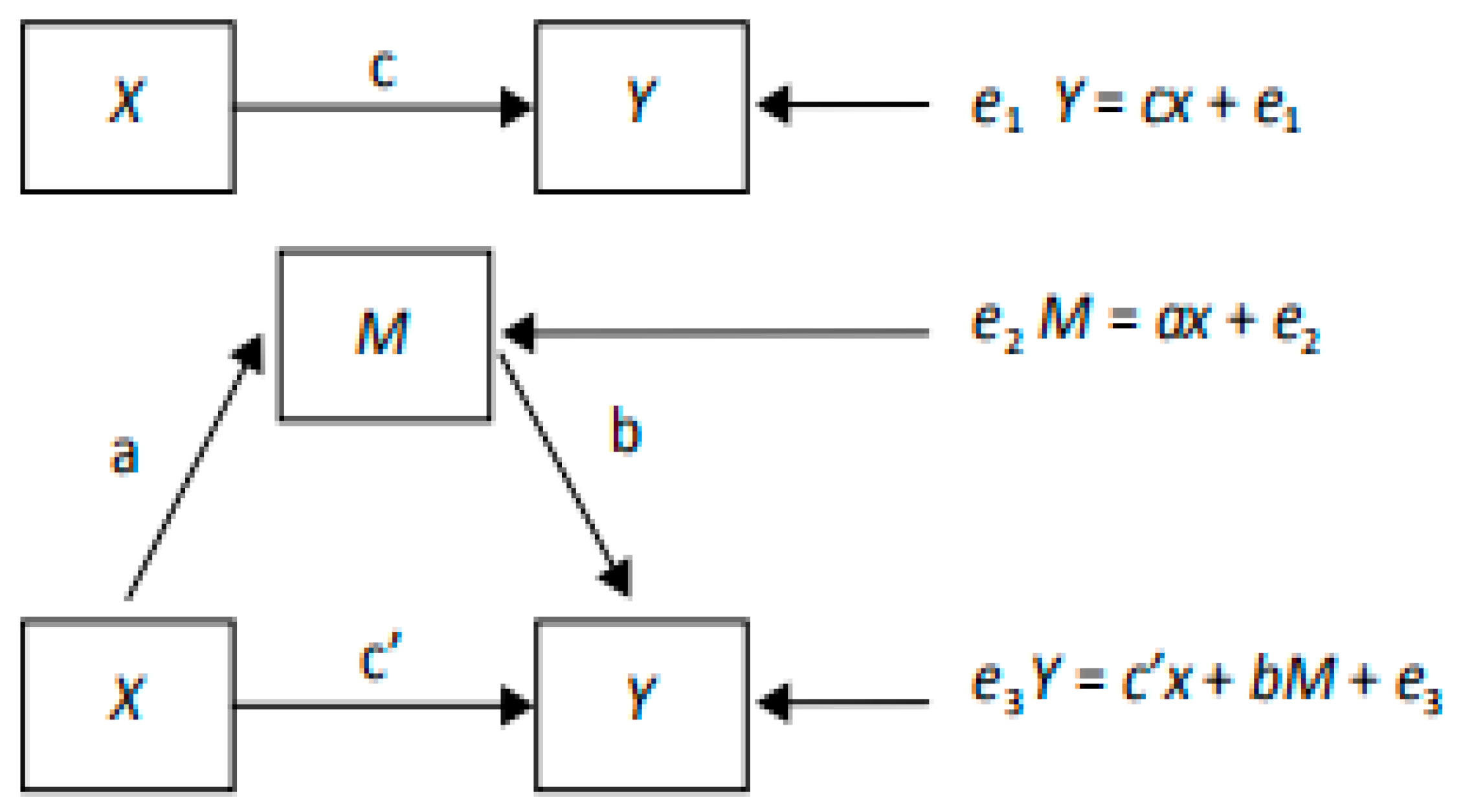
3.3. Mediating Role of Body Image between the Intervention and the Changes in Adiposity Indicators
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Dong, Y.; Jan, C.; Ma, Y.; Dong, B.; Zou, Z.; Yang, Y.; Xu, R.; Song, Y.; Ma, J.; Sawyer, S.M.; et al. Economic development and the nutritional status of Chinese school-aged children and adolescents from 1995 to 2014: An analysis of five successive national surveys. Lancet Diabetes Endocrinol. 2019, 7, 288–299. [Google Scholar] [CrossRef] [PubMed]
- Weihrauch-Blüher, S.; Schwarz, P.; Klusmann, J.H. Childhood obesity: Increased risk for cardiometabolic disease and cancer in adulthood. Metab. Clin. Exp. 2019, 92, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Weihrauch-Blüher, S.; Wiegand, S. Risk Factors and Implications of Childhood Obesity. Curr. Obes. Rep. 2018, 7, 254–259. [Google Scholar] [CrossRef]
- Sagar, R.; Gupta, T. Psychological Aspects of Obesity in Children and Adolescents. Indian J. Pediatr. 2018, 85, 554–559. [Google Scholar] [CrossRef]
- Sanders, R.H.; Han, A.; Baker, J.S.; Cobley, S. Childhood obesity and its physical and psychological co-morbidities: A systematic review of Australian children and adolescents. Eur. J. Pediatr. 2015, 174, 715–746. [Google Scholar] [CrossRef]
- Koch, P.A.; Contento, I.R.; Gray, H.L.; Burgermaster, M.; Bandelli, L.; Abrams, E.; Di Noia, J. Food, Health, & Choices: Curriculum and Wellness Interventions to Decrease Childhood Obesity in Fifth-Graders. J. Nutr. Educ. Behav. 2019, 51, 440–455. [Google Scholar] [CrossRef]
- Gába, A.; Mitáš, J.; Jakubec, L. Associations between accelerometer-measured physical activity and body fatness in school-aged children. Environ. Health Prev. Med. 2017, 22, 43. [Google Scholar] [CrossRef]
- Costa Lda, C.; Silva, D.A.; Almeida Sde, S.; de Vasconcelos Fde, A. Association between inaccurate estimation of body size and obesity in schoolchildren. Trends Psychiatry Psychother. 2015, 37, 220–226. [Google Scholar] [CrossRef]
- Cash, T.F. Body Image: Past, Present, and Future; Elsevier: Amsterdam, The Netherlands, 2004. [Google Scholar]
- Song, L.; Zhang, Y.; Chen, T.; Maitusong, P.; Lian, X. Association of body perception and dietary weight management behaviours among children and adolescents aged 6–17 years in China: Cross-sectional study using CHNS (2015). BMC Public Health 2022, 22, 175. [Google Scholar] [CrossRef]
- Aloufi, A.D.; Najman, J.M.; Mamun, A.A. The Association between Body Weight Misclassification in Adolescence and Body Fat and Waist Circumference in Adulthood: A Longitudinal Study. Nutrients 2022, 14, 4765. [Google Scholar] [CrossRef]
- Quick, V.; Nansel, T.R.; Liu, D.; Lipsky, L.M.; Due, P.; Iannotti, R.J. Body size perception and weight control in youth: 9-year international trends from 24 countries. Int. J. Obes. 2014, 38, 988–994. [Google Scholar] [CrossRef]
- Swaminathan, S.; Selvam, S.; Pauline, M.; Vaz, M. Associations between body weight perception and weight control behaviour in South Indian children: A cross-sectional study. BMJ Open 2013, 3, 2239. [Google Scholar] [CrossRef]
- Quan, G.H.; Xuan, W.B.; Li, S.L.; Ting, L.; Lu, W.; Guo, F.L.; Jun, M. The Mediating Effect of Body Dissatisfaction in Association between Obesity and Dietary Behavior Changes for Weight Loss in Chinese Children. Biomed. Environ. Sci. 2019, 32, 639. [Google Scholar] [CrossRef]
- Min, J.; Yan, A.F.; Wang, V.H.C.; Wang, Y. Obesity, body image, and its impact on children’s eating and exercise behaviors in China: A nationwide longitudinal study. Prev. Med. 2018, 106, 101–106. [Google Scholar] [CrossRef]
- Duchin, O.; Marin, C.; Mora-Plazas, M.; Mendes de Leon, C.; Lee, J.M.; Baylin, A.; Villamor, E. A prospective study of body image dissatisfaction and BMI change in school-age children. Public Health Nutr. 2015, 18, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Hunger, J.M.; Tomiyama, A.J. Weight Labeling and Obesity: A Longitudinal Study of Girls Aged 10 to 19 Years. JAMA Pediatr. 2014, 168, 579–580. [Google Scholar] [CrossRef] [PubMed]
- Incledon, E.; Gerner, B.; Hay, M.; Brennan, L.; Wake, M. Psychosocial predictors of 4-year BMI change in overweight and obese children in primary care. Obesity 2013, 21, E262–E270. [Google Scholar] [CrossRef]
- Huang, J.S.; Norman, G.J.; Zabinski, M.F.; Calfas, K.; Patrick, K. Body image and self-esteem among adolescents undergoing an intervention targeting dietary and physical activity behaviors. J. Adolesc. Health 2007, 40, 245–251. [Google Scholar] [CrossRef]
- Annesi, J.J.; Porter, K.J. Reciprocal effects of exercise and nutrition treatment-induced weight loss with improved body image and physical self-concept. Behav. Med. 2015, 41, 18–24. [Google Scholar] [CrossRef]
- Liu, Z.; Gao, P.; Gao, A.Y.; Lin, Y.; Feng, X.X.; Zhang, F.; Xu, L.Q.; Niu, W.Y.; Fang, H.; Zhou, S.; et al. Effectiveness of a Multifaceted Intervention for Prevention of Obesity in Primary School Children in China: A Cluster Randomized Clinical Trial. JAMA Pediatr. 2022, 176, e214375. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wu, Y.; Niu, W.Y.; Feng, X.; Lin, Y.; Gao, A.; Zhang, F.; Fang, H.; Gao, P.; Li, H.J.; et al. A school-based, multi-faceted health promotion programme to prevent obesity among children: Protocol of a cluster-randomised controlled trial (the DECIDE-Children study). BMJ Open 2019, 9, e027902. [Google Scholar] [CrossRef]
- Collins, M.E. Body figure perceptions and preferences among preadolescent children. Int. J. Eat. Disord. 1991, 10, 199–208. [Google Scholar] [CrossRef]
- Li, Y.; Hu, X.; Ma, W.; Wu, J.; Ma, G. Body image perceptions among Chinese children and adolescents. Body Image 2005, 2, 91–103. [Google Scholar] [CrossRef]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- WS/T 586-2018; Screening for Overweight and Obesity among School-Age Children and Adolescents. National Health Commission of the People’s Republic of China: Beijing, China, 2018.
- WS/T 456-2014; Screening for Malnutrition among School-Age Children and Adolescents. National Health Commission of the People’s Republic of China: Beijing, China, 2014.
- Chinese National Physical Fitness and Health Research Team. Research Report on Chinese Students’ Physical Fitness and Health 2005; Beijing Higher Education Press: Beijing, China, 2007. [Google Scholar]
- Gesell, S.B.; Scott, T.A.; Barkin, S.L. Accuracy of perception of body size among overweight Latino preadolescents after a 6-month physical activity skills building intervention. Clin. Pediatr. 2010, 49, 323–329. [Google Scholar] [CrossRef]
- O’Connor, J.N.; Golley, R.K.; Perry, R.A.; Magarey, A.M.; Truby, H. A longitudinal investigation of overweight children’s body perception and satisfaction during a weight management program. Appetite 2015, 85, 48–51. [Google Scholar] [CrossRef]
- Eldridge, G.; Paul, L.; Bailey, S.J.; Ashe, C.B.; Martz, J.; Lynch, W. Effects of parent-only childhood obesity prevention programs on BMIz and body image in rural preteens. Body Image 2016, 16, 143–153. [Google Scholar] [CrossRef]
- Nguyen, B.; Shrewsbury, V.A.; O’Connor, J.; Steinbeck, K.S.; Hill, A.J.; Shah, S.; Kohn, M.R.; Torvaldsen, S.; Baur, L.A. Two-year outcomes of an adjunctive telephone coaching and electronic contact intervention for adolescent weight-loss maintenance: The Loozit randomized controlled trial. Int. J. Obes. 2013, 37, 468–472. [Google Scholar] [CrossRef]
- Guest, E.; Zucchelli, F.; Costa, B.; Bhatia, R.; Halliwell, E.; Harcourt, D. A systematic review of interventions aiming to promote positive body image in children and adolescents. Body Image 2022, 42, 58–74. [Google Scholar] [CrossRef]
- Mastellos, N.; Gunn, L.H.; Felix, L.M.; Car, J.; Majeed, A. Transtheoretical model stages of change for dietary and physical exercise modification in weight loss management for overweight and obese adults. Cochrane Database Syst. Rev. 2014, 2014, Cd008066. [Google Scholar] [CrossRef] [PubMed]
- McArthur, L.H.; Riggs, A.; Uribe, F.; Spaulding, T.J. Health Belief Model Offers Opportunities for Designing Weight Management Interventions for College Students. J. Nutr. Educ. Behav. 2018, 50, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Harring, H.A.; Montgomery, K.; Hardin, J. Perceptions of body weight, weight management strategies, and depressive symptoms among US college students. J. Am. Coll. Health 2010, 59, 43–50. [Google Scholar] [CrossRef]
- Griffiths, S.; Murray, S.B.; Bentley, C.; Gratwick-Sarll, K.; Harrison, C.; Mond, J.M. Sex Differences in Quality of Life Impairment Associated With Body Dissatisfaction in Adolescents. J. Adolesc. Health 2017, 61, 77–82. [Google Scholar] [CrossRef]
- Gall, K.; van Zutven, K.; Lindstrom, J.; Bentley, C.; Gratwick-Sarll, K.; Harrison, C.; Lewis, V.; Mond, J. Obesity and emotional well-being in adolescents: Roles of body dissatisfaction, loss of control eating, and self-rated health. Obesity 2016, 24, 837–842. [Google Scholar] [CrossRef]
- Bullivant, B.; Denham, A.R.; Stephens, C.; Olson, R.E.; Mitchison, D.; Gill, T.; Maguire, S.; Latner, J.D.; Hay, P.; Rodgers, B.; et al. Elucidating knowledge and beliefs about obesity and eating disorders among key stakeholders: Paving the way for an integrated approach to health promotion. BMC Public Health 2019, 19, 1681. [Google Scholar] [CrossRef]
- Goldschmidt, A.B.; Wall, M.; Choo, T.H.; Becker, C.; Neumark-Sztainer, D. Shared risk factors for mood-, eating-, and weight-related health outcomes. Health Psychol. 2016, 35, 245–252. [Google Scholar] [CrossRef]
- Stabouli, S.; Erdine, S.; Suurorg, L.; Jankauskienė, A.; Lurbe, E. Obesity and Eating Disorders in Children and Adolescents: The Bidirectional Link. Nutrients 2021, 13, 4321. [Google Scholar] [CrossRef]
- Chung, A.E.; Perrin, E.M.; Skinner, A.C. Accuracy of child and adolescent weight perceptions and their relationships to dieting and exercise behaviors: A NHANES study. Acad. Pediatr. 2013, 13, 371–378. [Google Scholar] [CrossRef]
- Fan, M.; Jin, Y. The Effects of Weight Perception on Adolescents’ Weight-Loss Intentions and Behaviors: Evidence from the Youth Risk Behavior Surveillance Survey. Int. J. Environ. Res. Public Health 2015, 12, 14640–14668. [Google Scholar] [CrossRef]
- Cuypers, K.; Kvaløy, K.; Bratberg, G.; Midthjell, K.; Holmen, J.; Holmen, T.L. Being Normal Weight but Feeling Overweight in Adolescence May Affect Weight Development into Young Adulthood-An 11-Year Followup: The HUNT Study, Norway. J. Obes. 2012, 2012, 601872. [Google Scholar] [CrossRef] [PubMed]
- Sutin, A.R.; Terracciano, A. Body weight misperception in adolescence and incident obesity in young adulthood. Psychol. Sci. 2015, 26, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Liechty, J.M.; Lee, M.J. Body size estimation and other psychosocial risk factors for obesity onset among US adolescents: Findings from a longitudinal population level study. Int. J. Obes. 2015, 39, 601–607. [Google Scholar] [CrossRef]
- Poobalan, A.S.; Aucott, L.S.; Clarke, A.; Smith, W.C. Physical activity attitudes, intentions and behaviour among 18–25 year olds: A mixed method study. BMC Public Health 2012, 12, 640. [Google Scholar] [CrossRef] [PubMed]
- Roberto, C.A.; Swinburn, B.; Hawkes, C.; Huang, T.T.; Costa, S.A.; Ashe, M.; Zwicker, L.; Cawley, J.H.; Brownell, K.D. Patchy progress on obesity prevention: Emerging examples, entrenched barriers, and new thinking. Lancet 2015, 385, 2400–2409. [Google Scholar] [CrossRef]
- Franks, P.W.; Ravussin, E.; Hanson, R.L.; Harper, I.T.; Allison, D.B.; Knowler, W.C.; Tataranni, P.A.; Salbe, A.D. Habitual physical activity in children: The role of genes and the environment. Am. J. Clin. Nutr. 2005, 82, 901–908. [Google Scholar] [CrossRef]
- Cheng, T.O. China’s epidemic of child obesity: An ounce of prevention is better than a pound of treatment. Int. J. Cardiol. 2014, 172, 1–7. [Google Scholar] [CrossRef]
- Day, K.; Alfonzo, M.; Chen, Y.; Guo, Z.; Lee, K.K. Overweight, obesity, and inactivity and urban design in rapidly growing Chinese cities. Health Place 2013, 21, 29–38. [Google Scholar] [CrossRef]


{kind=link}
| Intervention (n = 648) | Control (n = 639) | P | |
|---|---|---|---|
| Number of schools | 12 | 12 | - |
| Number of children/school, median(range) | 54(47~60) | 53(46~58) | - |
| Sex, n (%) | 0.167 | ||
| Male | 329 (50.8) | 350 (54.8) | |
| Female | 319 (49.2) | 289 (45.2) | |
| Region, n (%) | 0.448 | ||
| Beijing | 234 (36.1) | 210 (32.9) | |
| Changzhi of Shanxi | 185 (28.5) | 187 (29.3) | |
| Urumuqi of Xinjiang | 229 (35.3) | 242 (37.9) | |
| Nutritional status | 0.232 | ||
| Normal weight with lower BMI, n (%) | 142 (21.9) | 130 (20.3) | |
| Normal weight with higher BMI, n (%) | 242 (37.4) | 216 (33.8) | |
| Overweight and obesity n (%) | 264 (40.7) | 293 (45.9) | |
| Age (year) | 9.6 (0.4) | 9.6 (0.4) | 0.748 |
| BMI (kg/m2) | 18.8 (3.6) | 19.0 (3.6) | 0.315 |
| BMI Z score | 0.8 (1.3) | 0.9 (1.3) | 0.244 |
| Waist circumference (cm) | 65.9 (10.0) | 66.3 (10.9) | 0.434 |
| Body fat percentage (%) | 21.4 (10.2) | 21.8 (10.2) | 0.542 |
| Baseline | End of Trial | Δ | OR (95%CI) | p | |
|---|---|---|---|---|---|
| Body size perception | |||||
| Control group | 334 (52.3%) | 376 (58.8%) | 6.5% | Ref | |
| Intervention group | 376 (58.0%) | 481 (74.2%) | 16.2% | 2.42 (1.70, 3.45) | <0.001 * |
| Body size expectation | |||||
| Control group | 162 (25.4%) | 125 (19.6%) | −5.8% | Ref | 0.010 * |
| Intervention group | 159 (24.5%) | 164 (25.3%) | 0.8% | 1.74 (1.14, 2.66) |
| BMI (kg/m2) | BMI Z Score | WC (cm) | BF (%) | |||||
|---|---|---|---|---|---|---|---|---|
| Β (95%CI) | p | β (95%CI) | p | β (95%CI) | p Value | β (95%CI) | p | |
| Body size perception b | ||||||||
| Overweight/obese | ||||||||
| Indirect effect | −0.08 (−0.15, −0.03) | 0.002 * | −0.04 (−0.06, −0.02) | <0.001 * | −0.16 (−0.39, 0.01) | 0.081 | −0.28 (−0.50, −0.10) | <0.001 * |
| Direct effect | −0.69 (1.07, 0.30) | 0.001 * | −0.17 (−0.27, −0.08) | <0.001 * | −1.89 (−3.63, −0.18) | 0.028 * | −1.10 (−2.19, 0.03) | 0.055 |
| Total effect | −0.77 (−1.15, −0.39) | <0.001 * | −0.21 (−0.30, −0.11) | <0.001 * | −2.05 (−3.77, −0.35) | 0.014 * | −1.38 (−2.47, −0.27) | 0.016 * |
| Normal weight with higher BMI | ||||||||
| Indirect effect | −0.09 (−0.19, −0.01) | 0.025 * | −0.04 (−0.07, −0.01) | 0.023 * | −0.16 (−0.37, −0.01) | 0.028 * | −0.18 (−0.41, −0.02) | 0.020 * |
| Direct effect | −0.16 (−0.36, 0.05) | 0.132 | −0.08 (−0.18, 0.02) | 0.119 | −1.11 (−2.39, 0.21) | 0.097 | −0.80 (−1.66, 0.05) | 0.070 |
| Total effect | −0.25 (−0.47, −0.03) | 0.023 * | −0.12 (−0.22, −0.01) | 0.022 * | −1.81 (−3.30, −0.31) | 0.018 * | −0.98 (−1.87, −0.12) | 0.025 * |
| Normal weight with lower BMI | ||||||||
| Indirect effect | 0.00 (−0.02, 0.02) | 0.832 | −0.00 (−0.01, 0.01) | 0.930 | 0.05 (−0.05, 0.21) | 0.417 | −0.01 (−0.08, 0.04) | 0.726 |
| Direct effect | −0.17 (−0.34, 0.01) | 0.074 | −0.11 (−0.22, 0.01) | 0.073 | −1.35 (−2.59, −0.09) | 0.037 * | −0.70 (−1.33, −0.07) | 0.027 * |
| Total effect | −0.17 (−0.34, 0.02) | 0.079 | −0.11 (−0.22, 0.01) | 0.074 | −1.30 (−2.56, −0.04) | 0.044 * | −0.71 (−1.34, −0.08) | 0.026 * |
| Body size expectation b | ||||||||
| Overweight/obese | ||||||||
| Indirect effect | −0.04 (−0.08, −0.01) | 0.032 * | −0.02 (−0.04, −0.01) | 0.003 * | −0.13 (−0.33, 0.01) | 0.080 | −0.15 (−0.30, −0.03) | 0.006 * |
| Direct effect | −0.74 (−1.09, −0.34) | <0.001 * | −0.19 (−0.29, −0.10) | <0.001 * | −1.99 (−3.83, −0.16) | 0.033 * | −1.26 (−2.33, −0.20) | 0.023 * |
| Total effect | −0.78 (−1.12, −0.38) | <0.001 * | −0.21 (−0.31, −0.11) | <0.001 * | −2.12 (−3.96, −0.28) | 0.022 * | −1.41 (−2.48, −0.35) | 0.013 * |
| Normal weight with higher BMI | ||||||||
| Indirect effect | −0.01 (−0.06, 0.03) | 0.544 | −0.01 (−0.04, 0.02) | 0.527 | −0.04 (−0.20, 0.09) | 0.521 | −0.03 (−0.14, 0.07) | 0.538 |
| Direct effect | −0.23 (−0.44, −0.02) | 0.035 * | −0.10 (−0.19, −0.01) | 0.042 * | −1.16 (−2.43, 0.06) | 0.067 | −0.93 (−1.83, −0.06) | 0.035 * |
| Total effect | −0.24 (−0.46, −0.03) | 0.028 * | −0.11 (−0.21, −0.01) | 0.034 * | −1.20 (−2.47, 0.04) | 0.058 | −0.96 (−1.86, −0.08) | 0.030 * |
| Normal weight with lower BMI | ||||||||
| Indirect effect | 0.00 (−0.02, 0.03) | 0.824 | 0.00 (−0.01, 0.02) | 0.830 | 0.00 (−0.12, 0.11) | 0.931 | 0.00 (−0.07, 0.07) | 0.942 |
| Direct effect | −0.17 (−0.34, 0.01) | 0.065 | −0.11 (−0.22, 0.01) | 0.074 | −1.31 (−2.61, −0.02) | 0.045 * | −0.67 (−1.28, −0.06) | 0.029 * |
| Total effect | −0.17 (−0.34, 0.01) | 0.070 | −0.11 (−0.22, 0.01) | 0.077 | −1.31 (−2.63, −0.03) | 0.046 * | −0.67 (−1.28, −0.06) | 0.030 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyu, J.; Wan, Z.; Liu, Z.; Zhou, S.; Feng, X.; Gao, A.; Lin, Y.; Zhang, F.; Wang, H. Effect of a Multifaceted Intervention on Children’s Body Image and the Mediating Role of Body Image in Changes in Adiposity Indicators. Nutrients 2023, 15, 3951. https://doi.org/10.3390/nu15183951
Lyu J, Wan Z, Liu Z, Zhou S, Feng X, Gao A, Lin Y, Zhang F, Wang H. Effect of a Multifaceted Intervention on Children’s Body Image and the Mediating Role of Body Image in Changes in Adiposity Indicators. Nutrients. 2023; 15(18):3951. https://doi.org/10.3390/nu15183951
Chicago/Turabian StyleLyu, Jinlang, Zhongshang Wan, Zheng Liu, Shuang Zhou, Xiangxian Feng, Aiyu Gao, Yi Lin, Fang Zhang, and Haijun Wang. 2023. "Effect of a Multifaceted Intervention on Children’s Body Image and the Mediating Role of Body Image in Changes in Adiposity Indicators" Nutrients 15, no. 18: 3951. https://doi.org/10.3390/nu15183951