

Effect of Mediterranean Dietary Pattern on Cognitive Status in Community-Dwelling Older Adults
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Cognitive Status Screening Tools
2.3. Sociodemographic-, Health-, and Nutrition-Related Data
2.4. Statistical Analysis
3. Results
3.1. Description of the Total Sample
3.2. Cognitive Status and Characteristics of the Sample Based on Literacy
3.3. Cognitive Status and Nutrient Adequacy
3.4. Cognitive Status and Food Intake
3.5. Dietary Patterns and Associated Factors
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. World Population Prospects 2019—Volume II Demog. [Internet]. 2020. Available online: https://population.un.org/wpp/Publications/Files/WPP2019_Volume-II-Demographic-Profiles.pdf (accessed on 23 June 2020).
- Department of Economic and Social Affairs, Population Division. World Population Ageing, 2019 Highlights; United Nations: New York, NY, USA, 2020.
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2017 Highlights. [Internet]. 2017. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2017_Highlights.pdf (accessed on 1 November 2021).
- Fabrício, D.d.M.; Chagas, M.H.N.; Diniz, B.S. Frailty and cognitive decline. Transl. Res. 2020, 221, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. Selective review of cognitive aging. J. Int. Neuropsychol. Soc. 2010, 16, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gómez, M.E.; Zapico, S.C. Frailty, Cognitive Decline, Neurodegenerative Diseases and Nutrition Interventions. Int. J. Mol. Sci. 2019, 20, 2842. [Google Scholar] [CrossRef] [PubMed]
- González-Gross, M.; Marcos, A.; Pietrzik, K. Nutrition and cognitive impairment in the elderly. Br. J. Nutr. 2001, 86, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. The New Geriatric Giants. Clin. Geriatr. Med. 2017, 33, xi–xii. [Google Scholar] [CrossRef]
- Robertson, D.A.; Savva, G.M.; Kenny, R.A. Frailty and cognitive impairment—A review of the evidence and causal mechanisms. Ageing Res. Rev. 2013, 12, 840–851. [Google Scholar] [CrossRef]
- Sugimoto, T.; Sakurai, T.; Ono, R.; Kimura, A.; Saji, N.; Niida, S.; Toba, K.; Chen, L.-K.; Arai, H. Epidemiological and clinical significance of cognitive frailty: A mini review. Ageing Res. Rev. 2018, 44, 1–7. [Google Scholar] [CrossRef]
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Wu, B.; Lyu, Y.B.; Cao, Z.J.; Wei, Y.; Shi, W.Y.; Gao, X.; Zhou, J.H.; Kraus, V.B.; Zhao, F.; Chen, X.; et al. Associations of Sarcopenia, Handgrip Strength and Calf Circumference with Cognitive Impairment among Chinese Older Adults. Biomed. Environ. Sci. 2021, 34, 859–870. [Google Scholar]
- Allès, B.; Samieri, C.; Féart, C.; Jutand, M.-A.; Laurin, D.; Barberger-Gateau, P. Dietary patterns: A novel approach to examine the link between nutrition and cognitive function in older individuals. Nutr. Res. Rev. 2012, 25, 207–222. [Google Scholar] [CrossRef]
- Bottiglieri, T. Folate, vitamin B12, and neuropsychiatric disorders. Nutr. Rev. 1996, 54, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Chouet, J.; Ferland, G.; Feart, C.; Rolland, Y.; Presse, N.; Boucher, K.; Barberger-Gateau, P.; Beauchet, O.; Annweiler, C. Dietary Vitamin K Intake Is Associated with Cognition and Behaviour among Geriatric Patients: The CLIP Study. Nutrients 2015, 7, 6739–6750. [Google Scholar] [CrossRef] [PubMed]
- Feart, C.; Letenneur, L.; Helmer, C.; Samieri, C.; Schalch, W.; Etheve, S.; Delcourt, C.; Dartigues, J.-F.; Barberger-Gateau, P. Plasma Carotenoids Are Inversely Associated with Dementia Risk in an Elderly French Cohort. J. Gerontol. Ser. A 2015, 71, 683–688. [Google Scholar] [CrossRef]
- Marseglia, A.; Xu, W.; Fratiglioni, L.; Fabbri, C.; Berendsen, A.A.M.; Bialecka-Debek, A.; Jennings, A.; Gillings, R.; Meunier, N.; Caumon, E.; et al. Effect of the NU-AGE Diet on Cognitive Functioning in Older Adults: A Randomized Controlled Trial. Front. Physiol. 2018, 9, 349. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and Prevention of Cognitive Impairment. The Lancet Neurology. [Internet]. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1474442218303387 (accessed on 13 October 2018).
- Selhub, J.; Troen, A.; Rosenberg, I.H. B vitamins and the aging brain. Nutr. Rev. 2010, 68, S112–S118. [Google Scholar]
- Cooper, J.K. Nutrition and the brain: What advice should we give? Neurobiol. Aging 2014, 35, S79–S83. [Google Scholar] [CrossRef]
- Allès, B.; Samieri, C.; Jutand, M.-A.; Carmichael, P.-H.; Shatenstein, B.; Gaudreau, P.; Ferland, G.; Barberger-Gateau, P.; Laurin, D. Nutrient Patterns, Cognitive Function, and Decline in Older Persons: Results from the Three-City and NuAge Studies. Nutrients 2019, 11, 1808. [Google Scholar] [CrossRef]
- Barberger-Gateau, P.; Lambert, J.-C.; Féart, C.; Pérès, K.; Ritchie, K.; Dartigues, J.-F.; Alpérovitch, A. From Genetics to Dietetics: The Contribution of Epidemiology to Understanding Alzheimer’s Disease. J. Alzheimer’s Dis. 2013, 33, S457–S463. [Google Scholar] [CrossRef]
- Barberger-Gateau, P.; Samieri, C.; Feart, C.; Plourde, M. Dietary Omega 3 Polyunsaturated Fatty Acids and Alzheimers Disease: Interaction with Apolipoprotein E Genotype. Curr. Alzheimer Res. 2011, 8, 479–491. [Google Scholar] [CrossRef]
- Barnard, N.D.; Bush, A.I.; Ceccarelli, A.; Cooper, J.; de Jager, C.A.; Erickson, K.I.; Fraser, G.; Kesler, S.; Levin, S.M.; Lucey, B.; et al. Dietary and lifestyle guidelines for the prevention of Alzheimer’s disease. Neurobiol. Aging 2014, 35, S74–S78. [Google Scholar] [CrossRef] [PubMed]
- Rathod, R.; Kale, A.; Joshi, S. Novel insights into the effect of vitamin B12 and omega-3 fatty acids on brain function. J. Biomed. Sci. 2016, 23, 17. [Google Scholar] [CrossRef] [PubMed]
- Samieri, C.; Féart, C.; Letenneur, L.; Dartigues, J.-F.; Pérès, K.; Auriacombe, S.; Peuchant, E.; Delcourt, C.; Barberger-Gateau, P. Low plasma eicosapentaenoic acid and depressive symptomatology are independent predictors of dementia risk. Am. J. Clin. Nutr. 2008, 88, 714–721. [Google Scholar] [CrossRef]
- Barnard, N.D.; Bunner, A.E.; Agarwal, U. Saturated and trans fats and dementia: A systematic review. Neurobiol. Aging 2014, 35, S65–S73. [Google Scholar] [CrossRef] [PubMed]
- Ancelin, M.-L.; Ripoche, E.; Dupuy, A.-M.; Samieri, C.; Rouaud, O.; Berr, C.; Carrière, I.; Ritchie, K. Gender-specific associations between lipids and cognitive decline in the elderly. Eur. Neuropsychopharmacol. 2014, 24, 1056–1066. [Google Scholar] [CrossRef] [PubMed]
- Angeloni, C.; Malaguti, M.; Barbalace, M.C.; Hrelia, S. Bioactivity of Olive Oil Phenols in Neuroprotection. Int. J. Mol. Sci. 2017, 18, 2230. [Google Scholar] [CrossRef]
- Cunnane, S.C.; Plourde, M.; Pifferi, F.; Bégin, M.; Féart, C.; Barberger-Gateau, P. Fish, docosahexaenoic acid and Alzheimer’s disease. Prog. Lipid Res. 2009, 48, 239–256. [Google Scholar] [CrossRef]
- Parkinson, L.; Keast, R. Oleocanthal, a Phenolic Derived from Virgin Olive Oil: A Review of the Beneficial Effects on Inflammatory Disease. Int. J. Mol. Sci. 2014, 15, 12323–12334. [Google Scholar] [CrossRef]
- Parkinson, L.; Cicerale, S. The Health Benefiting Mechanisms of Virgin Olive Oil Phenolic Compounds. Molecules 2016, 21, 1734. [Google Scholar] [CrossRef]
- Samieri, C.; Jutand, M.-A.; Féart, C.; Capuron, L.; Letenneur, L.; Barberger-Gateau, P. Dietary Patterns Derived by Hybrid Clustering Method in Older People: Association with Cognition, Mood, and Self-Rated Health. J. Am. Diet. Assoc. 2008, 108, 1461–1471. [Google Scholar] [CrossRef]
- Marcason, W. What Are the Components to the MIND Diet? J. Acad. Nutr. Diet. 2015, 115, 1744. [Google Scholar] [CrossRef] [PubMed]
- Féart, C.; Samieri, C.; Rondeau, V.; Amieva, H.; Portet, F.; Dartigues, J.F.; Scarmeas, N.; Barberger-Gateau, P. Adherence to a Mediterranean diet, cognitive decline, and risk of dementia. JAMA 2009, 302, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, C.A.; Yannakoulia, M.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Arampatzi, X.; Bougea, A.; Labropoulos, I.; Scarmeas, N. Mediterranean diet and cognitive health: Initial results from the Hellenic Longitudinal Investigation of Ageing and Diet. PLoS ONE 2017, 12, e0182048. [Google Scholar] [CrossRef]
- Capurso, C.; Bellanti, F.; Buglio, A.L.; Vendemiale, G. The Mediterranean Diet Slows Down the Progression of Aging and Helps to Prevent the Onset of Frailty: A Narrative Review. Nutrients 2019, 12, 35. [Google Scholar] [CrossRef]
- Pelletier, A.; Barul, C.; Féart, C.; Helmer, C.; Bernard, C.; Periot, O.; Dilharreguy, B.; Dartigues, J.; Allard, M.; Barberger-Gateau, P.; et al. Mediterranean diet and preserved brain structural connectivity in older subjects. Alzheimer’s Dement. 2015, 11, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.A. Epigenetics of Mediterranean Diet: Altering Disease Risk. In Mediterranean Diet. Nutrition and Health; Humana Press: Cham, Switzerland, 2016; pp. 203–216. [Google Scholar] [CrossRef]
- Talegawkar, S.A.; Jin, Y.; Simonsick, E.M.; Tucker, K.L.; Ferrucci, L.; Tanaka, T. The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet is associated with physical function and grip strength in older men and women. Am. J. Clin. Nutr. 2022, 115, 625–632. [Google Scholar] [CrossRef]
- Talegawkar, S.A.; Bandinelli, S.; Bandeen-Roche, K.; Chen, P.; Milaneschi, Y.; Tanaka, T.; Semba, R.D.; Guralnik, J.M.; Ferrucci, L. A Higher Adherence to a Mediterranean-Style Diet Is Inversely Associated with the Development of Frailty in Community-Dwelling Elderly Men and Women. J. Nutr. 2012, 142, 2161–2166. [Google Scholar] [CrossRef]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef]
- Abdulrahim, S.; Ajrouch, K.J.; Antonucci, T.C. Aging in Lebanon: Challenges and Opportunities. Gerontol. 2015, 55, 511–518. [Google Scholar] [CrossRef]
- Economic and Social Commission for Western Asia (ESCWA). Ageing in ESCWA Member States: Third Review and Appraisal of the Madrid International Plan of Action on Ageing; ESCWA: Beirut, Lebanon; p. 83.
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2020 Highlights: Living Arrangements of Older Persons; United Nations: New York, NY, USA, 2020.
- Faour, M.A. Religion, demography, and politics in Lebanon. Middle East. Studies 2007, 43, 909–921. [Google Scholar] [CrossRef]
- ESCWA. Launch of the National Strategy for Older Persons in Lebanon 2020–2030. Available online: http://www.unescwa.org/news/launch-national-strategy-older-persons-lebanon-2020-2030 (accessed on 25 October 2021).
- Pruchno, R. International Aging: Spotlighting the Spotlights. Gerontologist 2017, 57, 392–395. [Google Scholar] [CrossRef]
- Darwish, H.; Farran, N.; Assaad, S.; Chaaya, M. Cognitive Reserve Factors in a Developing Country: Education and Occupational Attainment Lower the Risk of Dementia in a Sample of Lebanese Older Adults. Front. Aging Neurosci. 2018, 10, 277. [Google Scholar] [CrossRef] [PubMed]
- Phung, K.T.T.; Chaaya, M.; Prince, M.; Atweh, S.; El Asmar, K.; Karam, G.; Khoury, R.M.; Ghandour, L.; Ghusn, H.; Nielsen, T.R.; et al. Dementia prevalence, care arrangement and access to care in lebnon: A pilot study. Alzheimers Dement. 2017, 13, 1317–1326. [Google Scholar] [CrossRef] [PubMed]
- Assaf, G.; Tanielian, M. Mild cognitive impairment in primary care: A clinical review. Postgrad. Med. J. 2018, 94, 647–652. [Google Scholar] [CrossRef]
- Hayek, M.; Tarabey, L.; Abou-Mrad, T.; Fadel, P.; Abou-Mrad, F. Normative Data for the Montreal Cognitive Assessment in a Lebanese Older Adult Population. J. Clin. Neurosci. 2020, 74, 81–86. [Google Scholar] [CrossRef]
- Boulos, C.; Salameh, P.; Barberger-Gateau, P. Factors associated with poor nutritional status among community dwelling Lebanese elderly subjects living in rural areas: Results of the AMEL study. J. Nutr. Health Aging 2014, 18, 487–494. [Google Scholar] [CrossRef]
- Jomaa, L.; Hwalla, N.; Itani, L.; Chamieh, M.C.; Mehio-Sibai, A.; Naja, F. A Lebanese dietary pattern promotes better diet quality among older adults: Findings from a national cross-sectional study. BMC Geriatr. 2016, 16, 85. [Google Scholar] [CrossRef]
- Yaghi, N.; Yaghi, C.; Abifadel, M.; Boulos, C.; Feart, C. Dietary Patterns and Risk Factors of Frailty in Lebanese Older Adults. Nutrients 2021, 13, 2188. [Google Scholar] [CrossRef]
- El-Hayeck, R.; Baddoura, R.; Wehbé, A.; Bassil, N.; Koussa, S.; Khaled, K.A.; Richa, S.; Khoury, R.; Alameddine, A.; Sellal, F. An Arabic Version of the Mini-Mental State Examination for the Lebanese Population: Reliability, Validity, and Normative Data. J. Alzheimer’s Dis. 2019, 71, 525–540. [Google Scholar] [CrossRef]
- El-Hayeck, R.; Baddoura, R.; Wehbé, A.; Bassil, N.; Koussa, S.; Khaled, K.A.; Richa, S.; Khoury, R.; Alameddine, A.; Sellal, F. An adapted Arabic version of the Test of Nine Images for the illiterate Lebanese population: Validation and preliminary normative data. J. Int. Neuropsychol. Soc. 2023, 29, 316–323. [Google Scholar] [CrossRef]
- Maillet, D.; Matharan, F.; Le Clésiau, H.; Bailon, O.; Pérès, K.; Amieva, H.; Belin, C. TNI-93: A New Memory Test for Dementia Detection in Illiterate and Low-Educated Patients. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2016, 31, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Tavares-Júnior, J.W.L.; de Souza, A.C.C.; Alves, G.S.; Bonfadini, J.d.C.; Siqueira-Neto, J.I.; Braga-Neto, P. Cognitive Assessment Tools for Screening Older Adults with Low Levels of Education: A Critical Review. Front. Psychiatry 2019, 10, 878. [Google Scholar] [CrossRef] [PubMed]
- Hallit, S.; Hallit, R.; Boulos, C.; Hachem, D.; Nasra, M.C.; Kheir, N.; Salameh, P. Validation of the Arabic Geriatric Depression Scale (GDS-5) among the Lebanese Geriatric Population. J. Psychopathol. 2017, 23, 87–90. [Google Scholar]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L.Z. Development and Testing of a Five-Item Version of the Geriatric Depression Scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Guigoz, Y. The mini nutritional assessment (MNA®) review of the literature-what does it tell us? J. Nutr. Health Aging 2006, 10, 466. [Google Scholar]
- Yaghi, N.; Boulos, C.; Baddoura, R.; Abifadel, M.; Yaghi, C. Validity and reliability of a food frequency questionnaire for community dwelling older adults in a Mediterranean country: Lebanon. Nutr. J. 2022, 21, 40. [Google Scholar] [CrossRef]
- Dietary Reference Intakes: The Essential Guide to Nutrient Requirements|The National Academies Press [Internet]. Available online: https://www.nap.edu/download/11537 (accessed on 5 February 2021).
- Harada, C.N.; Natelson Love, M.C.N.; Triebel, K.L. Normal Cognitive Aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef]
- Au, B.; Dale-McGrath, S.; Tierney, M.C. Sex differences in the prevalence and incidence of mild cognitive impairment: A meta-analysis. Ageing Res Rev. 2017, 35, 176–199. [Google Scholar] [CrossRef]
- Miquel, S.; Champ, C.; Day, J.; Aarts, E.; Bahr, B.A.; Bakker, M.; Bánáti, D.; Calabrese, V.; Cederholm, T.; Cryan, J. Poor cognitive ageing: Vulnerabilities, mechanisms and the impact of nutritional interventions. Ageing Res. Rev. 2018, 42, 40–55. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. Cognitive Reserve: Implications for Assessment and Intervention. Folia Phoniatr. et Logop. 2013, 65, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-R.; Xu, W.; Zhang, W.; Wang, H.-F.; Ou, Y.-N.; Qu, Y.; Shen, X.-N.; Chen, S.-D.; Wu, K.-M.; Zhao, Q.-H.; et al. Modifiable risk factors for incident dementia and cognitive impairment: An umbrella review of evidence. J. Affect. Disord. 2022, 314, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, J.S.; Zuidersma, M.; Zuidema, S.U.; Burgerhof, J.G.; Stolk, R.P.; Oude Voshaar, R.C.; Smidt, N. Social relationships and cognitive decline: A systematic review and meta-analysis of longitudinal cohort studies. Int. J. Epidemiol. 2016, 45, 1169–1206. [Google Scholar] [CrossRef]
- Marseglia, A.; Darin-Mattsson, A.; Skoog, J.; Rydén, L.; Hadarsson-Bodin, T.; Kern, S.; Sterner, T.R.; Shang, Y.; Zettergren, A.; Westman, E.; et al. Metabolic Syndrome Is Associated With Poor Cognition: A Population-Based Study of 70-Year-Old Adults Without Dementia. J. Gerontol. Ser. A 2021, 76, 2275–2283. [Google Scholar] [CrossRef] [PubMed]
- Chye, L.; Wei, K.; Nyunt, M.S.Z.; Gao, Q.; Wee, S.L.; Ng, T.-P. Strong Relationship Between Malnutrition And Cognitive Frailty In The Singapore Longitudinal Ageing Studies (SLAS-1 and SLAS-2). J. Prev. Alzheimer’s Dis. 2018, 5, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Chu, Z.; Quan, X.; Zhang, Y.; Yuan, W.; Yao, Y.; Zhao, Y.; Fu, S. Malnutrition is positively associated with cognitive decline in centenarians and oldest-old adults: A cross-sectional study. EClinicalMedicine 2022, 47, 101336. [Google Scholar] [CrossRef]
- Flicker, L. Cardiovascular Risk Factors, Cerebrovascular Disease Burden, and Healthy Brain Aging. Clin. Geriatr. Med. 2010, 26, 17–27. [Google Scholar] [CrossRef]
- Hajjar, I.; Quach, L.; Yang, F.; Chaves, P.H.; Newman, A.B.; Mukamal, K.; Longstreth, W., Jr.; Inzitari, M.; Lipsitz, L.A. Hypertension, white matter hyperintensities, and concurrent impairments in mobility, cognition, and mood: The Cardiovascular Health Study. Circulation 2011, 123, 858–865. [Google Scholar] [CrossRef]
- Wei, M.Y.; Levine, D.A.; Zahodne, L.B.; Kabeto, M.U.; Langa, K.M. Multimorbidity and Cognitive Decline Over 14 Years in Older Americans. J. Gerontol. Ser. A 2019, 75, 1206–1213. [Google Scholar] [CrossRef]
- Smith, A.D.; Smith, S.M.; de Jager, C.A.; Whitbread, P.; Johnston, C.; Agacinski, G.; Oulhaj, A.; Bradley, K.M.; Jacoby, R.; Refsum, H. Homocysteine-Lowering by B Vitamins Slows the Rate of Accelerated Brain Atrophy in Mild Cognitive Impairment: A Randomized Controlled Trial. PLoS ONE 2010, 8, e12244. [Google Scholar] [CrossRef]
- Robbins, R.N.; Scott, T.; Joska, J.A.; Gouse, H. Impact of urbanization on cognitive disorders. Curr. Opin. Psychiatry 2019, 32, 210–217. [Google Scholar] [CrossRef]
- Lehmann, M.; Regland, B.; Blennow, K.; Gottfries, C. Vitamin B12-B6-Folate Treatment Improves Blood-Brain Barrier Function in Patients with Hyperhomocysteinaemia and Mild Cognitive Impairment. Dement. Geriatr. Cogn. Disord. 2003, 16, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Merle, B.M.J.; Delyfer, M.-N.; Korobelnik, J.-F.; Rougier, M.-B.; Malet, F.; Féart, C.; Le Goff, M.; Peuchant, E.; Letenneur, L.; Dartigues, J.-F.; et al. High Concentrations of Plasma n3 Fatty Acids Are Associated with Decreased Risk for Late Age-Related Macular Degeneration. J. Nutr. 2013, 143, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Wang, S.; Gao, F.; Li, C. Vitamin B6, B9, and B12 Intakes and Cognitive Performance in Elders: National Health and Nutrition Examination Survey, 2011–2014. Neuropsychiatr. Dis. Treat. 2022, 18, 537–553. [Google Scholar] [CrossRef]
- Xu, Q.; Zhang, S.; Gu, Y.; Wang, P.; Zhang, Q.; Shan, C. Interaction of High-Sugar Diet and History of Stroke with Risk of Cognitive Decline in Older Adults. Experiment 2022, 28, e937572. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Gao, X.; Scott, T.; Tucker, K.L. Habitual sugar intake and cognitive function among middle-aged and older Puerto Ricans without diabetes. Br. J. Nutr. 2011, 106, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.-Q.; Yu, L.-L.; Qi, G.-Y.; Mi, Y.-S.; Wu, W.-Q.; Lee, Y.-K.; Zhai, Q.-X.; Tian, F.-W.; Chen, W. Can dietary patterns prevent cognitive impairment and reduce Alzheimer’s disease risk: Exploring the underlying mechanisms of effects. Neurosci. Biobehav. Rev. 2022, 135, 104556. [Google Scholar] [CrossRef]
- Feart, C.; Samieri, C.; Barberger-Gateau, P. Mediterranean diet and cognitive health: An update of available knowledge. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 51–62. [Google Scholar] [CrossRef]
- Gu, Y.; Brickman, A.M.; Stern, Y.; Habeck, C.G.; Razlighi, Q.R.; Luchsinger, J.A.; Manly, J.J.; Schupf, N.; Mayeux, R.; Scarmeas, N. Mediterranean diet and brain structure in a multiethnic elderly cohort. Neurology 2015, 85, 1744–1751. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Vernuccio, L.; Catanese, G.; Inzerillo, F.; Salemi, G.; Barbagallo, M. Nutrition, Physical Activity, and Other Lifestyle Factors in the Prevention of Cognitive Decline and Dementia. Nutrients 2021, 13, 4080. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef]
- Gu, Y.; Manly, J.J.; Mayeux, R.P.; Brickman, A.M. An Inflammation-related Nutrient Pattern is Associated with Both Brain and Cognitive Measures in a Multiethnic Elderly Population. Curr. Alzheimer Res. 2018, 15, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Misirli, G.; Benetou, V.; Lagiou, P.; Bamia, C.; Trichopoulos, D.; Trichopoulou, A. Relation of the Traditional Mediterranean Diet to Cerebrovascular Disease in a Mediterranean Population. Am. J. Epidemiol. 2012, 176, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Shivappa, N.; Nasreddine, L.; Kharroubi, S.; Itani, L.; Hwalla, N.; Sibai, A.M.; Hebert, J.R. Role of inflammation in the association between the western dietary pattern and metabolic syndrome among Lebanese adults. Int. J. Food Sci. Nutr. 2017, 68, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Shakersain, B.; Santoni, G.; Larsson, S.C.; Faxén-Irving, G.; Fastbom, J.; Fratiglioni, L.; Xu, W. Prudent diet may attenuate the adverse effects of Western diet on cognitive decline. Alzheimer’s Dement. 2016, 12, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; van Kan, G.A.; Ousset, P.-J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) International Consensus Group. J. Nutr. Heal. Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Mantovani, E.; Zucchella, C.; Schena, F.; Romanelli, M.G.; Venturelli, M.; Tamburin, S. Towards a Redefinition of Cognitive Frailty. J. Alzheimer’s Dis. 2020, 76, 831–843. [Google Scholar] [CrossRef]
- Sugimoto, T.; Arai, H.; Sakurai, T. An update on cognitive frailty: Its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatr. Gerontol. Int. 2022, 22, 99–109. [Google Scholar] [CrossRef]


{kind=link}
| Literate 248 (70.5) | Illiterate 104 (29.5) | ||||||
|---|---|---|---|---|---|---|---|
| GCS 167 (67.3) | CI 81 (32.7) | p-Value | GCS 40 (38.5) | CI 64 (61.5) | p-Value | ||
| Age (y) | 72 ± 7 (72) | 73 ± 9 (72) | 0.414 | 73.8 ± 6.4 (74) | 77 ± 7 (77) | 0.038 | |
| ≥80 | 21 (12.6) | 22 (27.2) | 0.004 | 4 (10) | 20 (31.2) | 0.012 | |
| Gender | Men | 90 (53.9) | 48 (59.3) | 0.425 | 14 (35) | 24 (37.5) | 0.797 |
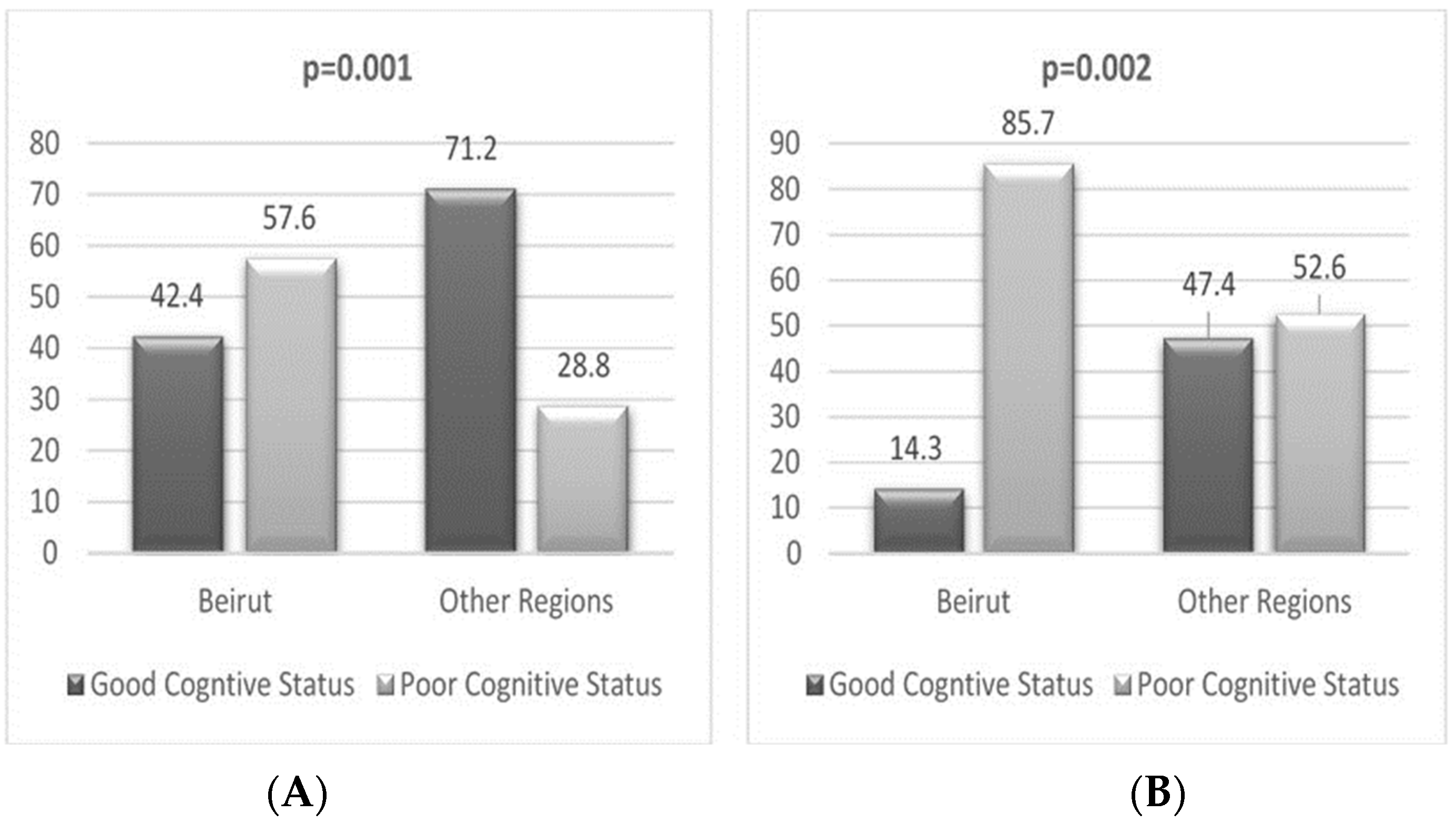
| Regions | Beirut | 14 (42.4) | 19 (57.6) | 0.001 | 4 (14.3) | 24 (85.7) | 0.002 |
| Other regions | 153 (71.2) | 62 (28.8) | 36 (47.4) | 40 (52.6) | |||
| Education | Less than elementary | 36 (21.6) | 6 (7.4) | 0.018 | |||
| Elementary | 44 (26.3) | 36 (44.4) | |||||
| Complementary | 32 (19.2) | 14 (17.3) | |||||
| Baccalaureate | 25 (15) | 15 (18.5) | |||||
| higher education | 28 (16.8) | 9 (11.1) | |||||
| Income | Insufficient | 84 (50.3) | 43 (53.1) | 0.68 | 26 (65) | 45 (70.3) | 0.571 |
| Marital status | Married | 117 (70.1) | 56 (69.1) | 0.822 | 19 (47.5) | 40 (62.5) | 0.372 |
| Divorced | 5 (3) | 1 (1.2) | 1 (2.5) | 3 (4.7) | |||
| Single | 10 (6) | 6 (7.4) | 1 (2.5) | 1 (1.6) | |||
| Widowed | 35 (21) | 18 (22.2) | 19 (47.5) | 20 (31.2) | |||
| Literate 248 (70.5) | Illiterate 104 (29.5) | ||||||
|---|---|---|---|---|---|---|---|
| GCS 167 (67.3) | CI 81 (32.7) | p-Value | GCS 40 (38.5) | CI 64 (61.5) | p-Value | ||
| Health and Functional Parameters | |||||||
| HGS (kg) | 26.2 ± 9.3 (25.6) | 26.4 ± 9.1 (23.9) | 0.874 | 22.3 ± 9 (19.7) | 18.4 ± 7.6 (17.9) | 0.026 | |
| Low HGS | 68 (43.3) | 33 (45.2) | 0.788 | 21 (52.5) | 49 (77.8) | 0.007 | |
| Physical Activity | Sedentary | 132 (79) | 58 (71.6) | 0.3 | 33 (82.5) | 52 (81.3) | 0.91 |
| Regular active | 34 (20.4) | 23 (28.4) | 6 (15) | 11 (17.2) | |||
| Optimal active | 1 (0.6) | 0 (0) | 1 (2.5) | 1 (1.6) | |||
| Poor mental health | 70 (41.9) | 44 (55) | 0.054 | 23 (65) | 46 (71.9) | 0.460 | |
| Multi-morbidity | >1 disease | 120 (72.3) | 59 (72.8) | 0.928 | 35 (87.5) | 56 (87.5) | 1 |
| Age-related conditions | >1 condition | 73 (43.7) | 39 (48.1) | 0.51 | 28 (70) | 49 (76.6) | 0.458 |
| Polypharmacy | 41 (24.7) | 16 (20.5) | 0.471 | 25 (62.5) | 42 (70) | 0.435 | |
| Frailty | 10 (6) | 15 (18.5) | 0.002 | 9 (22.5) | 19 (29.7) | 0.421 | |
| Smoker | never | 82 (49.1) | 40 (49.4) | 0.999 | 13 (32.5) | 31 (48.4) | 0.237 |
| present | 52 (31.1) | 25 (30.9) | 19 (47.5) | 21 (32.8) | |||
| previous | 33 (19.8) | 16 (19.8) | 8 (20) | 12 (18.8) | |||
| Family history of CD | 33 (19.8) | 14 (17.3) | 0.641 | 10 (19.6) | 12 (22.6) | 0.448 | |
| Nutritional status parameters | |||||||
| Nutritional status | Malnutrition | 3 (1.8) | 8 (9.9) | 0.004 | 2 (5) | 6 (9.4) | 0.415 |
| BMI (kg/m2) | 29.4 ± 5.6 (28.8) | 27.9 ± 4.9 (27.4) | 0.035 | 29.3 ± 6 (28.3) | 30.28 ± 7.1 (28.2) | 0.923 | |
| <22 | 46 (27.5) | 33 (40.7) | 0.111 | 9 (22.5) | 21 (32.8) | 0.774 | |
| 22–27 | 14 (8.4) | 6 (7.4) | 5 (12.5) | 5 (7.8) | |||
| >27 | 107 (64.1) | 42 (51.9) | 26 (65) | 38 (59.4) | |||
| Model 1 | p-Value | Model 2 | p-Value | Model 3 | p-Value | |
|---|---|---|---|---|---|---|
| Socio-demographic parameters | ||||||
| Age ≥ cut-offs * | 4.6 (2.48–8.54) | <0.001 | 3.32 (1.84–5.96) | <0.001 | 3.7 (2.1–6.55) | <0.001 |
| Living in Beirut | 4.6 (2.48–8.54) | <0.001 | 4.26 (2.18–8.3) | <0.001 | 4.51 (2.37–8.61) | <0.001 |
| Anthropometric and health-related parameters | ||||||
| Frailty | 2.24 (1.12–4.49) | 0.022 | ||||
| Health perception | 1.69 (1.01–2.82) | 0.044 | 2.01 (1.24–3.26) | 0.005 | ||
| Dietary patterns | ||||||
| MOD-MEDDP | 1 | 0.033 | ||||
| WDP | 2.04 (0.98–4.25) | 0.058 | ||||
| HI-MEDDP | 1.87 (1.07–3.29) | 0.029 | ||||
| Model 1 | p-Value | Model 2 | p-Value | Model 3 | p-Value | |
|---|---|---|---|---|---|---|
| Socio-demographic parameters | ||||||
| Age > 80 years | 2.89 (1.46–5.76) | 0.002 | 2.49 (1.14–5.42) | <0.001 | 2.24 (1.07–4.71) | 0.033 |
| Living in Beirut | 3.73 (1.73–8.04) | 0.001 | 2.25 (1.09–4.63) | 0.027 | 5.21 (2.26–11.99) | <0.001 |
| Anthropometric and health-related parameters | ||||||
| Frailty | 3.74 (1.49–9.42) | 0.005 | 4.3 (1.66–11.14) | 0.002 | ||
| Dietary patterns | ||||||
| MOD-MEDDP | 1 | 0.018 | ||||
| WDP | 3.08 (1.22–7.8) | 0.017 | ||||
| HI-MEDDP | 2.11 (1.05–4.22) | 0.035 | ||||
| Model 1 | p-Value | Model 2 | p-Value | Model 3 | p-Value | |
|---|---|---|---|---|---|---|
| Age > 78 years | 5.84 (1.9–17.92) | 0.002 | 5.39 (1.79–16.26) | 0.003 | 5.08 (1.71–15.07) | 0.003 |
| Living in Beirut | 6.59 (1.76–24.73) | 0.005 | 5.4 (1.51–19.26) | 0.009 | 5.85 (1.66–20.62) | 0.006 |
| Living conditions (compared with living alone) | 0.007 | 0.025 | 0.019 | |||
| Living with partner | 6.12 (1.63–22.93) | 0.007 | 4.04 (1.2–13.62) | 0.025 | 4.13 (1.25–13.63) | 0.020 |
| Living with others | 1.03 (0.3–3.52) | 0.963 | 1.07 (0.31–3.67) | 0.913 | 1.08 (0.33–3.61) | 0.896 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yaghi, N.; El Hayeck, R.; Boulos, C.; Abifadel, M.; Yaghi, C. Effect of Mediterranean Dietary Pattern on Cognitive Status in Community-Dwelling Older Adults. Nutrients 2023, 15, 3911. https://doi.org/10.3390/nu15183911
Yaghi N, El Hayeck R, Boulos C, Abifadel M, Yaghi C. Effect of Mediterranean Dietary Pattern on Cognitive Status in Community-Dwelling Older Adults. Nutrients. 2023; 15(18):3911. https://doi.org/10.3390/nu15183911
Chicago/Turabian StyleYaghi, Nathalie, Rita El Hayeck, Christa Boulos, Marianne Abifadel, and César Yaghi. 2023. "Effect of Mediterranean Dietary Pattern on Cognitive Status in Community-Dwelling Older Adults" Nutrients 15, no. 18: 3911. https://doi.org/10.3390/nu15183911