
Stem of Sorbus commixta Hedl. Extract Inhibits Cartilage Degradation and Arthritic Pain in Experimental Model via Anti-Inflammatory Activity


Abstract
:1. Introduction
2. Materials and Methods
2.1. Material Preparation
2.2. Data Sources and Search Strategy High Performance Liquid Chromatography (HPLC) Analysis
2.3. Animal
2.4. OA Induction and Diet Preparation
2.5. Serum Measurement of OA Induction in MIA Rats
2.6. Weight-Bearing Analysis
2.7. Writhing Response Induced by Acetic Acid (AA)
2.8. Cell Culture
2.9. Generation of NO and Cell Toxicity Evaluation
2.10. Quantitative Real-Time Polymerase Chain Reaction (qRT-PCR)
2.11. Western Blot
2.12. Statistics
3. Results
3.1. HPLC Analysis
3.2. Effects on Weight-Bearing Arrangement in OA-Induction MIA Rats
3.3. Effects on Knee Joint Damage in OA-Induction MIA Rats
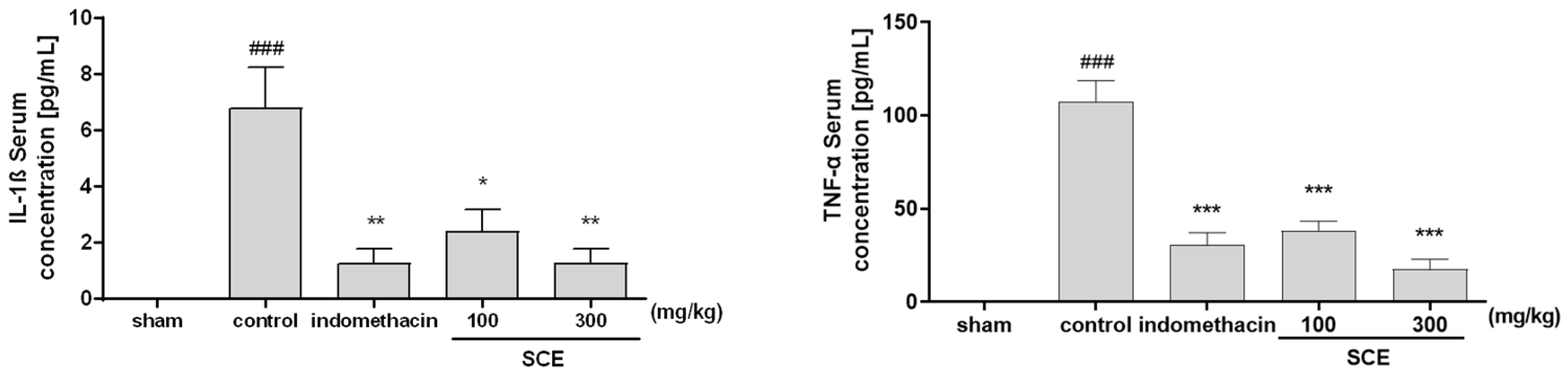
3.4. Effects on Inflammatory Cytokines in OA-Induction MIA Rats
3.5. Effect on Acetic Acid-Induced(AA) Writhing Responses
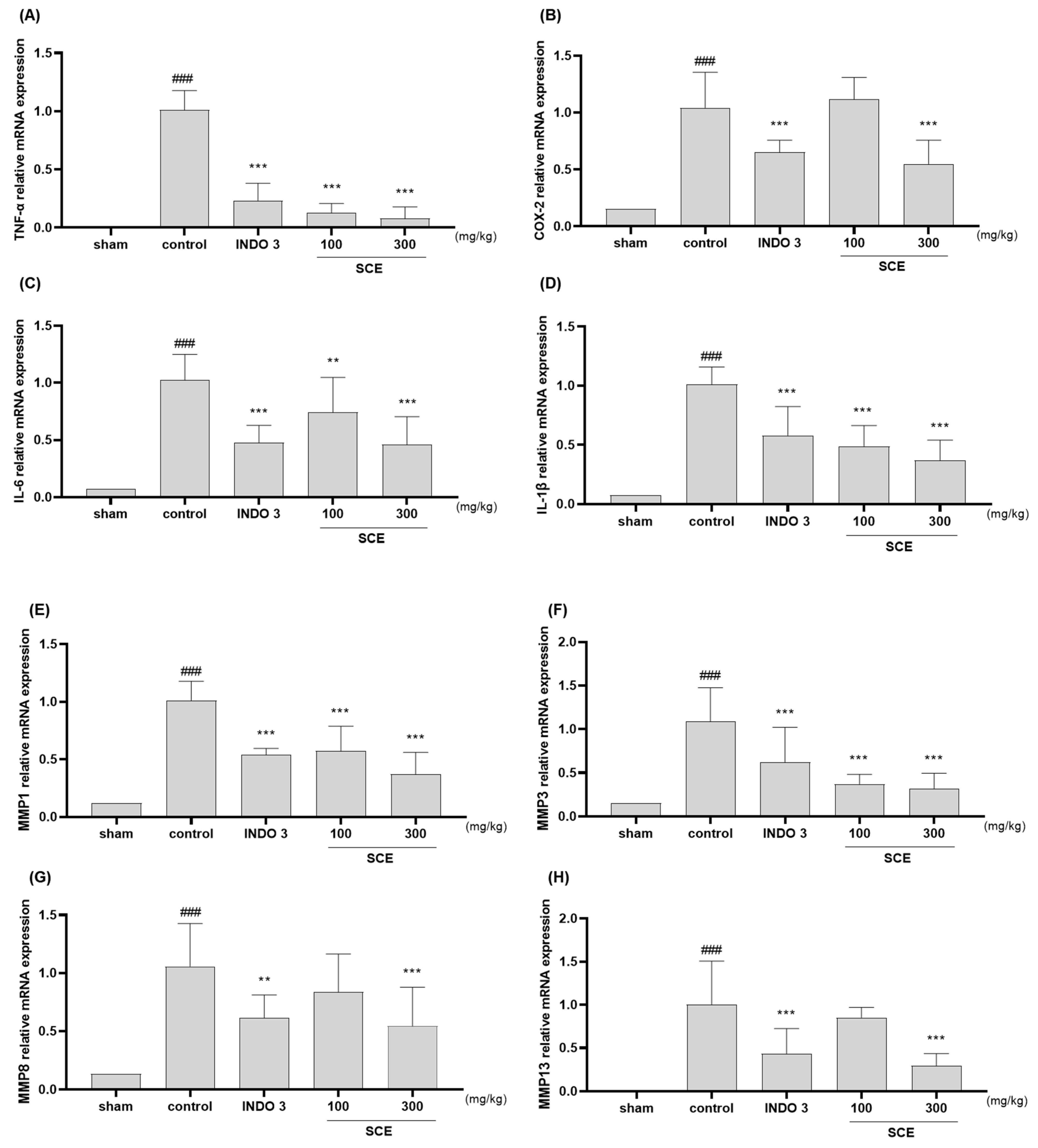
3.6. Effects on Cytokines Responses in Cartilage Tissue
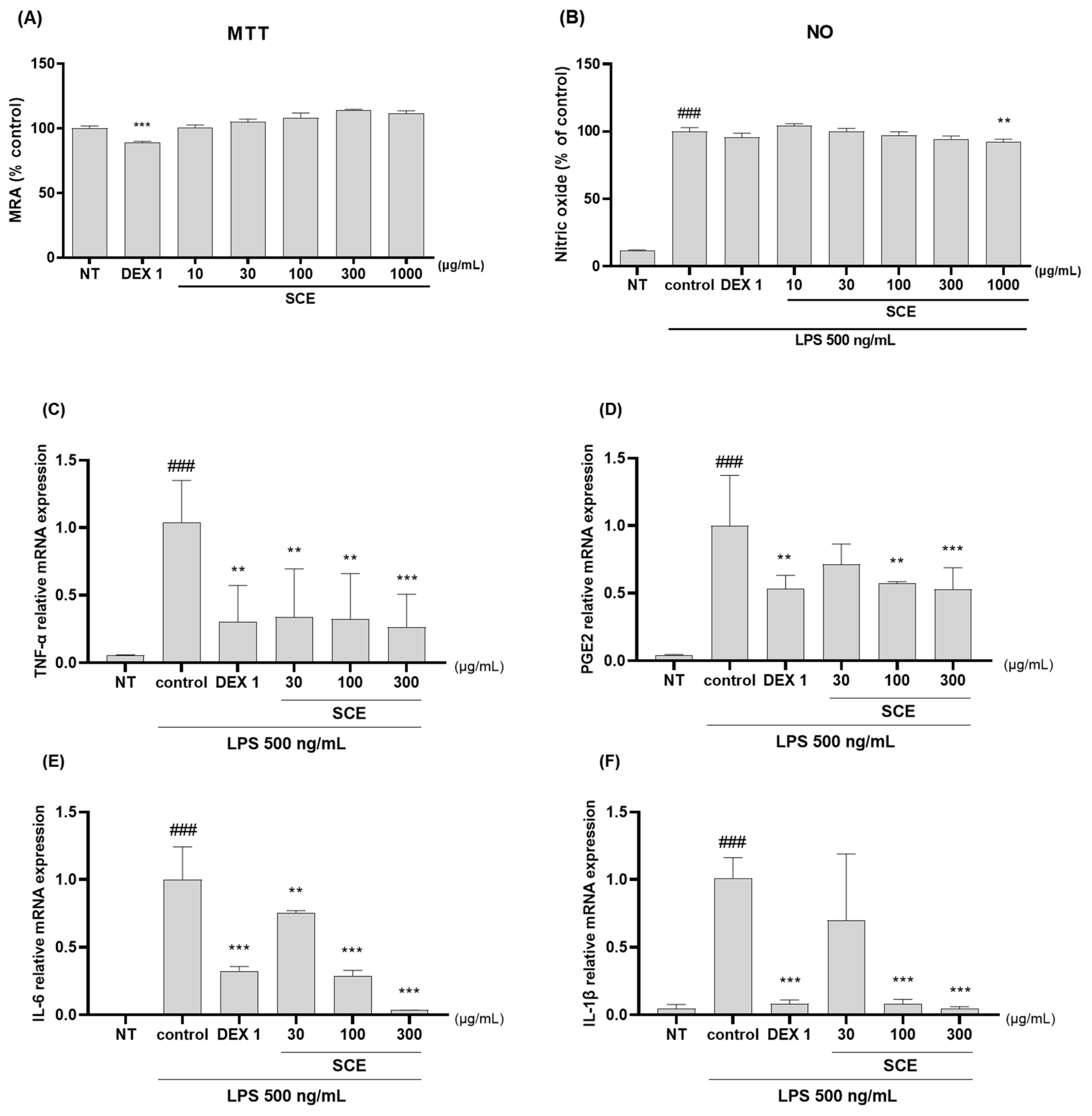
3.7. Effects on Anti-Inflammatory in the LPS-Activated RAW264.7 Cells
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Pigeolet, M.; Jayaram, A.; Park, K.B.; Meara, J.G. Osteoarthritis in 2020 and Beyond. Lancet 2021, 397, 1059–1060. [Google Scholar] [CrossRef]
- Mahmoudian, A.; Lohmander, L.S.; Mobasheri, A.; Englund, M.; Luyten, F.P. Early-Stage Symptomatic Osteoarthritis of the Knee—Time for Action. Nat. Rev. Rheumatol. 2021, 17, 621–632. [Google Scholar] [CrossRef] [PubMed]
- Tong, L.; Yu, H.; Huang, X.; Shen, J.; Xiao, G.; Chen, L.; Wang, H.; Xing, L.; Chen, D. Current Understanding of Osteoarthritis Pathogenesis and Relevant New Approaches. Bone Res. 2022, 10, 60. [Google Scholar] [CrossRef]
- Yang, G.; Wang, J.; Liu, Y.; Lu, H.; He, L.; Ma, C.; Zhao, Z. Burden of Knee Osteoarthritis in 204 Countries and Territories, 1990-2019: Results from the Global Burden of Disease Study 2019. Arthritis Care Res. 2023. [Google Scholar] [CrossRef] [PubMed]
- Leifer, V.P.; Katz, J.N.; Losina, E. The Burden of OA-Health Services and Economics. Osteoarthr. Cartil. 2022, 30, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Leopoldino, A.O.; Machado, G.C.; Ferreira, P.H.; Pinheiro, M.B.; Day, R.; McLachlan, A.J.; Hunter, D.J.; Ferreira, M.L. Paracetamol versus Placebo for Knee and Hip Osteoarthritis. Cochrane Database Syst. Rev. 2019, 2, CD013273. [Google Scholar] [CrossRef]
- Weng, Q.; Goh, S.-L.; Wu, J.; Persson, M.S.M.; Wei, J.; Sarmanova, A.; Li, X.; Hall, M.; Doherty, M.; Jiang, T.; et al. Comparative Efficacy of Exercise Therapy and Oral Non-Steroidal Anti-Inflammatory Drugs and Paracetamol for Knee or Hip Osteoarthritis: A Network Meta-Analysis of Randomised Controlled Trials. Br. J. Sports Med. 2023, 57, 990–996. [Google Scholar] [CrossRef]
- Gregori, D.; Giacovelli, G.; Minto, C.; Barbetta, B.; Gualtieri, F.; Azzolina, D.; Vaghi, P.; Rovati, L.C. Association of Pharmacological Treatments With Long-Term Pain Control in Patients With Knee Osteoarthritis: A Systematic Review and Meta-Analysis. JAMA 2018, 320, 2564–2579. [Google Scholar] [CrossRef] [PubMed]
- Roberts, E.; Delgado Nunes, V.; Buckner, S.; Latchem, S.; Constanti, M.; Miller, P.; Doherty, M.; Zhang, W.; Birrell, F.; Porcheret, M.; et al. Paracetamol: Not as Safe as We Thought? A Systematic Literature Review of Observational Studies. Ann. Rheum. Dis. 2016, 75, 552–559. [Google Scholar] [CrossRef]
- Zádori, Z.S.; Király, K.; Al-Khrasani, M.; Gyires, K. Interactions between NSAIDs, Opioids and the Gut Microbiota—Future Perspectives in the Management of Inflammation and Pain. Pharmacol. Ther. 2023, 241, 108327. [Google Scholar] [CrossRef]
- Sanchez-Lopez, E.; Coras, R.; Torres, A.; Lane, N.E.; Guma, M. Synovial Inflammation in Osteoarthritis Progression. Nat. Rev. Rheumatol. 2022, 18, 258–275. [Google Scholar] [CrossRef] [PubMed]
- Knights, A.J.; Redding, S.J.; Maerz, T. Inflammation in Osteoarthritis: The Latest Progress and Ongoing Challenges. Curr. Opin Rheumatol. 2023, 35, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Arra, M.; Abu-Amer, Y. Cross-Talk of Inflammation and Chondrocyte Intracellular Metabolism in Osteoarthritis. Osteoarthr. Cartil. 2023, 31, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Oo, W.M. Prospects of Disease-Modifying Osteoarthritis Drugs. Clin. Geriatr. Med. 2022, 38, 397–432. [Google Scholar] [CrossRef] [PubMed]
- Vincent, T.L. Of Mice and Men: Converging on a Common Molecular Understanding of Osteoarthritis. Lancet Rheumatol. 2020, 2, e633–e645. [Google Scholar] [CrossRef]
- Hadzic, E.; Beier, F. Emerging Therapeutic Targets for Osteoarthritis. Expert Opin. Ther. Targets 2023, 27, 111–120. [Google Scholar] [CrossRef]
- Luo, Y.; Wang, C.-Z.; Sawadogo, R.; Tan, T.; Yuan, C.-S. Effects of Herbal Medicines on Pain Management. Am. J. Chin. Med. 2020, 48, 1–16. [Google Scholar] [CrossRef]
- Yang, M.; Jiang, L.; Wang, Q.; Chen, H.; Xu, G. Traditional Chinese Medicine for Knee Osteoarthritis: An Overview of Systematic Review. PLoS ONE 2017, 12, e0189884. [Google Scholar] [CrossRef] [PubMed]
- Jo, H.-G.; Baek, E.; Lee, D. Comparative Efficacy of East Asian Herbal Formulae Containing Astragali Radix-Cinnamomi Ramulus Herb-Pair against Diabetic Peripheral Neuropathy and Mechanism Prediction: A Bayesian Network Meta-Analysis Integrated with Network Pharmacology. Pharmaceutics 2023, 15, 1361. [Google Scholar] [CrossRef]
- Ren, J.-L.; Yang, L.; Qiu, S.; Zhang, A.-H.; Wang, X.-J. Efficacy Evaluation, Active Ingredients, and Multitarget Exploration of Herbal Medicine. Trends Endocrinol. Metab. 2023, 34, 146–157. [Google Scholar] [CrossRef]
- Jo, H.-G.; Seo, J.; Choi, S.; Lee, D. East Asian Herbal Medicine to Reduce Primary Pain and Adverse Events in Cancer Patients: A Systematic Review and Meta-Analysis With Association Rule Mining to Identify Core Herb Combination. Front. Pharmacol. 2021, 12, 800571. [Google Scholar] [CrossRef]
- Panossian, A. Challenges in Phytotherapy Research. Front. Pharmacol. 2023, 14, 1199516. [Google Scholar] [CrossRef]
- Li, X.-Z.; Zhang, S.-N. Recent Advance in Treatment of Osteoarthritis by Bioactive Components from Herbal Medicine. Chin. Med. 2020, 15, 80. [Google Scholar] [CrossRef]
- Jo, H.-G.; Seo, J.; Lee, D. Clinical Evidence Construction of East Asian Herbal Medicine for Inflammatory Pain in Rheumatoid Arthritis Based on Integrative Data Mining Approach. Pharmacol. Res. 2022, 185, 106460. [Google Scholar] [CrossRef]
- Wang, M.; Liu, L.; Zhang, C.S.; Liao, Z.; Jing, X.; Fishers, M.; Zhao, L.; Xu, X.; Li, B. Mechanism of Traditional Chinese Medicine in Treating Knee Osteoarthritis. J. Pain Res. 2020, 13, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Li, K.; Kamali, A.; Ziadlou, R.; Ahmad, P.; Wang, X.; Richards, R.G.; Alini, M.; Basoli, V.; Li, Z.; et al. Small Molecules of Herbal Origin for Osteoarthritis Treatment: In Vitro and In Vivo Evidence. Arthritis Res. Ther. 2022, 24, 105. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Xu, Y.; Zhu, Y.; Ye, H.; Wang, Q.; Xu, G. Efficacy and Safety of Chinese Herbal Medicine for Knee Osteoarthritis: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phytomedicine 2022, 100, 154029. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Efferth, T.; Hua, X.; Zhang, X.-A. Medicinal Plants and Their Secondary Metabolites in Alleviating Knee Osteoarthritis: A Systematic Review. Phytomedicine 2022, 105, 154347. [Google Scholar] [CrossRef]
- Li, W.; Yu, L.; Li, W.; Ge, G.; Ma, Y.; Xiao, L.; Qiao, Y.; Huang, W.; Huang, W.; Wei, M.; et al. Prevention and Treatment of Inflammatory Arthritis with Traditional Chinese Medicine: Underlying Mechanisms Based on Cell and Molecular Targets. Ageing Res. Rev. 2023, 89, 101981. [Google Scholar] [CrossRef]
- Yu, T.; Lee, Y.J.; Jang, H.-J.; Kim, A.R.; Hong, S.; Kim, T.W.; Kim, M.-Y.; Lee, J.; Lee, Y.G.; Cho, J.Y. Anti-Inflammatory Activity of Sorbus Commixta Water Extract and Its Molecular Inhibitory Mechanism. J. Ethnopharmacol. 2011, 134, 493–500. [Google Scholar] [CrossRef]
- Bae, J.-T.; Sim, G.-S.; Kim, J.-H.; Pyo, H.-B.; Yun, J.-W.; Lee, B.-C. Antioxidative Activity of the Hydrolytic Enzyme Treated Sorbus Commixta Hedl. and Its Inhibitory Effect on Matrix Metalloproteinase-1 in UV Irradiated Human Dermal Fibroblasts. Arch. Pharm. Res. 2007, 30, 1116–1123. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; An, H.-J. β-Sitosteryl-3-O-β-Glucopyranoside Isolated from the Bark of Sorbus Commixta Ameliorates pro-Inflammatory Mediators in RAW 264.7 Macrophages. Immunopharmacol. Immunotoxicol. 2014, 36, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Im, N.K.; Lee, D.-S.; Lee, S.-R.; Jeong, G.S. Lupeol Isolated from Sorbus Commixta Suppresses 1α,25-(OH)2D3-Mediated Osteoclast Differentiation and Bone Loss in Vitro and in Vivo. J. Nat. Prod. 2016, 79, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Tudorachi, N.B.; Totu, E.E.; Fifere, A.; Ardeleanu, V.; Mocanu, V.; Mircea, C.; Isildak, I.; Smilkov, K.; Cărăuşu, E.M. The Implication of Reactive Oxygen Species and Antioxidants in Knee Osteoarthritis. Antioxidants 2021, 10, 985. [Google Scholar] [CrossRef]
- Nejadhosseinian, M.; Djalalinia, S.; Haerian, H.; Alikhani, M.; Mansour, A.; Mousavian, A.-H.; Mardani-Fard, H.A.; Kasaeian, A.; Faezi, S.T. The Effects of Antioxidants on Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 1026450. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- De Roover, A.; Escribano-Núñez, A.; Monteagudo, S.; Lories, R. Fundamentals of Osteoarthritis: Inflammatory Mediators in Osteoarthritis. Osteoarthr. Cartil. 2023. [Google Scholar] [CrossRef]
- Conaghan, P.G.; Cook, A.D.; Hamilton, J.A.; Tak, P.P. Therapeutic Options for Targeting Inflammatory Osteoarthritis Pain. Nat. Rev. Rheumatol. 2019, 15, 355–363. [Google Scholar] [CrossRef]
- Latourte, A.; Kloppenburg, M.; Richette, P. Emerging Pharmaceutical Therapies for Osteoarthritis. Nat. Rev. Rheumatol. 2020, 16, 673–688. [Google Scholar] [CrossRef]
- Yu, H.; Huang, T.; Lu, W.W.; Tong, L.; Chen, D. Osteoarthritis Pain. Int. J. Mol. Sci. 2022, 23, 4642. [Google Scholar] [CrossRef]
- Jenei-Lanzl, Z.; Meurer, A.; Zaucke, F. Interleukin-1β Signaling in Osteoarthritis—Chondrocytes in Focus. Cell Signal. 2019, 53, 212–223. [Google Scholar] [CrossRef]
- Kusakabe, T.; Sawaji, Y.; Endo, K.; Suzuki, H.; Konishi, T.; Maekawa, A.; Murata, K.; Yamamoto, K. DUSP-1 Induced by PGE2 and PGE1 Attenuates IL-1β-Activated MAPK Signaling, Leading to Suppression of NGF Expression in Human Intervertebral Disc Cells. Int. J. Mol. Sci. 2021, 23, 371. [Google Scholar] [CrossRef]
- Li, L.; Li, Z.; Li, Y.; Hu, X.; Zhang, Y.; Fan, P. Profiling of Inflammatory Mediators in the Synovial Fluid Related to Pain in Knee Osteoarthritis. BMC Musculoskelet. Disord. 2020, 21, 99. [Google Scholar] [CrossRef]
- Eitner, A.; Hofmann, G.O.; Schaible, H.-G. Mechanisms of Osteoarthritic Pain. Studies in Humans and Experimental Models. Front. Mol. Neurosci. 2017, 10, 349. [Google Scholar] [CrossRef]
- Leung, Y.Y.; Huebner, J.L.; Haaland, B.; Wong, S.B.S.; Kraus, V.B. Synovial Fluid Pro-Inflammatory Profile Differs According to the Characteristics of Knee Pain. Osteoarthr. Cartil. 2017, 25, 1420–1427. [Google Scholar] [CrossRef]
- Latourte, A.; Cherifi, C.; Maillet, J.; Ea, H.-K.; Bouaziz, W.; Funck-Brentano, T.; Cohen-Solal, M.; Hay, E.; Richette, P. Systemic Inhibition of IL-6/Stat3 Signalling Protects against Experimental Osteoarthritis. Ann. Rheum. Dis. 2017, 76, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Grillet, B.; Pereira, R.V.S.; Van Damme, J.; Abu El-Asrar, A.; Proost, P.; Opdenakker, G. Matrix Metalloproteinases in Arthritis: Towards Precision Medicine. Nat. Rev. Rheumatol. 2023, 19, 363–377. [Google Scholar] [CrossRef]
- Huang, X.; Xi, Y.; Pan, Q.; Mao, Z.; Zhang, R.; Ma, X.; You, H. Caffeic Acid Protects against IL-1β-Induced Inflammatory Responses and Cartilage Degradation in Articular Chondrocytes. Biomed. Pharmacother. 2018, 107, 433–439. [Google Scholar] [CrossRef]
- Sun, W.; Xie, W.; Huang, D.; Cui, Y.; Yue, J.; He, Q.; Jiang, L.; Xiong, J.; Sun, W.; Yi, Q. Caffeic Acid Phenethyl Ester Attenuates Osteoarthritis Progression by Activating NRF2/HO-1 and Inhibiting the NF-κB Signaling Pathway. Int. J. Mol. Med. 2022, 50, 134. [Google Scholar] [CrossRef] [PubMed]
- de Almeida, L.G.N.; Thode, H.; Eslambolchi, Y.; Chopra, S.; Young, D.; Gill, S.; Devel, L.; Dufour, A. Matrix Metalloproteinases: From Molecular Mechanisms to Physiology, Pathophysiology, and Pharmacology. Pharmacol. Rev. 2022, 74, 712–768. [Google Scholar] [CrossRef] [PubMed]
- Yao, Q.; Wu, X.; Tao, C.; Gong, W.; Chen, M.; Qu, M.; Zhong, Y.; He, T.; Chen, S.; Xiao, G. Osteoarthritis: Pathogenic Signaling Pathways and Therapeutic Targets. Signal Transduct. Target. Ther. 2023, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.; Zhang, G.; Li, X.; Qiu, X.; Ouyang, J.; Dai, J.; Min, S. Matrix Metalloproteinase 3: A Promoting and Destabilizing Factor in the Pathogenesis of Disease and Cell Differentiation. Front. Physiol. 2021, 12, 663978. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Name | Primer Sequence (5′ → 3′) | |
|---|---|---|
| TNF-α | F | GCATGATCCGAGATGTGGAA |
| R | GATGAGAGGGAGCCCATTTG | |
| COX-2 | F | GTTCCAACCCATGTCAAAAC |
| R | TGTCAGGAATCTCGGCGTAG | |
| IL-6 | F | TCCGCAAGAGACTTCCAGC |
| R | CCTCCGACTTGTGAAGTGG | |
| IL-1β | F | AACTCAACTGTGAAATAGCAGC |
| R | TCCACAGCCACAATGAGTG | |
| MMP-1 | F | AACTTGGGTGAAGACGTCCA |
| R | TCCTGTCACTTTCAGCCCAA | |
| MMP-3 | F | GTACGGCTGTGTGCTCATCC |
| R | TCAGCCCAAGGAACTTCTGC | |
| MMP-8 | F | TCTGTTCTTCTTCCACACACAG |
| R | GCAATCATAGTGGCATTCCT | |
| MMP-13 | F | ACCTTCTTCTTGTTGAGTTGGA |
| R | CTGCATTTCTCGGAGTCTA | |
| NOS2 | F | AGTCAACTACAAGCCCCACG |
| R | GCAGCTTGTCCAGGGATTCT | |
| PGE2 | F | TGTGTGTACTGTCCGTCTGC |
| R | CAGGGATCCAGTCTCGGTGT | |
| GAPDH | F | CTTGTGACAAAGTGGACATTGTT |
| R | TGACCAGCTTCCCATTCTC | |
| Gene Name | Primer Sequence (5′ → 3′) | |
|---|---|---|
| TNF-α | F | GAGAAGTTCCCAAATGGCCT |
| R | AGCCACTCCAGCTGCTCCT | |
| PGE2 | F | CTGGTAACGGAATTGGTGC |
| R | TGGCCAGACTAAAGAAGGTC | |
| IL-6 | F | CACTTCACAAGTCGGAGGCT |
| R | CAAGTGCATCATCGTTGTTC | |
| IL-1β | F | CCAGCTTCAAATCTCGCAGC |
| R | GTGCTCATGTCCTCATCCTGG | |
| MMP-1 | F | ATGCCTAGCCTTCCTTTGCT |
| R | TTCCAGGTATTTCCAGACTG | |
| MMP-3 | F | AAGTTCCTCGGGTTGGAGAT |
| R | ACCAACATCAGGAACACCAC | |
| MMP-8 | F | CAATCAATTCCGGTCTTCGA |
| R | GGTTAGCAAGAAATCACCAGA | |
| MMP-13 | F | AACCAAGATGTGGAGTGCCT |
| R | GACCAGACCTTGAAGGCTTT | |
| GAPDH | F | ATGGTGAAGGTCGGTGTG |
| R | GCCGTGAGTGGAGTCATAC | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, H.-G.; Baek, C.Y.; Kim, D.; Lee, D.; Song, H.S. Stem of Sorbus commixta Hedl. Extract Inhibits Cartilage Degradation and Arthritic Pain in Experimental Model via Anti-Inflammatory Activity. Nutrients 2023, 15, 3774. https://doi.org/10.3390/nu15173774
Jo H-G, Baek CY, Kim D, Lee D, Song HS. Stem of Sorbus commixta Hedl. Extract Inhibits Cartilage Degradation and Arthritic Pain in Experimental Model via Anti-Inflammatory Activity. Nutrients. 2023; 15(17):3774. https://doi.org/10.3390/nu15173774
Chicago/Turabian StyleJo, Hee-Geun, Chae Yun Baek, Donghwan Kim, Donghun Lee, and Ho Sueb Song. 2023. "Stem of Sorbus commixta Hedl. Extract Inhibits Cartilage Degradation and Arthritic Pain in Experimental Model via Anti-Inflammatory Activity" Nutrients 15, no. 17: 3774. https://doi.org/10.3390/nu15173774