
The Effect of Long Chain n-3 Fatty Acid Supplementation on Muscle Strength in Older Adults: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. The Materials and Methods
2.1. Data Sources and Searches
2.2. Selection Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Statistical Analysis
3. Results
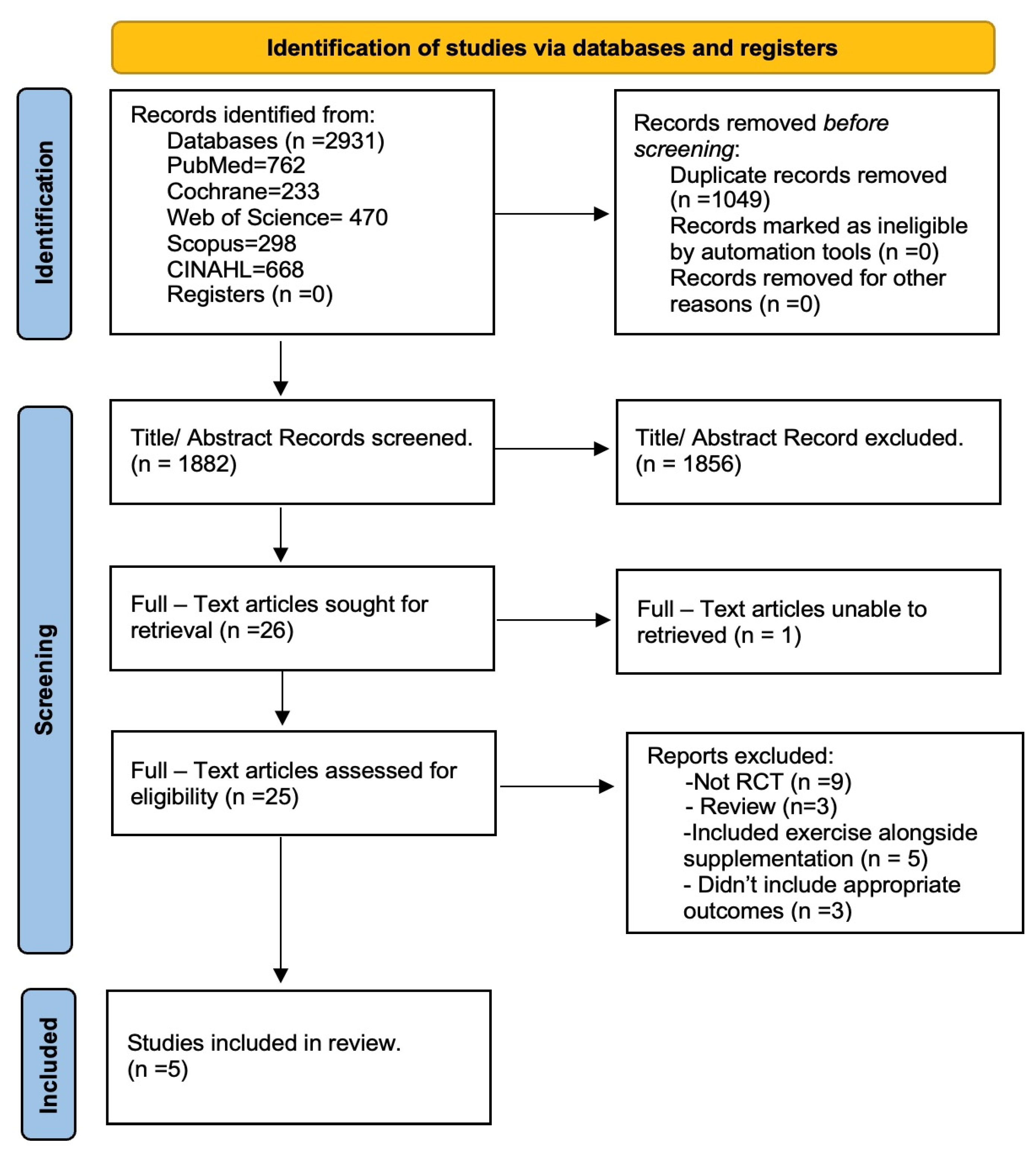
3.1. Study Identification
3.2. Study Characteristics

| Author | Country | Design | Sample | Intervention | Main Effects of LCn-3 PUFA Relative to Placebo |
|---|---|---|---|---|---|
| Alkhedhairi et al. [27]. | UK | Double-blind | n = 94; n = 53 female, n = 41 male; age = 71 ± 5 years. | (4 g/day; of Krill oil 772 mg/d EPA and 384 mg/day DHA) or placebo (4 g/day mixed vegetable oil) for 6 months. | Increase in grip strength (10.9%), leg strength (9.3%), and vastus lateralis muscle thickness (3.5%). No effect on the short-performance physical battery test or whole-body bioelectrical impedance measured muscle mass. |
| Hutchins-Wiese et al. [26]. | USA | Double-blind | n = all females; 126; age = 75 ± 6 years. | (2 capsules Fish oil, 1.2 g/day EPA and DHA) or placebo (2 capsules olive oil, 1.8 g/day olive oil) for 24 weeks. | No effect on grip strength or repeated chair rise test. Increased walking speed (3%) (p = 0.038). |
| Logan [25]. | Canada | Single-blind | n = all female; 24; age = 66 ± 1 years. | (5 g/day Fish oil (2 g/day EPA and 1 g/day DHA)) or placebo (3 g/day olive oil) for 12 weeks. | No effect on grip strength or the 30-s sit-to-stand test. Increased whole-body bioelectrical impedance measured lean mass (4%) and TUG test (7%). |
| Smith et al. [24]. | USA | Double-blind | n = 44; male = 15 and female = 29; age = 69 ± 6 years. | (4 × 1 g pills/day of Fish oil providing 1.86 g/day EPA and 1.5 g/day DHA) or placebo (4 × 1 g pills/day of corn oil) for 6 months. | Increased thigh muscle volume (3.6%), handgrip strength (2.3 kg), and 1-RM muscle strength (4.0%). Average isokinetic power tended to be increased (5.6%) (p = 0.075). |
| Dengfeng Xu [28]. | China | Double-blind | n = 200; female, n = 116; male, n = 84; age = 67 ± 5 years. | (4 g/day; 1.34 g of Fish oil/d EPA and 1.07 g/day DHA) or placebo (4 g/day corn oil) for 6 months. | Increased thigh muscle volume (3.66 cm), handgrip strength (4.91 kg), and Timed Up and Go strength (1.85 s). |
3.3. Intervention and Comparators
3.4. Risk of Bias
3.5. The Effects of LCn-3 PUFA on Muscle Mass and Function
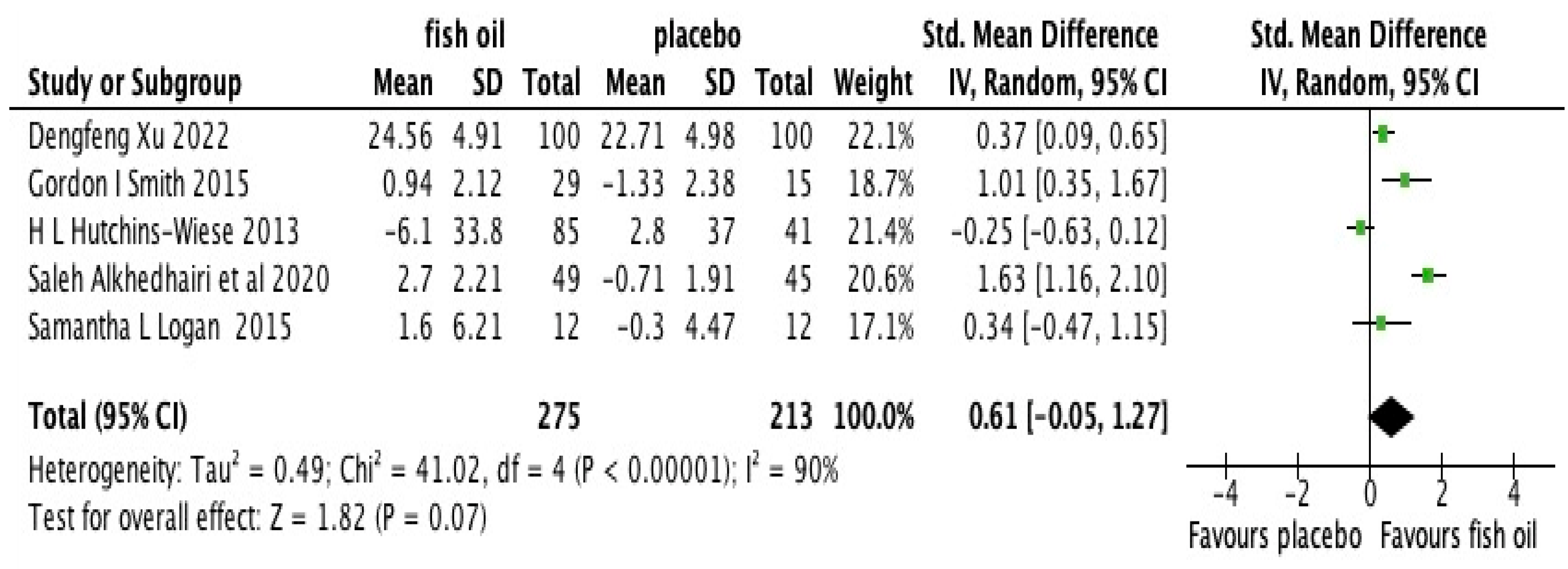
3.6. The Effects of n-3 Fatty Acids on Hand Grip Strength—Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- McGlory, C.; Calder, P.C.; Nunes, E.A. The Influence of Omega-3 Fatty Acids on Skeletal Muscle Protein Turnover in Health, Disuse, and Disease. Front. Nutr. 2019, 6, 144. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, J.L.; Robitaille, Y.; Boivin, J.-F.; Suissa, S. Incidence of and Risk Factors for Falls and Injurious Falls among the Community-dwelling Elderly. Am. J. Epidemiol. 1993, 137, 342–354. [Google Scholar] [CrossRef] [PubMed]
- Mijnarends, D.M. Burden-of-illness of Dutch community-dwelling older adults with sarcopenia: Health-related outcomes and costs. Eur. Geriatr. Med. 2016, 7, 276–284. [Google Scholar] [CrossRef]
- Bruyère, O.; Beaudart, C.; Ethgen, O.; Reginster, J.-Y.; Locquet, M. The health economics burden of sarcopenia: A systematic review. Maturitas 2019, 119, 61–69. [Google Scholar] [CrossRef]
- Pinedo-Villanueva, R.; Westbury, L.D.; Syddall, H.E.; Sanchez-Santos, M.T.; Dennison, E.M.; Robinson, S.M.; Cooper, C. Health Care Costs Associated with Muscle Weakness: A UK Population-Based Estimate. Calcif. Tissue Int. 2019, 104, 137–144. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global prevalence of sarcopenia and severe sarcopenia: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2021, 13, 86–99. [Google Scholar] [CrossRef]
- Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationprojections/bulletins/nationalpopulationprojections/2020basedinterim#changing-age-structure (accessed on 21 June 2023).
- Fiatarone, M.A.; Marks, E.C.; Ryan, N.D.; Meredith, C.N.; Lipsitz, L.A.; Evans, W.J. High-intensity strength training in nonagenarians: Effects on skeletal muscle. JAMA 1990, 263, 3029–3034. [Google Scholar] [CrossRef]
- Greig, C.; Gray, C.; Rankin, D.; Young, A.; Mann, V.; Noble, B.; Atherton, P. Blunting of adaptive responses to resistance exercise training in women over 75 years. Exp. Gerontol. 2011, 46, 884–890. [Google Scholar] [CrossRef]
- Strain, T.; Fitzsimons, C.; Kelly, P.; Mutrie, N. The forgotten guidelines: Cross-sectional analysis of participation in muscle strengthening and balance & co-ordination activities by adults and older adults in Scotland. BMC Public Health 2016, 16, 1108. [Google Scholar] [CrossRef]
- ter Borg, S.; Luiking, Y.C.; van Helvoort, A.; Boirie, Y.; Schols, J.M.G.A.; de Groot, C.P.G.M. Low Levels of Branched Chain Amino Acids, Eicosapentaenoic Acid and Micronutrients are Associated with Low Muscle Mass, Strength and Function in Community-Dwelling Older Adults. J. Nutr. Health Aging 2018, 23, 27–34. [Google Scholar] [CrossRef]
- Robinson, S.M.; Jameson, K.A.; Batelaan, S.F.; Martin, H.J.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Sayer, A.A.; Hertfordshire Cohort Study Group. Diet and its relationship with grip strength in community-dwelling older men and women: The Hert-fordshire cohort study. J. Am. Geriatr. Soc. 2008, 56, 84–90. [Google Scholar] [CrossRef]
- Gedmantaite, A.; Celis-Morales, C.; Ho, F.; Pell, J.; Ratkevicius, A.; Gray, S. Associations between diet and handgrip strength: A cross-sectional study from UK Biobank. Mech. Ageing Dev. 2020, 189, 111269. [Google Scholar] [CrossRef]
- Kamolrat, T.; Gray, S.R. The effect of eicosapentaenoic and docosahexaenoic acid on protein synthesis and breakdown in murine C2C12 myotubes. Biochem. Biophys. Res. Commun. 2013, 432, 593–598. [Google Scholar] [CrossRef]
- Kamolrat, T.; Gray, S.R.; Thivierge, M.C. Fish oil positively reg- ulates anabolic signalling alongside an increase in whole-body gluconeogenesis in ageing skeletal muscle. Eur. J. Nutr. 2013, 52, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Atherton, P.; Reeds, D.N.; Mohammed, B.S.; Rankin, D.; Rennie, M.J.; Mittendorfer, B. Dietary omega-3 fatty acid supplementation increases the rate of muscle protein synthesis in older adults: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 93, 402–412. [Google Scholar] [CrossRef]
- Huang, Y.-H.; Chiu, W.-C.; Hsu, Y.-P.; Lo, Y.-L.; Wang, Y.-H. Effects of Omega-3 Fatty Acids on Muscle Mass, Muscle Strength and Muscle Performance among the Elderly: A Meta- Analysis. Nutrients 2020, 12, 3739. [Google Scholar] [CrossRef] [PubMed]
- Cornish, S.M.; Cordingley, D.M.; Shaw, K.A.; Forbes, S.C.; Leonhardt, T.; Bristol, A.; Candow, D.G.; Chilibeck, P.D. Effects of Omega-3 Supplementation Alone and Combined with Resistance Exercise on Skeletal Muscle in Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2221. [Google Scholar] [CrossRef] [PubMed]
- Bird, J.K.; Troesch, B.; Warnke, I.; Calder, P.C. The effect of long chain omega-3 polyunsaturated fatty acids on muscle mass and function in sarcopenia: A scoping systematic review and meta-analysis. Clin. Nutr. ESPEN 2021, 46, 73–86. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Deeks, J.J. Chapter 7: Selecting studies and collecting data. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 (Updated September 2008); Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2008; Available online: https://training.cochrane.org/handbook (accessed on 21 June 2023).
- Smith, G.I.; Julliand, S.; Reeds, D.N.; Sinacore, D.R.; Klein, S.; Mittendorfer, B. Fish oil–derived n−3 PUFA therapy increases muscle mass and function in healthy older adults. Am. J. Clin. Nutr. 2015, 102, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Logan, S.L.; Spriet, L.L. Omega-3 Fatty Acid Supplementation for 12 Weeks Increases Resting and Exercise Metabolic Rate in Healthy Community-Dwelling Older Females. PLoS ONE 2015, 10, e0144828. [Google Scholar] [CrossRef] [PubMed]
- Hutchins-Wiese, H.L.; Kleppinger, A.; Annis, K.; Liva, E.; Lammi-Keefe, C.J.; Durham, H.A.; Kenny, A.M. The impact of supplemental N-3 long chain polyunsaturated fatty acids and dietary antioxidants on physical performance in postmenopausal women. J. Nutr. Health Aging 2012, 17, 76–80. [Google Scholar] [CrossRef]
- Alkhedhairi, S.A.; Alkhayl, F.F.A.; Ismail, A.D.; Rozendaal, A.; German, M.; MacLean, B.; Johnston, L.; Miller, A.A.; Hunter, A.M.; Macgregor, L.J.; et al. The effect of krill oil supplementation on skeletal muscle function and size in older adults: A ran-domised controlled trial. Clin. Nutr. 2022, 41, 1228–1235. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Lu, Y.; Yang, X.; Pan, D.; Wang, Y.; Yin, S.; Wang, S.; Sun, G. Effects of fish oil-derived n-3 polyunsaturated fatty acid on body composition, muscle strength and physical performance in older people: A secondary analysis of a randomised, double-blind, placebo-controlled trial. Age Ageing 2022, 51, afac274. [Google Scholar] [CrossRef]
- Distefano, G.; Goodpaster, B.H. Effects of Exercise and Aging on Skeletal Muscle. Cold Spring Harb. Perspect. Med. 2018, 8, a029785. [Google Scholar] [CrossRef]
- Won, C.W. Management of Sarcopenia in Primary Care Settings. Korean J. Fam. Med. 2023, 44, 71–75. [Google Scholar] [CrossRef]
- Arnal-Gómez, A.; i Iranzo, M.A.C.; Tomas, J.M.; Tortosa-Chuliá, M.A.; Balasch-Bernat, M.; Sentandreu-Mañó, T.; Forcano, S.; Cezón-Serrano, N. Using the Updated EWGSOP2 Definition in Diagnosing Sarcopenia in Spanish Older Adults: Clinical Approach. J. Clin. Med. 2021, 10, 1018. [Google Scholar] [CrossRef]
- Gray, S.R.; Middendorf, B. Fish oil-derived n-3 polyunsaturated fatty acids for the prevention and treatment of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 104–109. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Vellas, B.; Rizzoli, R.; Kressig, R.W.; da Silva, J.A.P.; Blauth, M.; Felson, D.T.; McCloskey, E.V.; Watzl, B.; Hofbauer, L.C.; et al. Effect of Vitamin D Supplementation, Omega-3 Fatty Acid Supplementation, or a Strength-Training Exercise Program on Clinical Outcomes in Older Adults The DO-HEALTH Randomized Clinical Trial. JAMA-J. Am. Med. Assoc. 2020, 324, 1855–1868. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Atherton, P.; Reeds, D.N.; Mohammed, B.S.; Rankin, D.; Rennie, M.J.; Mittendorfer, B. Omega-3 polyunsaturated fatty acids augment the muscle protein anabolic response to hyperinsulinae-mia-hyperaminoacidaemia in healthy young and middle-aged men and women. Clin. Sci. 2011, 121, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Štěpán, M.; Daďová, K.; Matouš, M.; Krauzová, E.; Sontáková, L.; Koc, M.; Larsen, T.; Kuda, O.; Štich, V.; Rossmeislová, L.; et al. Exercise Training Combined with Calanus Oil Sup- plementation Improves the Central Cardiodynamic Function in Older Women. Nutrients 2021, 14, 149. [Google Scholar] [CrossRef] [PubMed]
- Salem, N., Jr.; Litman, B.; Kim, H.-Y.; Gawrisch, K. Mechanisms of action of docosahexaenoic acid in the nervous system. Lipids 2001, 36, 945–959. [Google Scholar] [CrossRef]
- Lewis, E.J.H.; Radonic, P.W.; Wolever, T.M.S.; Wells, G.D. 21 days of mammalian omega-3 fatty acid supplementation improves aspects of neuromuscular function and performance in male athletes compared to olive oil placebo. J. Int. Soc. Sports Nutr. 2015, 12, 28. [Google Scholar] [CrossRef]
- Jammes, Y.; Adjriou, N.; Kipson, N.; Criado, C.; Charpin, C.; Rebaudet, S.; Stavris, C.; Guieu, R.; Fenouillet, E.; Retornaz, F. Altered muscle membrane potential and redox status differentiates two subgroups of patients with chronic fatigue syndrome. J. Transl. Med. 2020, 18, 173. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timraz, M.; Binmahfoz, A.; Quinn, T.J.; Combet, E.; Gray, S.R. The Effect of Long Chain n-3 Fatty Acid Supplementation on Muscle Strength in Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 3579. https://doi.org/10.3390/nu15163579
Timraz M, Binmahfoz A, Quinn TJ, Combet E, Gray SR. The Effect of Long Chain n-3 Fatty Acid Supplementation on Muscle Strength in Older Adults: A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(16):3579. https://doi.org/10.3390/nu15163579
Chicago/Turabian StyleTimraz, Maha, Ahmad Binmahfoz, Terry J. Quinn, Emilie Combet, and Stuart R. Gray. 2023. "The Effect of Long Chain n-3 Fatty Acid Supplementation on Muscle Strength in Older Adults: A Systematic Review and Meta-Analysis" Nutrients 15, no. 16: 3579. https://doi.org/10.3390/nu15163579