
Diets, Lifestyles and Metabolic Risk Factors among Corporate Information Technology (IT) Employees in South India
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Selection of the Study Sites and Participants Recruitment
2.3. Data Collection
2.3.1. Anthropometric Measurements
2.3.2. Clinical Assessment
2.3.3. Biochemical Assessment
2.3.4. Assessment of Selected Biomarker Levels
2.4. Statistical Analysis
3. Results
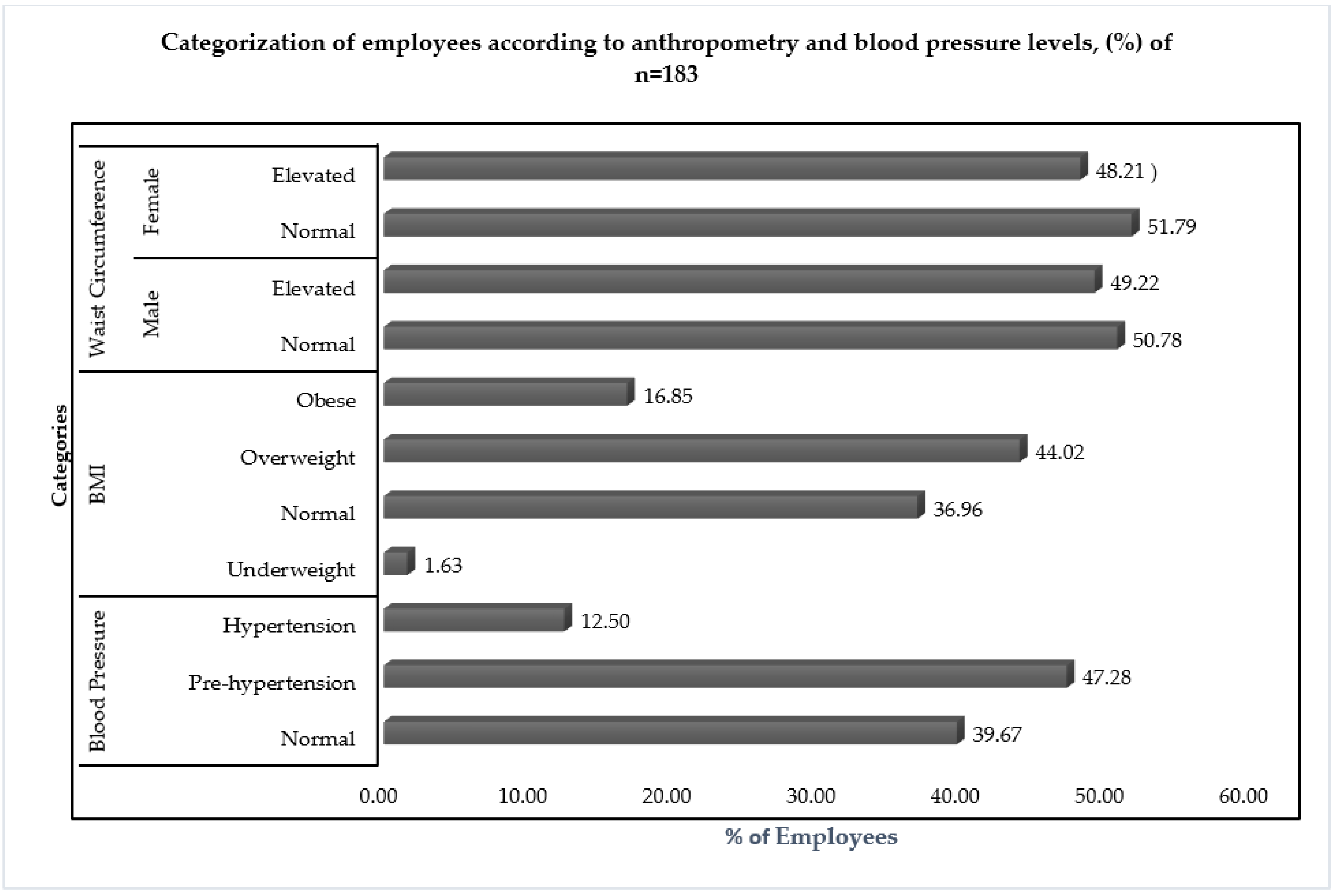
3.1. Health and Nutrition Status of the Employees
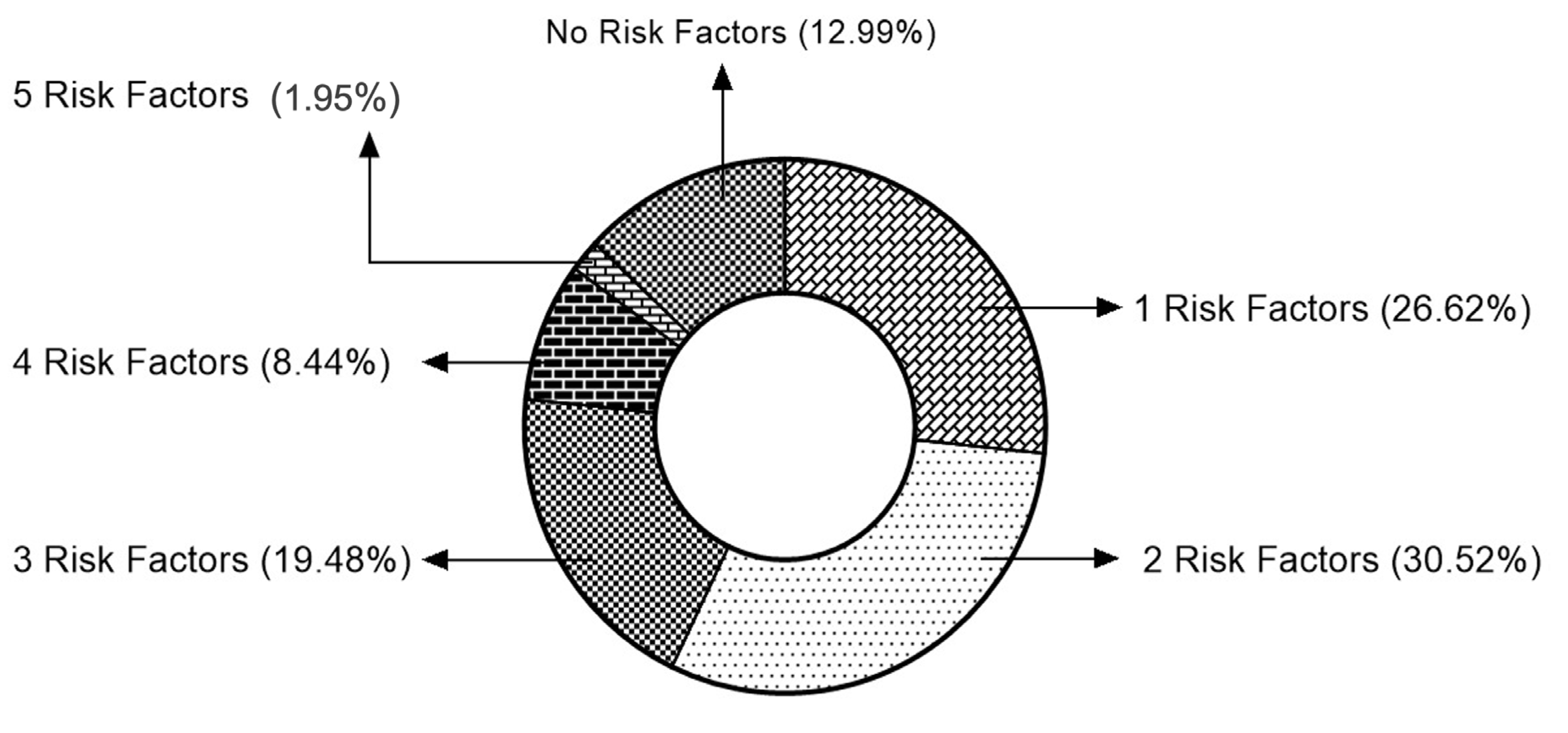
3.2. Prevalence of Metabolic Risk Factors and Metabolic Syndrome
3.3. KAP of the Employees on Health, Food and Lifestyle
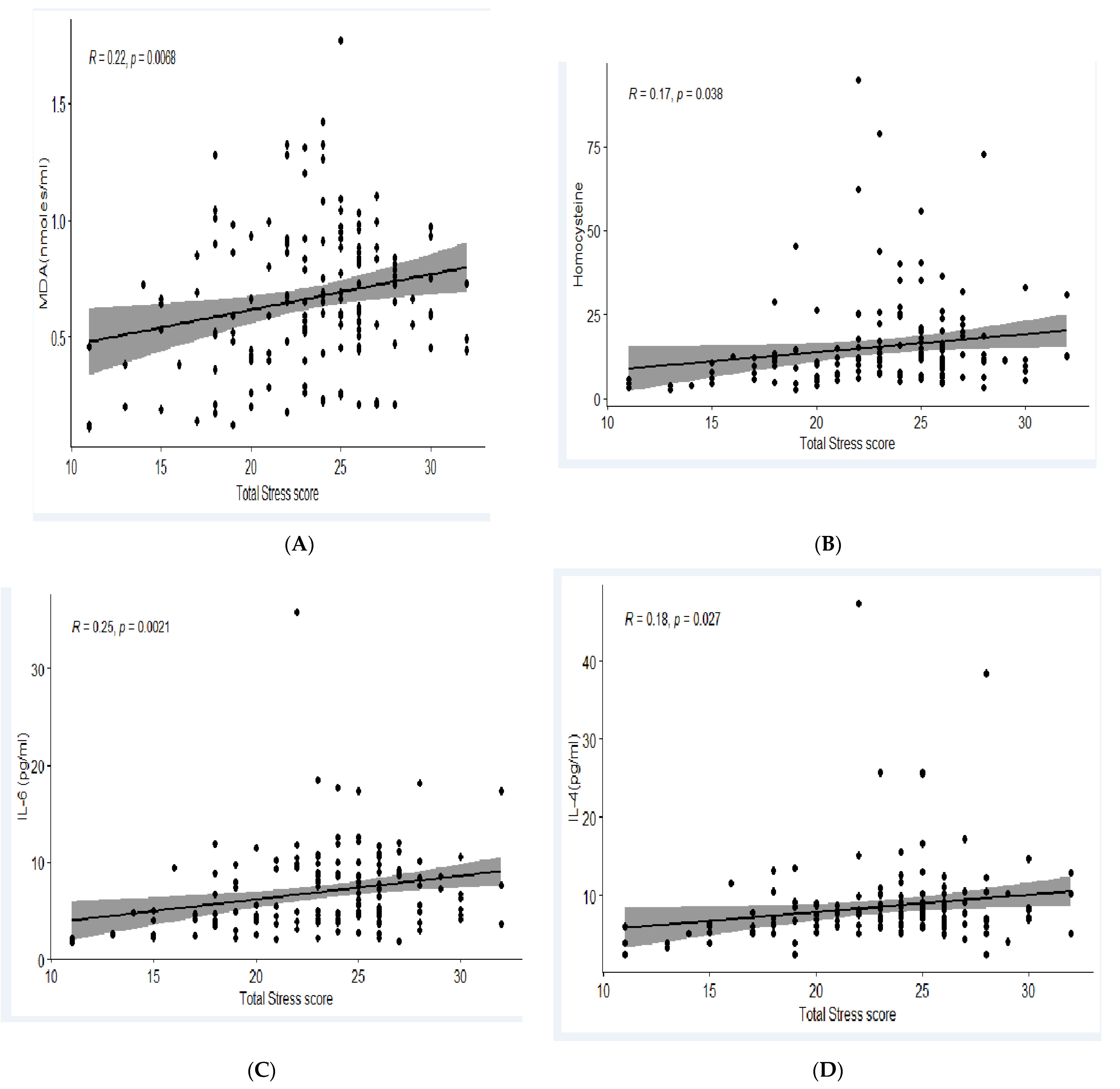
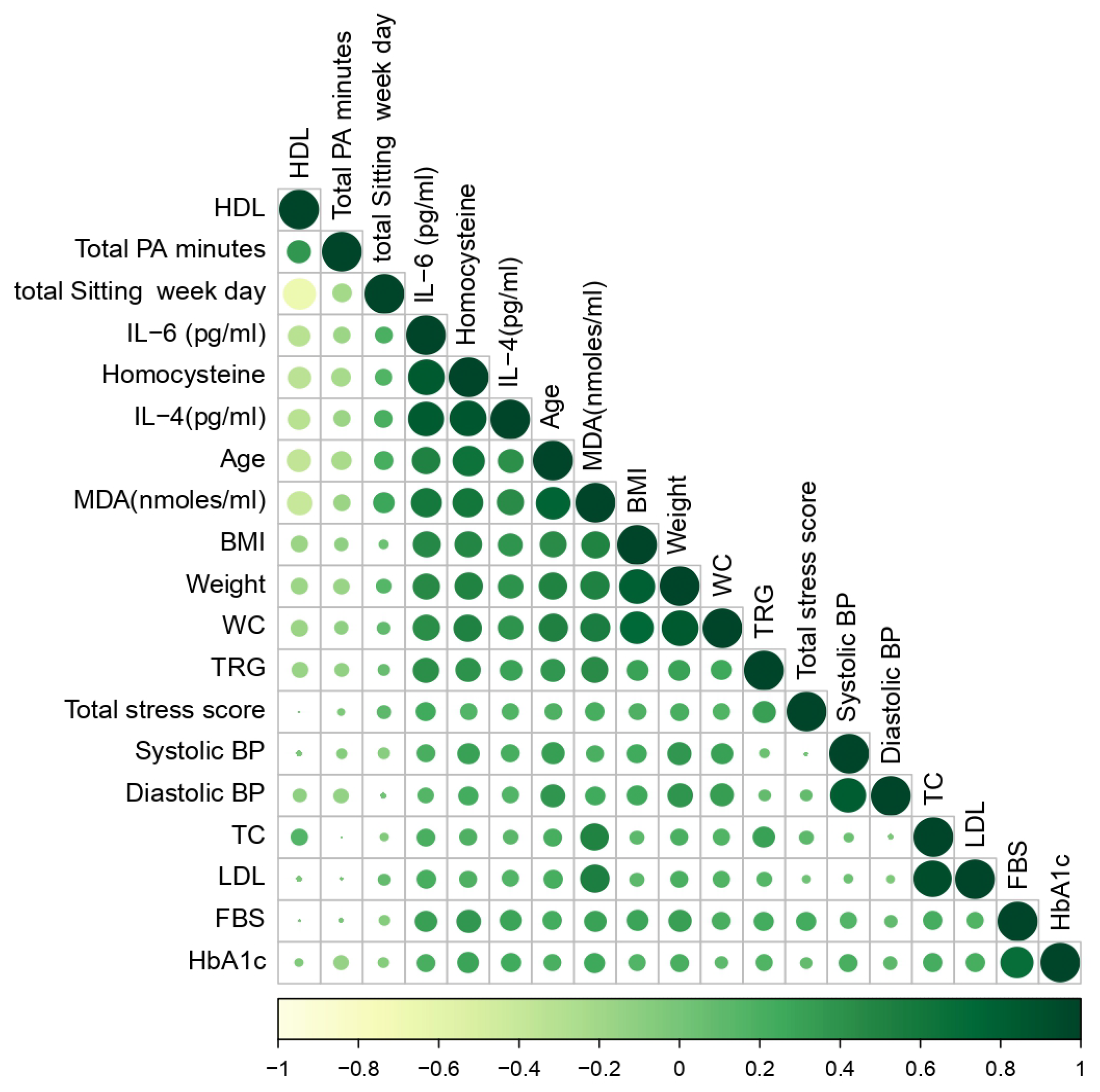
3.4. Association of Biomarkers with Perceived Stress Score, Diet and PA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhatnagar, S. India’s Software Industry. In Technology, Adaptation, and Exports: How Some Developing Countries Get It Right; Chandra, V., Ed.; World Bank: New York, NY, USA, 2006. [Google Scholar]
- Chandra, V. (Ed.) Technology, Adaptation, and Exports: How Some Developing Countries Got It Right; World Bank Publications: Washington, DC, USA, 2006. [Google Scholar]
- India Brand Equity Foundation. IT and BPM Industry Report; c2010-15. 2022. Available online: https://www.ibef.org/industry/informationtechnology-india (accessed on 23 May 2022).
- Seema, M. Prevalence of Lifestyle Diseases and the Impact of Nutrition Education Programme among the Professionals of Corporate Sector. Int. J. Sci. Res. 2013, 4, 2020–2022. [Google Scholar]
- Rameswarapu, R.; Lakshman, R.L.; Valsangkar, S. Self-reported prevalence and practices impacting the outcome of non-communicable diseases among corporate professional employees in India. Mrims J. Health Sci. 2014, 2, 15. [Google Scholar] [CrossRef]
- Esmailnasab, N.; Moradi, G.; Delaveri, A. Risk factors of noncommunicable diseases and metabolic syndrome. Iran. J. Public Health 2012, 41, 77–85. [Google Scholar] [PubMed]
- Limaye, T.Y.; Kulkarni, R.L.; Deokar, M.R.; Kumaran, K. High prevalence of cardiometabolic risk factors in young employees of Information Technology industry. Indian J. Occup. Environ. Med. 2016, 20, 64–67. [Google Scholar] [CrossRef]
- Gillespie, D.R. Burnout among health service providers. Adm. Policy Ment. Health Ment. Health Serv. 1991, 18, 161–171. [Google Scholar] [CrossRef]
- Maes, M.; Van Gastel, A.; Delmeire, L.; Kenis, G.; Bosmans, E.; Song, C. Platelet α2-adrenoceptor density in humans: Relationships to stress-induced anxiety, psychasthenic constitution, gender and stress-induced changes in the inflammatory response system. Psychol. Med. 2002, 32, 919–928. [Google Scholar] [CrossRef]
- Almadi, T.; Cathers, I.; Hamdan Mansour, A.M.; Chow, C.M. The association between work stress and inflammatory biomarkers in J ordanian male workers. Psychophysiology 2012, 49, 172–177. [Google Scholar] [CrossRef]
- Chandola, T.; Brunner, E.; Marmot, M. Chronic stress at work and the metabolic syndrome: Prospective study. BMJ 2006, 332, 521–525. [Google Scholar] [CrossRef] [Green Version]
- Padma, V.; Anand, N.N.; Gurukul, S.M.; Javid, S.M.; Prasad, A.; Arun, S. Health problems and stress in Information Technology and Business Process Outsourcing employees. J. Pharm. Bioallied Sci. 2015, 7 (Suppl. S1), S9–S13. [Google Scholar] [CrossRef]
- Casado, Á.; De Lucas, N.; López-Fernández, E.; Sánchez, A.; Jimenez, J.A. Lipid peroxidation, occupational stress and aging in workers of a prehospital emergency service. Eur. J. Emerg. Med. 2006, 13, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Salaroli, L.B.; Saliba, R.A.; Zandonade, E.; Molina, M.D.; Bissoli, N.S. Prevalence of metabolic syndrome and related factors in bank employees according to different defining criteria, Vitória/ES, Brazil. Clinics 2013, 68, 69–74. [Google Scholar] [CrossRef]
- Ryu, H.; Chin, D.L. Factors associated with metabolic syndrome among Korean office workers. Arch. Environ. Occup. Health 2017, 72, 249–257. [Google Scholar] [CrossRef]
- Vangelova, K. Cardiovascular risk factors in white collar workers under shift work. Acta Medica Bulg. 2017, 44, 5–9. [Google Scholar] [CrossRef]
- Roomi, M.A.; Mohammadnezhad, M. Prevalence of metabolic syndrome among apparently healthy workforce. J. Ayub Med. Coll. Abbottabad 2019, 31, 252–264. [Google Scholar]
- Schultz, A.B.; Edington, D.W. Metabolic syndrome in a workplace: Prevalence, co-morbidities, and economic impact. Metab. Syndr. Relat. Disord. 2009, 7, 459–468. [Google Scholar] [CrossRef] [Green Version]
- Alzeidan, R.; Rabiee, F.; Mandil, A.; Hersi, A.; Fayed, A. Noncommunicable disease risk factors among employees and their families of a Saudi university: An epidemiological study. PLoS ONE 2016, 11, e0165036. [Google Scholar] [CrossRef] [Green Version]
- Stamatakis, E.; Chau, J.Y.; Pedisic, Z.; Bauman, A.; Macniven, R.; Coombs, N.; Hamer, M. Are sitting occupations associated with increased all-cause, cancer, and cardiovascular disease mortality risk? A pooled analysis of seven British population cohorts. PLoS ONE 2013, 8, e73753. [Google Scholar] [CrossRef] [Green Version]
- Chaudhury, N.; Modi, S. Employee Wellness Programmes in the Context of an Emerging Epidemic of Lifestyle Diseases: What Works and What Doesn’t? NHRD Netw. J. 2016, 9, 33–38. [Google Scholar] [CrossRef]
- Kundu, M.K.; Hazra, S.; Pal, D.; Bhattacharya, M. A review on Noncommunicable Diseases (NCDs) burden, its socio-economic impact and the strategies for prevention and control of NCDs in India. Indian J. Public Health 2018, 62, 302–304. [Google Scholar] [CrossRef]
- Healthy Workplaces: A Model for Action. 2010. Available online: https://www.who.int/publications/i/item/9789241599313 (accessed on 18 June 2023).
- Genin, P.; Beaujouan, J.; Thivel, D.; Duclos, M. Is workplace an appropriate setting for the promotion of physical activity? A new framework for worksite interventions among employees. Work 2019, 62, 421–426. [Google Scholar] [CrossRef]
- Soler, R.E.; Leeks, K.D.; Razi, S.; Hopkins, D.P.; Griffith, M.; Aten, A.; Chattopadhyay, S.K.; Smith, S.C.; Habarta, N.; Goetzel, R.Z.; et al. Task Force on Community Preventive Services. A systematic review of selected interventions for worksite health promotion: The assessment of health risks with feedback. Am. J. Prev. Med. 2010, 38, S237–S262. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, P.; Gavaravarapu, S.M. Wellness programmes in the workplace in India. Lancet Public Health 2018, 3, e515. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, P.; Reddy, B.G.; Gavaravarapu, S.M. Identifying opportunities and barriers for introducing a workplace nutrition and health programme for employees: Findings from formative research. Work 2022, 73, 1175–1187. [Google Scholar] [CrossRef]
- HYSEA. Hyderabad: Global Technology Destination, 1st ed.; Hyderabad Software Enterprises Association (HYSEA): Telangana, India, 2019; Available online: https://hysea.in/hysea.in/wp-content/uploads/2019/08/Scale@Hyderabad.pdf (accessed on 9 June 2019).
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Moreto, F.; de Oliveira, E.P.; Manda, R.M.; Burini, R.C. The higher plasma malondialdehyde concentrations are determined by metabolic syndromerelated glucolipotoxicity. Oxidative Med. Cell. Longev. 2014, 2014, 505368. [Google Scholar] [CrossRef] [Green Version]
- Von Känel, R.; Bellingrath, S.; Kudielka, B.M. Association between burnout and circulating levels of pro-and anti-inflammatory cytokines in schoolteachers. J. Psychosom. Res. 2008, 65, 51–59. [Google Scholar] [CrossRef]
- De Koning, A.L.; Werstuck, G.H.; Zhou, J.; Austin, R.C. Hyperhomocysteinemia and its role in the development of atherosclerosis. Clin. Biochem. 2003, 36, 431–441. [Google Scholar] [CrossRef]
- Bhuyan, K.C.; Bhuyan, D.K.; Johansen, N. Estimation of Malondildehyde. PRCS Med. Sci. 1981, 9, 126–127. [Google Scholar]
- Alberti, K.G. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Kang, D.R.; Ha, Y.; Hwang, W.J. Prevalence and associated risk factors of the metabolic syndrome in the Korean workforce. Ind. Health 2013, 51, 256–265. [Google Scholar] [CrossRef] [Green Version]
- Burton, W.N.; Chen, C.Y.; Li, X.; Schultz, A.B.; Abrahamsson, H. The association of self-reported employee physical activity with metabolic syndrome, health care costs, absenteeism, and presenteeism. J. Occup. Environ. Med. 2014, 56, 919–926. [Google Scholar] [CrossRef] [Green Version]
- Owiredu WK, B.A.; Amidu, N.; Gockah-Adapoe, E.; Ephraim RK, D. The prevalence of metabolic syndrome among active sportsmen/sportswomen and sedentary workers in the Kumasi metropolis. J. Sci. Technol. 2011, 31, 1. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, N.; Kukkonen-Harjula, K.T.; Verbeek, J.H.; Ijaz, S.; Hermans, V.; Pedisic, Z. Workplace interventions for reducing sitting at work. Cochrane Database Syst. Rev. 2018, 6, CD010912. [Google Scholar]
- Rao, J.V.; Chandraiah, K. Occupational stress, mental health and coping among information technology professionals. Indian J. Occup. Environ. Med. 2012, 16, 22. [Google Scholar] [CrossRef] [Green Version]
- Steptoe, A.; Brunner, E.; Marmot, M. Stress-induced inflammatory responses and risk of the metabolic syndrome: A longitudinal analysis. In Proceedings of the Obesity Research North Amer Assoc Study Obesity, Las Vegas, NV, USA, 14–18 November 2004; Volume 12, p. A76. [Google Scholar]
- Vimala, B.; Madhavi, C. A study on stress and depression experienced by women IT professionals in Chennai, India. Psychol. Res. Behav. Manag. 2009, 2, 81–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botha, C.; Pienaar, J. South African correctional official occupational stress: The role of psychological strengths. J. Crim. Justice 2006, 34, 73–84. [Google Scholar] [CrossRef]
- Taap Manshor, A.; Fontaine, R.; Siong Choy, C. Occupational stress among managers: A Malaysian survey. J. Manag. Psychol. 2003, 18, 622–628. [Google Scholar] [CrossRef]
- Prasad, K.D.; Vaidya, R.; Kumar, V.A. A Comparative Analysis: Causes of Stress among the Employees and its Effect on the Performance at the Workplace in Agricultural Research and Information Technology Sectors. AIMA J. Manag. Res. 2016, 10, 1–23. [Google Scholar]
- Geaney, F.; Kelly, C.; Di Marrazzo, J.S.; Harrington, J.M.; Fitzgerald, A.P.; Greiner, B.A.; Perry, I.J. The effect of complex workplace dietary interventions on employees’ dietary intakes, nutrition knowledge and health status: A cluster controlled trial. Prev. Med. 2016, 89, 76–83. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biochemical Parameters | Number of Participants (n = 154) and Median (P25–P75) Values |
|---|---|
| Fasting Blood Glucose (FBG) mg/dL | 88 (82–93.5) |
| Glycosylated Haemoglobin (HbA1c %) | 5.6 (5.3–5.8) |
| Total Cholesterol (TC) mg/dL | 175.6 (150.4–212) |
| High-Density Lipoprotein (HDL-C) mg/dL | 40 (32–48) |
| Low-Density Lipoprotein (LDL-C) mg/dL | 105 (87–142.5) |
| Triglycerides (TG) mg/dL | 128.5 (104.5–157) |
| Metabolic Risk Factor | Percentage of Study Population (n = 154) |
|---|---|
| n (%) | |
| Elevated Blood pressure (≥130/85 mmHg) | 32 (20.77) |
| Low High-density lipoprotein (<40 mg/dL-Males, <50 mg/dL Females) | 89 (57.79) |
| High Triglycerides (≥150 mg/dL) | 57 (37.01) |
| Elevated Fasting Blood Sugar (≥100 mg/dL) | 30 (19.48) |
| Elevated Waist Circumference (Males-≥90 cm, Females ≥80 cm) | 84 (54.54) |
| Parameters | No MetS (Score 0–2) | MetS (Score 3–5) | p Value |
|---|---|---|---|
| Age (Years) | 28 (21–40) | 38.5 (22–50) | 0.000 * |
| Homocysteine (µmole/L) | 9.80 (2.66–23.95) | 25.37 (5.7–94.94) | 0.001 * |
| MDA (nmoles/mL) | 0.55 (0.12–1.09) | 0.92 (0.6–1.77) | 0.003 * |
| IL-6 (pg/mL) | 4.60 (1.67–12.04) | 9.5 (4.63–35.86) | 0.017 * |
| IL-4 (pg/mL) | 6.56 (2.34–13.2) | 9.4 (6.18–47.45) | 0.000 * |
| Behavioural Risk Factors | Indicators | Prevalence (n, %) |
|---|---|---|
| Dietary Risk Factors | Skipping at least 1 meal every day | 50 (30.12%) |
| Consuming >400 g of fruits or vegetables every day | 64 (38.55%) | |
| Adding extra salt to food on table | 51 (30.7%) | |
| Eating out frequency > once every week | 111 (66.8%) | |
| Activity Status | Not involved in intentional physical activity | 87 (52.4%) |
| Total intentional physical activity time <150 min/week | 128 (77.10) | |
| Total sitting time >8 h/day | 147 (88.55%) | |
| Smoking habits | Regular smoking | 37 (22.2%) |
| Alcohol consumption | Regular consumption of alcohol | 35 (0.21%) |
| Stress Level | High self-perceived stress level (stress score ≥ 26) | 56 (33.73%) |
| Risk Factors | <30 Years (n, %) | ≥30 Years (n, %) | X2 | Significance |
|---|---|---|---|---|
| Skipping meals | 39 (50.6) | 8 (10.4) | 29.42 | 0.000 * |
| <400 g of fruits & veggies | 46 (59.7) | 55 (71.4) | 2.33 | 0.127 |
| Adding extra salt | 19 (24.7 | 26 (33.8) | 1.53 | 0.215 |
| Frequent eating out | 72 (93.5) | 51 (66.3) | 23.93 | 0.000 * |
| >8 h sitting time/day | 68 (83.3) | 71 (92.2) | .665 | 0.415 |
| No involvement in intentional physical activity | 31 (40.3) | 52 (67.5) | 11.52 | 0.001 * |
| <150 min Physical Activity/week | 56 (72.7) | 68 (88.3) | 5.96 | 0.015 |
| Smoking | 34 (44.2) | 42 (54.5) | 3.85 | 0.197 |
| Alcoholism | 45 (58.5) | 45 (58.5) | 3.87 | 0.144 |
| High perceived Stress | 47 (61.1) | 63 (81.8) | 9.48 | 0.000 * |
| Metabolic syndrome | 2 (2.6) | 44 (28.57) | 5.468 | 0.000 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banerjee, P.; Reddy, G.B.; Panda, H.; Angadi, K.K.; Reddy, T.; Gavaravarapu, S.M. Diets, Lifestyles and Metabolic Risk Factors among Corporate Information Technology (IT) Employees in South India. Nutrients 2023, 15, 3404. https://doi.org/10.3390/nu15153404
Banerjee P, Reddy GB, Panda H, Angadi KK, Reddy T, Gavaravarapu SM. Diets, Lifestyles and Metabolic Risk Factors among Corporate Information Technology (IT) Employees in South India. Nutrients. 2023; 15(15):3404. https://doi.org/10.3390/nu15153404
Chicago/Turabian StyleBanerjee, Paromita, G. Bhanuprakash Reddy, Hrusikesh Panda, Kiran Kumar Angadi, Thirupathi Reddy, and SubbaRao M. Gavaravarapu. 2023. "Diets, Lifestyles and Metabolic Risk Factors among Corporate Information Technology (IT) Employees in South India" Nutrients 15, no. 15: 3404. https://doi.org/10.3390/nu15153404