
Longer-Term Weight Loss Outcomes Are Not Primarily Driven by Diet Following Roux-en-Y Gastric Bypass and Sleeve Gastrectomy
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Recruitment
2.2. Study Design and Timeline
2.3. Biometrics and Dietary Recall
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
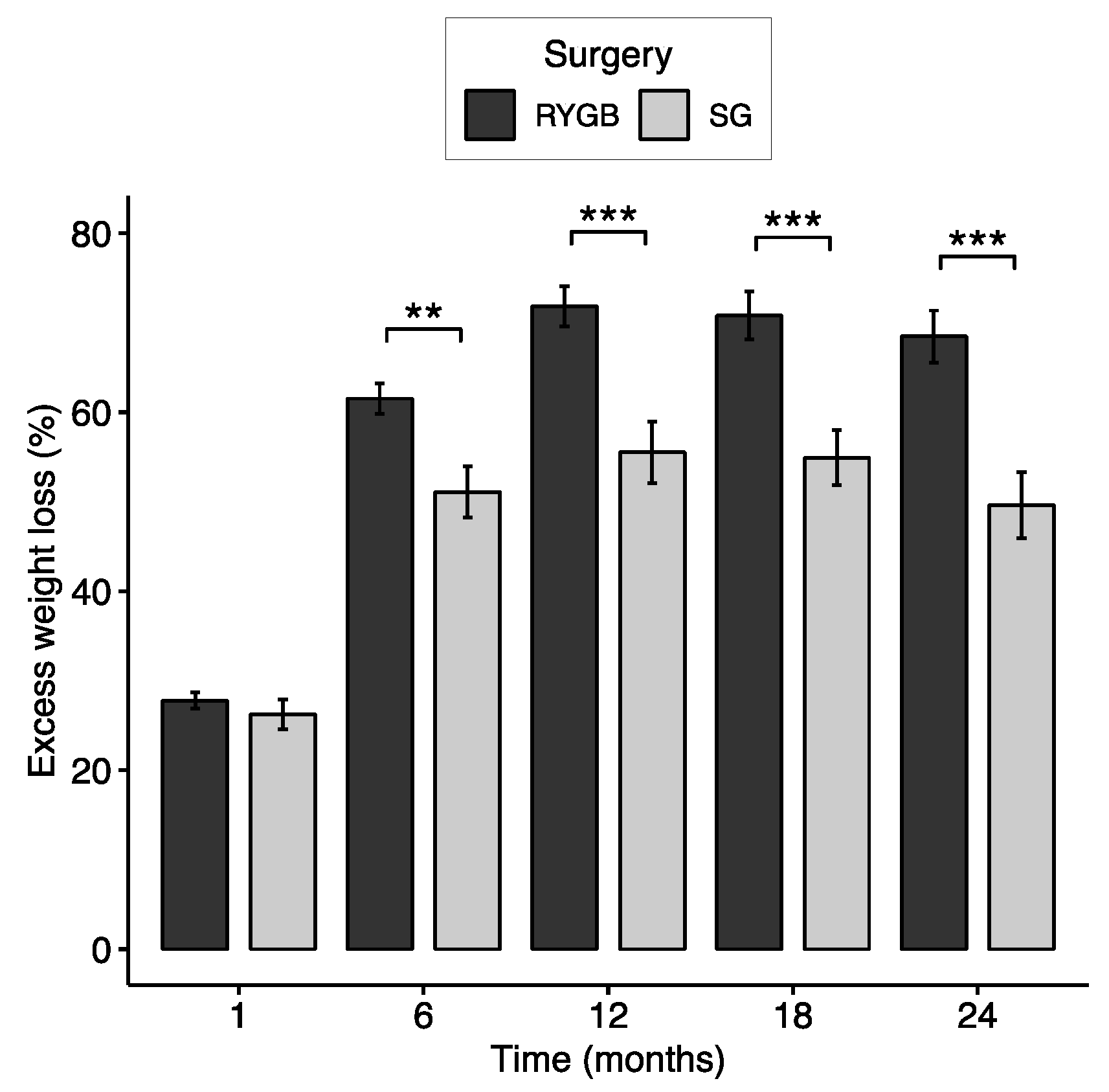
3.2. Excess Weight Loss and Responder Status
3.3. Changes in Total Energy and Macronutrient Intake
3.4. Direct Associations between Nutrient Intake and %EWL at 12-, 18-, and 24-Months
3.5. Changes in Total Energy and Macronutrient Intake over Time by Weight Loss Response
3.5.1. Dietary Intake and Weight Loss Outcomes at 12 Months
3.5.2. Dietary Intake and Weight Loss Outcomes at 18 Months
3.5.3. Dietary Intake and Weight Loss Outcomes at 24 Months
3.6. Differences in Sample Size and Power Do Not Explain Differences in Outcome between 12 and 24 Months
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- King, W.C.; Hinerman, A.S.; White, G.E.; Courcoulas, A.P.; Saad, M.A.B.; Belle, S.H. Associations between Physical Activity and Changes in Weight across 7 Years after Roux-En-Y Gastric Bypass Surgery: A Multicenter Prospective Cohort Study. Ann. Surg. 2022, 275, 718–726. [Google Scholar] [CrossRef]
- Madsbad, S.; Holst, J.J. Bariatric Surgery—Which Procedure Is the Optimal Choice? Lancet 2019, 393, 1263–1264. [Google Scholar] [CrossRef]
- American Society for Metabolic and Bariatric Surgery Estimate of Bariatric Surgery Numbers, 2011–2020. Available online: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers (accessed on 21 September 2022).
- Reinhold, R.B. Critical Analysis of Long Term Weight Loss Following Gastric Bypass. Surg. Gynecol. Obstet. 1982, 155, 385–394. [Google Scholar] [PubMed]
- Van de Laar, A.; de Caluwé, L.; Dillemans, B. Relative Outcome Measures for Bariatric Surgery. Evidence against Excess Weight Loss and Excess Body Mass Index Loss from a Series of Laparoscopic Roux-En-Y Gastric Bypass Patients. Obes. Surg. 2011, 21, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D.; Kahan, S. Maintenance of Lost Weight and Long-Term Management of Obesity. Med. Clin. N. Am. 2018, 102, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Lozano, T.; Vidal, J.; de Hollanda, A.; Scheer, F.A.J.L.; Garaulet, M.; Izquierdo-Pulido, M. Timing of Food Intake Is Associated with Weight Loss Evolution in Severe Obese Patients after Bariatric Surgery. Clin. Nutr. 2016, 35, 1308–1314. [Google Scholar] [CrossRef] [Green Version]
- Handzlik-Orlik, G.; Holecki, M.; Orlik, B.; Wyleżoł, M.; Duława, J. Nutrition Management of the Post–Bariatric Surgery Patient. Nutr. Clin. Pract. 2015, 30, 383–392. [Google Scholar] [CrossRef]
- Sherf Dagan, S.; Goldenshluger, A.; Globus, I.; Schweiger, C.; Kessler, Y.; Kowen Sandbank, G.; Ben-Porat, T.; Sinai, T. Nutritional Recommendations for Adult Bariatric Surgery Patients: Clinical Practice. Adv. Nutr. 2017, 8, 382–394. [Google Scholar] [CrossRef] [Green Version]
- Healthy Diet. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 5 July 2023).
- Healthy Weight Loss. Available online: https://www.cdc.gov/healthyweight/losing_weight/index.html (accessed on 5 July 2023).
- Maintain a Healthy Weight. Available online: https://www.nhlbi.nih.gov/health/educational/lose_wt/index.htm (accessed on 5 July 2023).
- Kanerva, N.; Larsson, I.; Peltonen, M.; Lindroos, A.-K.; Carlsson, L.M. Changes in Total Energy Intake and Macronutrient Composition after Bariatric Surgery Predict Long-Term Weight Outcome: Findings from the Swedish Obese Subjects (SOS) Study. Am. J. Clin. Nutr. 2017, 106, 136–145. [Google Scholar] [CrossRef] [Green Version]
- Miller, G.D.; Norris, A.; Fernandez, A. Changes in Nutrients and Food Groups Intake Following Laparoscopic Roux-En-Y Gastric Bypass (RYGB). Obes. Surg. 2014, 24, 1926–1932. [Google Scholar] [CrossRef] [Green Version]
- Raatz, S.K.; Johnson, L.K.; Caliquary, A.; King, W.C.; Kalarchian, M.A.; Devlin, M.J.; Marcus, M.D.; Mitchell, J.E. Reported Nutrient Intake over 7 Years after Roux-En-Y Gastric Bypass in the Longitudinal Assessment of Bariatric Surgery-3 (LABS-3) Psychosocial Study. Surg. Obes. Relat. Dis. 2020, 16, 1022–1029. [Google Scholar] [CrossRef]
- Cani, P.D. Metabolism in 2013: The Gut Microbiota Manages Host Metabolism. Nat. Rev. Endocrinol. 2014, 10, 74–76. [Google Scholar] [CrossRef]
- Karmali, S.; Brar, B.; Shi, X.; Sharma, A.M.; de Gara, C.; Birch, D.W. Weight Recidivism Post-Bariatric Surgery: A Systematic Review. Obes. Surg. 2013, 23, 1922–1933. [Google Scholar] [CrossRef]
- Courcoulas, A.P.; Christian, N.J.; Belle, S.H.; Berk, P.D.; Flum, D.R.; Garcia, L.; Horlick, M.; Kalarchian, M.A.; King, W.C.; Mitchell, J.E.; et al. Weight Change and Health Outcomes at 3 Years after Bariatric Surgery among Individuals with Severe Obesity. JAMA 2013, 310, 2416–2425. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.-S.; Kim, Y.J.; Lee, J.; Yoon, S.-J.; Lee, B. Establishment of Adequate Nutrient Intake Criteria to Achieve Target Weight Loss in Patients Undergoing Bariatric Surgery. Nutrients 2020, 12, 1774. [Google Scholar] [CrossRef] [PubMed]
- Heinberg, L.J.; Bond, D.S.; Carroll, I.; Crosby, R.; Fodor, A.; Fouladi, F.; Gunstad, J.; Mitchell, J.; Peat, C.; Steffen, K. Identifying Mechanisms That Predict Weight Trajectory after Bariatric Surgery: Rationale and Design of the BioBehavioral Trial. Surg. Obes. Relat. Dis. 2020, 16, 1816–1826. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health Automated Self-Administered 24-Hour (ASA24®) Dietary Assessment Tool. Available online: https://epi.grants.cancer.gov/asa24/ (accessed on 5 April 2023).
- Widaman, A.M.; Keim, N.L.; Burnett, D.J.; Miller, B.; Witbracht, M.G.; Widaman, K.F.; Laugero, K.D. A Potential Tool for Clinicians; Evaluating a Computer-Led Dietary Assessment Method in Overweight and Obese Women during Weight Loss. Nutrients 2017, 9, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Courcoulas, A.; Coley, R.Y.; Clark, J.M.; McBride, C.L.; Cirelli, E.; McTigue, K.; Arterburn, D.; Coleman, K.J.; Wellman, R.; Anau, J.; et al. Interventions and Operations 5 Years after Bariatric Surgery in a Cohort from the US National Patient-Centered Clinical Research Network Bariatric Study. JAMA Surg. 2020, 155, 194–204. [Google Scholar] [CrossRef]
- Gutiérrez-Repiso, C.; Molina-Vega, M.; Bernal-López, M.R.; Garrido-Sánchez, L.; García-Almeida, J.M.; Sajoux, I.; Moreno-Indias, I.; Tinahones, F.J. Different Weight Loss Intervention Approaches Reveal a Lack of a Common Pattern of Gut Microbiota Changes. J. Pers. Med. 2021, 11, 109. [Google Scholar] [CrossRef]
- Lanyon, R.I.; Maxwell, B.M.; Kraft, A.J. Prediction of Long-Term Outcome after Gastric Bypass Surgery. Obes. Surg. 2009, 19, 439–445. [Google Scholar] [CrossRef]
- Kruseman, M.; Leimgruber, A.; Zumbach, F.; Golay, A. Dietary, Weight, and Psychological Changes among Patients with Obesity, 8 Years after Gastric Bypass. J. Am. Diet. Assoc. 2010, 110, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Courcoulas, A.P.; King, W.C.; Belle, S.H.; Berk, P.; Flum, D.R.; Garcia, L.; Gourash, W.; Horlick, M.; Mitchell, J.E.; Pomp, A.; et al. Seven-Year Weight Trajectories and Health Outcomes in the Longitudinal Assessment of Bariatric Surgery (LABS) Study. JAMA Surg. 2018, 153, 427–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, W.C.; Belle, S.H.; Hinerman, A.S.; Mitchell, J.E.; Steffen, K.J.; Courcoulas, A.P. Patient Behaviors and Characteristics Related to Weight Regain after Roux-En-Y Gastric Bypass: A Multicenter Prospective Cohort Study. Ann. Surg. 2020, 272, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Courcoulas, A.P.; Christian, N.J.; O’Rourke, R.W.; Dakin, G.; Dellinger, E.P.; Flum, D.R.; Kalarchian, M.; Mitchell, J.E.; Patterson, E.; Pomp, A.; et al. Preoperative Factors and Three Year Weight Change in the Longitudinal Assessment of Bariatric Surgery (LABS) Consortium. Surg. Obes. Relat. Dis. 2015, 11, 1109–1118. [Google Scholar] [CrossRef] [Green Version]
- Colles, S.L.; Dixon, J.B.; O’Brien, P.E. Grazing and Loss of Control Related to Eating: Two High-Risk Factors Following Bariatric Surgery. Obesity 2008, 16, 615–622. [Google Scholar] [CrossRef]
- Pinto-Bastos, A.; de Lourdes, M.; Brandão, I.; Machado, P.P.P.; Conceição, E.M. Weight Loss Trajectories and Psychobehavioral Predictors of Outcome of Primary and Reoperative Bariatric Surgery: A 2-Year Longitudinal Study. Surg. Obes. Relat. Dis. 2019, 15, 1104–1112. [Google Scholar] [CrossRef]
- Fouladi, F.; Carroll, I.M.; Sharpton, T.J.; Bulik-Sullivan, E.; Heinberg, L.; Steffen, K.; Fodor, A.A. A Microbial Signature Following Bariatric Surgery Is Robustly Consistent across Multiple Cohorts. medRxiv 2020. [Google Scholar] [CrossRef]
- Puzziferri, N.; Roshek, T.B., III; Mayo, H.G.; Gallagher, R.; Belle, S.H.; Livingston, E.H. Long-Term Follow-up after Bariatric Surgery: A Systematic Review. JAMA 2014, 312, 934–942. [Google Scholar] [CrossRef] [Green Version]
- Fouladi, F.; Brooks, A.E.; Fodor, A.A.; Carroll, I.M.; Bulik-Sullivan, E.C.; Tsilimigras, M.C.B.; Sioda, M.; Steffen, K.J. The Role of the Gut Microbiota in Sustained Weight Loss Following Roux-En-Y Gastric Bypass Surgery. Obes. Surg. 2019, 29, 1259–1267. [Google Scholar] [CrossRef] [Green Version]
- Marceau, P.; Hould, F.-S.; Simard, S.; Lebel, S.; Bourque, R.-A.; Potvin, M.; Biron, S. Biliopancreatic Diversion with Duodenal Switch. World J. Surg. 1998, 22, 947–954. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method Reduces Bias in the Collection of Energy Intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, C.; Spiegelman, D.; Rimm, E.B.; Rosner, B.A.; Stampfer, M.J.; Barnett, J.B.; Chavarro, J.E.; Rood, J.C.; Harnack, L.J.; Sampson, L.K.; et al. Relative Validity of Nutrient Intakes Assessed by Questionnaire, 24-Hour Recalls, and Diet Records as Compared with Urinary Recovery and Plasma Concentration Biomarkers: Findings for Women. Am. J. Epidemiol. 2018, 187, 1051–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, E.; Lee, C.; Imamura, F.; Hollidge, S.E.; Westgate, K.L.; Venables, M.C.; Poliakov, I.; Rowland, M.K.; Osadchiy, T.; Bradley, J.C.; et al. Validity and Reliability of an Online Self-Report 24-h Dietary Recall Method (Intake24): A Doubly Labelled Water Study and Repeated-Measures Analysis. J. Nutr. Sci. 2019, 8, e29. [Google Scholar] [CrossRef] [Green Version]
- Grivetti, L.E. Culture, Diet, and Nutrition: Selected Themes and Topics. BioScience 1978, 28, 171–177. [Google Scholar] [CrossRef]
- Inocian, E.P.; Nolfi, D.A.; Felicilda-Reynaldo, R.F.D.; Bodrick, M.M.; Aldohayan, A.; Kalarchian, M.A. Bariatric Surgery in the Middle East and North Africa: Narrative Review with Focus on Culture-Specific Considerations. Surg. Obes. Relat. Dis. 2021, 17, 1933–1941. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Timepoint | n | Weight (kg) | BMI (kg/m2) | Percent Loss (%) | EWL (%) |
|---|---|---|---|---|---|
| Baseline | 124 | 131.64 ± 25.21 | 45.93 ± 6.79 | - | - |
| RYGB—87 | 129.51 ± 21.58 | 45.28 ± 5.66 | - | - | |
| SG—37 | 136.66 ± 31.97 | 47.46 ± 8.82 | - | - | |
| Postop 1 month | 122 | 115.89 ± 22.41 | 40.52 ± 6.37 | 11.81 ± 3.44 | 27.32 ± 8.94 |
| RYGB—86 | 114.07 ± 18.46 | 39.9 ± 5.02 | 12.02 ± 3.4 | 27.77 ± 8.49 | |
| SG—36 | 120.23 ± 29.68 | 41.99 ± 8.72 | 11.31 ± 3.55 | 26.23 ± 9.96 | |
| Postop 6 months | 114 | 97.85 ± 20.93 | 34.37 ± 6.09 | 25.3 ± 5.95 | 58.32 ± 16.36 |
| RYGB—79 | 94.29 ± 15.76 | 33.26 ± 4.58 | 26.69 ± 5.66 *** | 61.53 ± 15.16 ** | |
| SG—35 | 105.88 ± 28.12 * | 36.88 ± 8.1 * | 22.15 ± 5.43 | 51.09 ± 16.88 | |
| Postop 12 months | 110 | 93.13 ± 21.66 | 32.69 ± 6.34 | 28.79 ± 7.99 | 66.51 ± 21.19 |
| RYGB—74 | 88.32 ± 16.32 | 31.12 ± 4.68 | 31 ± 7.29 *** | 71.85 ± 19.44 *** | |
| SG—36 | 103.02 ± 27.5 ** | 35.91 ± 7.99 ** | 24.23 ± 7.52 | 55.53 ± 20.64 | |
| Postop 18 months | 101 | 93.31 ± 21.76 | 32.73 ± 6.16 | 28.25 ± 8.48 | 65.46 ± 21.93 |
| RYGB—67 | 88.61 ± 17.32 | 31.21 ± 4.86 | 30.46 ± 8.57 *** | 70.81 ± 21.98 *** | |
| SG—34 | 102.58 ± 26.5 ** | 35.73 ± 7.32 ** | 23.89 ± 6.45 | 54.93 ± 17.86 | |
| Postop 24 months | 93 | 94.87 ± 21.64 | 33.36 ± 6.41 | 27.25 ± 9.26 | 62.59 ± 23.8 |
| RYGB—64 | 89.3 ± 17.45 | 31.62 ± 5.03 | 29.45 ± 9.01 *** | 68.47 ± 23.24 *** | |
| SG—29 | 107.18 ± 25 ** | 37.19 ± 7.5 ** | 22.42 ± 7.99 | 49.62 ± 19.82 |
| Responder | Suboptimal Responder | ||||
|---|---|---|---|---|---|
| (n = 85) | (n = 25) | R2 | p-Value | ||
| Baseline | Weight (kg) | 126.01 ± 21.13 | 146.67 ± 31.57 | 0.118 | 0.002 |
| Energy (kcal) | 1865.58 ± 842.97 | 1973.37 ± 756.42 | 0.003 | 0.392 | |
| Carbohydrates (g) | 198.29 ± 119.14 (43.7%) | 209.78 ± 101.33 (46.5%) | 0.002 | 0.448 | |
| Protein (g) | 109.6 ± 86.56 (27.7%) | 117.28 ± 70.75 (30.2%) | 0.002 | 0.267 | |
| Total fat (g) | 98.8 ± 94.24 (52.4%) | 111.46 ± 70.2 (62.8%) | 0.004 | 0.053 | |
| Postop | Weight (kg) | 110.27 ± 18.12 | 130.76 ± 29.13 | 0.143 | 0.001 |
| 1 month | Energy (kcal) | 668.69 ± 253.94 | 930.85 ± 295.61 | 0.148 | <0.001 |
| Carbohydrates (g) | 58.41 ± 50.72 (35.8%) | 79.96 ± 47.85 (33.5%) | 0.031 | 0.013 | |
| Protein (g) | 59.97 ± 45.52 (36.8%) | 64.17 ± 22.47 (28.9%) | 0.002 | 0.105 Δ | |
| Total fat (g) | 33.71 ± 44.01 (46.7%) | 39.33 ± 17.15 (37.5%) | 0.003 | 0.007 | |
| Postop | Weight (kg) | 91.35 ± 15.01 | 119.82 ± 25.38 | 0.311 | <0.001 |
| 6 months | Energy (kcal) | 1021.7 ± 427.11 | 1285.95 ± 458.12 | 0.06 | 0.009Δ |
| Carbohydrates (g) | 91.51 ± 63.07 (35.1%) | 110.9 ± 54.65 (34.4%) | 0.017 | 0.038Δ | |
| Protein (g) | 74.4 ± 53.24 (30.9%) | 76.09 ± 28.62 (24.0%) | <0.001 | 0.247 | |
| Total fat (g) | 50.88 ± 48.29 (45.0%) | 59.21 ± 25.22 (41.2%) | 0.006 | 0.017Δ | |
| Postop | Weight (kg) | 85.72 ± 14.63 | 118.35 ± 22.9 | 0.402 | <0.001 |
| 12 months | Energy (kcal) | 1156.08 ± 416.19 | 1436.55 ± 466.82 | 0.072 | 0.018Δ |
| Carbohydrates (g) | 110.25 ± 61.81 (36.8%) | 116.61 ± 58.31 (31.1%) | 0.002 | 0.685 Δ | |
| Protein (g) | 71.27 ± 36.12 (26.0%) | 85.48 ± 24.49 (25.1%) | 0.031 | 0.002Δ | |
| Total fat (g) | 52.42 ± 33.14 (40.6%) | 66.43 ± 25.31 (41.5%) | 0.034 | 0.005Δ |
| Responder | Suboptimal Responder | ||||
|---|---|---|---|---|---|
| (n = 64) | (n = 29) | R2 | p-Value | ||
| Baseline | Weight (kg) | 126.81 ± 19.42 | 138.62 ± 32.7 | 0.049 | 0.121 |
| Energy (kcal) | 1807.96 ± 681.19 | 1820.37 ± 762.13 | <0.001 | 0.879 | |
| Carbohydrates (g) | 179.03 ± 81.77 (38.7%) | 222.75 ± 161.77 (53%) | 0.032 | 0.673 | |
| Protein (g) | 91.19 ± 28.57 (21.8%) | 141.41 ± 141 (38.3%) | 0.077 | 0.167 | |
| Total fat (g) | 76.24 ± 31.16 (37.7%) | 133.3 ± 142.57 (79.2%) | 0.094 | 0.048 | |
| Postop | Weight (kg) | 110.99 ± 16.18 | 124.25 ± 30.1 | 0.077 | 0.042 |
| 1 month | Energy (kcal) | 676.96 ± 263.61 | 833.98 ± 291.5 | 0.068 | 0.011 |
| Carbohydrates (g) | 58.46 ± 49.11 (34.8%) | 69.71 ± 41.96 (32.8%) | 0.012 | 0.094 | |
| Protein (g) | 58.87 ± 42.55 (36.9%) | 62.09 ± 24.22 (30.4%) | 0.002 | 0.229 Δ | |
| Total fat (g) | 32.14 ± 41.13 (45%) | 34.11 ± 15.19 (36.6%) | 0.001 | 0.091 | |
| Postop | Weight (kg) | 92 ± 14.54 | 110.37 ± 27.77 | 0.162 | <0.001 |
| 6 months | Energy (kcal) | 1016.07 ± 434.96 | 1206.94 ± 488.45 | 0.037 | 0.053 Δ |
| Carbohydrates (g) | 90.74 ± 67.43 (35.1%) | 99.74 ± 53.14 (33%) | 0.004 | 0.205 Δ | |
| Protein (g) | 77.92 ± 60.31 (32.5%) | 75.54 ± 31.86 (25.5%) | <0.001 | 0.39 | |
| Total fat (g) | 53.3 ± 55.04 (47.7%) | 54.91 ± 26.24 (40.2%) | <0.001 | 0.086 Δ | |
| Postop | Weight (kg) | 85.46 ± 14.82 | 109.01 ± 26.16 | 0.252 | <0.001 |
| 12 months | Energy (kcal) | 1143.68 ± 426.09 | 1338 ± 476.48 | 0.04 | 0.141 Δ |
| Carbohydrates (g) | 108.7 ± 66.45 (36.3%) | 109.96 ± 57.76 (31.6%) | <0.001 | 0.905 Δ | |
| Protein (g) | 72.11 ± 38.97 (26.9%) | 84.65 ± 25.65 (26.9%) | 0.026 | 0.005Δ | |
| Total fat (g) | 52.15 ± 36.69 (40.8%) | 61.4 ± 27.24 (40.8%) | 0.016 | 0.109 Δ | |
| Postop | Weight (kg) | 85.99 ± 14.88 | 110.35 ± 24.31 | 0.28 | <0.001 |
| 18 months | Energy (kcal) | 1261.91 ± 498.21 | 1364.14 ± 530.58 | 0.009 | 0.467 |
| Carbohydrates (g) | 121.91 ± 61.32 (37.4%) | 121.67 ± 60.63 (35.3%) | <0.001 | 0.754 | |
| Protein (g) | 65.56 ± 21.83 (22.7%) | 84.3 ± 28.94 (25.2%) | 0.115 | 0.003 | |
| Total fat (g) | 53.67 ± 23.26 (38.3%) | 59.44 ± 25.43 (39.1%) | 0.012 | 0.402 | |
| Postop | Weight (kg) | 86.36 ± 14.77 | 113.67 ± 22.7 | 0.346 | <0.001 |
| 24 months | Energy (kcal) | 1218.42 ± 472.41 | 1296.49 ± 542.18 | 0.005 | 0.451 |
| Carbohydrates (g) | 116.14 ± 62.55 (39.9%) | 121.33 ± 71.11 (36.3%) | 0.001 | 0.808 | |
| Protein (g) | 75.65 ± 41.86 (28.6%) | 71.23 ± 22.48 (23.9%) | 0.003 | 0.976 | |
| Total fat (g) | 56.64 ± 43.52 (47.6%) | 53.28 ± 21.87 (38%) | 0.002 | 0.724 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorgen, A.A.; Fodor, A.A.; Steffen, K.J.; Carroll, I.M.; Bond, D.S.; Crosby, R.; Heinberg, L.J. Longer-Term Weight Loss Outcomes Are Not Primarily Driven by Diet Following Roux-en-Y Gastric Bypass and Sleeve Gastrectomy. Nutrients 2023, 15, 3323. https://doi.org/10.3390/nu15153323
Sorgen AA, Fodor AA, Steffen KJ, Carroll IM, Bond DS, Crosby R, Heinberg LJ. Longer-Term Weight Loss Outcomes Are Not Primarily Driven by Diet Following Roux-en-Y Gastric Bypass and Sleeve Gastrectomy. Nutrients. 2023; 15(15):3323. https://doi.org/10.3390/nu15153323
Chicago/Turabian StyleSorgen, Alicia A., Anthony A. Fodor, Kristine J. Steffen, Ian M. Carroll, Dale S. Bond, Ross Crosby, and Leslie J. Heinberg. 2023. "Longer-Term Weight Loss Outcomes Are Not Primarily Driven by Diet Following Roux-en-Y Gastric Bypass and Sleeve Gastrectomy" Nutrients 15, no. 15: 3323. https://doi.org/10.3390/nu15153323