

Association between Vitamin D Deficiency and Clinical Parameters in Men and Women Aged 50 Years or Older: A Cross-Sectional Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
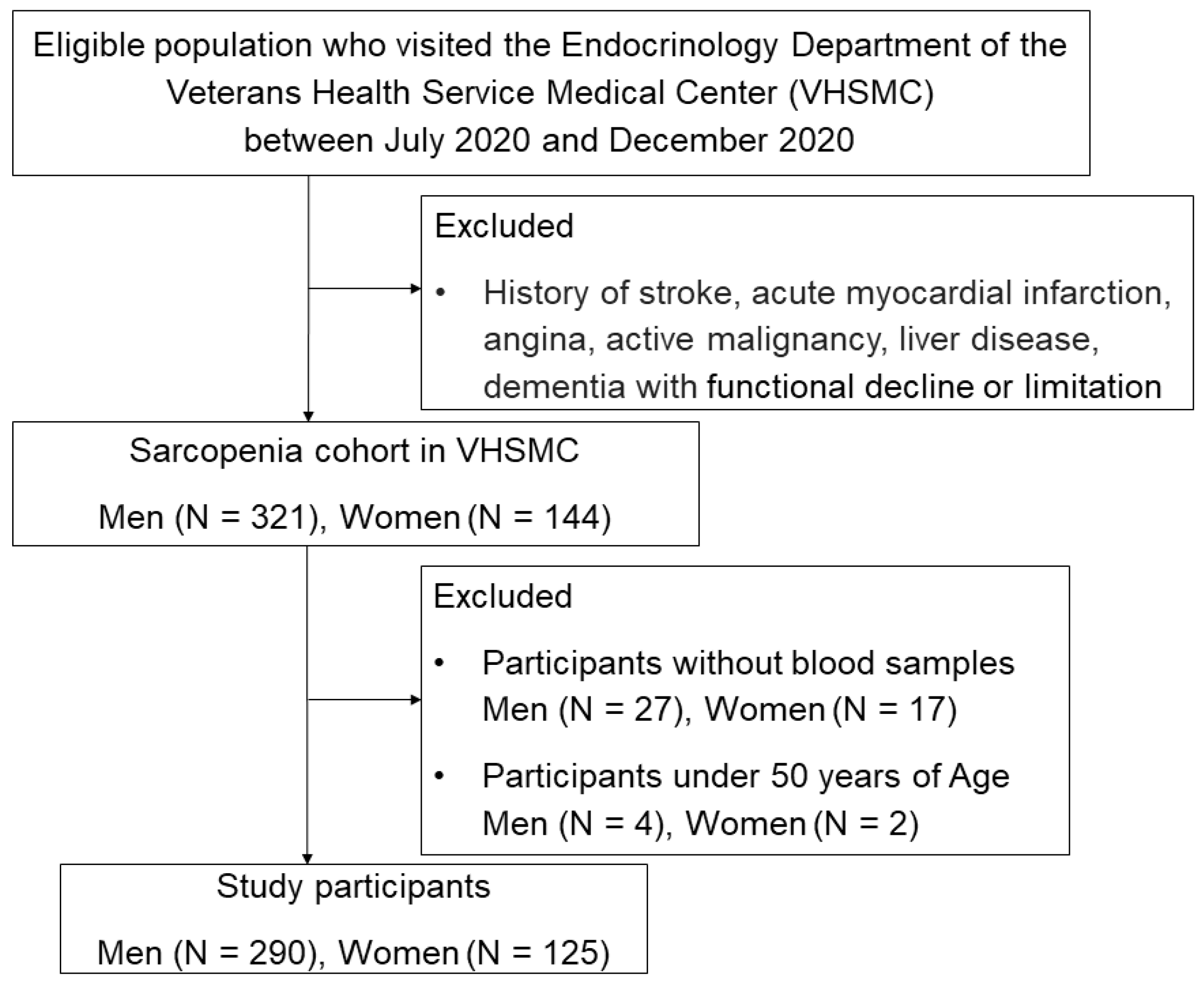
2.1. Participants and Study Design
2.2. Laboratory Tests
2.3. Covariates Assessment
2.4. Assessment of Sarcopenia
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Study Participants
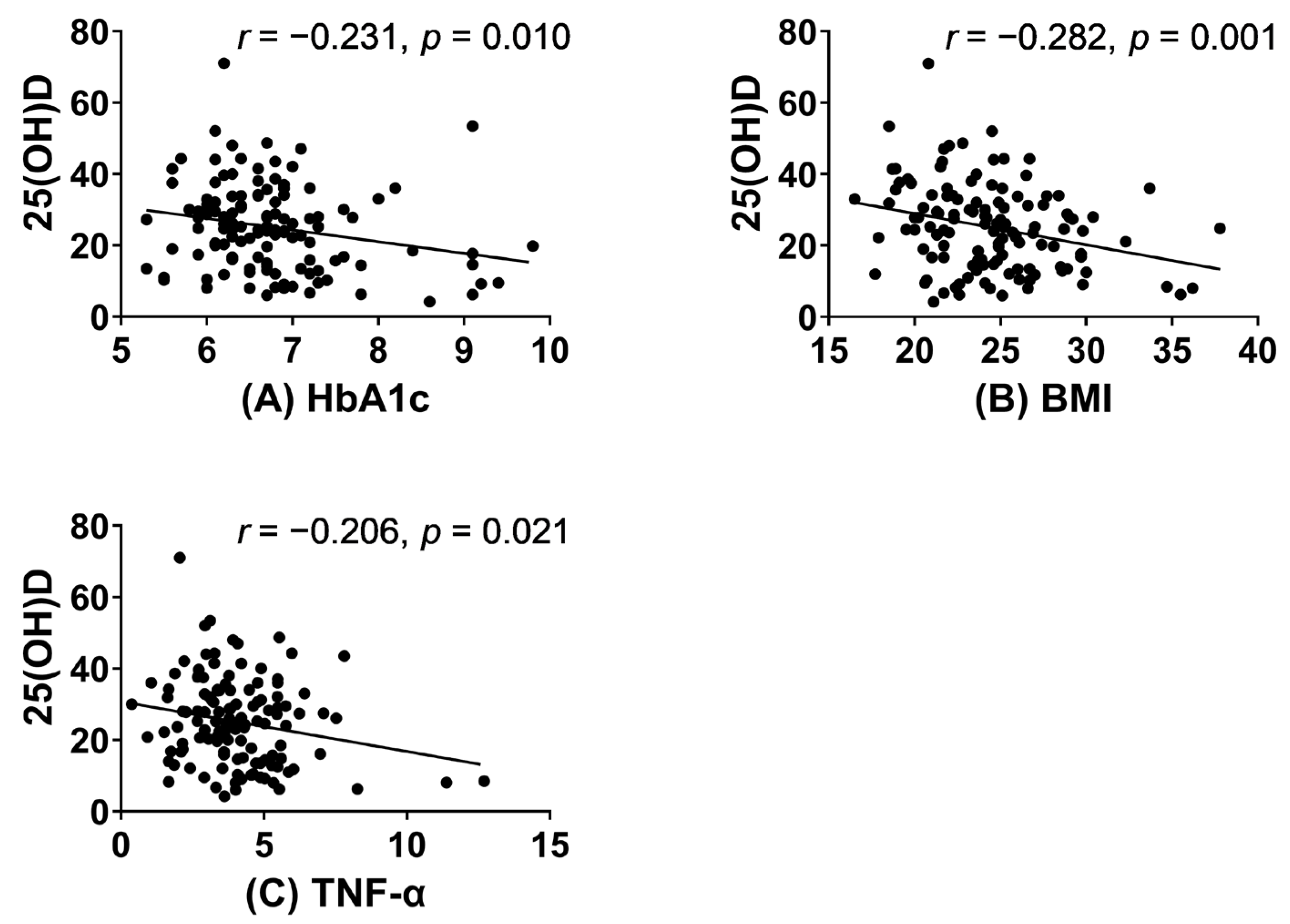
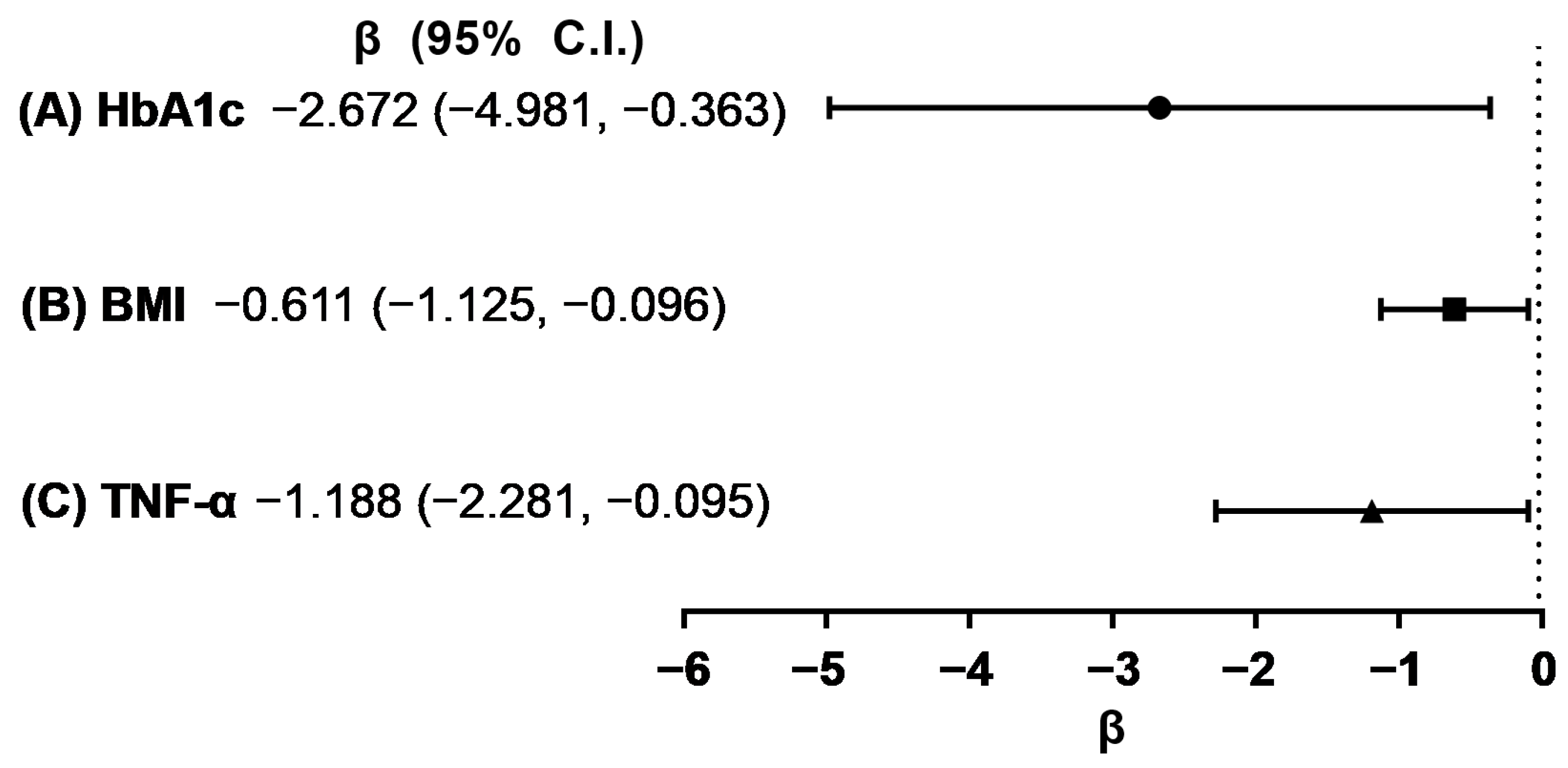
3.2. Association between Vitamin D and Clinical Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Institute of Medicine Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. The National Academies Collection: Reports funded by National Institutes of Health. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academies Press (US), National Academy of Sciences: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D Status and Ill Health: A Systematic Review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef]
- Pittas, A.G.; Lau, J.; Hu, F.B.; Dawson-Hughes, B. The Role of Vitamin D and Calcium in Type 2 Diabetes. A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2007, 92, 2017–2029. [Google Scholar] [CrossRef] [Green Version]
- Forouhi, N.G.; Luan, J.a.; Cooper, A.; Boucher, B.J.; Wareham, N.J. Baseline Serum 25-Hydroxy Vitamin D Is Predictive of Future Glycemic Status and Insulin Resistance: The Medical Research Council Ely Prospective Study 1990–2000. Diabetes 2008, 57, 2619–2625. [Google Scholar] [CrossRef] [Green Version]
- Aly, Y.E.; Abdou, A.S.; Rashad, M.M.; Nassef, M.M. Effect of Exercise on Serum Vitamin D and Tissue Vitamin D Receptors in Experimentally Induced Type 2 Diabetes Mellitus. J. Adv. Res. 2016, 7, 671–679. [Google Scholar] [CrossRef] [Green Version]
- Mousa, A.; Naderpoor, N.; Teede, H.J.; De Courten, M.; Scragg, R.; De Courten, B. Vitamin D and Cardiometabolic Risk Factors and Diseases. Minerva Endocrinol. 2015, 40, 213–230. [Google Scholar]
- Walsh, J.S.; Bowles, S.; Evans, A.L. Vitamin D in Obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 389–394. [Google Scholar] [CrossRef] [PubMed]
- McKibben, R.A.; Zhao, D.; Lutsey, P.L.; Schneider, A.L.; Guallar, E.; Mosley, T.H.; Michos, E.D. Factors Associated With Change in 25-Hydroxyvitamin D Levels Over Longitudinal Follow-up in the ARIC Study. J. Clin. Endocrinol. Metab. 2016, 101, 33–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenstreich, S.J.; Rich, C.; Volwiler, W. Deposition in and Release of Vitamin D3 From Body Fat: Evidence for a Storage Site in the Rat. J. Clin. Investig. 1971, 50, 679–687. [Google Scholar] [CrossRef] [Green Version]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased Bioavailability of Vitamin D in Obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Etten, E.; Mathieu, C. Immunoregulation by 1, 25-Dihydroxyvitamin D3: Basic Concepts. J. Steroid Biochem. Mol. Biol. 2005, 97, 93–101. [Google Scholar] [CrossRef]
- Helming, L.; Böse, J.; Ehrchen, J.; Schiebe, S.; Frahm, T.; Geffers, R.; Probst-Kepper, M.; Balling, R.; Lengeling, A. 1α, 25-Dihydroxyvitamin D3 Is a Potent Suppressor of Interferon γ–Mediated Macrophage Activation. Blood 2005, 106, 4351–4358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halim, C.; Mirza, A.F.; Sari, M.I. The Association Between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 195. [Google Scholar] [CrossRef]
- Lee, B.-N.-R.; Kim, T.-H.; Jun, J.-B.; Yoo, D.-H.; Woo, J.-H.; Choi, S.J.; Lee, Y.H.; Song, G.G.; Kim, Y.; Lee, J.Y.; et al. Upregulation of Interleukin-1β Production by 1,25-Dihydroxyvitamin D3 in Activated Human Macrophages. Mol. Biol. Rep. 2011, 38, 2193–2201. [Google Scholar] [CrossRef] [PubMed]
- Botelho, I.M.B.; Neto, A.M.; Silva, C.A.; Tambascia, M.A.; Alegre, S.M.; Zantut-Wittmann, D.E. Vitamin D in Hashimoto’s Thyroiditis and Its Relationship With Thyroid Function and Inflammatory Status. Endocr. J. 2018, 65, 1029–1037. [Google Scholar] [CrossRef] [Green Version]
- Komisarenko, Y.I.; Bobryk, M.I. Vitamin D Deficiency and Immune Disorders in Combined Endocrine Pathology. Front. Endocrinol. 2018, 9, 600. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Tian, L.; Xiao, Y.; Huang, G.; Zhang, M. Effect of vitamin D supplementation on some inflammatory biomarkers in type 2 diabetes mellitus subjects: A systematic review and meta-analysis of randomized controlled trials. Ann Nutr Metab. 2018, 73, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Ke, W.; Sun, T.; Zhang, Y.; He, L.; Wu, Q.; Liu, J.; Zha, B. 25-Hydroxyvitamin D Serum Level in Hashimoto’s Thyroiditis, but Not Graves’ Disease Is Relatively Deficient. Endocr. J. 2017, 64, 581–587. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.A.; Lee, S.H.; Koh, J.M.; Kwon, S.h.; Lee, Y.; Cho, H.J.; Kim, H.; Kim, S.J.; Lee, J.H.; Yoo, H.J. Fatty Acid Amides as Potential Circulating Biomarkers for Sarcopenia. J. Cachexia Sarcopenia Muscle 2023, 14, 1558–1568. [Google Scholar] [CrossRef]
- Zanin-Silva, D.C.; Santana-Gonçalves, M.; Kawashima-Vasconcelos, M.Y.; Lima-Júnior, J.R.; Dias, J.B.E.; Moraes, D.A.; Covas, D.T.; Malmegrim, K.C.R.; Ramalho, L.; Oliveira, M.C. Autologous Hematopoietic Stem Cell Transplantation Promotes Connective Tissue Remodeling in Systemic Sclerosis Patients. Arthritis Res. Ther. 2022, 24, 95. [Google Scholar] [CrossRef]
- Florkowski, C.M.; Chew-Harris, J.S. Methods of Estimating GFR—Different Equations Including CKD-EPI. Clin. Biochem. Rev. 2011, 32, 75–79. [Google Scholar]
- Ryu, J.Y.; Kim, M.; Kim, K.S.; Kim, S.; Won, C.W. Chair Stand Test as a Proxy for Physical Performance and Muscle Strength in Sarcopenia Diagnosis: The Korean Frailty and Aging Cohort Study. Aging Clin. Exp. Res. 2022, 34, 2449–2456. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Niroomand, M.; Fotouhi, A.; Irannejad, N.; Hosseinpanah, F. Does High-Dose Vitamin D Supplementation Impact Insulin Resistance and Risk of Development of Diabetes in Patients With Pre-diabetes? A Double-Blind Randomized Clinical Trial. Diabetes Res. Clin. Pract. 2019, 148, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kositsawat, J.; Freeman, V.L.; Gerber, B.S.; Geraci, S. Association of A1C Levels With Vitamin D Status in US Adults: Data From the National Health and Nutrition Examination Survey. Diabetes Care 2010, 33, 1236–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Wang, F.; Jia, Y.; Guo, F.; Chen, S. The Relationship Between Hemoglobin Glycation Variation Index and Vitamin D in Type 2 Diabetes Mellitus. Diabetes Metab. Syndr. Obes. 2021, 14, 1937–1948. [Google Scholar] [CrossRef]
- Maestro, B.; Dávila, N.; Carranza, M.C.; Calle, C. Identification of a Vitamin D Response Element in the Human Insulin Receptor Gene Promoter. J. Steroid Biochem. Mol. Biol. 2003, 84, 223–230. [Google Scholar] [CrossRef]
- Manna, P.; Achari, A.E.; Jain, S.K. Vitamin D Supplementation Inhibits Oxidative Stress and Upregulate SIRT1/AMPK/GLUT4 Cascade in High Glucose-Treated 3T3L1 Adipocytes and in Adipose Tissue of High Fat Diet-Fed Diabetic Mice. Arch. Biochem. Biophys. 2017, 615, 22–34. [Google Scholar] [CrossRef]
- Narvaez, C.J.; Simmons, K.M.; Brunton, J.; Salinero, A.; Chittur, S.V.; Welsh, J.E. Induction of STEAP4 Correlates With 1,25-Dihydroxyvitamin D3 Stimulation of Adipogenesis in Mesenchymal Progenitor Cells Derived From Human Adipose Tissue. J. Cell Physiol. 2013, 228, 2024–2036. [Google Scholar] [CrossRef] [PubMed]
- Saneei, P.; Salehi-Abargouei, A.; Esmaillzadeh, A. Serum 25-Hydroxy Vitamin D Levels in Relation to Body Mass Index: A Systematic Review and Meta-Analysis. Obes. Rev. 2013, 14, 393–404. [Google Scholar] [CrossRef] [PubMed]
- Oliai Araghi, S.; van Dijk, S.C.; Ham, A.C.; Brouwer-Brolsma, E.M.; Enneman, A.W.; Sohl, E.; Swart, K.M.; van der Zwaluw, N.L.; van Wijngaarden, J.P.; Dhonukshe-Rutten, R.A.; et al. BMI and Body Fat Mass Is Inversely Associated with Vitamin D Levels in Older Individuals. J. Nutr. Health Aging 2015, 19, 980–985. [Google Scholar] [CrossRef]
- Marcotorchino, J.; Gouranton, E.; Romier, B.; Tourniaire, F.; Astier, J.; Malezet, C.; Amiot, M.J.; Landrier, J.F. Vitamin D Reduces the Inflammatory Response and Restores Glucose Uptake in Adipocytes. Mol. Nutr. Food Res. 2012, 56, 1771–1782. [Google Scholar] [CrossRef] [PubMed]
- Kolb, H.; Mandrup-Poulsen, T. An Immune Origin of Type 2 Diabetes? Diabetologia 2005, 48, 1038–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, C.A.; Heffernan, M.E. Serum Tumor Necrosis Factor-Alpha Concentrations Are Negatively Correlated With Serum 25 (OH) D Concentrations in Healthy Women. J. Inflamm. 2008, 5, 10. [Google Scholar] [CrossRef] [Green Version]
- Tiwari, S.; Pratyush, D.D.; Gupta, S.K.; Singh, S.K. Vitamin D Deficiency Is Associated With Inflammatory Cytokine Concentrations in Patients With Diabetic Foot Infection. Br. J. Nutr. 2014, 112, 1938–1943. [Google Scholar] [CrossRef]
- Orrù, B.; Szekeres-Bartho, J.; Bizzarri, M.; Spiga, A.M.; Unfer, V. Inhibitory Effects of Vitamin D on Inflammation and Il-6 Release. A Further Support for COVID-19 Management? Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 8187–8193. [Google Scholar] [CrossRef] [PubMed]
- Inanir, A.; Özoran, K.; Tutkak, H.; Mermerci, B. The Effects of Calcitriol Therapy on Serum Interleukin-1, Interleukin-6 and Tumour Necrosis Factor-α Concentrations in Post-menopausal Patients With Osteoporosis. J. Int. Med. Res. 2004, 32, 570–582. [Google Scholar] [CrossRef]
- Colotta, F.; Jansson, B.; Bonelli, F. Modulation of Inflammatory and Immune Responses by Vitamin D. J. Autoimmun. 2017, 85, 78–97. [Google Scholar] [CrossRef] [PubMed]
- Mohan, M.; Cherian, J.J.; Sharma, A. Exploring Links Between Vitamin D Deficiency and COVID-19. PLoS Pathog. 2020, 16, e1008874. [Google Scholar] [CrossRef]
- Popa, C.; Netea, M.G.; van Riel, P.L.; van der Meer, J.W.; Stalenhoef, A.F. The Role of TNF-alpha in Chronic Inflammatory Conditions, Intermediary Metabolism, and Cardiovascular Risk. J. Lipid Res. 2007, 48, 751–762. [Google Scholar] [CrossRef] [Green Version]
- Cantorna, M.T. Vitamin D and Autoimmunity: Is Vitamin D Status an Environmental Factor Affecting Autoimmune Disease Prevalence? Proc. Soc. Exp. Biol. Med. 2000, 223, 230–233. [Google Scholar] [CrossRef]
- Cantorna, M.T.; Zhu, Y.; Froicu, M.; Wittke, A. Vitamin D Status, 1,25-Dihydroxyvitamin D3, and the Immune System. Am. J. Clin. Nutr. 2004, 80, 1717s–1720s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantorna, M.T.; Mahon, B.D. D-Hormone and the Immune System. J. Rheumatol. Suppl. 2005, 76, 11–20. [Google Scholar]
- Jones, S.A.; Jenkins, B.J. Recent Insights Into Targeting the Il-6 Cytokine Family in Inflammatory Diseases and Cancer. Nat. Rev. Immunol. 2018, 18, 773–789. [Google Scholar] [CrossRef] [PubMed]
- Kotsiou, O.S.; Siachpazidou, D.I.; Pastaka, C.; Gogou, E.; Stavrou, V.; Kechagia, M.; Varsamas, C.; Hatzoglou, C.; Gourgoulianis, K.I. Association Between Interleukin-6 and Vitamin D Serum Levels in Patients With Obstructive Sleep Apnea Syndrome and Impact of Long-Term Continuous Positive Airway Pressure Therapy on Biomarker Levels. Respir. Physiol. Neurobiol. 2022, 296, 103806. [Google Scholar] [CrossRef] [PubMed]
- Houston, D.K.; Cesari, M.; Ferrucci, L.; Cherubini, A.; Maggio, D.; Bartali, B.; Johnson, M.A.; Schwartz, G.G.; Kritchevsky, S.B. Association Between Vitamin D Status and Physical Performance: The InCHIANTI Study. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Annweiler, C.; Beauchet, O.; Berrut, G.; Fantino, B.; Bonnefoy, M.; Herrmann, F.; Schott, A. Is There an Association Between Serum 25-Hydroxyvitamin D Concentration and Muscle Strength Among Older Women? Results From Baseline Assessment of the EPIDOS Study. J. Nutr. Health Aging 2009, 13, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Dwyer, T.; Hynes, K.L.; Parameswaran, V.; Greenaway, T.M. Vitamin D Insufficiency in Adolescent Males in Southern Tasmania: Prevalence, Determinants, and Relationship to Bone Turnover Markers. Osteoporos. Int. 2005, 16, 636–641. [Google Scholar] [CrossRef]
- Scott, D.; Blizzard, L.; Fell, J.; Ding, C.; Winzenberg, T.; Jones, G. A Prospective Study of the Associations Between 25-Hydroxy-Vitamin D, Sarcopenia Progression and Physical Activity in Older Adults. Clin. Endocrinol. 2010, 73, 581–587. [Google Scholar] [CrossRef]
- Herrick, K.A.; Storandt, R.J.; Afful, J.; Pfeiffer, C.M.; Schleicher, R.L.; Gahche, J.J.; Potischman, N. Vitamin D Status in the United States, 2011–2014. Am. J. Clin. Nutr. 2019, 110, 150–157. [Google Scholar] [CrossRef]
- Mogire, R.M.; Mutua, A.; Kimita, W.; Kamau, A.; Bejon, P.; Pettifor, J.M.; Adeyemo, A.; Williams, T.N.; Atkinson, S.H. Prevalence of Vitamin D Deficiency in Africa: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2020, 8, e134–e142. [Google Scholar] [CrossRef] [Green Version]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D Deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, K.; Kitamura, K.; Takachi, R.; Saito, T.; Kobayashi, R.; Oshiki, R.; Watanabe, Y.; Tsugane, S.; Sasaki, A.; Yamazaki, O. Impact of Demographic, Environmental, and Lifestyle Factors on Vitamin D Sufficiency in 9084 Japanese Adults. Bone 2015, 74, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Hu, J.; Fang, Y.; Wang, P.; Lu, Y.; Shen, N. Vitamin D status in Mainland of China: A Systematic Review and Meta-Analysis. EClinicalMedicine 2021, 38, 101017. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Zhu, A.; Ji, J.S. A Comparison Study of Vitamin D Deficiency among Older Adults in China and the United States. Sci. Rep. 2019, 9, 19713. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.A.; Yoon, J.W.; Lee, Y.; Choi, H.J.; Yun, J.W.; Bae, E.; Kwon, S.H.; Ahn, S.E.; Do, A.R.; Jin, H.; et al. Unveiling Genetic Variants Underlying Vitamin D Deficiency in Multiple Korean Cohorts by a Genome-Wide Association Study. Endocrinol. Metab. 2021, 36, 1189–1200. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.W.; Shin, H.T.; Seo, J. Risk Allele Frequency Analysis of Single-Nucleotide Polymorphisms for Vitamin D Concentrations in Different Ethnic Group. Genes 2021, 12, 1530. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Men (n = 290) | Women (n = 125) |
|---|---|---|
| Age (years) | 72.7 ± 6.1 | 70.1 ± 5.9 |
| Weight (kg) | 65.2 ± 9.3 | 58.1 ± 9.7 |
| Height (cm) | 166.1 ± 5.6 | 154.3 ± 4.8 |
| BMI (kg/m2) | 23.6 ± 2.9 | 24.5 ± 3.9 |
| 25(OH) D (ng/mL) | 18.1 ± 10.6 | 25.1 ± 12.1 |
| 25(OH) D < 20, n (%) | 187 (64.5) | 44 (35.2) |
| Exercise, n (%) | 197 (67.9%) | 86 (68.8) |
| Alcohol drinking, n (%) | 145 (50.0%) | 19 (15.2) |
| Current smoker, n (%) | 52 (17.9%) | 2 (1.6) |
| Vitamin D replacement, n (%) | 97 (33.4%) | 59 (47.2) |
| Diabetes mellitus, n (%) | 283 (97.6) | 107 (85.6) |
| Hand grip strength (kg) | 29.4 ± 6.6 | 19.9 ± 4.4 |
| Chair stand test (s) | 5.0 ± 2.6 | 4.9 ± 3.2 |
| Fat mass (kg) | 17.3 ± 5.6 | 21.5 ± 6.6 |
| Percent fat mass (%) | 25.9 ± 5.8 | 35.7 ± 5.8 |
| Lean mass (kg) | 45.6 ± 5.3 | 35.4 ± 4.2 |
| ASM (kg) | 20.2 ±2.8 | 14.7 ±2.3 |
| SMI (kg/m2) | 7.3 [6.8; 7.8] | 6.0 [5.6; 6.7] |
| Sarcopenia, n (%) | 79 (27.2) | 45 (36.0) |
| SARC-F | 0.0 [0.0; 1.0] | 1.0 [0.0; 2.0] |
| EQ-VAS | 70.0 [60.0; 80.0] | 70.0 [60.0; 80.0] |
| HbA1c (NGSP) (%) | 6.9 ± 0.9 | 6.8 ± 0.9 |
| TNF-α (pg/mL) | 4.7 ± 2.0 | 4.1 ± 1.8 |
| IL-6 (pg/mL) | 2.1 ± 3.2 | 1.5 ± 1.6 |
| IL-1β (pg/mL) | 4.7 ± 2.0 | 5.7 ± 1.4 |
| Creatinine (mg/dL) | 1.0 ± 0.5 | 0.8 ± 0.2 |
| CKD-EPI eGFR (mL/min/1.73 m2) | 87.4 ± 6.9 | 103.4 ± 18.7 |
| Men | Women | |||||
|---|---|---|---|---|---|---|
| 25(OH)D ≥ 20 (n = 103) | 25(OH)D < 20 (n = 187) | p-Value | 25(OH)D ≥ 20 (n = 81) | 25(OH)D < 20 (n = 44) | p-Value | |
| Age (years) | 72.7 ± 6.3 | 72.7 ± 5.9 | ns | 69.5 ± 5.7 | 71.2 ± 6.0 | ns |
| Weight (kg) | 64.1 ± 8.5 | 65.8 ± 9.6 | ns | 57.0 ± 9.3 | 60.1 ± 10.4 | ns |
| Height (cm) | 166.0 ± 5.4 | 166.1± 5.7 | ns | 154.6 ± 5.0 | 153.7 ± 4.6 | ns |
| BMI (kg/m2) | 23.2 ± 2.8 | 23.8 ± 2.9 | ns | 23.9 ± 3.8 | 25.4 ± 4.0 | * |
| 25(OH)D (ng/mL) | 30.0 ± 8.5 | 11.6 ± 3.7 | – | 32.0 ± 9.1 | 12.4 ± 4.1 | – |
| Exercise (≥3/wk), n(%) | 69 (67.0%) | 128 68.4%) | ns | 61 (75.3) | 25 (56.8) | * |
| Alcohol drinking, n (%) | 55 (53.4%) | 90 (48.1%) | ns | 16 (19.8) | 3 (6.8) | ns |
| Current smoker, n (%) | 15 (14.6%) | 37 (19.8%) | ns | 0 (0) | 2 (4.5) | ns |
| Vitamin D replacement, n (%) | 51 (49.5%) | 46 (24.6%) | *** | 49 (60.5) | 10 (22.7) | *** |
| Diabetes mellitus, n (%) | 100 (97.1%) | 183 (97.9%) | ns | 67 (82.7) | 40 (90.9) | ns |
| Hypertension, n (%) | 64 (62.1) | 112 (59.9) | ns | 41 (50.6) | 25 (56.8) | ns |
| Hand grip strength (kg) | 30.4 ± 6.1 | 28.8 ± 6.9 | * | 20.3 ± 4.0 | 19.2 ± 4.9 | ns |
| Chair stand test (s) | 5.5 ± 2.4 | 4.8 ± 2.6 | * | 5.1 ± 3.1 | 4.4 ± 3.4 | ns |
| Fat mass (kg) | 16.2 ± 5.4 | 17.9 ± 5.6 | * | 20.8 ± 6.2 | 22.8 ± 7.2 | ns |
| Percent fat mass (%) | 24.8 ± 5.8 | 26.6 ± 5.7 | * | 35.1 ± 5.7 | 36.7 ± 5.8 | ns |
| Lean mass (kg) | 45.6 ± 5.0 | 45.6 ± 5.4 | ns | 35.0 ± 4.1 | 36.1 ± 4.3 | ns |
| ASM (kg) | 20.2 ± 2.6 | 20.3 ± 2.9 | ns | 14.5 ± 2.3 | 15.0 ±2.4 | ns |
| SMI (kg/m2) | 7.3 [6.9; 7.8] | 7.3 [6.8; 7.8] | ns | 6.0 [5.5; 6.7] | 6.3 [5.7; 6.9] | ns |
| Sarcopenia, n (%) | 32 (31.1%) | 47 (25.1%) | ns | 34 (42.0) | 11 (25.0) | ns |
| SARC-F | 0.0 [0.0; 1.0] | 0.0 [0.0; 1.0] | ns | 1.0 [0.0; 2.0] | 1.0 [0.0; 2.0] | ns |
| EQ-VAS | 70 [60; 80] | 70 [55; 80] | ns | 70 [60; 80] | 70 [50; 80] | ns |
| HbA1c (NGSP) (%) | 6.8 ± 0.8 | 7.0 ± 1.0 | * | 6.6 ± 0.6 | 7.1 ± 1.1 | *** |
| TNF-α (pg/mL) | 4.6 ± 2.2 | 4.7 ± 2.0 | ns | 3.8 ± 1.5 | 4.6 ± 2.2 | * |
| IL-6 (pg/mL) | 2.7 ± 5.0 | 1.7 ± 1.2 | ns | 5.7 ± 1.3 | 5.6 ±1.5 | ns |
| IL-1β (pg/mL) | 5.4 ± 1.6 | 5.3 ± 1.6 | ns | 1.5 ± 1.9 | 1.5 ± 0.9 | ns |
| Creatinine (mg/dl) | 1.0 ± 0.3 | 1.0 ± 0.5 | ns | 0.7 ± 0.1 | 0.8 ± 0.3 | * |
| CKD-EPI eGFR (mL/min/1.73 m2) | 87.2 ± 6.8 | 87.6 ± 7.0 | ns | 107.0 ± 14.6 | 96.8 ± 23.2 | * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.H.; Kim, Y.A.; Kim, Y.S.; Lee, Y.; Seo, J.H. Association between Vitamin D Deficiency and Clinical Parameters in Men and Women Aged 50 Years or Older: A Cross-Sectional Cohort Study. Nutrients 2023, 15, 3043. https://doi.org/10.3390/nu15133043
Lee JH, Kim YA, Kim YS, Lee Y, Seo JH. Association between Vitamin D Deficiency and Clinical Parameters in Men and Women Aged 50 Years or Older: A Cross-Sectional Cohort Study. Nutrients. 2023; 15(13):3043. https://doi.org/10.3390/nu15133043
Chicago/Turabian StyleLee, Ji Hyun, Ye An Kim, Young Sik Kim, Young Lee, and Je Hyun Seo. 2023. "Association between Vitamin D Deficiency and Clinical Parameters in Men and Women Aged 50 Years or Older: A Cross-Sectional Cohort Study" Nutrients 15, no. 13: 3043. https://doi.org/10.3390/nu15133043