
Interventions for Picky Eaters among Typically Developed Children—A Scoping Review
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Stage 1—Identify the Research Question
- What are the key concepts (focusing on the types of intervention and the most common approaches) applied in intervention programs for PE children?
- What are the reported outcomes of the interventions?
2.2. Stage 2—Identify Relevant Studies
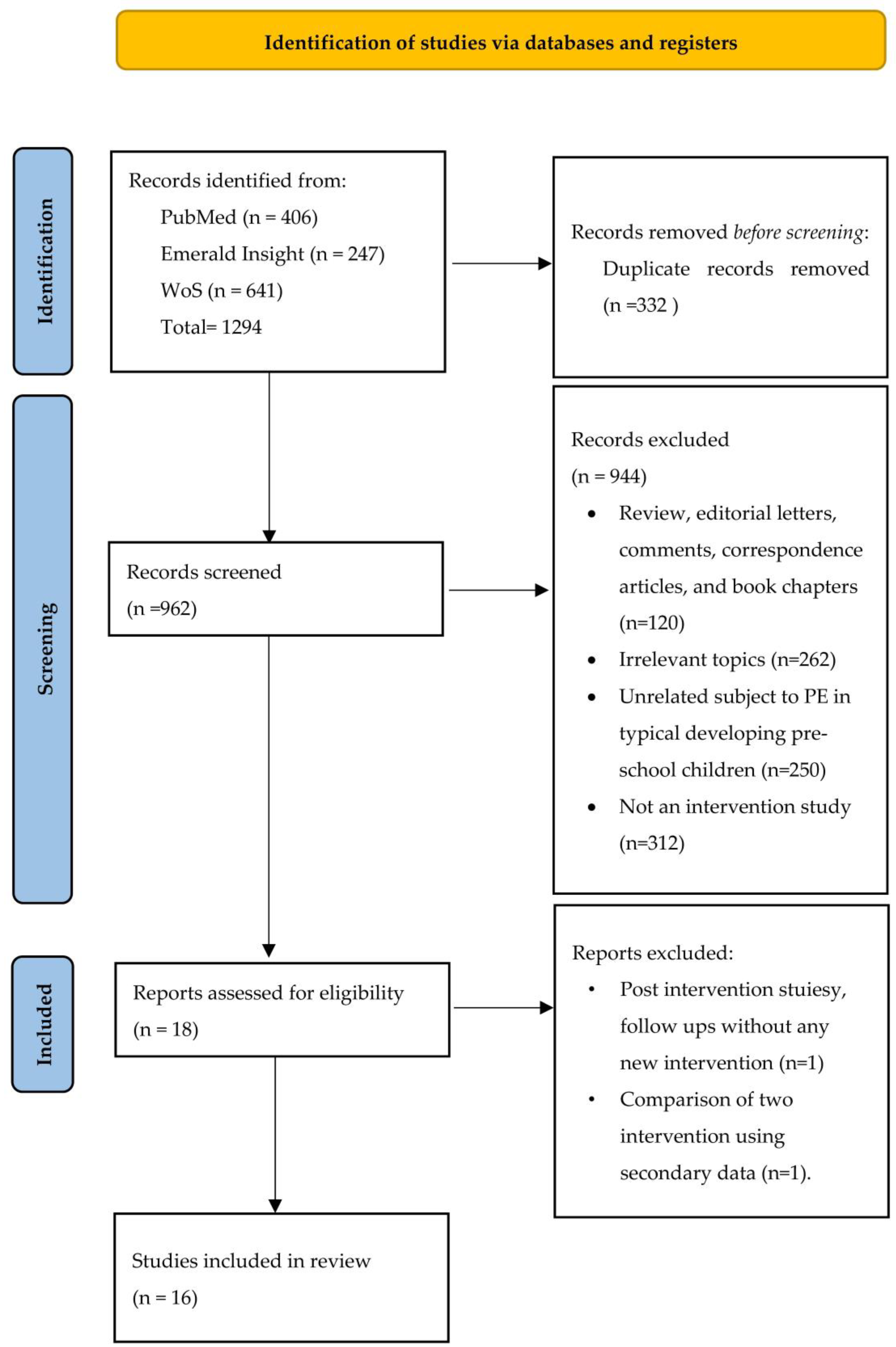
2.3. Stage 3—Study Selection
- 3.
- Intervention studies.
- 4.
- Subjects are preschool children aged between three to five years old.
- 5.
- Study outcomes focusing on sensory, nutrition, and behavioural aspects associated with picky eating
- 6.
- Studies involving children with non-typical developmental issues.
2.4. Stage 4—Charting the Data
2.5. Stage 5—Collating, Summarising, and Reporting Results
3. Results
3.1. Study Characteristic
3.2. Screening Tools to Identify PE
3.3. Types of Intervention and Component Approaches
3.4. Intervention Outcomes and General Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gibson, E.L.; Cooke, L. Understanding Food Fussiness and Its Implications for Food Choice, Health, Weight and Interventions in Young Children: The Impact of Professor Jane Wardle. Curr. Obes. Rep. 2017, 6, 46–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grey, K.; Gonzales, G.B.; Abera, M.; Lelijveld, N.; Thompson, D.; Berhane, M.; Abdissa, A.; Girma, T.; Kerac, M. Severe malnutrition or famine exposure in childhood and cardiometabolic non-communicable disease later in life: A systematic review. BMJ Glob. Health 2021, 6, e003161. [Google Scholar] [CrossRef] [PubMed]
- Kerzner, B. Clinical Investigation of Feeding Difficulties in Young Children A Practical Approach. Clin. Pediatr. 2009, 48, 960–965. [Google Scholar] [CrossRef] [PubMed]
- van der Horst, K. Overcoming picky eating. Eating enjoyment as a central aspect of children’s eating behaviors. Appetite 2012, 58, 567–574. [Google Scholar] [CrossRef]
- Machado, B.C.; Dias, P.; Lima, V.S.; Campos, J.; Gonçalves, S. Prevalence and correlates of picky eating in preschool-aged children: A population-based study. Eat. Behav. 2016, 22, 16–21. [Google Scholar] [CrossRef]
- Li, Z.; van der Horst, K.; Eldelson-Fries, L.; Yu, K.; You, L.; Zhang, Y.; Vinyes-Pares, G.; Wang, P.; Yang, X.; Qin, L.; et al. Perceptions of food intake and weight status among parents of picky eating infants and toddlers in China: A cross-sectional study. Appetite 2017, 108, 456–463. [Google Scholar] [CrossRef] [Green Version]
- Taylor, C.M.; Wernimont, S.M.; Northstone, K.; Emmett, P.M. Picky/fussy eating in children: Review of definitions, assessment, prevalence and dietary intakes. Appetite 2015, 95, 349–359. [Google Scholar] [CrossRef] [Green Version]
- Joseph-Louise, S.P.; Tan, S.T. Association between eating behaviours and weight status of picky eaters and non-picky eaters among Malaysian children aged 5–10 years old. In Proceedings of the Nutrition Society of Malaysia Conference, Kuala Lumpur, Malaysia, 24–25 November 2020. [Google Scholar]
- Mohd Hanapi, H.; Mohd Fahmi Teng, N.I. Picky Eating Behaviour an Nutritional Status of Preschool Children in Kuala Selangor, Malaysia. Malays. J. Med. Health Sci. 2022, 18, 145–150. [Google Scholar]
- Samuel, T.M.; Musa-Veloso, K.; Ho, M.; Venditti, C.; Shahkhalili-Dulloo, Y. A Narrative Review of Childhood Picky Eating and Its Relationship to Food Intakes, Nutritional Status, and Growth. Nutrients 2018, 10, 1992. [Google Scholar] [CrossRef] [Green Version]
- Goh, D.Y.T.; Jacob, A. Perception of picky eating among children in Singapore and its impact on caregivers: A questionnaire survey. Asia Pac. Fam. Med. 2012, 11, 5. [Google Scholar] [CrossRef] [Green Version]
- Toyama, H.; Agras, W.S. A test to identify persistent picky eaters. Eat. Behav. 2016, 23, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Rohde, J.F.; Handel, M.N.; Stougaard, M.; Olsen, N.J.; Traerup, M.; Mortensen, E.L.; Heitmann, B.L. Relationship between pickiness and subsequent development in body mass index and diet intake in obesity prone normal weight preschool children. PLoS ONE 2017, 12, e0172772. [Google Scholar] [CrossRef] [Green Version]
- Taylor, C.M.; Steer, C.D.; Hays, N.P.; Emmett, P.M. Growth and body composition in children who are picky eaters: A longitudinal view. Eur. J. Clin. Nutr. 2018, 73, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the Children’s Eating Behaviour Questionnaire. J. Child Psychol. Psychiatry 2001, 42, 963–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaacobi, C.; Agras, W.S.; Bryson, S.; Hammer, L.D. Behavioral Validation, Precursors, and Concomitants of Picky Eating in Childhood. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, P.M.; Holm-Denoma, J.M.; Gau, J.M.; Joiner Jr, T.E.; Striegel-Moore, R.; Bear, P.; Lamoureux, B. Problematic Eating and FeedingBehaviors of 36-Month Old Children. Int. J. Eat. Disord. 2005, 38, 208–219. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef]
- Antoniou, E.E.; Roefs, A.; Kremers, S.P.; Jansen, A.; Gubbels, J.S.; Sleddens, E.F.; Thijs, C. Picky eating and child weight status development: A longitudinal study. J. Hum. Nutr. Diet. 2016, 29, 298–307. [Google Scholar] [CrossRef]
- Ekstein, S.; Laniado, D.; Glick, B. Does picky eating affect weight-for-length measurements in young children? Clin. Pediatr. 2010, 49, 217–220. [Google Scholar] [CrossRef]
- Xue, Y.; Lee, E.; Ning, K.; Zheng, Y.; Ma, D.; Gao, H.; Yang, B.; Bai, Y.; Wang, P.; Zhang, Y. Prevalence of picky eating behaviour in Chinese school-age children and associations with anthropometric parameters and intelligence quotient. A cross-sectional study. Appetite 2015, 91, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Tharner, A.; Jansen, P.W.; Kiefte-de Jong, J.C.; Moll, H.A.; van der Ende, J.; Jaddoe, V.W.; Hoffman, A.; Tiemeier, H.; Franco, O.H. Toward an operative diagnosis of fussy/picky eating: A latent profile approach in a population-based cohort. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- de Barse, L.M.; Tiemeier, H.; Leermakers, E.T.M.; Voortman, T.; Jaddoe, V.W.V.; Edelson, L.R.; Franco, O.H.; Jansen, P.W. Longitudinal association between preschool fussy eating and body composition at 6 years of age: The Generation R Study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Horst, K.; Deming, D.; Lesniauskas, R.; Carr, T.; Reidy, K. Picky eating: Associations with child eating characteristics and food intake. Appetite 2016, 103, 286–293. [Google Scholar] [CrossRef] [Green Version]
- Esfarjani, F.; Roustaee, R.; Mohammadi-Nasrabadi, F.; Esmaillzadeh, A. Major Dietary Patterns in Relation to Stunting among Children in Tehran, Iran. J. Health Popul. Nutr. 2013, 31, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grulichova, M.; Kuruczova, D.; Svancara, J.; Pikhart, H.; Bienertova-Vasku, J. Association of Picky Eating with Weight and Height-The European Longitudinal Study of Pregnancy and Childhood (ELSPAC-CZ). Nutrients 2022, 14, 444. [Google Scholar] [CrossRef] [PubMed]
- Chao, H.C.; Lu, J.J.; Yang, C.Y.; Yeh, P.J.; Chu, S.M. Serum Trace Element Levels and Their Correlation with Picky Eating Behavior, Development, and Physical Activity in Early Childhood. Nutrients 2021, 13, 2295. [Google Scholar] [CrossRef] [PubMed]
- Maggini, S.; Wintergerst, E.S.; Beveridge, S.; Hornig, D.H. Selected vitamins and trace elements support immune function by strengthening epithelial barriers and cellular and humoral immune responses. Br. J. Nutr. 2007, 98, S29–S35. [Google Scholar] [CrossRef] [PubMed]
- Salgueiro, M.J.; Zubillaga, M.B.; Lysionek, A.E.; Caro, R.A.; Weill, R.; Boccio, J.R. The Role of Zinc in the Growth and Development of Children. Nutrition 2002, 18, 510–519. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Marchand, V.; Reginald, S.S. The ‘picky eater’: The toddler or preschooler who does not eat. Paediatr. Child Health 2012, 17, 455–457. [Google Scholar] [CrossRef]
- Caton, S.J.; Blundell, P.; Ahern, S.M.; Nekitsing, C.; Olsen, A.; Møller, P.; Hausner, H.; Remy, E.s.; Nicklaus, S.; Chabanet, C.; et al. Learning to Eat Vegetables in Early Life: The Role of Timing, Age and Individual Eating Traits. PLoS ONE 2014, 9, e97609. [Google Scholar] [CrossRef] [Green Version]
- Coulthard, H.; Sealy, A. Play with your food! Sensory play is associated with tasting of fruits and vegetables in preschool children. Appetite 2017, 113, 84–90. [Google Scholar] [CrossRef]
- de Wild, V.W.T.; de Graaf, C.; Jager, G. Use of Different Vegetable Products to Increase Preschool-Aged Children’s Preference for and Intake of a Target Vegetable: A Randomized Controlled Trial. J. Acad. Nutr. Diet. 2016, 117, 859–866. [Google Scholar] [CrossRef]
- Hoppu, U.; Prinz, M.; Ojansivu, P.; Laaksonen, O.; Sandell, M.A. Impact of sensory-based food education in kindergarten on willingness to eat vegetables and berries. Food Nutr. Res. 2015, 59, 28795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nekitsing, C.; Blundell-Birtill, P.; Cockroft, J.E.; Fildes, A.; Hetherington, M.M. Increasing Intake of an Unfamiliar Vegetable in Preschool Children Through Learning Using Storybooks and Sensory Play: A Cluster Randomized Trial. J. Acad. Nutr. Diet. 2019, 119, 2014–2027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, A.L.; Brown, E.; Goodale, T.; McLachlan, M.; Parrett, A. A Nursery-Based Cooking Skills Programme with Parents and Children Reduced Food Fussiness and Increased Willingness to Try Vegetables: A Quasi-Experimental Study. Nutrients 2020, 12, 2623. [Google Scholar] [CrossRef] [PubMed]
- Karagiannaki, K.; Ritz, C.; Jensen, L.G.H.; Torsleff, E.H.; Moller, P.; Hausner, H.; Olsen, A. Optimising Repeated Exposure: Determining Optimal Exposure Frequency for Introducing a Novel Vegetable among Children. Foods 2021, 10, 913. [Google Scholar] [CrossRef] [PubMed]
- Hamzaid, N.H.; Rajikan, R.; Sulaiman, S.; Abd Manaf, Z. Semi-Reality Simulated Patient (SRSP) Assessment Technique in Enhancing Students’ Learning Experience For Medical Nutrition Therapy For Picky-Eater Children With Special Health Care Needs. In Proceedings of the Redesigning Assessment for Holistic Learning Conference, Johor Bahru, Malaysia, 20–21 November 2017. [Google Scholar]
- Sandvik, P.; Ek, A.; Eli, K.; Somaraki, M.; Bottai, M.; Nowicka, P. Picky eating in an obesity intervention for preschool-aged children—What role does it play, and does the measurement instrument matter? Int. J. Behav. Nutr. Phys. Act. 2019, 16, 76. [Google Scholar] [CrossRef] [Green Version]
- Bellows, L.L.; Johnson, S.L.; Davies, P.L.; Anderson, J.; Gavin, W.J.; Boles, R.E. The Colorado LEAP study: Rationale and design of a study to assess the short term longitudinal effectiveness of a preschool nutrition and physical activity program. BMC Public Health 2013, 13, 1146. [Google Scholar] [CrossRef] [Green Version]
- Mallan, K.M.; Fildes, A.; Magarey, A.M.; Daniels, L.A. The Relationship between Number of Fruits, Vegetables, and Noncore Foods Tried at Age 14 Months and Food Preferences, Dietary Intake Patterns, Fussy Eating Behavior, and Weight Status at Age 3.7 Years. J. Acad. Nutr. Diet. 2015, 116, 630–637. [Google Scholar] [CrossRef] [Green Version]
- Skouteris, H.; Hill, B.; McCabe, M.; Swinburn, B.; Busija, L. A parent-based intervention to promote healthy eating and active behaviours in pre-school children: Evaluation of the MEND 2–4 randomized controlled trial. Pediatr. Obes. 2015, 11, 4–10. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid.-Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of internal medicine: Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.; Lee, J.; Paik, H.Y.; Yoon, J.; Ryu, B.; Shim, J.E. Effects of multiple herb formula SEC-22 supplementation on dietary intake, picky eating behaviors, and growth indices in thin preschool children. Nutr. Res. Pract. 2015, 9, 393–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alarcon, P.A.; Lin, L.H.; Noche, M., Jr.; Hernandez, V.C.; Cimafranca, L.; Lam, W.; Comer, G.M. Effect of oral supplementation on catch-up growth in picky eaters. Clin. Pediatr. 2003, 42, 209–217. [Google Scholar] [CrossRef]
- Sheng, X.; Tong, M.; Zhao, D.; Leung, T.F.; Zhang, F.; Hays, N.P.; Ge, J.; Ho, W.M.; Northington, R.; Terry, D.L.; et al. Randomized controlled trial to compare growth parameters and nutrient adequacy in children with picky eating behaviors who received nutritional counseling with or without an oral nutritional supplement. Nutr. Metab. Insights 2014, 7, 85–94. [Google Scholar] [CrossRef]
- Ghosh, A.K.; Kishore, B.; Shaikh, I.; Satyavrat, V.; Kumar, A.; Shah, T.; Pote, P.; Shinde, S.; Berde, Y.; Low, Y.L.; et al. Effect of oral nutritional supplementation on growth and recurrent upper respiratory tract infections in picky eating children at nutritional risk: A randomized, controlled trial. J. Int. Med. Res. 2018, 46, 2186–2201. [Google Scholar] [CrossRef]
- Khanna, D.; Yalawar, M.; Saibaba, P.V.; Bhatnagar, S.; Ghosh, A.; Jog, P.; Khadilkar, A.V.; Kishore, B.; Paruchuri, A.K.; Pote, P.D.; et al. Oral Nutritional Supplementation Improves Growth in Children at Malnutrition Risk and with Picky Eating Behaviors. Nutrients 2021, 13, 3590. [Google Scholar] [CrossRef]
- Carruth, B.R.; Ziegler, P.J.; Gordon, A.; Barr, S.I. Prevalence of Picky Eaters among Infants and Toddlers and Their Caregivers’ Decisions about Offering a New Food. J. Am. Diet. Assoc. 2003, 104, S57–S64. [Google Scholar] [CrossRef]
- Chilman, L.; Kennedy-Behr, A.; Frakking, T.; Swanepoel, L.; Verdonck, M. Picky Eating in Children: A Scoping Review to Examine Its Intrinsic and Extrinsic Features and How They Relate to Identification. Int. J. Environ. Res. Public Health 2021, 18, 9067. [Google Scholar] [CrossRef]
- Nekitsing, C.; Blundell-Birtill, P.; Cockroft, J.E.; Hetherington, M.M. Systematic review and meta-analysis of strategies to increase vegetable consumption in preschool children aged 2-5 years. Appetite 2018, 127, 138–154. [Google Scholar] [CrossRef] [PubMed]
- Nekitsing, C.; Hetherington, M.M.; Blundell-Birtill, P. Developing Healthy Food Preferences in Preschool Children Through Taste Exposure, Sensory Learning, and Nutrition Education. Curr. Obes. Rep. 2018, 7, 60–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.M.; Suchdev, P.S. Assessing and Improving Childhood Nutrition and Growth Globally. Pediatr. Clin. N. Am. 2017, 64, 755–768. [Google Scholar] [CrossRef] [PubMed]
- Podlesak, A.K.M.; Mozer, M.E.; Smith-Simpson, S.; Lee, S.Y.; Donovan, S.M. Associations between Parenting Style and Parent and Toddler Mealtime Behaviors. Curr. Dev. Nutr. 2017, 1, e000570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashid, A.F.; Wafa, S.W.; Abd Talib, R.; Abu Bakar, N.M. An interactive Malaysian Childhood Healthy Lifestyle (i-MaCHeL) intervention programme to change weight-related behaviour in preschool child-parent dyads: Study protocol of a cluster randomised controlled trial. PLoS ONE 2022, 17, e0276843. [Google Scholar] [CrossRef]
- Mitchell, G.L.; Farrow, C.; Haycraft, E.; Meyer, C. Parental influences on children’s eating behaviour and characteristics of successful parent-focussed interventions. Appetite 2013, 60, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Steinsbekk, S.; Sveen, T.H.; Fildes, A.; Llewellyn, C.; Wichstrom, L. Screening for pickiness—A validation study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 2. [Google Scholar] [CrossRef] [Green Version]
- Pliner, P. Development of measures of food neophobia in children. Appetite 1994, 23, 147–163. [Google Scholar] [CrossRef]
- West, F.; Sanders, M.R. The Lifestyle Behaviour Checklist: A measure of weight-related problem behaviour in obese children. Int. J. Pediatr. Obes. 2009, 4, 266–273. [Google Scholar] [CrossRef]
- Smith, A.D.; Herle, M.; Fildes, A.; Cooke, L.; Steinsbekk, S.; Llewellyn, C.H. Food fussiness and food neophobia share a common etiology in early childhood. J. Child Psychol. Psychiatry 2017, 58, 189–196. [Google Scholar] [CrossRef] [Green Version]
- Holley, C.E.; Haycraft, E.; Farrow, C. Predicting children’s fussiness with vegetables: The role of feeding practices. Matern. Child Nutr. 2018, 14, e12442. [Google Scholar] [CrossRef] [PubMed]
- Lafraire, J.; Rioux, C.; Giboreau, A.; Picard, D. Food rejections in children: Cognitive and social/environmental factors involved in food neophobia and picky/fussy eating behavior. Appetite 2016, 96, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Sarvanathan, R.; Tan, S.Y.; Yang, W.W. Nutrition and behaviour modification for picky eaters. MIMS J. Paediatr. Obstet. Gynaecol. 2017, 168–169. [Google Scholar]



{kind=link}
{kind=link}
| First Author (Year) | Country | Age/Mean/Range | Sample Size Intervention (I), Control (C) | Duration of Intervention |
|---|---|---|---|---|
| Single Intervention Component: 13 Studies | ||||
| ||||
| Caton et al., 2014 [31] | France | 4–38 months | I1 = 112 I2 = 112 I3 = 108 | 5 weeks |
| de Wild et al., 2016 [33] | Netherlands | 2–4 years old | I1 = 26 I2 = 25 I3 = 26 C = 26 | 8 weeks |
| Hoppu et al., 2016 [34] | Finland | 3–6 years old | I = 44 C = 24 | 5 weeks |
| Coulthard and Sealy., 2017 [32] | UK | 2–5 years old | I = 21 C1 = 20 C2 = 21 | 1 day |
| Nekitsing et al., 2019 [35] | UK | 2–5 years old | I1 = 59 I2 = 66 I3 = 65 I4 = 74 | 15 days |
| Garcia et al., 2020 [36] | UK | 3–5 years old | I = 64 C = 57 | 4 weeks |
| Karagiannaki et al., 2021 [37] | Denmark | 3–6 years old | I1 = 47 I2 = 32 I3 = 30 C = 50 | 6 months |
| ||||
| Alarcon et al., 2003 [47] | Taiwan and the Philippines | 3–5 years old | I = 53 C = 51 | 3 months |
| Sheng et al., 2014 [48] | China | 2.5–5 years old | I = 77 C = 76 | 4 months |
| Kim et al., 2015 [46] | Korea | 2–5 years old | I = 35 C = 44 | 2 months (follow-up at 2 months) |
| Ghosh et al., 2018 [49] | India | 2–6 years old | I = 127 C = 128 | 3 months |
| Khanna et al. 2021 [50] | India | 2–4 years old | I1 = 107 I2 = 107 C = 107 | 3 months |
| ||||
| Sandvik et al., 2019 [39] | Sweden | 4–6 years old | I = 65 C = 65 | 14–16 weeks (follow-up at 12 months) |
| Multi-Component Intervention: 3 Studies | ||||
| Bellows et al., 2013 [40] | USA | 4 years old (4.7 ± 0.4) | I = 143 C = 107 | 12 weeks (follow-up at 24 months) |
| Mallan et al., 2015 [41] | Australia | There are 4 data collection sessions: 1st: 4.3 ± 1.0 months 2nd: 13.7 ± 1.3 months 3rd: 24.1 ± 0.7 months 4th: 44.5 ± 3.1 months | I = 174 C = 166 | 10 months (follow-up at 10 months and 30 months) |
| Skouteris et al., 2016 [42] | Australia | 2–4 years old | I = 104 C = 97 | 15 months |
| Type of Intervention | Author (Year) | Screening Tools for PE | Intervention Components | Implementation | Outcome Finding |
|---|---|---|---|---|---|
| Single-component intervention: sensory component approach (single or multisensory): 54% | Caton et al., 2014 [31] | None (evaluation of intervention using CEBQ) | Sensory (taste). Repeated exposure and flavour masking. | Consumption of three types of artichoke: (a) artichoke puree, (b) flavour-learning: artichoke puree and sweetness, and (c) flavour-nutrient learning: artichoke puree and energy. Each subject received 5–10 exposures. | Behaviour assessment:
|
| de Wild et al., 2016 [33] | None (evaluation of intervention using CFNS) | Sensory (taste and texture). Repeated exposure and flavour masking. | Consumption of three types of spinach: (a) pure spinach, (b) cream spinach (flavour masking), and (c) ravioli spinach (hidden). It is frozen and sent home. | Behaviour assessment:
| |
| Hoppu et al. 2016 [34] | None | Sensory (multisensory). Multisensory play. | Five sessions of sensory learning (once per week), 20–30 min. Food play (multisensory play) involved a visual card and acting (fairy tales and puppets). | Behaviour assessment:
| |
| Coulthard and Sealy. 2017 [32] | None (CFNS was used as an outcome) | Sensory (multiple sensory). Multisensory play. | This study used visual food play. In the intervention, participants created photos using fruits and vegetables (FV). They were allowed to chop, reshape, or squish the food. | Behaviour assessment:
| |
| Nekitsing et al. 2019 [35] | None | Sensory (multisensory). Multisensory play and storybooks. | Multisensory play: The exercises covered sound (listening to the vegetable’s name and tapping it to hear a sound), sight, touch, and smell (picking and sniffing the various shapes), but not taste. Storybook: Storybook featuring targeted vegetables (picture). Throughout the intervention, multiple storybook readings were conducted. | Behaviour assessment:
| |
| Garcia et al. 2020 [36] | Yes (reports by caregivers) | Sensory (taste and texture). Preparing a meal together and repetitive vegetable exposure and sensory play. | Parent-child cooking session. Children used cooking tools to learn to chop, grate, mix, and measure food ingredients that included vegetables. Each weekly session encouraged the use of smell. | Behaviour assessment:
| |
| Karagiannaki et al., 2021 [37] | None (evaluation of intervention using CFNS and CEBQ) | Sensory (taste). Repeated exposure. | All group interventions were given 100 g of daikon. The difference was the time exposure (once per week, twice per week, or bi-weekly), but each group received a total of seven-time exposure. | Behaviour assessment:
| |
| Single-component intervention: nutrition component approach (anthropometry, food intake and behaviour): 38% | Alarcon et al., 2003 [47] | Yes (reports by caregivers and analysis from 3-day diet recall) | Nutrition (anthropometry). Oral nutrition supplement (ONS) and diet counselling (DC). | ONS: PediaSure consumed 40 mL/kg/day of the supplement in addition to the irregular diet. DC: Individualised counselling by a doctor focusing on healthy eating, portion control, reducing sugar and fat intake, and giving praise when eating refused dishes. | Nutrition status and food intake:
|
| Sheng et al., 2014 [48] | Yes (reports by caregivers) | Nutrition (anthropometry and food intake). Oral nutrition supplement (ONS) and diet counselling (DC). | ONS: Milk-based powder (S-26 PE GOLD), taken at least 230 mL servings/day. DC: An individualised dietary approach using the Child Nutrition Branch Dietary Guidelines for children. Scheduled meals and snacks, portion sizes, a distraction-free mealtime setting, and providing a mealtime role model. | Nutrition status and food intake:
| |
| Kim et al., 2015 [46] | None (Evaluation of intervention using a modified version of Carruth’s (2004)) | Nutrition (anthropometry, eating behaviour and food intake) and ONS. | Herbal supplementation: SEC-22 (herbs) was provided orally in the mornings and nights after being boiled. | Nutrition status and food intake:
| |
| Ghosh et al., 2018 [49] | Yes (set of a question of PE behaviours, identified as a PE if shows two or more behaviours) | Nutrition (anthropometry). Oral nutrition supplement (ONS) and diet counselling (DC). | ONS: PediaSure. Children aged 24 to 48 months consumed one serving (224 mL) of ONS, while those aged 48 to 72 months were provided with two servings (448 mL). DC: No details provided. | Nutrition status and food intake:
| |
| Khanna et al., 2021 [50] | Yes (set of a question of PE behaviours, identified as a PE if it shows two or more behaviours) | Nutrition (anthropometry). oral nutrition supplement (ONS) and diet counselling (DC). | ONS: PediaSure (ONS1-milk base; ONS2-lactose-free) taking 1–2 servings daily. DC: The counselling focused on eating a well-balanced diet that included foods from various food categories, improving the diet’s quality, and meeting the child’s daily nutritional needs. | Nutrition status and food intake:
| |
| Single-component intervention: parenting component approach: 8% | Sandvik et al., 2019 [39] | None (evaluation of intervention using CEBQ and the LBC Lifestyle Behaviour Checklist) | Parenting. To support a healthy environment, healthy eating, and physical activity. | Group discussions and practice through role-playing; 10 sessions of creating a suitable environment and parenting support to eat sufficiently were conducted. | Behaviour assessment:
|
| Multiple intervention components | Bellows et al., 2013 [40] | None | Cognitive Behaviour. Used vegetable cartoons in activities. Sensory (taste and texture). Repeated exposure. Social and Environmental. A repeated message from earlier phases. | Cognitive Behaviour. Fun and creative activities such as a puppet show, fruit and vegetable mystery bag, a tasting party, and puzzles. Sensory-Jicama was offered and repeatedly exposed to the children. Used posters and banners to display in the school environment. Parents received a newsletter (chef’s hat, spatula, and recipe book). | Behaviour assessment:
|
| Mallan et al., 2015 [41] | None (evaluation of intervention using CEBQ) | Nutrition (food intake). Texture and taste variety, and neutral exposure to healthful meals. Social and Environmental. Positive feeding environment and toddler eating behaviour management. Parenting. Authoritative parenting practice. | Group-interactive sessions. Workbooks were distributed to ensure optimal intervention dose, monitored home-based tactics, and promoted retention. | Behaviour assessment:
Nutrition status and food intake:
| |
| Skouteris et al., 2016 [42] | None (evaluation of intervention using CFNS and CEBQ) | Nutrition (food intake and behaviour). Healthy eating and cooking together. Parenting. Parenting behavioural model. | All interventions were organised in a workshop. Discussion and presentation, child play, and healthy food demonstration. | Behaviour assessment:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamarudin, M.S.; Shahril, M.R.; Haron, H.; Kadar, M.; Safii, N.S.; Hamzaid, N.H. Interventions for Picky Eaters among Typically Developed Children—A Scoping Review. Nutrients 2023, 15, 242. https://doi.org/10.3390/nu15010242
Kamarudin MS, Shahril MR, Haron H, Kadar M, Safii NS, Hamzaid NH. Interventions for Picky Eaters among Typically Developed Children—A Scoping Review. Nutrients. 2023; 15(1):242. https://doi.org/10.3390/nu15010242
Chicago/Turabian StyleKamarudin, Mohd Shah, Mohd Razif Shahril, Hasnah Haron, Masne Kadar, Nik Shanita Safii, and Nur Hana Hamzaid. 2023. "Interventions for Picky Eaters among Typically Developed Children—A Scoping Review" Nutrients 15, no. 1: 242. https://doi.org/10.3390/nu15010242