

Evaluation of the Usefulness of a Serological Test for Diagnosis of Celiac Disease Simultaneously Detecting Specific Antibodies and Total IgA
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
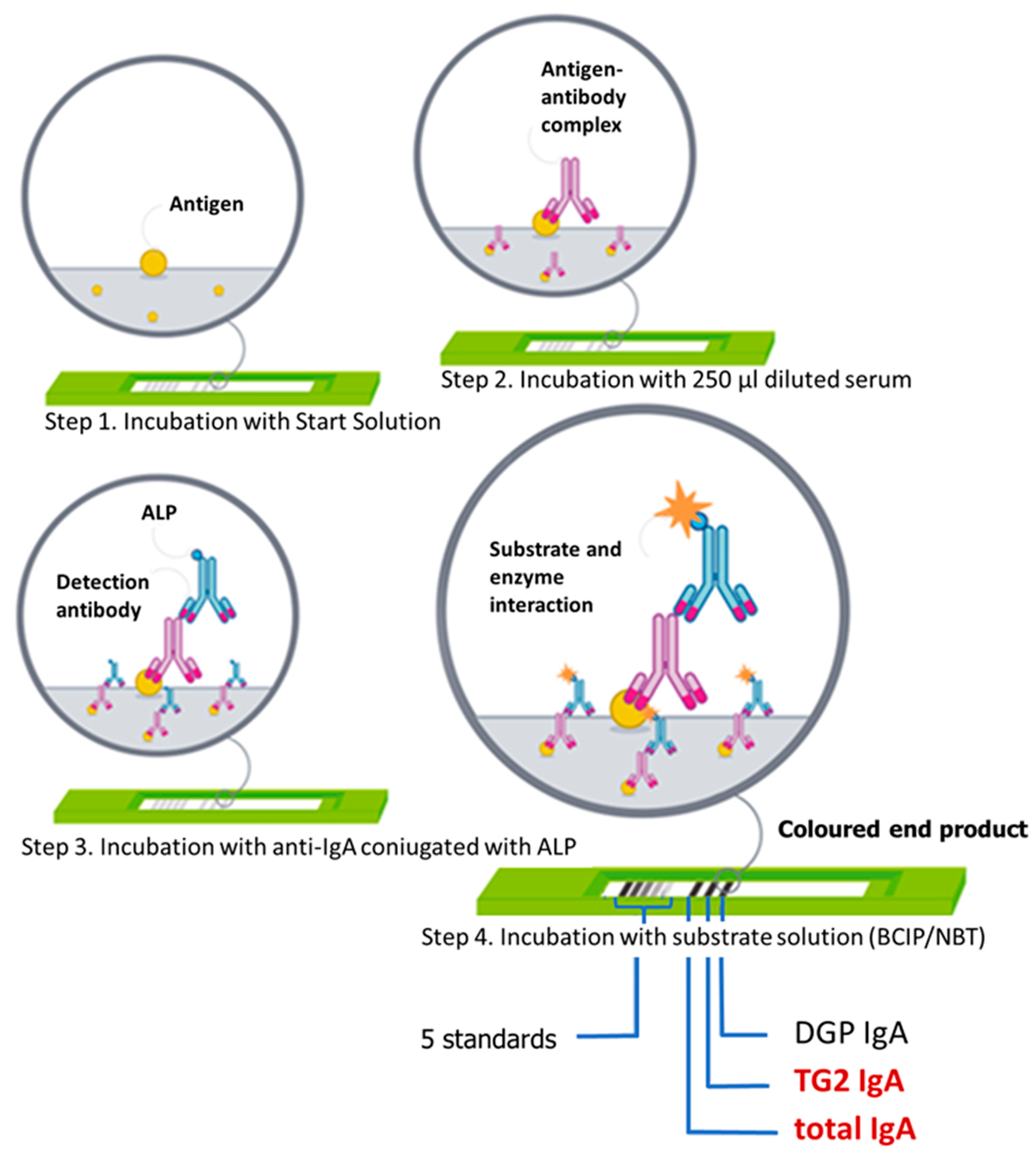
2.2. Antibody Determination by Multiparametric Immunoassay
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Asri, N.; Rostami-Nejad, M.; Barzegar, M.; Nikzamir, A.; Rezaei-Tavirani, M.; Razzaghi, M.; Zali, M.R. Suppressive Mechanisms Induced by Tregs in Celiac Disease. Iran. Biomed. J. 2020, 24, 140–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majsiak, E.; Cichoz-Lach, H.; Gubska, O.; Cukrowska, B. Celiac disease—Disease of children and adults: Symptoms, disease complications, risk groups and comorbidities. Pol. Merkur. Lek. Organ Pol. Tow. Lek. 2018, 44, 31–35. [Google Scholar]
- Glissen Brown, J.R.; Singh, P. Coeliac disease. Paediatr. Int. Child Health 2019, 39, 23–31. [Google Scholar] [CrossRef]
- Majsiak, E.; Choina, M.; Golicki, D.; Gray, A.M.; Cukrowska, B. The impact of symptoms on quality of life before and after diagnosis of coeliac disease: The results from a Polish population survey and comparison with the results from the United Kingdom. BMC Gastroenterol. 2021, 21, 99. [Google Scholar] [CrossRef]
- Majsiak, E.; Choina, M.; Gray, A.M.; Wysokiński, M.; Cukrowska, B. Clinical Manifestation and Diagnostic Process of Celiac Disease in Poland-Comparison of Pediatric and Adult Patients in Retrospective Study. Nutrients 2022, 14, 491. [Google Scholar] [CrossRef]
- Rodrigo, L. Celiac Disease: A Common Unrecognized Health Problem with a Very Delayed Diagnosis. Medicina 2019, 56, 9. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, V.; Kurppa, K.; Huhtala, H.; Mäki, M.; Kekkonen, L.; Kaukinen, K. Delayed celiac disease diagnosis predisposes to reduced quality of life and incremental use of health care services and medicines: A prospective nationwide study. United Eur. Gastroenterol. J. 2018, 6, 567–575. [Google Scholar] [CrossRef]
- Husby, S.; Koletzko, S.; Korponay-Szabo, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef] [Green Version]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Mearin, M.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition Guidelines for the Diagnosis of Coeliac Disease. JPGN 2012, 54, 136–160. [Google Scholar] [CrossRef]
- Husby, S.; Murray, J.A.; Katzka, D.A. AGA Clinical Practice Update on Diagnosis and Monitoring of Celiac Disease-Changing Utility of Serology and Histologic Measures: Expert Review. Gastroenterology 2019, 156, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Baykan, A.R.; Cerrah, S.; Ciftel, S.; Vural, M.K.; Kasap, E. A No-Biopsy Approach for the Diagnosis of Celiac Disease in Adults: Can It Be Real? Cureus 2022, 14, e26521. [Google Scholar] [CrossRef] [PubMed]
- Bierła, J.B.; Trojanowska, I.; Konopka, E.; Czarnowska, E.; Sowińska, A.; Cukrowska, B. Diagnostyka celiakii i badania przesiewowe w grupach ryzyka. Diagn. Lab. 2016, 52, 205–210. [Google Scholar]
- Barker, J.M.; Liu, E. Celiac disease: Pathophysiology, clinical manifestations, and associated autoimmune conditions. Adv. Pediatr. 2008, 55, 349–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nachman, F.; Vazquez, H.; Gonzalez, A.; Andrenacci, P.; Compagni, L.; Reyes, H.; Sugai, E.; Moreno, M.L.; Smecuol, E.; Hwang, H.J.; et al. Gastroesophageal reflux symptoms in patients with celiac disease and the effects of a gluten-free diet. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2011, 9, 214–219. [Google Scholar] [CrossRef]
- Spatola, B.N.; Kaukinen, K.; Collin, P.; Maki, M.; Kagnoff, M.F.; Daugherty, P.S. Persistence of elevated deamidated gliadin peptide antibodies on a gluten-free diet indicates nonresponsive coeliac disease. Aliment. Pharmacol. Ther. 2014, 39, 407–417. [Google Scholar] [CrossRef] [Green Version]
- Burgin-Wolff, A.; Mauro, B.; Faruk, H. Intestinal biopsy is not always required to diagnose celiac disease: A retrospective analysis of combined antibody tests. BMC Gastroenterol. 2013, 13, 19. [Google Scholar] [CrossRef] [Green Version]
- Vermeersch, P.; Geboes, K.; Marien, G.; Hoffman, I.; Hiele, M.; Bossuyt, X. Serological diagnosis of celiac disease: Comparative analysis of different strategies. Clin. Chim. Acta Int. J. Clin. Chem. 2012, 413, 1761–1767. [Google Scholar] [CrossRef]
- Konopka, E.; Grzywnowicz, M.; Oralewska, B.; Cielecka-Kuszyk, J.; Trojanowska, I.; Cukrowska, B. Clinical utility of quantitative multi-antibody Polycheck immunoassays in the diagnosis of coeliac disease. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 254–260. [Google Scholar] [CrossRef]
- Oberhuber, G.; Granditsch, G.; Vogelsang, H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1185–1194. [Google Scholar] [CrossRef]
- Poddighe, D.; Capittini, C. The Role of HLA in the Association between IgA Deficiency and Celiac Disease. Dis. Markers 2021, 2021, 8632861. [Google Scholar] [CrossRef]
- Grossmann, K.; Rober, N.; Hiemann, R.; Rodiger, S.; Schierack, P.; Reinhold, D.; Laass, M.W.; Conrad, K.; Roggenbuck, D. Simultaneous detection of celiac disease-specific IgA antibodies and total IgA. Auto Immun. Highlights 2016, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Owczarek, H.; Nahaczewska, W.; Paliszkiewicz, A. Test results in laboratory medicine support on Evidence-Based Medicine. Diagn. Lab. J. Lab. Diagn. 2009, 45, 247–251. [Google Scholar]
- Damoiseaux, J. Multiparametric autoimmune diagnostics: Recent advances. Pathol. Lab. Med. Int. 2016, 2016, 15. [Google Scholar] [CrossRef] [Green Version]
- Hill, M.; Watkins, R.; Leonard-Puppa, E.; Waddell, J.; Blanchard, S.; Kader, H. Usefulness of deamidated gliadin peptide antibodies in diagnosing coeliac disease in children younger than 3 years old. J. Paediatr Child Health 2022, 58, 815–819. [Google Scholar] [CrossRef] [PubMed]
- Lenti, M.V.; Rossi, C.M.; Melazzini, F.; Gastaldi, M.; Bugatti, S.; Rotondi, M.; Bianchi, P.I.; Gentile, A.; Chiovato, L.; Montecucco, C.; et al. Seronegative autoimmune diseases: A challenging diagnosis. Autoimmun. Rev. 2022, 21, 103143. [Google Scholar] [CrossRef] [PubMed]
- Monzani, A.; Rapa, A.; Fonio, P.; Tognato, E.; Panigati, L.; Oderda, G. Use of deamidated gliadin peptide antibodies to monitor diet compliance in childhood celiac disease. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 55–60. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CD Patients | No CD Patients | |||
|---|---|---|---|---|
| 48 (46%) | 56 (54%) | |||
| CD with IgA Deficiency | CD without IgA Deficiency | Non-CD with IgA Deficiency | Non-CD and no IgA Deficiency | |
| Number of patients | 20 (19%) | 28 (27%) | 28 (27%) | 28 (27%) |
| Females | 7 (35%) | 16 (57%) | 16 (57%) | 15 (54%) |
| Males | 13 (65%) | 12 (43%) | 12 (43%) | 13 (46%) |
| Mean age in years (median) | 10.3 (10.00) | 9.2 (8.7) | 10.2 (8.7) | 11.9 (13.4) |
| CD Patients | No CD Patients | |||
|---|---|---|---|---|
| CD with IgA Deficiency (n = 20) | CD without IgA Deficiency (n = 28) | Non-CD with IgA Deficiency (n = 28) | Non-CD and no IgA Deficiency (n = 28) | |
| Marsh 0 | 0 | 0 | 28 (100%) | 28 (100%) |
| Marsh II | 2 (10%) | 0 | 0 | 0 |
| Marsh III | 18 (90%) | 23 (82%) | 0 | 0 |
| CD diagnosis without biopsy | 0 | 5 (18%) | 0 | 0 |
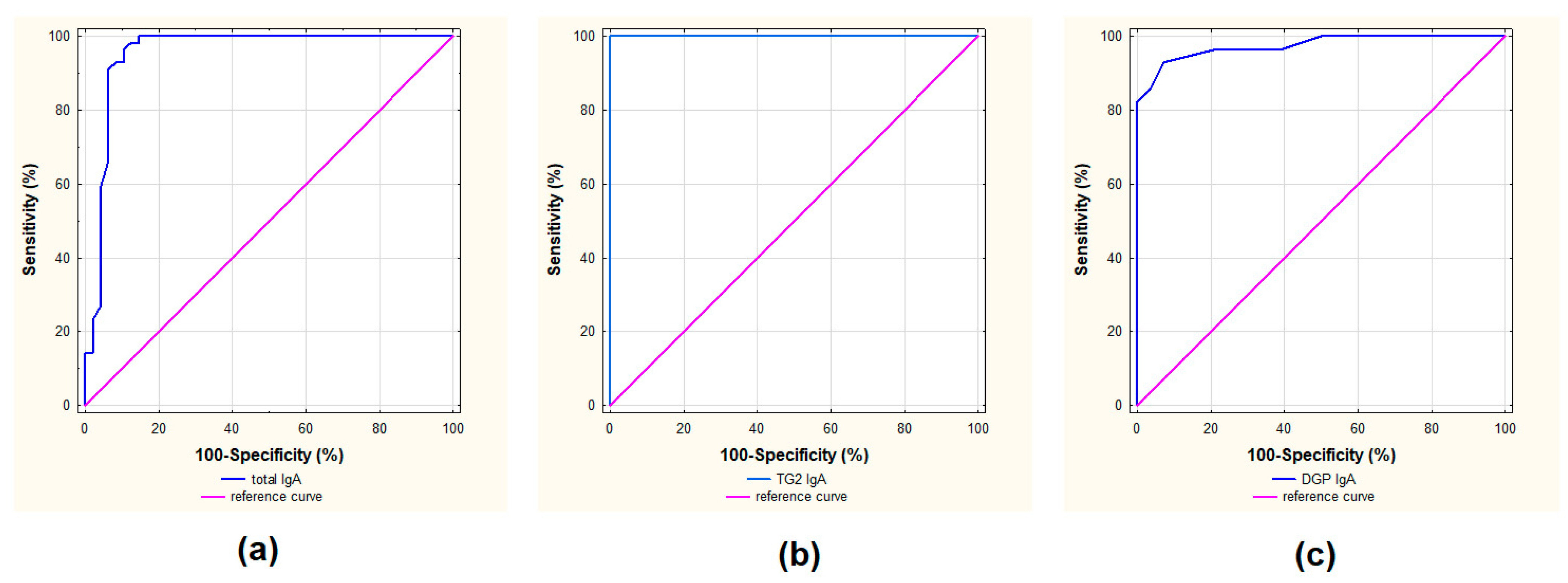
| Cut-Off in kU/L | Sensitivity | Specificity | PPV | NPV | ACC | LR+ | LR− | Youden Index | Error Rate | |
|---|---|---|---|---|---|---|---|---|---|---|
| TG2 IgA | 0.8 | 96% | 100% | 1.000 | 0.966 | 0.982 | - | 0.036 | 0.964 | 0.018 |
| DGP IgA | 0.8 | 18% | 100% | 1.000 | 0.549 | 0.589 | - | 0.821 | 0.179 | 0.411 |
| tIgA | 0.5 | 100% | 79% | 0.848 | 1.000 | 0.904 | 4.800 | 0.000 | 0.792 | 0.096 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Majsiak, E.; Cukrowska, B.; Choina, M.; Bielawski, K.; Cielecka-Kuszyk, J.; Konopka, E.; Wysokiński, M.; Bierła, J.B. Evaluation of the Usefulness of a Serological Test for Diagnosis of Celiac Disease Simultaneously Detecting Specific Antibodies and Total IgA. Nutrients 2023, 15, 202. https://doi.org/10.3390/nu15010202
Majsiak E, Cukrowska B, Choina M, Bielawski K, Cielecka-Kuszyk J, Konopka E, Wysokiński M, Bierła JB. Evaluation of the Usefulness of a Serological Test for Diagnosis of Celiac Disease Simultaneously Detecting Specific Antibodies and Total IgA. Nutrients. 2023; 15(1):202. https://doi.org/10.3390/nu15010202
Chicago/Turabian StyleMajsiak, Emilia, Bożena Cukrowska, Magdalena Choina, Kornel Bielawski, Joanna Cielecka-Kuszyk, Ewa Konopka, Mariusz Wysokiński, and Joanna Beata Bierła. 2023. "Evaluation of the Usefulness of a Serological Test for Diagnosis of Celiac Disease Simultaneously Detecting Specific Antibodies and Total IgA" Nutrients 15, no. 1: 202. https://doi.org/10.3390/nu15010202