
Prevalence of Childhood Obesity by Country, Family Socio-Demographics, and Parental Obesity in Europe: The Feel4Diabetes Study

 , , ,
, , ,  , ,
, ,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling Procedures
2.2. Ethics Approvals and Consent Forms
2.3. Data Collection
2.3.1. Socio-Demographic Characteristics
2.3.2. Anthropometry
2.4. Data Analysis
3. Results
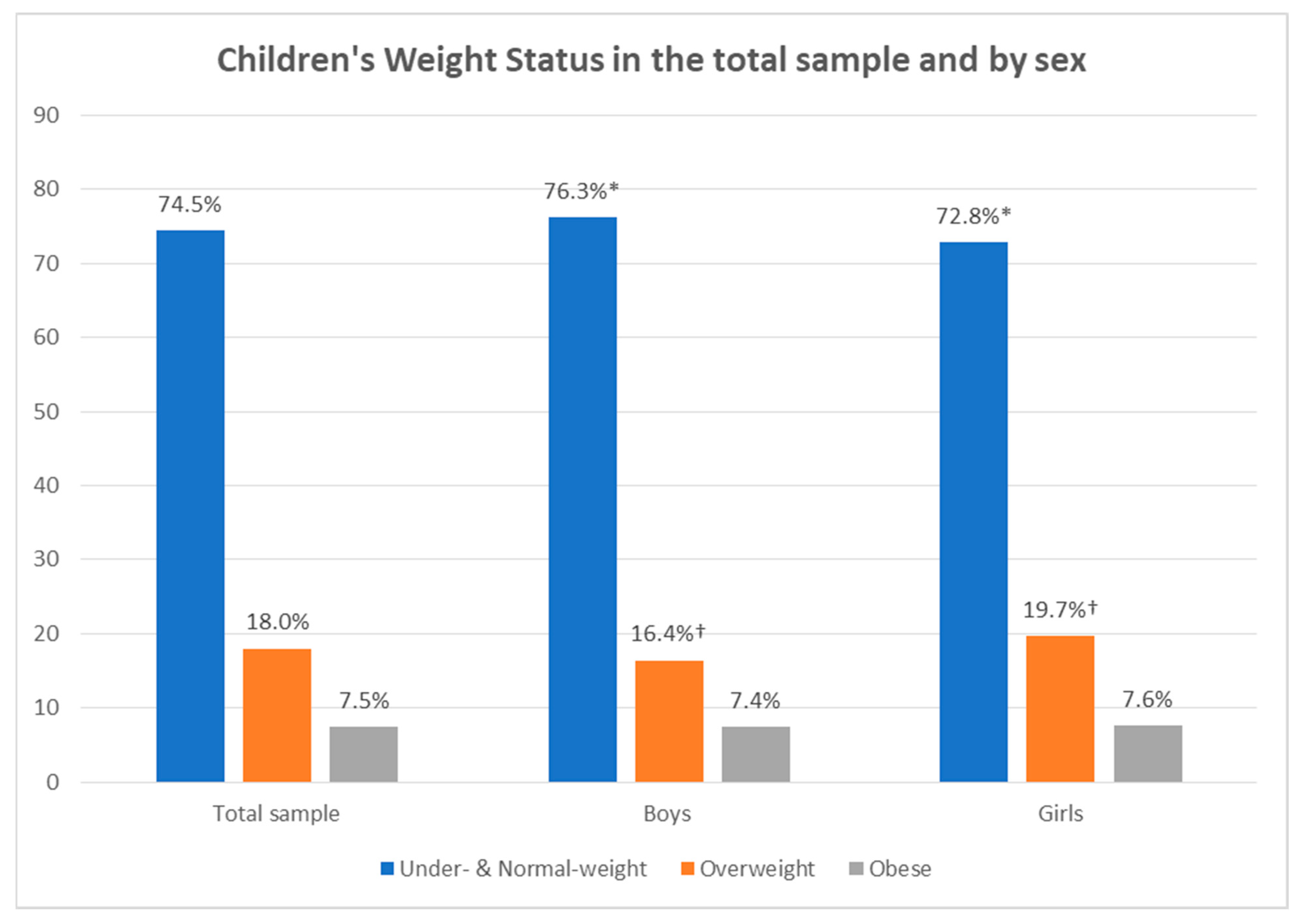
3.1. Weight Status of Participating Children
3.2. Parental Socio-Demographic Characteristics and Obesity Status
3.3. Weight Status of Participating Children by Economic Classification of Country and Parental Socio-Demographic Characteristics
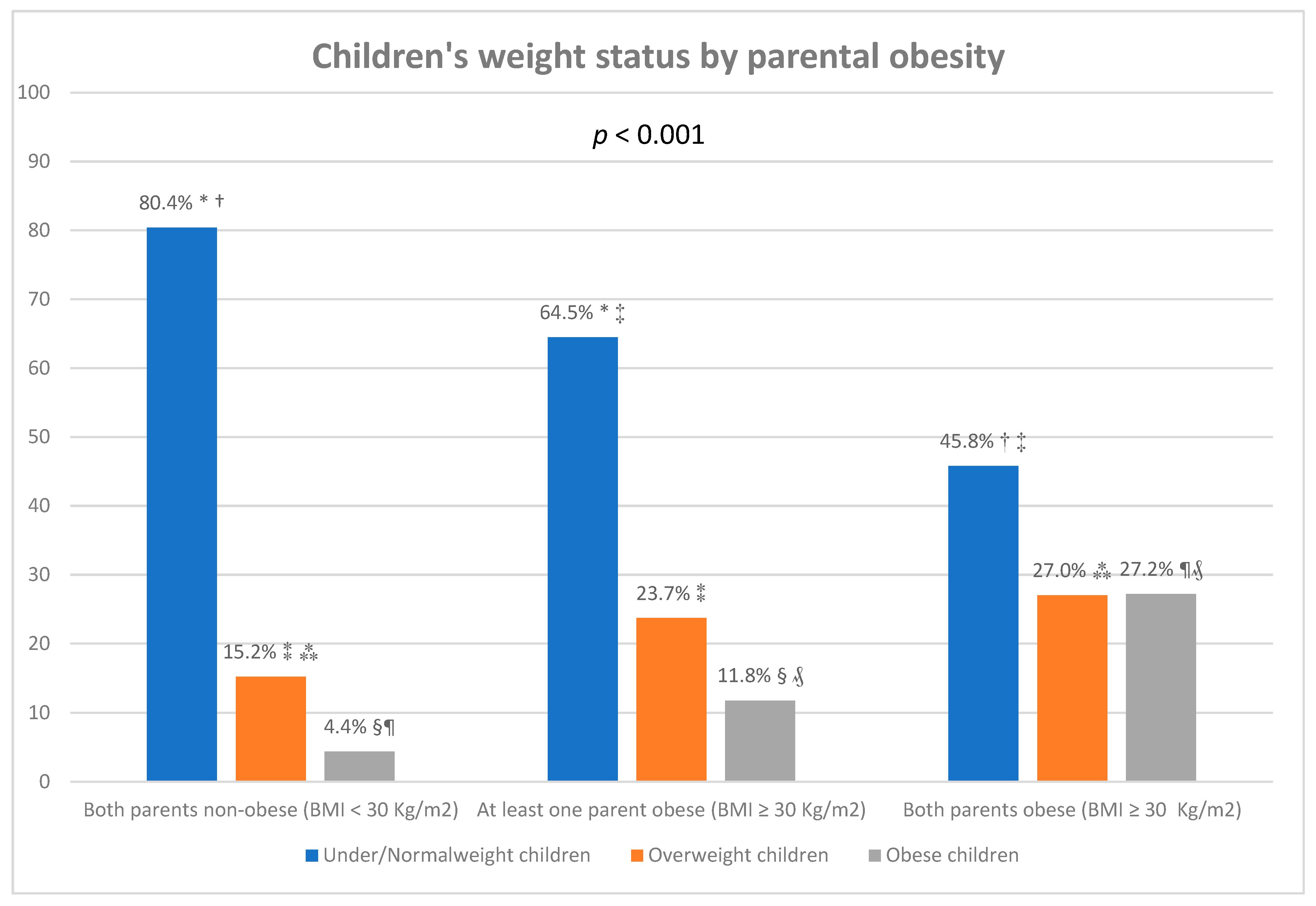
3.4. Weight Status of Participating Children by Parental Obesity
3.5. Associations between Childhood Obesity with Country’s Economic Classification, Parental Socio-Demographic Characteristics and Weight Status
4. Discussion
5. Conclusions and Implications for Future Practice and Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Obesity and Overweight. Updated on 9 June 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 7 January 2022).
- World Health Organization. The Global Health Observatory. Noncommunicable Diseases. Available online: https://www.who.int/data/gho/data/themes/noncommunicable-diseases (accessed on 7 January 2022).
- Centers for Disease and Control Prevention. Morbidity and Mortality Weekly Report. Body Mass Index and Risk for COVID-19–Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death—United States, March–December 2020. Available online: https://www.cdc.gov/mmwr/volumes/70/wr/mm7010e4.htm?s_cid=mm7010e4_x (accessed on 7 January 2022).
- World Obesity. COVID-19 and Obesity: The 2021 Atlas. The Cost of Not Addressing the Global Obesity Crisis. March 2021. Available online: https://www.worldobesityday.org/assets/downloads/COVID-19-and-Obesity-The-2021-Atlas.pdf (accessed on 7 January 2022).
- Christakis, N.A.; Fowler, J.H. The spread of obesity in a large social network over 32 years. N. Engl. J. Med. 2007, 357, 370–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, A.; Lobstein, T.; Knai, C. Obesity and Socio-Economic Groups in Europe: Evidence Review and Implications for Action. November 2007. Available online: https://ec.europa.eu/health/ph_determinants/life_style/nutrition/documents/ev20081028_rep_en.pdf (accessed on 7 January 2022).
- World Health Organisation. Regional Office for Europe. New analysis from WHO/Europe Identifies Surprising Trends in Rates of Overweight and Obesity across the Region. Updated on 7 December 2021. Available online: https://www.euro.who.int/en/health-topics/noncommunicable-diseases/obesity/news/news/2021/12/new-analysis-from-whoeurope-identifies-surprising-trends-in-rates-of-overweight-and-obesity-across-the-region (accessed on 7 January 2022).
- Manios, Y.; Androutsos, O.; Lambrinou, C.-P.; Cardon, G.; Lindström, J.; Annemans, L.; Mateo-Gallego, R.; De Sabata, M.S.; Iotova, V.; Kivelä, J.; et al. A school- and community-based intervention to promote healthy lifestyle and prevent type 2 diabetes in vulnerable families across Europe: Design and implementation of the Feel4Diabetes-study. Public Health Nutr. 2018, 21, 3281–3290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Stappen, V.; Cardon, G.; de Craemer, M.; Mavrogianni, C.; Usheva, N.; Kivelä, J.; Wikström, K.; De Miquel-Etayo, P.; González-Gil, E.M.; Radó, A.S.; et al. The effect of a cluster-randomized controlled trial on lifestyle behaviors among families at risk for developing type 2 diabetes across Europe: The Feel4Diabetes-study. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 86. [Google Scholar] [CrossRef] [PubMed]
- Moschonis, G.; Karatzi, K.; Apergi, K.; Liatis, S.; Kivelä, J.; Wikström, K.; Ayala-Marín, A.M.; Mateo-Gallego, R.; Tsochev, K.; Chakarova, N.; et al. Socio-Demographic Characteristics and Body Weight Perceptions of Study Participants Benefitting Most from the Feel4Diabetes Program Based on Their Anthropometric and Glycaemic Profile Changes. Nutrients 2020, 12, 3117. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. World Bank Country and Lending Groups–Country Classification. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519 (accessed on 8 January 2022).
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Androutsos, O.; Anastasiou, C.; Lambrinou, C.-P.; Mavrogianni, C.; Cardon, G.; Van Stappen, V.; Kivelä, J.; Wikström, K.; Moreno, L.A.; Iotova, V.; et al. Intra- and inter- observer reliability of anthropometric measurements and blood pressure in primary schoolchildren and adults: The Feel4Diabetes-study. BMC Endocr. Disord. 2020, 20, 27. [Google Scholar] [CrossRef] [Green Version]
- Lexico. Middle Age. Available online: https://www.lexico.com/en/definition/middle_age (accessed on 11 January 2022).
- Merriam-Webster. Middle Age. Available online: https://www.merriam-webster.com/dictionary/middle%20age (accessed on 11 January 2022).
- Collins. Middle Age. Available online: https://www.collinsdictionary.com/dictionary/english/middle-age (accessed on 11 January 2022).
- European Commision/EACEA/Eurydice, 2018. Compulsory Education in Europe 2018/19. Eurydice–Facts and Figures. Luxemburg: Publications Office of the European Union. Available online: https://eacea.ec.europa.eu/national-policies/eurydice/sites/default/files/compulsory_education_2018_19.pdf (accessed on 11 January 2022).
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [Green Version]
- Frieden, J.; Walter, S. Understanding the Political Economy of the Eurozone Crisis. Annu. Rev. Political Sci. 2017, 20, 371–390. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child. Adolesc Health. 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Telford, R.M.; Telford, R.D.; Olive, L.S.; Cochrane, T.; Davey, R. Why Are Girls Less Physically Active than Boys? Findings from the LOOK Longitudinal Study. PLoS ONE 2016, 11, e0150041. [Google Scholar] [CrossRef] [PubMed]
- Verloigne, M.; Van Lippevelde, W.; Maes, L.; Yildirim, M.; Chinapaw, M.; Manios, Y.; Androutsos, O.; Kovacs, E.; Bringolf-Isler, B.; Brug, J.; et al. Levels of physical activity and sedentary time among 10- to 12-year-old boys and girls across 5 European countries using accelerometers: An observational study within the ENERGY-project. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riddoch, C.J.; Andersen, L.B.; Wedderkopp, N.; Harro, M.; Klasson-Heggebø, L.; Sardinha, L.B.; Cooper, A.R.; Ekelund, U. Physical activity levels and patterns of 9- and 15-yr-old European children. Med. Sci. Sports Exerc. 2004, 36, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Brug, J.; van Stralen, M.; Velde, S.J.T.; Chinapaw, M.J.M.; De Bourdeaudhuij, I.; Lien, N.; Bere, E.; Maskini, V.; Singh, A.S.; Maes, L.; et al. Differences in weight status and energy-balance related behaviors among schoolchildren across Europe: The ENERGY-project. PLoS ONE 2012, 7, e34742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forkert, E.C.O.; De Moraes, A.C.F.; Carvalho, H.B.; Manios, Y.; Widhalm, K.; González-Gross, M.; Gutierrez, A.; Kafatos, A.; Censi, L.; De Henauw, S.; et al. Skipping breakfast is associated with adiposity markers especially when sleep time is adequate in adolescents. Sci. Rep. 2019, 9, 6380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Parliament. Directorate General for Research. Health care systems in the EU. A Comparative Study. Public Health and Consumer Protection Series. Available online: https://www.europarl.europa.eu/workingpapers/saco/pdf/101_en.pdf (accessed on 11 January 2022).
- Mohammed, S.H.; Habtewold, T.D.; Birhanu, M.M.; Sissay, T.A.; Tegegne, B.S.; Abuzerr, S.; Esmaillzadeh, A. Neighbourhood socioeconomic status and overweight/obesity: A systematic review and meta-analysis of epidemiological studies. BMJ Open 2019, 9, e028238. [Google Scholar] [CrossRef]
- Yang, Z.; Phung, H.; Hughes, A.-M.; Sherwood, S.; Harper, E.; Kelly, P. Trends in overweight and obesity by socioeconomic status in Year 6 school children, Australian Capital Territory, 2006–2018. BMC Public Health 2019, 15, 1512. [Google Scholar] [CrossRef]
- Ghosh, A.; Charlton, K.E.; Batterham, M.J. Socioeconomic disadvantage and its implications for population health planning of obesity and overweight, using cross-sectional data from general practices from a regional catchment in Australia. BMJ Open 2016, 6, e010405. [Google Scholar] [CrossRef] [Green Version]
- Siopis, G.; Jones, A.; Allman-Farinelli, M. The dietetic workforce distribution geographic atlas provides insight into the inequitable access for dietetic services for people with type 2 diabetes in Australia. Nutr. Diet. 2020, 77, 121–130. [Google Scholar] [CrossRef]
- Siopis, G.; Colagiuri, S.; Allman-Farinelli, M. People with type 2 diabetes report dietitians, social support and health literacy facilitate their dietary change. J. Nutr. Ed. Behav. 2020, 53, 43–53. [Google Scholar] [CrossRef]
- Siopis, G.; Colagiuri, S.; Allman-Farinelli, M. Doctors identify regulatory barriers for their patients with type 2 diabetes to access the nutrition expertise of dietitians. Aust. J. Prim. Care. 2020, 27, 312. [Google Scholar] [CrossRef] [PubMed]
- Broyles, S.T.; for the ISCOLE Research Group; Denstel, K.D.; Church, T.S.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. The epidemiological transition and the global childhood obesity epidemic. Int. J. Obes Suppl. 2015, 5, S3–S8. [Google Scholar] [CrossRef] [Green Version]
- Siren, R.; Eriksson, J.G.; Peltonen, M.; Vanhanen, H. Impact of Health Counselling on Cardiovascular Disease Risk in Middle Aged Men: Influence of Socioeconomic Status. PLoS ONE 2014, 9, e88959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H. Educational attainment moderates the associations of diabetes education with health outcomes. Int. J. Nurs Pract. 2016, 22, 444–450. [Google Scholar] [CrossRef]
- Karter, A.J.; Stevens, M.R.; Brown, A.F.; Duru, O.K.; Gregg, E.W.; Gary, T.L.; Beckles, G.L.; Chien-Wen, T.; Marrero, D.G.; Waitzfelder, B.; et al. Educational disparities in health behaviors among patients with diabetes: The Translating Research Into Action for Diabetes (TRIAD) Study. BMC Public Health 2007, 7, 308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaby, A.; Friis, K.; Christensen, B.; Rowlands, G.; Maindal, H.T. Health literacy is associated with health behaviour and self-reported health: A large population-based study in individuals with cardiovascular disease. Eur. J. Prev. Cardiol. 2017, 24, 1880–1888. [Google Scholar] [CrossRef] [Green Version]
- Brouwer, S.I.; Küpers, L.K.; Kors, L.; Sijtsma, A.; Sauer, P.J.J.; Renders, C.M.; Corpeleijn, E. Parental physical activity is associated with objectively measured physical activity in young children in a sex-specific manner: The GECKO Drenthe cohort. BMC Public Health 2018, 18, 1033. [Google Scholar] [CrossRef]
- Zecevic, C.A.; Tremblay, L.; Lovsin, T.; Michel, L. Parental Influence on Young Children’s Physical Activity. Int. J. Pediatr. 2010, 2010, 468526. [Google Scholar] [CrossRef] [Green Version]
- Bartley, M.; Owen, C. Relation between socioeconomic status, employment, and health during economic change, 1973–1993. BMJ 1996, 313, 445–449. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Armstrong, J.; Dorosty-Motlagh, A.-R.; Emmett, P.; Ness, A.; Rogers, I.; Steer, C.; Sherriff, A. Early life risk factors for obesity in childhood: Cohort study. BMJ 2005, 330, 1357. [Google Scholar] [CrossRef] [Green Version]
- Whitaker, K.L.; Jarvis, M.J.; Beeken, R.J.; Boniface, D.; Wardle, J. Comparing maternal and paternal intergenerational transmission of obesity risk in a large population-based sample. Am. J. Clin. Nutr. 2010, 91, 1560–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, L.J.; Hawkins, S.S.; Cole, T.J.; Dezateux, C.; Millennium Cohort Study Child Health Group. Risk factors for rapid weight gain in preschool children: Findings from a UK-wide prospective study. Int. J. Obes. 2010, 34, 624–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, P.J.; Okely, A.D.; Cliff, D.P.; Jones, R.A.; Baur, L.A. Correlates of objectively measured physical activity in obese children. Obesity 2008, 16, 2634–2641. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Guthrie, C.; Sanderson, S.; Birch, L.; Plomin, R. Food and activity preferences in children of lean and obese parents. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 971–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, J.S.; Fisher, J.O.; Birch, L.L. Parental influence on eating behavior: Conception to adolescence. J. Law Med. Ethics. 2007, 35, 22–34. [Google Scholar] [CrossRef] [Green Version]
- Yee, A.Z.; Lwin, M.O.; Ho, S.S. The influence of parental practices on child promotive and preventive food consumption behaviors: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 47. [Google Scholar] [CrossRef]
- Bhupathiraju, S.N.; Hu, F.B. Epidemiology of Obesity and Diabetes and Their Cardiovascular Complications. Circ. Res. 2016, 118, 1723–1735. [Google Scholar] [CrossRef]
- Morandi, A.; Meyre, D.; Lobbens, S.; Kleinman, K.; Kaakinen, M.; Rifas-Shiman, S.L.; Vatin, V.; Gaget, S.; Pouta, A.; Hartikainen, A.L.; et al. Estimation of newborn risk for child or adolescent obesity: Lessons from longitudinal birth cohorts. PLoS ONE 2012, 7, e49919. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total Sample | By Economic Classification * | |||||
|---|---|---|---|---|---|---|
| Low Income | Under Economic Crisis | High Income | p-Value | |||
| (n = 12,030) | (n = 3281) | (n = 3948) | (n = 4801) | |||
| Child sex (%) | boy | 49.4 | 48.5 | 50.0 | 50.0 | 0.260 |
| girl | 50.6 | 51.5 | 50.0 | 50.0 | ||
| Child age [mean (SD)] | 8.2 (1.0) | 8.5 (1.0) a,b | 7.8 (0.9) a,c | 8.3 (1.0) b,c | <0.001 | |
| Age of Mother (%) | <45 years old | 90.4 | 93.1 a | 85.6 a,c | 91.9 c | <0.001 |
| ≥45 years old | 9.6 | 6.9 a | 14.4 a,c | 8.1 c | ||
| Age of Father (%) | <45 years old | 77.7 | 81.3 a | 68.6 a,c | 83.3 c | <0.001 |
| ≥45 years old | 22.3 | 18.7 a | 31.4 a,c | 16.7 c | ||
| Education of Mother (%) ** | <9 years | 8.4 | 11.9 a,b | 7.7 a,c | 4.1 b,c | <0.001 |
| 9–14 years | 35.3 | 34.3 a | 39.2 a,c | 32.6 c | ||
| >14 years | 51.9 | 53.8 a | 53.1 b | 63.3 a,b | ||
| Education of Father (%) ** | <9 years | 9.7 | 10.9 b | 11.3 c | 6.2 b,c | <0.001 |
| 9–14 years | 44.4 | 48.3 a | 37.9 a,c | 45.5 c | ||
| >14 years | 46.0 | 40.8 a,b | 50.8 a | 48.3 b | ||
| Occupation of Mother (%) | unemployed/other # | 29.5 | 32.1 a,b | 35.5 a,c | 19.3 b,c | <0.001 |
| employed full-time | 57.5 | 62.0 a | 48.2 a,c | 60.9 c | ||
| employed part-time | 13.1 | 6.0 a,b | 16.5 a,c | 19.8 b,c | ||
| Occupation of Father (%) | unemployed/other # | 14.1 | 19.2 a,b | 11.9 a,c | 9.4 b,c | <0.001 |
| employed full-time | 81.5 | 75.4a,b | 83.1a,c | 88.6 b,c | ||
| employed part-time | 4.3 | 5.4 b | 5.0 c | 2.0 b,c | ||
| BMI of Mother (%) | <25 kg/m2 | 66.8 | 70.0 a,b | 65.4 a | 63.5 b | <0.001 |
| 25–29.9 kg/m2 | 22.3 | 20.1 b | 23.0 c | 24.5 b,c | ||
| ≥30 kg/m2 | 11.0 | 9.8 b | 11.6 c | 11.9 b,c | ||
| BMI of Father (%) | <25 kg/m2 | 31.5 | 27.5 b | 30.3 c | 39.0 b,c | <0.001 |
| 25–29.9 kg/m2 | 47.5 | 47.0 | 49.5 c | 45.8 c | ||
| ≥30 kg/m2 | 21.0 | 25.5 a,b | 20.1 a,c | 15.2 b,c | ||
| Parental BMI classification (%) | Both parents without obesity (BMI < 30 kg/m2) | 72.1 | 68.2 a,b | 72.9 a,c | 77.0 b,c | <0.001 |
| At least one parent with obesity (BMI ≥ 30 kg/m2) | 24.1 | 28.1 a,b | 22.9 a,c | 19.7 b,c | ||
| Both parents with obesity (BMI ≥ 30 kg/m2) | 3.8 | 3.7 | 4.2 | 3.3 | ||
| Children’s Weight Status | |||
|---|---|---|---|
| Under- & Normal Weight | Overweight | Obesity | |
| Country economic classification * | % | % | % |
| Low Income | 74.5 a,b | 17.4 a,b | 8.2 a |
| Under economic crisis | 68.0 a,c | 22.7 a,c | 9.3 b |
| High income | 82.4 b,c | 13.4 b,c | 4.2 a,b |
| p-value | <0.001 | ||
| Age of mother | |||
| <45 years old | 75.0 a | 17.8 | 7.2 a |
| ≥45 years old | 72.1 a | 18.8 | 9.1 a |
| p-value | 0.037 | ||
| Age of father | |||
| <45 years old | 75.3 | 17.7 | 7.0 |
| ≥45 years old | 73.7 | 19.2 | 7.1 |
| p-value | 0.231 | ||
| Education of mother ** | |||
| <9 years | 71.4 a | 17.9 | 10.7 a |
| 9–14 years | 69.9 b | 20.0 a | 10.0 b |
| >14 years | 78.6 a,b | 16.3 a | 5.1 a,b |
| p-value | <0.001 | ||
| Education of father ** | |||
| <9 years | 69.5 a | 18.5 | 11 a,b |
| 9–14 years | 72.1 b | 19.4 a | 8.4 a,c |
| >14 years | 79.6 a,b | 15.9 a | 4.5 b,c |
| p-value | <0.001 | ||
| Occupation of mother | |||
| unemployed/other # | 71.6 a,b | 19.4 a | 9.1 a,b |
| employed full-time | 75.7 a | 17.4 | 6.8 a |
| employed part-time | 78 b | 16.2 a | 5.8 b |
| p-value | <0.001 | ||
| Occupation of father | |||
| unemployed/other # | 73.4 | 18.5 | 8.1 |
| employed full-time | 75.8 | 17.6 | 6.6 a |
| employed part-time | 70.9 | 18.7 | 10.4 a |
| p-value | 0.007 | ||
| Dependent Variable: Childhood Obesity | ||
|---|---|---|
| Independent Variables | OR | 95% CI |
| Sex | ||
| boys | 1.00 | |
| girls | 1.01 | 0.86, 1.20 |
| Country economic classification * | ||
| High income | 1.00 | |
| Low Income | 2.11 | 1.62, 2.74 |
| Under economic crisis | 2.48 | 1.89, 3.24 |
| Age of mother | ||
| <45 years old | 1.00 | |
| ≥45 years old | 1.17 | 0.88, 1.55 |
| Education of mother ** | ||
| >14 years | 1.00 | |
| 9–14 years | 1.56 | 1.26, 1.93 |
| <9 years | 1.28 | 0.88, 1.86 |
| Education of father ** | ||
| >14 years | 1.00 | |
| 9–14 years | 1.63 | 1.31, 2.03 |
| <9 years | 2.16 | 1.54, 3.05 |
| Occupation of mother | ||
| unemployed/other # | 1.00 | |
| employed full-time | 1.07 | 0.88, 1.31 |
| employed part-time | 0.88 | 0.64, 1.20 |
| Occupation of father | ||
| unemployed/other # | 1.00 | |
| employed full-time | 1.09 | 0.85, 1.40 |
| employed part-time | 1.25 | 0.83, 1.89 |
| Parental weight status | ||
| Both parents without obesity (BMI < 30 kg/m2) | 1.00 | |
| At least one parent with obesity (BMI ≥ 30 kg/m2) | 2.49 | 2.07, 2.99 |
| Both parents with obesity (BMI ≥ 30 kg/m2) | 6.83 | 5.15, 9.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moschonis, G.; Siopis, G.; Anastasiou, C.; Iotova, V.; Stefanova, T.; Dimova, R.; Rurik, I.; Radó, A.S.; Cardon, G.; De Craemer, M.; et al. Prevalence of Childhood Obesity by Country, Family Socio-Demographics, and Parental Obesity in Europe: The Feel4Diabetes Study. Nutrients 2022, 14, 1830. https://doi.org/10.3390/nu14091830
Moschonis G, Siopis G, Anastasiou C, Iotova V, Stefanova T, Dimova R, Rurik I, Radó AS, Cardon G, De Craemer M, et al. Prevalence of Childhood Obesity by Country, Family Socio-Demographics, and Parental Obesity in Europe: The Feel4Diabetes Study. Nutrients. 2022; 14(9):1830. https://doi.org/10.3390/nu14091830
Chicago/Turabian StyleMoschonis, George, George Siopis, Costas Anastasiou, Violeta Iotova, Tanya Stefanova, Roumyana Dimova, Imre Rurik, Anette Si Radó, Greet Cardon, Marieke De Craemer, and et al. 2022. "Prevalence of Childhood Obesity by Country, Family Socio-Demographics, and Parental Obesity in Europe: The Feel4Diabetes Study" Nutrients 14, no. 9: 1830. https://doi.org/10.3390/nu14091830