
Effects of a 12-Month Hybrid (In-Person + Virtual) Education Program in the Glycemic Status of Arab Youth

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
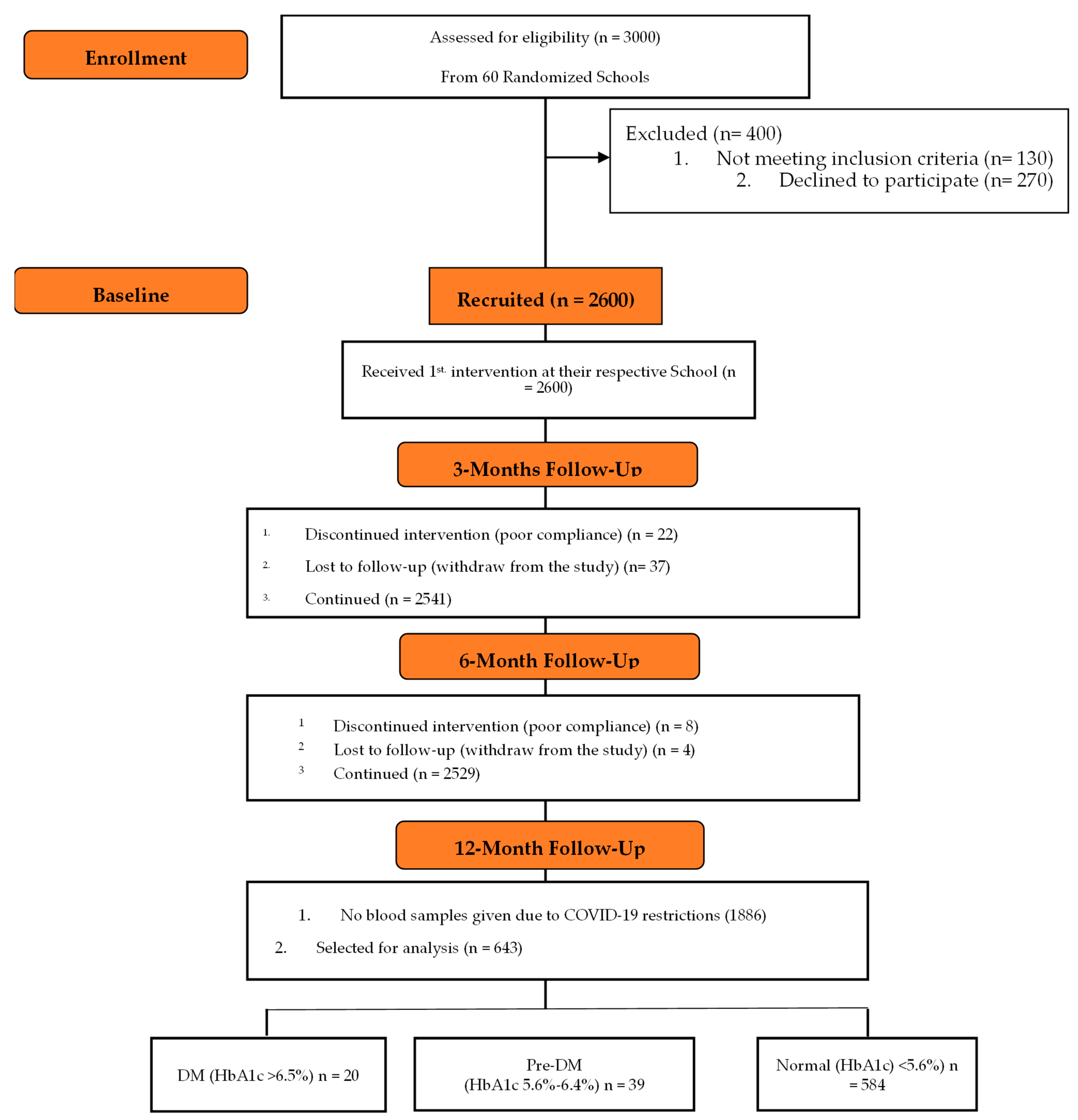
2.1. Participants
2.2. Intervention
2.3. Anthropometric Measurements
2.4. Biochemical Analyses
2.5. Definition of DM
2.6. Physical Activity
2.7. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zimmet, P.; Alberti, K.G.; Shaw, J. Global and societal implications of the diabetes epidemic. Nature 2001, 414, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Bloomgarden, Z.T. Type 2 diabetes in the young: The evolving epidemic. Diabetes Care 2004, 27, 998–1010. [Google Scholar] [CrossRef] [Green Version]
- Alberti, G.; Zimmet, P.; Shaw, J.; Bloomgarden, Z.; Kaufman, F.; Silink, M.; Consensus Workshop Group. Type 2 diabetes in the young: The evolving epidemic: The international diabetes federation consensus workshop. Diabetes Care 2004, 27, 1798–1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matyka, K.A. Type 2 diabetes in childhood: Epidemiological and clinical aspects. Br. Med. Bull. 2008, 86, 59–75. [Google Scholar] [CrossRef] [Green Version]
- Alotaibi, M.; Alibrahim, L.; Alharbi, N. Challenges associated with treating children with diabetes in Saudi Arabia. Diabetes Res. Clin. Pract. 2016, 120, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Patterson, C.; Guariguata, L.; Dahlquist, G.; Soltesz, G.; Ogle, G.; Silink, M. Diabetes in the young—A global view and worldwide estimates of numbers of children with type 1 diabetes. Diabetes Res. Clin. Pract. 2014, 103, 161–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gale, E.A. The rise of childhood type 1 diabetes in the 20th century. Diabetes 2002, 51, 3353–3361. [Google Scholar] [CrossRef] [PubMed]
- Awa, W.L.; Fach, E.; Krakow, D.; Welp, R.; Kunder, J.; Voll, A.; Zeyfang, A.; Wagner, C.; Schtt, M.; Boehm, B.; et al. DPV Initiative; German BMBF Competence Networks Diabetes mellitus and Obesity. Type 2 diabetes from pediatric to geriatric age: Analysis of gender and obesity among 120,183 patients from the German/Austrian DPV database. Eur. J. Endocrinol. 2012, 167, 245–254. [Google Scholar] [CrossRef]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. NCHS Data Brief 2017, 288, 1–8. [Google Scholar] [PubMed]
- Scott, C.R.; Smith, J.M.; Cradock, M.M.; Pihoker, C. Characteristics of youth-onset noninsulin-dependent diabetes mellitus and insulin-dependent diabetes mellitus at diagnosis. Pediatrics 1997, 100, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Articles, S. Screening for obesity in children and Adolescents: US preventive Services Task Force. Recomm. Statement 2010, 125, 361–367. [Google Scholar]
- El Mouzan, M.I.; Foster, P.J.; Al Herbish, A.S.; Al Salloum, A.A.; Al Omer, A.A.; Qurachi, M.M.; Kecojevic, T. Prevalence of overweight and obesity in Saudi children and adolescents. Ann. Saudi Med. 2010, 30, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Enazy, W.H.; Al Dahi, S.K.; Al Hariri, I.M. Prevalence of overweight and obesity among Saudi primary school students in Tabuk, Saudi Arabia. Sch. J. Otolarngol. 2014, 2, 13. [Google Scholar]
- AlBuhairan, F.S.; Tamim, H.; Al Dubayee, M.; AlDhukair, S.; Al Shehri, S.; Tamimi, W.; El Bcheraoui, C.; Magzoub, M.E.; De Vries, N.; Al Alwan, I. Time for an adolescent health surveillance system in Saudi Arabia: Findings from “jeeluna”. J. Adolesc. Health 2015, 57, 263–269. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Preventing Suicide: A Global Imperative; WHO Press: Geneva, Switzerland, 2014; Available online: http://apps.who.int/iris/bitstream/10665/131056/1/9789241564779_eng.pdf?ua (accessed on 16 October 2021).
- Al-Hussaini, A.; Bashir, M.S.; Khormi, M.; AlTuraiki, M.; Alkhamis, W.; Alrajhi, M.; Halal, T. Overweight and obesity among Saudi children and adolescents: Where do we stand today? Saudi J. Gastroenterol. 2019, 25, 229–235. [Google Scholar] [CrossRef]
- Al-Rubeaan, K. National surveillance for type 1, type 2 diabetes and prediabetes among children and adolescents: A population-based study (SAUDI-DM). J. Epidemiol. Commun. Health 2015, 69, 1045–1051. [Google Scholar] [CrossRef] [Green Version]
- Braham, R.; Robert, A.A.; Mujammami, M.; Ahmad, R.A.; Zitouni, M.; Sobki, S.H.; Al Dawish, M.A. Double diabetes in Saudi Arabia: A new entity or an underestimated condition. World J. Diabetes 2016, 7, 621–626. [Google Scholar] [CrossRef]
- Alfawaz, H.; Naeef, A.F.; Wani, K.; Khattak, M.N.K.; Sabico, S.; Alnaami, A.M.; Al-Daghri, N.M. Improvements in Glycemic, Micronutrient, and Mineral Indices in Arab Adults with Pre-Diabetes Post-Lifestyle Modification Program. Nutrients 2019, 11, 2775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hamdan, R.; Avery, A.; Al-Disi, D.; Sabico, S.; Al-Daghri, N.M.; McCullough, F. Efficacy of lifestyle intervention program for Arab women with prediabetes using social media as an alternative platform of delivery. J. Diabetes Investig. 2021, 12, 1872–1880. [Google Scholar] [CrossRef]
- Wani, K.; Alfawaz, H.; Alnaami, A.M.; Sabico, S.; Khattak, M.N.K.; Al-Attas, O.; Alokail, M.S.; Alharbi, M.; Chrousos, G.; Kumar, S.; et al. Effects of A 12-Month Intensive Lifestyle Monitoring Program in Predominantly Overweight/Obese Arab Adults with Prediabetes. Nutrients 2020, 12, 464. [Google Scholar] [CrossRef] [Green Version]
- Al-Daghri, N.M.; Rahman, S.; Sabico, S.; Yakout, S.; Wani, K.; Al-Attas, O.S.; Saravanan, P.; Tripathi, G.; McTernan, P.G.; Alokail, M.S. Association of Vitamin B12 with Pro-Inflammatory Cytokines and Biochemical Markers Related to Cardiometabolic Risk in Saudi Subjects. Nutrients 2016, 8, 460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.S.; Alkharfy, K.M.; Hussain, T.; Sabico, S. Gender differences exist in the association of leptin and adiponectin levels with insulin resistance parameters in prepubertal Arab children. J. Pediatr. Endocrinol. Metab. 2011, 24, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43 (Suppl. 1), S14–S31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monzavi, R.; Dreimane, D.; Geffner, M.E.; Braun, S.; Conrad, B.; Klier, M.; Kaufman, F.R. Improvement in risk factors for metabolic syndrome and insulin resistance in overweight youth who are treated with lifestyle intervention. Pediatrics 2006, 117, e1111–e1118. [Google Scholar] [CrossRef]
- Arabic Short Version of International Physical Activity Questionnaire. Stockholm: Karolinska Institutet. Available online: http://www.ipaq.ki.se/questionnaires/ArabicIQShtel_coverpage.pdf (accessed on 2 July 2014).
- Al-Hazzaa, H.M. The public health burden of physical inactivity in Saudi Arabia. J. Family Community Med. 2004, 11, 45–51. [Google Scholar] [PubMed]
- Awadalla, N.J.; Aboelyazed, A.E.; Hassanein, M.A.; Khalil, S.N.; Aftab, R.; Gaballa, I.I.; Mahfouz, A.A. Assessment of physical inactivity and perceived barriers to physical activity among health college students, south-western Saudi Arabia. East. Mediterr. Health J. 2014, 20, 597–604. [Google Scholar] [CrossRef]
- Moshibah, A.M.; Almazarigeh, S.D.; Al-Dowan, A.A.; Assiri, H.M.; Al-Shahrani, S.F.; Assiri, I.M. Physical activity and quality of life among Saudi Adults. Al-Azhar Assiut Med. J. 2015, 13, 126–131. [Google Scholar]
- Lindström, J.; Eriksson, J.G.; Valle, T.T.; Aunola, S.; Cepaitis, Z.; Hakumäki, M.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; et al. Prevention of diabetes mellitus in subjects with impaired glucose tolerance in the Finnish Diabetes Prevention Study: Results from a randomized clinical trial. J. Am. Soc. Nephrol. 2003, 14 (Suppl. 2), S108–S113. [Google Scholar] [CrossRef] [Green Version]
- Savoye, M.; Caprio, S.; Dziura, J.; Camp, A.; Germain, G.; Summers, C.; Li, F.; Shaw, M.; Nowicka, P.; Kursawe, R.; et al. Tamborlane; Reversal of Early Abnormalities in Glucose Metabolism in Obese Youth: Results of an Intensive Lifestyle Randomized Controlled Trial. Diabetes Care 2014, 37, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Amer, O.E.; Sabico, S.; Alfawaz, H.A.; Aljohani, N.; Hussain, S.D.; Alnaami, A.M.; Wani, K.; Al-Daghri, N.M. Reversal of Prediabetes in Saudi Adults: Results from an 18 Month Lifestyle Intervention. Nutrients 2020, 12, 804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Watson, P.G.; Mendoza, J.T.; Smith, K.A.; et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [PubMed]
- Numbenjapon, N.; Nakavachara, P.; Santiprabhob, J.; Kiattisakthavee, P.; Wongarn, R.; Likitmaskul, S. Successful strategy to improve glucose tolerance in Thai obese youth. J. Med. Assoc. Thai. 2010, 93 (Suppl. 6), S131–S138. [Google Scholar] [PubMed]
- Freemark, M.; Bursey, D. The effects of metformin on body mass index and glucose tolerance in obese adolescents with fasting hyperinsulinemia and a family history of type 2 diabetes. Pediatrics 2001, 107, E55. [Google Scholar] [CrossRef] [Green Version]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Mei, Z.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. CDC growth charts: United States. Adv Data 2000, 314, 1–27. [Google Scholar]
- Yeckel, C.W.; Weiss, R.; Dziura, J.; Taksali, S.E.; Dufour, S.; Burgert, T.S.; Tamborlane, W.V.; Caprio, S. Validation of insulin sensitivity indices from oral glucose tolerance test parameters in obese children and adolescents. J. Clin. Endocrinol. Metab. 2004, 89, 1096–1101. [Google Scholar] [CrossRef] [Green Version]
- Savoye, M.; Nowicka, P.; Shaw, M.; Yu, S.; Dziura, J.; Chavent, G.; O’Malley, G.; Serrecchia, J.B.; Tamborlane, W.V.; Caprio, S. Long term results of an obesity program in an ethnically diverse pediatric population. Pediatrics 2011, 127, 402–410. [Google Scholar] [CrossRef] [Green Version]
- Al-Daghri, N.M.; Sabico, S.; Al-Saleh, Y.; Al-Attas, O.S.; Alnaami, A.M.; AlRehaili, M.M.; Al-Harbi, M.; Alfawaz, H.; Chrousos, G.; Alokail, M.S. Calculated adiposity and lipid indices in healthy Arab children as influenced by vitamin D status. J. Clin. Lipidol. 2016, 10, 775–781. [Google Scholar] [CrossRef]
- Johnson, S.T.; Newton, A.S.; Chopra, M.; Buckingham, J.; Huang, T.T.; Franks, P.W.; Jetha, M.M.; Ball, G.D. In search of quality evidence for lifestyle management and glycemic control in children and adolescents with type 2 diabetes: A systematic review. BMC Pediatr. 2010, 10, 97. [Google Scholar] [CrossRef] [Green Version]
- Amer, O.E.; Sabico, S.; Khattak, M.N.K.; Alnaami, A.M.; Aljohani, N.J.; Alfawaz, H.; AlHameidi, A.; Al-Daghri, N.M. Increasing Prevalence of Pediatric Metabolic Syndrome and Its Components among Arab Youth: A Time-Series Study from 2010–2019. Children 2021, 8, 1129. [Google Scholar] [CrossRef]
- Rodríguez-Muñoz, S.; Corella, C.; Abarca-Sos, A.; Zaragoza, J. Validation of three short physical activity questionnaires with accelerometers among university students in Spain. J. Sports Med. Phys. Fit. 2017, 57, 1660–1668. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | All | Boys | Girls | p-Value |
|---|---|---|---|---|
| N | 643 | 300 | 343 | |
| Age | 14.8 ± 1.7 | 14.7 ± 1.6 | 14.9 ± 1.8 | 0.13 |
| Height (cm) | 156.2 ± 9.3 | 158.2 ± 10.5 | 154.4 ± 7.6 | <0.001 |
| Height Z-score | 0.0 ± 1.0 | 0.22 ± 1.1 | −0.19 ± 0.8 | <0.001 |
| Weight (kg) | 56.4 ± 17.5 | 60.1 ± 20.3 | 53.4 ± 14.1 | <0.001 |
| Weight Z-score | 0.0 ± 1.0 | 0.21 ± 1.2 | −0.18 ± 0.8 | <0.001 |
| BMI (kg/m2) | 23.0 ± 6.0 | 23.7 ± 6.7 | 22.4 ± 5.4 | 0.009 |
| BMI Z-score | 0.0 ± 1.0 | 0.12 ± 1.1 | −0.10 ± 0.9 | 0.009 |
| Glucose | 5.21 ± 0.8 | 5.30 ± 1.1 | 5.13 ± 0.5 | 0.008 |
| HbA1c (%) | 5.11 ± 0.6 | 5.21 ± 0.6 | 5.02 ± 0.6 | <0.001 |
| Physical Activities Status N (%) | <0.001 | |||
| Yes | 301 (46.8) | 117 (39.0) | 184 (53.6) | |
| No | 342 (53.2) | 183 (61.0) | 159 (46.4) | |
| DM N(%) | 0.45 | |||
| Normal | 584 (90.8) | 269 (89.7) | 315 (91.8) | |
| Pre-DM | 39 (6.1) | 22 (7.3) | 17 (5.0) | |
| Diabetes | 20 (3.1) | 9 (3.0) | 11 (3.2) | |
| Obesity Status N (%) | <0.001 | |||
| Normal | 391 (64.2) | 159 (57.4) | 232 (69.9) | |
| Overweight | 112 (18.4) | 48 (17.3) | 64 (19.3) | |
| Obese | 106 (17.4) | 70 (25.3) | 36 (10.8) |
| Parameters | Normal | Prediabetes | Diabetes | Between Group Adjusted p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | p-Value | Baseline | Follow-Up | p-Value | Baseline | Follow-Up | p-Value | ||
| Age (Years) | 14.8 ± 1.7 | 15.3 ± 1.7 | 15.3 ± 1.3 | |||||||
| Weight (kg) | 55.8 ± 17.1 | 57.8 ± 15.6 | <0.001 | 65.8 ± 21.5 | 68.1 ± 19.1 | <0.001 | 54.9 ± 14.3 | 57.3 ± 13.3 | <0.001 | |
| Weight Z-score | −0.03 ± 0.9 | −0.04 ± 0.9 | 0.39 | 0.54 ± 1.2 | 0.61 ± 1.2 | 0.01 | −0.09 ± 0.8 | −0.07 ± 0.8 | 0.43 | |
| Height (cm) | 156.0 ± 9.3 | 164.6 ± 6.5 | <0.001 | 156.4 ± 9.9 | 166.8 ± 7.3 | <0.001 | 160.1 ± 7.3 | 166.4 ± 6.9 | 0.003 | |
| Height Z-score | −0.02 ± 1.0 | −0.03 ± 0.9 | 0.78 | 0.02 ± 1.1 | 0.32 ± 1.1 | 0.13 | 0.42 ± 0.8 | 0.25 ± 1.0 | 0.50 | |
| BMI (kg/m2) | 22.8 ± 5.9 | 21.4 ± 5.7 | <0.001 | 26.4 ± 6.7 | 24.3 ± 6.5 | <0.001 | 21.4 ± 4.9 | 20.6 ± 4.6 | 0.14 | |
| BMI Z-score | −0.02 ± 0.04 | −0.03 ± 0.04 | 0.81 | 0.48 ± 0.19 | 0.55 ± 0.18 | 0.29 | −0.17 ± 0.2 | −0.27 ± 0.2 | 0.28 | |
| Glucose | 5.2 ± 0.5 | 5.7 ± 2.8 | <0.001 | 5.4 ± 0.9 | 5.5 ± 2.2 | 0.89 | 6.6 ± 3.4 | 6.6 ± 3.4 | 0.99 | 0.02 |
| HbA1c (%) | 5.0 ± 0.3 | 5.3 ± 1.3 | <0.001 | 5.9 ± 0.2 | 5.3 ± 0.9 | <0.001 | 7.4 ± 0.9 | 5.9 ± 1.3 | <0.001 | 0.01 |
| BMI Status | Baseline | Post-Intervention | p-Value | |||
|---|---|---|---|---|---|---|
| Normal | Overweight | Obese | ||||
| Normal | 391 (64.3) | 372 (95.1) | 19 (4.9) | 0 (0.0) | <0.001 | |
| Overweight | 110 (18.3) | 53 (48.6) | 55 (49.5) | 2 (1.8) | ||
| Obese | 105 (17.4) | 3 (2.8) | 38 (35.8) | 65 (61.3) | ||
| Physical Activity (N) | ||||||
| Normal | High PA | 34 | 32 (94.1) | 2 (5.9) | 0 | 0.13 |
| Moderated PA | 143 | 140 (97.9) | 3 (2.1) | 0 | ||
| Low PA | 205 | 191 (93.2) | 14 (6.8) | 0 | ||
| Overweight | High PA | 13 | 8 (61.8) | 5 (38.5) | 0 | 0.10 |
| Moderated PA | 31 | 20 (64.5) | 11 (35.5) | 0 | ||
| Low PA | 66 | 25 (37.9) | 39 (59.1) | 2 (3.0) | ||
| Obese | High PA | 10 | 0 | 6 (60.0) | 4 (40.0) | 0.25 |
| Moderated PA | 35 | 2 (5.7) | 14 (40.0) | 19 (54.3) | ||
| Low PA | 60 | 1 (1.7) | 18 (30.0) | 41 (68.3) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Daghri, N.M.; Amer, O.E.; Hameidi, A.; Alfawaz, H.; Alharbi, M.; Khattak, M.N.K.; Alnaami, A.M.; Aljohani, N.J.; Alkhaldi, G.; Wani, K.; et al. Effects of a 12-Month Hybrid (In-Person + Virtual) Education Program in the Glycemic Status of Arab Youth. Nutrients 2022, 14, 1759. https://doi.org/10.3390/nu14091759
Al-Daghri NM, Amer OE, Hameidi A, Alfawaz H, Alharbi M, Khattak MNK, Alnaami AM, Aljohani NJ, Alkhaldi G, Wani K, et al. Effects of a 12-Month Hybrid (In-Person + Virtual) Education Program in the Glycemic Status of Arab Youth. Nutrients. 2022; 14(9):1759. https://doi.org/10.3390/nu14091759
Chicago/Turabian StyleAl-Daghri, Nasser M., Osama E. Amer, AbdulAziz Hameidi, Hanan Alfawaz, Mohammed Alharbi, Malak N. K. Khattak, Abdullah M. Alnaami, Naji J. Aljohani, Ghadah Alkhaldi, Kaiser Wani, and et al. 2022. "Effects of a 12-Month Hybrid (In-Person + Virtual) Education Program in the Glycemic Status of Arab Youth" Nutrients 14, no. 9: 1759. https://doi.org/10.3390/nu14091759