
Characterizing Undernourished Children Under-Five Years Old with Diarrhoea in Mozambique: A Hospital Based Cross-Sectional Study, 2015–2019

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
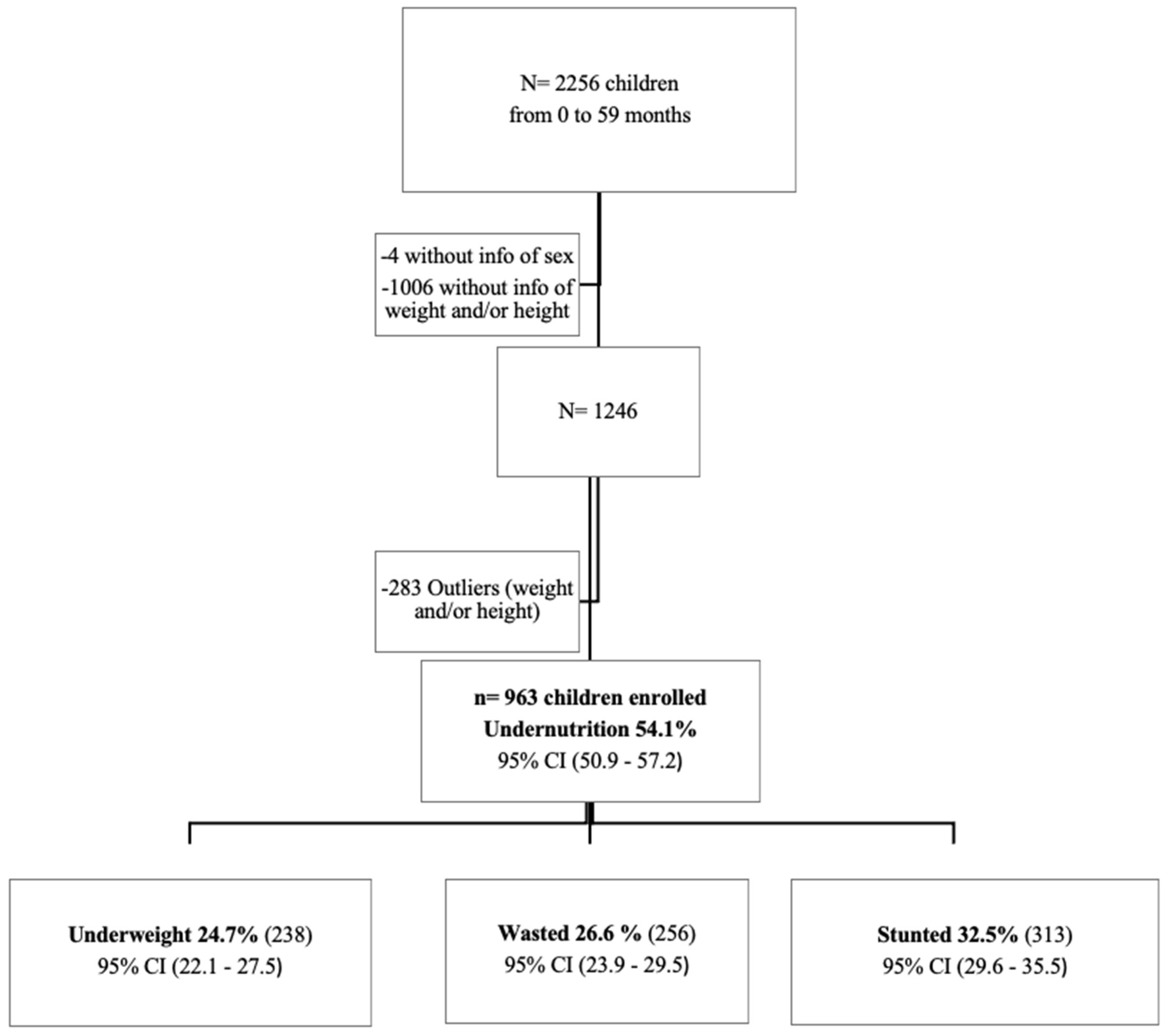
2.1. Study Design and Population
2.2. Case Report Form
2.3. Anthropometric Measurements
2.4. Sample Collection and Laboratory Procedures
2.5. Statistical Analysis
3. Results
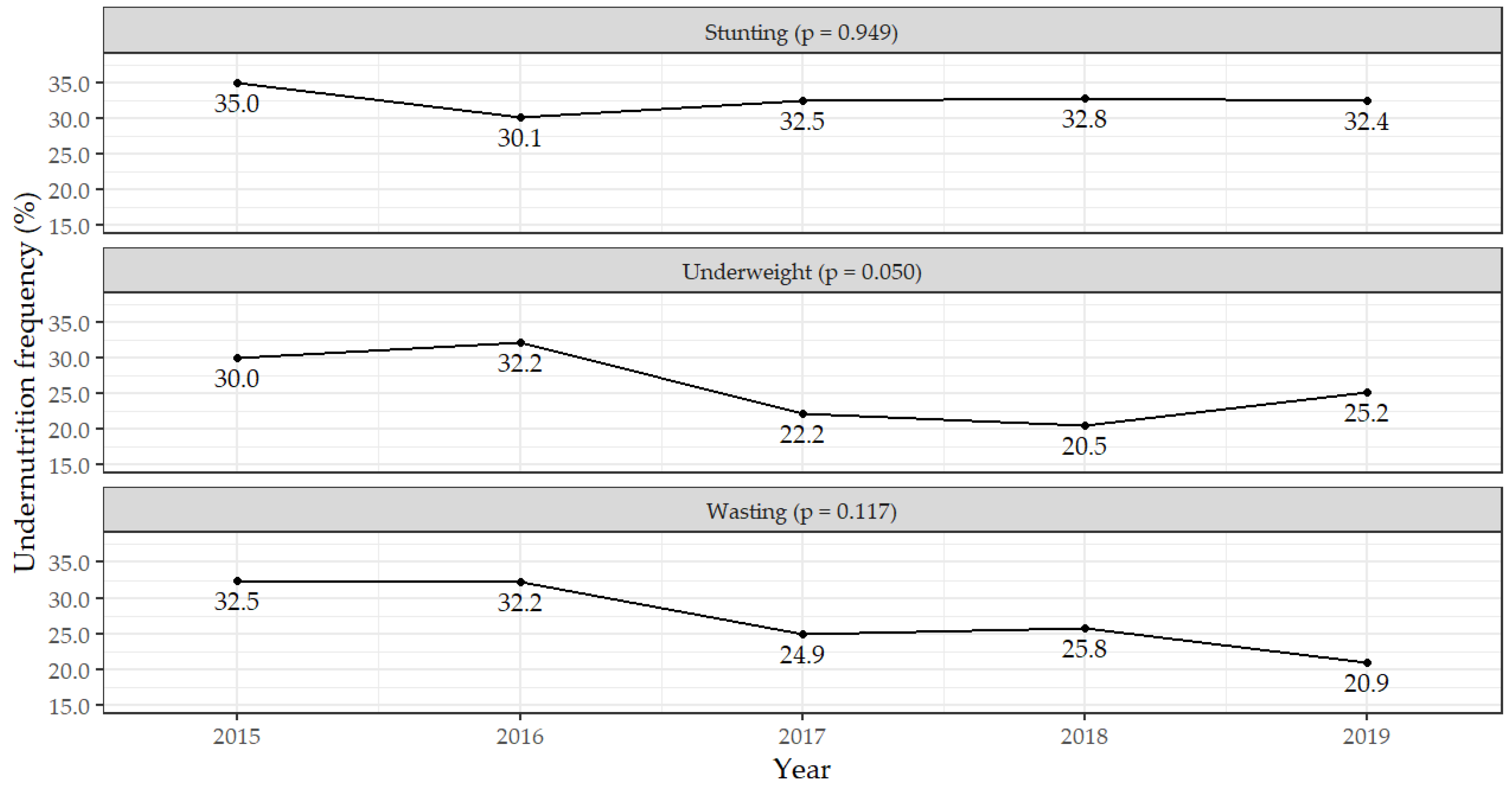
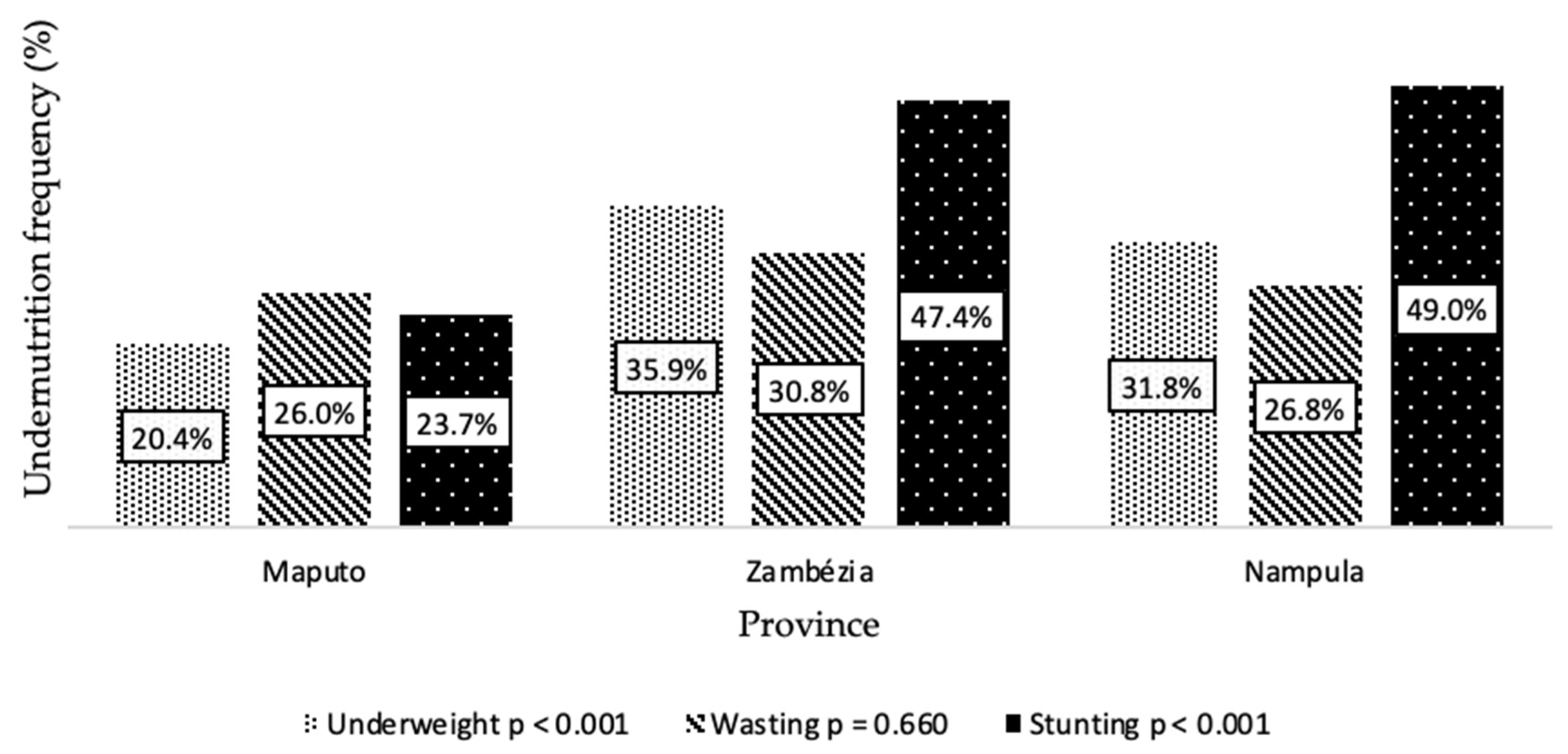
3.1. Frequency of Undernutrition Status across Years and Sociodemographic Characteristics
3.2. Clinical Characteristics
3.3. Factors Associated with Nutritional Status in Children with Diarrhoea
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferdous, F.; Das, S.K.; Ahmed, S.; Farzana, F.D.; Latham, J.R.; Chisti, M.J.; Ud-Din, A.I.M.S.; Azmi, I.J.; Talukder, K.A.; Faruque, A.S.G. Severity of Diarrhea and Malnutrition among Under Five-Year-Old Children in Rural Bangladesh. Am. J. Trop. Med. Hyg. 2013, 89, 223–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fonseca, A.M.; Fernandes, N.; Ferreira, F.S.; Gomes, J.; Centeno-Lima, S. Intestinal Parasites in Children Hospitalized at the Central Hospital in Maputo, Mozambique. J. Infect. Dev. Ctries. 2014, 8, 786–789. [Google Scholar] [CrossRef] [PubMed]
- Paulson, K.R.; Kamath, A.M.; Alam, T.; Bienhoff, K.; Abady, G.G.; Abbas, J.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abd-Elsalam, S.M.; et al. Global, Regional, and National Progress towards Sustainable Development Goal 3.2 for Neonatal and Child Health: All-Cause and Cause-Specific Mortality Findings from the Global Burden of Disease Study 2019. Lancet 2021, 398, 870–905. [Google Scholar] [CrossRef]
- Chissaque, A.; de Deus, N.; Vubil, D.; Mandomando, I. The Epidemiology of Diarrhea in Children Under 5 Years of Age in Mozambique. Curr. Trop. Med. Rep. 2018, 5, 115–124. [Google Scholar] [CrossRef]
- WHO. Number of Under-Five Deaths—by Cause. Available online: https://www.who.int/data/maternal-newborn-child-adolescent-ageing/documents/mca (accessed on 28 January 2021).
- MISAU; INE; ICF. Inquérito de Indicadores de Imunização, Malária e HIV/SIDA Em Moçambique (IMASIDA) 2015; MISAU: Misau, NI, USA; INE: Mexico City, Mexico; ICF: Lexington, KY, USA, 2018. [Google Scholar]
- Tette, E.M.A.; Sifah, E.K.; Nartey, E.T. Factors Affecting Malnutrition in Children and the Uptake of Interventions to Prevent the Condition. BMC Pediatr. 2015, 15, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micha, R.; Mannar, V.; Afshin, A.; Allemandi, L.; Baker, P.; Battersby, J.; Bhutta, Z.; Chen, K.; Corvalan, C.; Di Cesare, M.; et al. 2020 Global Nutrition Report: Action on Equity to End Malnutrition. Available online: https://globalnutritionreport.org/reports/2020-global-nutrition-report/ (accessed on 25 January 2021).
- WHO; UNICEF; World Bank. Levels and Trends in Child Malnutrition: Key Findings of the 2019 Edition of the Joint Child Malnutrition Estimates; World Health Organization: Geneva, Switzerland, 2019; p. 16. [Google Scholar]
- WHO. Prevalence of Stunting among Children Under-Five Years of Age (Height-for-Age <-2SD of the Median) (SDG 2.2.1). Available online: https://www.who.int/data/maternal-newborn-child-adolescent-ageing/indicator-explorer-new/mca/prevalence-of-stunting-among-children-under-five-years-of-age-(height-for-age--2sd-of-the-median) (accessed on 28 January 2021).
- WHO. Prevalence of Wasting among Children Under-Five Years of Age (Weight-for-Height <-2SD of the Median). Available online: https://www.who.int/data/maternal-newborn-child-adolescent-ageing/indicator-explorer-new/mca/prevalence-of-wasting-among-children-under-five-years-of-age-(weight-for-height--2sd-of-the-median) (accessed on 28 January 2021).
- WHO Prevalence of Underweight among Children Under-Five Years of Age (Weight-for-Age <-2SD of the Median). Available online: https://www.who.int/data/maternal-newborn-child-adolescent-ageing/indicator-explorer-new/mca/prevalence-of-underweight-among-children-under-five-years-of-age-(weight-for-age--2sd-of-the-median) (accessed on 28 January 2021).
- Brown, K.H. Diarrhea and Malnutrition. J. Nutr. 2003, 133, 328s–332s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acácio, S.; Mandomando, I.; Nhampossa, T.; Quintó, L.; Vubil, D.; Sacoor, C.; Kotloff, K.; Farag, T.; Nasrin, D.; Macete, E.; et al. Risk Factors for Death among Children 0–59 Months of Age with Moderate-to-Severe Diarrhea in Manhiça District, Southern Mozambique. BMC Infect. Dis. 2019, 19, 322. [Google Scholar] [CrossRef]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and Child Undernutrition: Global and Regional Exposures and Health Consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Wasihun, A.G.; Dejene, T.A.; Teferi, M.; Marugán, J.; Negash, L.; Yemane, D.; McGuigan, K.G. Risk Factors for Diarrhoea and Malnutrition among Children under the Age of 5 Years in the Tigray Region of Northern Ethiopia. PLoS ONE 2018, 13, e0207743. [Google Scholar] [CrossRef]
- Akombi, B.J.; Agho, K.E.; Renzaho, A.M.; Hall, J.J.; Merom, D.R. Trends in Socioeconomic Inequalities in Child Undernutrition: Evidence from Nigeria Demographic and Health Survey (2003–2013). PLoS ONE 2019, 14, e0211883. [Google Scholar] [CrossRef]
- Global Network Against Food Crises; Food Security Information Network. 2020 Global Report on Food Crises: Joint Analyses for Better Decisions; 2020. Available online: https://www.wfp.org/publications/2020-global-report-food-crises (accessed on 28 January 2021).
- UNICEF. Pobreza Infantil e Disparidades Em Moçambique 2010—Sobrevivência e Desenvolvimento Infantil; UNICEF: Maputo, Mozambique, 2011. [Google Scholar]
- Nhampossa, T.; Sigaúque, B.; Machevo, S.; Macete, E.; Alonso, P.; Bassat, Q.; Menéndez, C.; Fumadó, V. Severe Malnutrition among Children under the Age of 5 Years Admitted to a Rural District Hospital in Southern Mozambique. Public Health Nutr. 2013, 16, 1565–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, M.S.; Howlader, T.; Masud, M.S.; Rahman, M.L. Association of Low-Birth Weight with Malnutrition in Children under Five Years in Bangladesh: Do Mother’s Education, Socio-Economic Status, and Birth Interval Matter? PLoS ONE 2016, 11, e0157814. [Google Scholar]
- Bauhofer, A.F.L.; Cossa-Moiane, I.; Marques, S.; Guimarães, E.L.; Munlela, B.; Anapakala, E.; Chilaúle, J.J.; Cassocera, M.; Langa, J.S.; Chissaque, A.; et al. Intestinal Protozoan Infections among Children 0-168 Months with Diarrhea in Mozambique: June 2014—January 2018. PLoS Negl. Trop. Dis. 2020, 14, e0008195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- INS; INE; ICF. Inquérito Nacional de Prevalência, Riscos Comportamentais e Informação Sobre o HIV e SIDA Em Moçambique 2009; INS: Calverton, MD, USA; INE: Mexico City, Mexico; ICF: Lexington, KY, USA, 2010. [Google Scholar]
- Pedrini, M.; Moraleda, C.; Macete, E.; Gondo, K.; Brabin, B.J.; Menéndez, C. Clinical, Nutritional and Immunological Characteristics of HIV-Infected Children in an Area of High HIV Prevalence. J. Trop. Pediatr. 2015, 61, 286–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chissaque, A.; Cassocera, M.; Gasparinho, C.; Langa, J.S.; Bauhofer, A.F.L.; Chilaúle, J.J.; João, E.D.; Munlela, B.A.; Sambo, J.A.M.; Boene, S.S.; et al. Rotavirus A Infection in Children under Five Years Old with a Double Health Problem: Undernutrition and Diarrhoea—A Cross-Sectional Study in Four Provinces of Mozambique. BMC Infect. Dis. 2021, 21, 18. [Google Scholar] [CrossRef]
- De Deus, N.; Chilaúle, J.J.; Cassocera, M.; Bambo, M.; Langa, J.S.; Sitoe, E.; Chissaque, A.; Anapakala, E.; Sambo, J.; Guimarães, E.L.; et al. Early Impact of Rotavirus Vaccination in Children Less than Five Years of Age in Mozambique. Vaccine 2018, 36, 7205–7209. [Google Scholar] [CrossRef]
- WHO. WHO Child Growth Standards: Training Course on Child Growth Assessment Modules; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Woolley, C.S.C.; Handel, I.G.; Bronsvoort, B.M.; Schoenebeck, J.J.; Clements, D.N. Is It Time to Stop Sweeping Data Cleaning under the Carpet? A Novel Algorithm for Outlier Management in Growth Data. PLoS ONE 2020, 15, e0228154. [Google Scholar] [CrossRef]
- WHO. World Health Organization Manual of Basic Techniques for a Health Laboratory; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- WHO. WHO Anthro for Personal Computers Manual; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Sergeant, E. Epitools Epidemiological Calculators; Ausvet. 2018. Available online: https://epitools.ausvet.com.au) (accessed on 28 January 2021).
- MISAU; INE; ICFI. Moçambique Inquérito Demográfico e de Saúde 2011; MISUA: Calverton, MD, USA; INE: Mexico City, Mexico; ICFI: Fairfax, VI, USA, 2013. [Google Scholar]
- Mozambique: FY 2011–2015 Multi-Year Strategy; Feed the Future: Washington, DC, USA, 2011; p. 52. Available online: https://pdf.usaid.gov/pdf_docs/pdacu531.pdf (accessed on 28 January 2021).
- INE. Relatório Final Do Inquérito Ao Orçamento Familiar—IOF-2014/15; 2015. Available online: http://www.ine.gov.mz/operacoes-estatisticas/inqueritos/inquerito-sobre-orcamento-familiar/relatorio-final-do-inquerito-ao-orcamento-familiar-iof-2014-15 (accessed on 28 January 2021).
- Abuya, B.A.; Ciera, J.; Kimani-Murage, E. Effect of Mother’s Education on Child’s Nutritional Status in the Slums of Nairobi. BMC Pediatr. 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Nagahori, C.; Tchuani, J.P.; Yamauchi, T. Factors Associated with Nutritional Status in Children Aged 5–24 Months in the Republic of Cameroon. Nurs. Health Sci. 2015, 17, 229–235. [Google Scholar] [CrossRef]
- Siddiqi, N.A.; Haque, N.; Goni, A. Malnutrition of Under-Five Children: Evidence from Bangladesh. Asian J. Med. Sci. 2011, 2, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Abubakar, A.; Uriyo, J.; Msuya, S.E.; Swai, M.; Stray-Pedersen, B. Prevalence and Risk Factors for Poor Nutritional Status among Children in the Kilimanjaro Region of Tanzania. Int. J. Environ. Res. Public. Health 2012, 9, 3506–3518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alemayehu, M.; Tinsae, F.; Haileslassie, K.; Seid, O.; Gebregziabher, G.; Yebyo, H. Undernutrition Status and Associated Factors in Under-5 Children, in Tigray, Northern Ethiopia. Nutrition 2015, 31, 964–970. [Google Scholar] [CrossRef] [PubMed]
- Muche, A. Predictors of Stunting among Children Age 6–59 Months in Ethiopia Using Bayesian Multi-Level Analysis. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, E.C.B.; Castro, d.T.G.; Sartorelli, D.S. Associated Factors of Malnutrition among African Children under Five Years Old, Bom Jesus, Angola. Rev. Nutr. 2017, 30, 33–44. [Google Scholar] [CrossRef]
- Amadu, I.; Seidu, A.-A.; Duku, E.; Okyere, J.; Hagan, J.E.; Hormenu, T.; Ahinkorah, B.O. The Joint Effect of Maternal Marital Status and Type of Household Cooking Fuel on Child Nutritional Status in Sub-Saharan Africa: Analysis of Cross-Sectional Surveys on Children from 31 Countries. Nutrients 2021, 13, 1541. [Google Scholar] [CrossRef]
- Otsuka, Y.; Agestika, L.; Widyarani; Sintawardani, N.; Yamauchi, T. Risk Factors for Undernutrition and Diarrhea Prevalence in an Urban Slum in Indonesia: Focus on Water, Sanitation, and Hygiene. Am. J. Trop. Med. Hyg. 2019, 100, 727–732. [Google Scholar] [CrossRef] [Green Version]
- Goldhar, C.; Bell, T.; Wolf, J. Rethinking Existing Approaches to Water Security in Remote Communities: An Analysis of Two Drinking Water Systems in Nunatsiavut, Labrador, Canada. Water-Altern. 2013, 6, 25. [Google Scholar]
- Boah, M.; Azupogo, F.; Amporfro, D.A.; Abada, L.A. The Epidemiology of Undernutrition and Its Determinants in Children under Five Years in Ghana. PLoS ONE 2019, 14, e0219665. [Google Scholar] [CrossRef] [Green Version]
- Mukalay, A.W.M.; Kalenga, p.M.K.; Dramaix, M.; Hennart, P.; Schirvel, C.; Kabamba, L.M.; Kabyla, B.I.; Donnen, P. Factors Associated with Malnutrition in Children under Five in Lubumbashi (DRC). Sante Publique (Bucur.) 2010, 22, 541–550. [Google Scholar] [CrossRef]
- Cumming, O.; Cairncross, S. Can Water, Sanitation and Hygiene Help Eliminate Stunting? Current Evidence and Policy Implications. Matern. Child. Nutr. 2016, 12, 91–105. [Google Scholar] [CrossRef] [Green Version]
- Ali, D.; Saha, K.K.; Nguyen, p.H.; Diressie, M.T.; Ruel, M.T.; Menon, P.; Rawat, R. Household Food Insecurity Is Associated with Higher Child Undernutrition in Bangladesh, Ethiopia, and Vietnam, but the Effect Is Not Mediated by Child Dietary Diversity. J. Nutr. 2013, 143, 2015–2021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fikadu, T.; Assegid, S.; Dube, L. Factors Associated with Stunting among Children of Age 24 to 59 Months in Meskan District, Gurage Zone, South Ethiopia: A Case-Control Study. BMC Public Health 2014, 14, 800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gari, T.; Loha, E.; Deressa, W.; Solomon, T.; Lindtjørn, B. Malaria Increased the Risk of Stunting and Wasting among Young Children in Ethiopia: Results of a Cohort Study. PLoS ONE 2018, 13, e0190983. [Google Scholar] [CrossRef]
- Ntenda, P.A.M. Association of Low Birth Weight with Undernutrition in Preschool-Aged Children in Malawi. Nutr. J. 2019, 18, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alebel, A.; Wagnew, F.; Tesema, C.; Kibret, G.D.; Petrucka, P.; Eshite, S. Effects of Undernutrition on Survival of Human Immunodeficiency Virus Positive Children on Antiretroviral Therapy. Ital. J. Pediatr. 2018, 44, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melku, M.; Enawgaw, B.; Ayana, S.; Anlay, D.Z.; Kebede, A.; Haile, A.; Muchie, K.F.; Damtie, D.; Lemma, M.; Getawa, S. Magnitude of Anemia and Undernutrition among HIV-Infected Children Who Took HAART: A Retrospective Follow-up Study. Am. J. Blood Res. 2020, 10, 198–209. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total | Underweight | p-Value | Wasting | p-Value | Stunting | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | n | (%) | ||||
| Total | 963 | 100 | 238 | 24.7 | 256 | 26.6 | 313 | 32.5 | |||
| Sex | 0.350 a | 0.813 a | 0.733 a | ||||||||
| Male | 574 | 59.6 | 148 | 25.8 | 151 | 26.3 | 189 | 32.9 | |||
| Female | 389 | 40.4 | 90 | 23.1 | 105 | 27.0 | 124 | 31.9 | |||
| Child age group (in months) | 0.398 a | 0.866 a | 0.080 a | ||||||||
| 0–5 | 65 | 6.7 | 13 | 20.0 | 20 | 30.8 | 12 | 18.5 | |||
| 6–11 | 365 | 37.9 | 84 | 23.0 | 94 | 25.8 | 120 | 32.9 | |||
| 12–23 | 374 | 38.8 | 95 | 25.4 | 99 | 26.5 | 124 | 33.2 | |||
| 24–59 | 159 | 16.5 | 46 | 28.9 | 43 | 27.0 | 57 | 35.8 | |||
| Caregiver Education Level | <0.001 a | 0.019 a | 0.002 a | ||||||||
| No education | 91 | 9.4 | 44 | 48.4 | 35 | 38.5 | 44 | 48.4 | |||
| Primary | 369 | 38.3 | 95 | 25.7 | 99 | 26.8 | 122 | 33.1 | |||
| Secondary/higher | 495 | 51.4 | 98 | 19.8 | 120 | 24.2 | 146 | 29.5 | |||
| Missing | 8 | 0.8 | - | - | - | - | - | - | |||
| Mother’s marital status | 0.544 b | 0.788 b | 0.005 b | ||||||||
| Single | 287 | 29.8 | 65 | 22.6 | 80 | 27.9 | 72 | 25.1 | |||
| Married/co-habitation | 637 | 66.1 | 163 | 25.6 | 167 | 26.2 | 227 | 35.6 | |||
| Divorced/widower | 13 | 1.3 | 4 | 30.8 | 4 | 30.8 | 4 | 30.8 | |||
| Missing | 26 | 2.7 | - | - | - | - | - | - | |||
| Child’s caregiver | 0.333 a | 0.567 a | 0.213 a | ||||||||
| Mother | 870 | 90.3 | 220 | 25.3 | 235 | 27.0 | 289 | 33.2 | |||
| Others | 83 | 8.6 | 17 | 20.5 | 20 | 24.1 | 22 | 26.5 | |||
| Missing | 10 | 1.0 | - | - | - | - | - | - | |||
| Caregiver age (in years) | 0.319 a | 0.129 a | 0.253 a | ||||||||
| <21 | 162 | 16.8 | 43 | 26.5 | 43 | 26.5 | 61 | 37.7 | |||
| 21–30 | 537 | 55.8 | 121 | 22.5 | 130 | 24.2 | 166 | 30.9 | |||
| >30 | 241 | 25.0 | 65 | 27.0 | 75 | 31.1 | 75 | 31.1 | |||
| Missing | 23 | 2.4 | - | - | - | - | - | - | |||
| Type of house | <0.001 b | 0.045 b | <0.001 b | ||||||||
| Reed | 45 | 4.7 | 20 | 44.4 | 16 | 35.6 | 16 | 35.6 | |||
| Mud | 219 | 22.7 | 77 | 35.2 | 65 | 29.7 | 114 | 52.1 | |||
| Brick | 674 | 70.0 | 132 | 19.6 | 167 | 24.8 | 175 | 26.0 | |||
| Others | 9 | 0.9 | 6 | 66.7 | 5 | 55.6 | 3 | 33.3 | |||
| Missing | 16 | 1.7 | - | - | - | - | - | - | |||
| Piped water | <0.001 a | 0.101 a | <0.001 a | ||||||||
| Yes | 540 | 56.1 | 106 | 19.6 | 131 | 24.3 | 141 | 26.2 | |||
| No | 407 | 42.3 | 125 | 30.7 | 119 | 29.1 | 167 | 40.8 | |||
| Missing | 16 | 1.7 | - | - | - | - | - | - | |||
| Treated water | 0.452 a | 0.094 a | 0.145 a | ||||||||
| Yes | 349 | 36.2 | 89 | 25.5 | 80 | 22.9 | 122 | 35.0 | |||
| No | 503 | 52.5 | 117 | 23.3 | 141 | 28.0 | 152 | 30.2 | |||
| Missing | 111 | 11.5 | - | - | - | - | - | - | |||
| Season | 0.066 a | 0.003 a | 0.911 a | ||||||||
| Wet | 424 | 44.0 | 117 | 27.6 | 133 | 31.4 | 137 | 32.3 | |||
| Dry | 539 | 56.0 | 121 | 22.4 | 123 | 22.8 | 176 | 32.7 | |||
| Family members in household | 0.794 a | 0.563 a | 0.047 a | ||||||||
| <5 | 435 | 45.2 | 110 | 25.3 | 115 | 26.4 | 127 | 29.2 | |||
| ≥5 | 422 | 43.8 | 110 | 26.1 | 119 | 28.2 | 150 | 35.5 | |||
| Missing | 106 | 11.0 | - | - | - | - | - | - | |||
| Characteristic | Total | Underweight | p-Value | Wasting | p-Value | Stunting | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | N | (%) | ||||
| Total | 963 | 100 | 238 | 24.7 | 256 | 26.6 | 313 | 32.5 | |||
| Birthweight | <0.001 a | 0.001 a | 0.116 a | ||||||||
| <2500 g | 112 | 11.6 | 43 | 38.4 | 44 | 39.3 | 43 | 38.4 | |||
| ≥2500 g | 749 | 77.8 | 165 | 22.0 | 179 | 23.9 | 232 | 31.0 | |||
| Missing | 102 | 10.6 | - | - | - | - | - | - | |||
| Someone with diarrhoea at home (Last 7 days) | 0.255 a | 0.582 a | 0.603 a | ||||||||
| Yes | 113 | 11.7 | 33 | 29.2 | 33 | 29.2 | 38 | 33.6 | |||
| No | 763 | 79.2 | 185 | 24.2 | 204 | 26.7 | 238 | 31.2 | |||
| Missing | 87 | 9.0 | - | - | - | - | - | - | |||
| Malaria | 0.080 a | 0.159 a | 0.544 a | ||||||||
| Yes | 58 | 6.0 | 20 | 34.5 | 20 | 34.5 | 21 | 36.2 | |||
| No | 887 | 92.1 | 215 | 24.2 | 231 | 26.0 | 287 | 32.4 | |||
| Missing | 18 | 1.9 | - | - | - | - | - | - | |||
| Pneumonia | 0.784 b | 1.000 b | 0.343 a | ||||||||
| Yes | 18 | 1.9 | 5 | 27.8 | 5 | 27.8 | 4 | 22.2 | |||
| No | 930 | 96.6 | 230 | 24.7 | 247 | 26.6 | 305 | 32.8 | |||
| Missing | 15 | 1.6 | - | - | - | - | - | - | |||
| Parasitic Infection | 0.028 a | 0.254 a | 0.194 a | ||||||||
| Positive | 93 | 9.7 | 33 | 35.5 | 30 | 32.3 | 37 | 39.8 | |||
| Negative | 661 | 68.6 | 164 | 24.8 | 176 | 26.6 | 218 | 33.0 | |||
| Missing * | 209 | 21.7 | - | - | - | - | - | - | |||
| Immunization | 0.226 a | 0.548 a | 0.615 a | ||||||||
| Yes | 801 | 83.2 | 193 | 24.1 | 211 | 26.3 | 259 | 32.3 | |||
| No | 157 | 16.3 | 45 | 28.7 | 45 | 28.7 | 54 | 34.4 | |||
| Missing | 5 | 0.5 | - | - | - | - | - | - | |||
| Child HIV status | <0.001 a | <0.001 a | <0.001 a | ||||||||
| Positive | 67 | 7.0 | 35 | 52.2 | 32 | 47.8 | 37 | 55.2 | |||
| Negative | 630 | 65.4 | 127 | 20.2 | 148 | 23.5 | 166 | 26.3 | |||
| Missing | 266 | 27.6 | - | - | - | - | - | - | |||
| Characteristic | Underweight | Wasting | Stunting | |||
|---|---|---|---|---|---|---|
| OR (95% IC) | p-Value | OR (95% IC) | p-Value | OR (95% IC) | p-Value | |
| Year | 0.100 | 0.223 | 0.126 | |||
| 2015 | 4.71 (1.40–15.83) | 0.012 | 3.30 (0.97–11.22) | 0.560 | 4.76 (1.11–20.42) | 0.036 |
| 2016 | 1.32 (0.63–2.79) | 0.466 | 1.55 (0.75–3.22) | 0.238 | 0.68 (0.28–1.61) | 0.380 |
| 2017 | 0.95 (0.50–1.80) | 0.882 | 1.08 (0.59–1.99) | 0.802 | 1.40 (0.71–2.79) | 0.332 |
| 2018 | 0.96 (0.49–1.87) | 0.906 | 1.49 (0.80–2.78) | 0.205 | 1.40 (0.56–3.48) | 0.457 |
| 2019 | Ref. | Ref. | Ref. | |||
| Province | 0.127 | 0.919 | 0.016 | |||
| Maputo | Ref. | Ref. | Ref. | |||
| Zambézia | 2.65 (0.99–7.10) | 0.052 | 1.21 (0.45–3.23) | 0.704 | 2.99 (0.82–10.87) | 0.097 |
| Nampula | 2.00 (0.82–4.88) | 0.128 | 1.03 (0.43–2.45) | 0.954 | 4.68 (1.63–13.41) | 0.004 |
| Sex | 0.749 | 0.424 | 0.437 | |||
| Male | 1.08 (0.68–1.70) | 1.19 (0.78–1.81) | 0.82 (0.49–1.36) | |||
| Female | Ref. | Ref. | Ref. | |||
| Child age group (in months) | 0.052 | 0.882 | 0.253 | |||
| 0–5 | Ref. | Ref. | Ref. | |||
| 6–11 | 2.19 (0.69–6.94) | 0.184 | 0.81 (0.35–1.90) | 0.630 | 3.22 (0.95–10.98) | 0.061 |
| 12–23 | 2.64 (0.84–8.23) | 0.095 | 0.92 (0.40–2.10) | 0.835 | 3.54 (1.03–12.15) | 0.044 |
| 24–59 | 4.36 (1.31–14.47) | 0.016 | 1.08 (0.43–2.67) | 0.874 | 3.04 (0.81–11.39) | 0.099 |
| Caregiver Education Level | <0.001 | 0.079 | 0.141 | |||
| No education | 5.16 (2.39–11.13) | <0.001 | 2.06 (0.97–4.36) | 0.060 | 1.41 (0.56–3.57) | 0.467 |
| Primary | 1.39 (0.85–2.28) | 0.195 | 0.88 (0.56–1.39) | 0.585 | 1.73 (1.00–2.97) | 0.049 |
| Secondary/above | Ref. | Ref. | Ref. | |||
| Mother’s marital status | 0.792 | |||||
| Single | Ref. | |||||
| Married/co-habitation | 0.84 (0.14–5.01) | 0.846 | ||||
| Divorced/widower | 0.69 (0.12–3.99) | 0.680 | ||||
| Care giver age (in years) | 0.327 | 0.044 | ||||
| <21 | 0.89 (0.44–1.82) | 0.757 | 0.45 (0.22–0.91) | 0.026 | ||
| 21–30 | 0.68 (0.26–1.72) | 0.150 | 0.62 (0.39–0.99) | 0.046 | ||
| >30 | Ref. | Ref. | ||||
| Type of house | 0.685 | 0.888 | 0.611 | |||
| Reed | Ref. | Ref. | Ref. | |||
| Mud | 0.50 (0.16–1.53) | 0.224 | 1.08 (0.34–3.42) | 0.900 | 1.30 (0.35–4.85) | 0.697 |
| Brick | 0.67 (0.26–1.72) | 0.406 | 1.34 (0.50–3.60) | 0.561 | 0.70 (0.22–2.29) | 0.559 |
| Others | - | - | 2.19 (0.10–46.32) | 0.614 | 0.55 (0.03–9.35) | 0.682 |
| Piped water | 0.931 | 0.054 | ||||
| Yes | Ref. | Ref. | Ref. | 0.526 | ||
| No | 1.03 (0.58–1.82) | 1.66 (0.99–2.79) | 0.81 (0.41–1.57) | |||
| Treated water | 1.000 | 0.125 | 0.774 | |||
| Yes | 1.00 (0.62–1.62) | 0.70 (0.45–1.10) | 1.08 (0.63–1.85) | |||
| No | Ref. | Ref. | Ref. | |||
| Season | 0.269 | 0.012 | ||||
| Wet | 1.29 (0.82–2.02) | 1.70 (1.12–2.56) | ||||
| Dry | Ref. | Ref. | ||||
| Family members in household | 0.178 | |||||
| <5 | Ref. | |||||
| ≥5 | 0.675 (0.38–1.20) | |||||
| Birthweight | <0.001 | <0.001 | 0.010 | |||
| <2500 g | 2.75 (1.53–4.95) | 2.73 (1.57–4.77) | 2.64 (1.26–5.50) | |||
| ≥2500 g | Ref. | Ref. | Ref. | |||
| Malaria | 0.415 | 0.415 | ||||
| Yes | 0.61 (0.18–2.10) | 1.55 (0.54–4.46) | ||||
| No | Ref. | Ref. | ||||
| Parasitic Infection | 0.882 | |||||
| Positive | 1.06 (0.49–2.32) | |||||
| Negative | Ref. | |||||
| Child HIV status | 0.006 | 0.061 | 0.004 | |||
| Positive | 2.64 (1.33–5.26) | 1.88 (0.97–3.63) | 3.37 (1.46–7.80) | |||
| Negative | Ref. | Ref. | Ref. | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sambo, J.; Cassocera, M.; Chissaque, A.; Bauhofer, A.F.L.; Roucher, C.; Chilaúle, J.; Cossa-Moiane, I.; Guimarães, E.L.; Manhique-Coutinho, L.; Anapakala, E.; et al. Characterizing Undernourished Children Under-Five Years Old with Diarrhoea in Mozambique: A Hospital Based Cross-Sectional Study, 2015–2019. Nutrients 2022, 14, 1164. https://doi.org/10.3390/nu14061164
Sambo J, Cassocera M, Chissaque A, Bauhofer AFL, Roucher C, Chilaúle J, Cossa-Moiane I, Guimarães EL, Manhique-Coutinho L, Anapakala E, et al. Characterizing Undernourished Children Under-Five Years Old with Diarrhoea in Mozambique: A Hospital Based Cross-Sectional Study, 2015–2019. Nutrients. 2022; 14(6):1164. https://doi.org/10.3390/nu14061164
Chicago/Turabian StyleSambo, Júlia, Marta Cassocera, Assucênio Chissaque, Adilson Fernando Loforte Bauhofer, Clémentine Roucher, Jorfélia Chilaúle, Idalécia Cossa-Moiane, Esperança L. Guimarães, Lena Manhique-Coutinho, Elda Anapakala, and et al. 2022. "Characterizing Undernourished Children Under-Five Years Old with Diarrhoea in Mozambique: A Hospital Based Cross-Sectional Study, 2015–2019" Nutrients 14, no. 6: 1164. https://doi.org/10.3390/nu14061164