
The Association between Postpartum Practice and Chinese Postpartum Depression: Identification of a Postpartum Depression-Related Dietary Pattern

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistics
3. Results
3.1. Prevalence of PPD
3.2. Association between PPD and Postpartum Practices
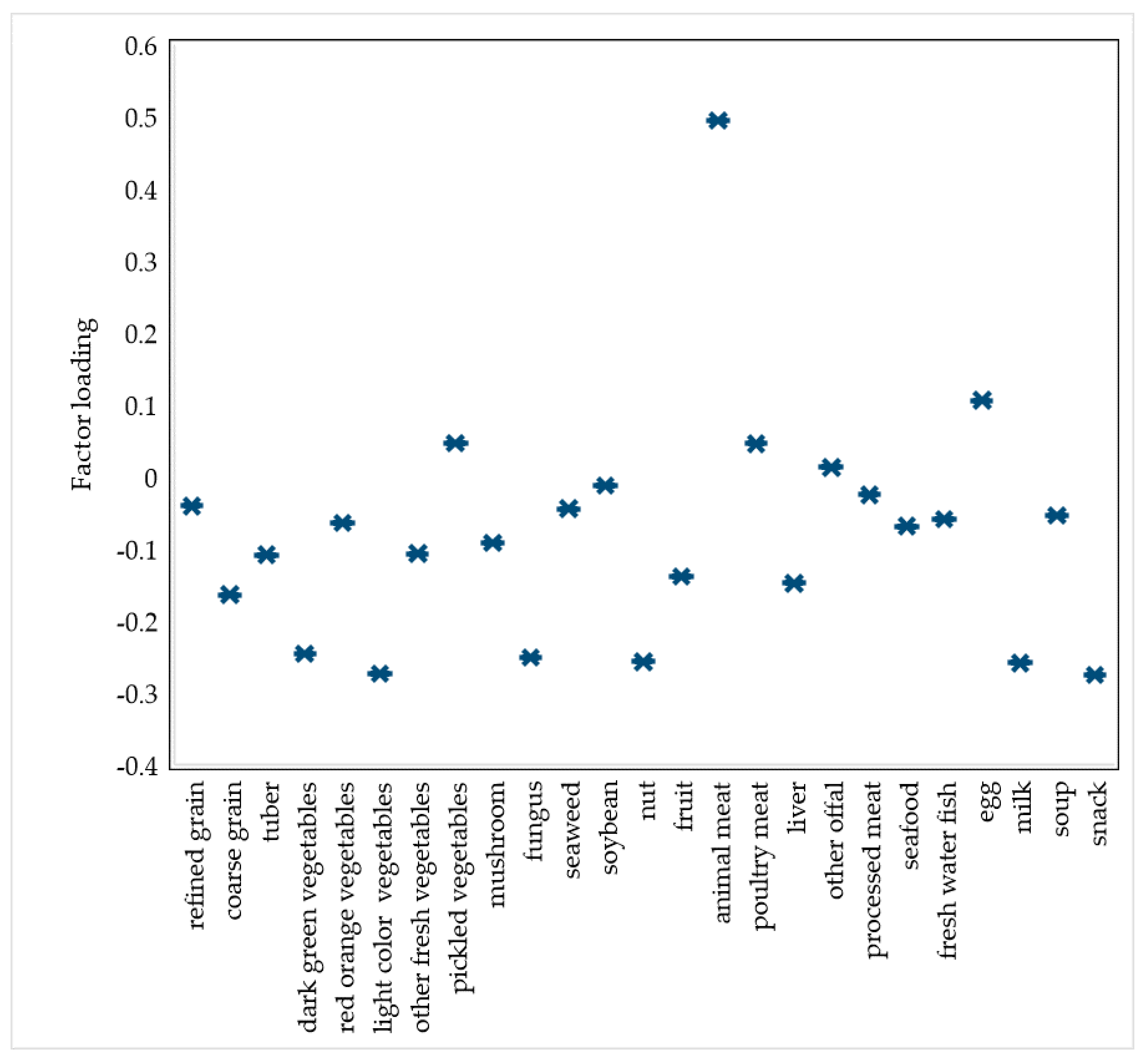
3.3. PPD-Related Dietary Pattern
3.4. Pathway Analysis
4. Discussion
4.1. Association of Postpartum Practices with PPD
4.2. PPD-Related Dietary Pattern
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bao, W.; Ma, A.; Mao, L.; Lai, J.; Xiao, M.; Sun, G.; Ouyang, Y.; Wu, S.; Yang, W.; Wang, N.; et al. Diet and lifestyle interventions in postpartum women in China: Study design and rationale of a multicenter randomized controlled trial. BMC Public Health 2010, 10, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raven, J.H.; Lin, X.; Li, F.; Hu, M.L.; Ren, J.C.; Wang, Z.X. The transition of dietary practices in postpartum Chinese women: Studies in parts of China. Matern. Child Health Care China 2018, 33, 5552–5556. [Google Scholar]
- Chan, S.M.; Nelson, E.; Leung, S.; Cheung, P.; Li, C.Y. Special postpartum dietary practices of Hong Kong Chinese women. Eur. J. Clin. Nutr. 2000, 54, 797–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, N.; Mao, L.; Sun, X.; Liu, L.; Chen, B.; Ding, Q. Postpartum practices of puerperal women and their influencing factors in three regions of Hubei, China. BMC Public Health 2006, 6, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.Q.; Petrini, M.; Maloni, J.A. Doing the month: Postpartum practices in Chinese women. Nurs. Health Sci. 2015, 17, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Ma, L.; Liu, N.; Chen, B.; Lu, Q.; Ying, C.; Sun, X. Self-reported health problems related to traditional dietary practices in postpartum women from urban, suburban and rural areas of Hubei province, China: The zuo yuezi. Asia Pac. J. Clin. Nutr. 2016, 25, 158–164. [Google Scholar]
- Zhao, A.; Xue, Y.; Zhang, Y.; Li, W.; Yu, K.; Wang, P. Nutrition Concerns of Insufficient and Excessive Intake of Dietary Minerals in Lactating Women: A Cross-Sectional Survey in Three Cities of China. PLoS ONE 2016, 11, e0146483. [Google Scholar] [CrossRef]
- Ding, G.; Yu, J.; Vinturache, A.; Gu, H.; Lu, M. Therapeutic Effects of the Traditional “Doing the Month” Practices on Postpartum Depression in China. Am. J. Psychiatry 2018, 175, 1071–1072. [Google Scholar] [CrossRef]
- Guo, P.; Xu, D.; Liew, Z.; He, H.; Brocklehurst, P.; Taylor, B.; Zhang, C.; Jin, X.; Gong, W. Adherence to Traditional Chinese Postpartum Practices and Postpartum Depression: A Cross-Sectional Study in Hunan, China. Front. Psychiatry 2021, 12, 649972. [Google Scholar] [CrossRef]
- Ding, G.; Niu, L.; Vinturache, A.; Zhang, J.; Lu, M.; Gao, Y.; Pan, S.; Tian, Y. “Doing the month” and postpartum depression among Chinese women: A Shanghai prospective cohort study. Women Birth 2020, 33, e151–e158. [Google Scholar] [CrossRef]
- Ho, M.; Li, T.-C.; Liao, C.-H.; Su, S.-Y.; Su, S.-Y. The Association between Behavior Restrictions in Doing-the-Month Practice and Mental Health Status among Postpartum Women. J. Altern. Complement. Med. 2015, 21, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Rose, N.; Koperski, S.; Golomb, B.A. Mood Food: Chocolate and Depressive Symptoms in a Cross-sectional Analysis. Arch. Intern. Med. 2010, 170, 699–703. [Google Scholar] [CrossRef] [PubMed]
- Suradom, C.; Suttajit, S.; Oon-Arom, A.; Maneeton, B.; Srisurapanont, M. Omega-3 polyunsaturated fatty acid (n-3 PUFA) supplementation for prevention and treatment of perinatal depression: A systematic review and meta-analysis of randomized-controlled trials. Nord. J. Psychiatry 2021, 75, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, L.; Ma, S.; Ye, J.; Zhang, H.; Li, Y.; Sair, A.T.; Pan, J.; Liu, X.; Li, X.; et al. High-Dietary Fiber Intake Alleviates Antenatal Obesity-Induced Postpartum Depression: Roles of Gut Microbiota and Microbial Metabolite Short-chain Fatty Acid Involved. J. Agric. Food Chem. 2020, 68, 13697–13710. [Google Scholar] [CrossRef] [PubMed]
- Gila-Díaz, A.; Carrillo, G.H.; Arribas, S.M.; Ramiro-Cortijo, D. Healthy Habits and Emotional Balance in Women during the Postpartum Period: Differences between Term and Preterm Delivery. Children 2021, 8, 937. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.W.; McCabe, J.E. Postpartum Depression: Current Status and Future Directions. Annu. Rev. Clin. Psychol. 2013, 9, 379–407. [Google Scholar] [CrossRef] [PubMed]
- Nisar, A.; Yin, J.; Waqas, A.; Bai, X.; Wang, D.; Rahman, A.; Li, X. Prevalence of perinatal depression and its determinants in Mainland China: A systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 1022–1037. [Google Scholar] [CrossRef]
- Lee, D.T.; Yip, S.K.; Chiu, H.F.; Leung, T.Y.; Chan, K.P.; Chau, I.O.; Leung, H.C.; Chung, T.K. Chung, Detecting postnatal depression in Chinese women. Validation of the Chinese version of the Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1998, 172, 433–437. [Google Scholar] [CrossRef]
- Huang, R.; Lei, B.; Fu, B.; Zhang, L.; Chen, Z.; Xiao, M.; Yang, D.; Yan, C.; Lei, J. Research progress in Perinatal Depression assessment. Chin. Nurs. Manag. 2019, 19, 1105–1109. [Google Scholar]
- Chinese Nutrition Society. The Chinese Nutrition Guidelines (2016); People’s Medical Publishing House: Beijing, China, 2016. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Fan, M.; Lyu, J.; He, P. Chinese guidelines for data processing and analysis concerning the International Physical Activity Questionnaire. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 961–964. [Google Scholar] [PubMed]
- Holroyd, E.; Katie, F.K.L.; Chun, L.S.; Ha, S.W. “Doing the month”: An exploration of postpartum practices in Chinese women. Health Care Women Int. 1997, 18, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Fisher, J. The role of traditional confinement practices in determining postpartum depression in women in Chinese cultures: A systematic review of the English language evidence. J. Affect. Disord. 2009, 116, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.H.; Zhang, Z.H. Risk factors for postpartum depression: An evidence-based systematic review of systematic reviews and meta-analyses. Asian J. Psychiatry 2020, 53, 102353. [Google Scholar] [CrossRef]
- Wan, E.Y.; Moyer, C.A.; Harlow, S.D.; Fan, Z.; Jie, Y.; Yang, H. Postpartum depression and traditional postpartum care in China: Role of Zuoyuezi. Int. J. Gynecol. Obstet. 2009, 104, 209–213. [Google Scholar] [CrossRef]
- Hung, C.H. Women’s postpartum stress, social support, and health status. West. J. Nurs. Res. 2005, 27, 148–159. [Google Scholar] [CrossRef]
- Demirel, G.; Egri, G.; Yesildag, B.; Doganer, A. Effects of traditional practices in the postpartum period on postpartum depression. Health Care Women Int. 2018, 39, 65–78. [Google Scholar] [CrossRef]
- Tang, L.; Zhu, R.; Zhang, X. Postpartum Depression and Social Support in China: A Cultural Perspective. J. Health Commun. 2016, 21, 1055–1061. [Google Scholar] [CrossRef]
- Okun, M.L. Sleep and postpartum depression. Curr. Opin. Psychiatry 2015, 28, 490–496. [Google Scholar] [CrossRef]
- Liu, Y.Q.; Maloni, J.A.; Petrini, M.A. Effect of postpartum practices of doing the month on Chinese women’s physical and psychological health. Biol. Res. Nurs. 2014, 16, 55–63. [Google Scholar] [CrossRef]
- Daher-Abdi, A.; Hernández, S.O.; Castro, L.A.R.; Mezo-González, C.E.; Croyal, M.; García-Santillán, J.A.; Ouguerram, K.; Zambrano, E.; Bolaños-Jiménez, F. Maternal DHA Supplementation during Pregnancy and Lactation in the Rat Protects the Offspring against High-Calorie Diet-Induced Hepatic Steatosis. Nutrients 2021, 13, 3075. [Google Scholar] [CrossRef] [PubMed]
- Hameed, S.; Naser, I.A.; Al Ghussein, M.A.; Ellulu, M.S. Is Iron Deficiency a Risk Factor for Postpartum Depression? A Case-Control Study in the Gaza Strip, Palestine. Public Health Nutr. 2021, 31, 1–8. [Google Scholar] [CrossRef]
- Dobersek, U.; Teel, K.; Altmeyer, S.; Adkins, J.; Wy, G.; Peak, J. Meat and mental health: A meta-analysis of meat consumption, depression, and anxiety. Crit. Rev. Food Sci. Nutr. 2021, 6, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Oliván-Blázquez, B.; Aguilar-Latorre, A.; Motrico, E.; Gómez-Gómez, I.; Zabaleta-Del-Olmo, E.; Couso-Viana, S.; Clavería, A.; Maderuelo-Fernandez, J.; Recio-Rodríguez, J.; Moreno-Peral, P.; et al. The Relationship between Adherence to the Mediterranean Diet, Intake of Specific Foods and Depression in an Adult Population (45–75 Years) in Primary Health Care. A Cross-Sectional Descriptive Study. Nutrients 2021, 13, 2724. [Google Scholar] [CrossRef] [PubMed]
- Doglikuu, B.D.; Djazayery, A.; Mirzababaei, A.; Sajjadi, S.F.; Badruj, N.; Mirzaei, K. Does Interaction between Sleep Quality and Major Dietary Patterns Predicts Depression among Overweight and Obese Women in Iran? Iran. J. Public Health 2021, 50, 1445–1453. [Google Scholar] [CrossRef]
- Patan, M.J.; Kennedy, D.O.; Husberg, C.; Hustvedt, S.O.; Calder, P.C.; Middleton, B.; Khan, J.; Forster, J.; Jackson, P.A. Differential Effects of DHA- and EPA-Rich Oils on Sleep in Healthy Young Adults: A Randomized Controlled Trial. Nutrients 2021, 13, 248. [Google Scholar] [CrossRef]
- Kumar, R.R.; Singh, L.; Thakur, A.; Singh, S.; Kumar, B. Role of Vitamins in Neurodegenerative Diseases: A Review. CNS Neurol. Disord. Drug Targets 2021, in press. [Google Scholar] [CrossRef]
- Singh, J.; Bhardwaj, B. To Study the Effect of Calorie Deficit Diet and Strength Training in Patients with Mild to Moderate Obstructive Sleep Apnoea. Indian J. Otolaryngol. Head Neck Surg. 2020, 72, 284–291. [Google Scholar] [CrossRef]
- He, F.; Dong, H.; Fernandez-Mendoza, J.; Bixler, E.O.; Liao, J.; Liao, D. Racial/ethnic disparity in habitual sleep is modified by caloric intake in adolescents. Sleep Med. 2020, 76, 65–71. [Google Scholar] [CrossRef]
- Avalos, L.A.; Caan, B.; Nance, N.; Zhu, Y.; Li, D.-K.; Quesenberry, C.; Hyde, R.J.; Hedderson, M.M. Prenatal Depression and Diet Quality During Pregnancy. J. Acad. Nutr. Diet. 2020, 120, 972–984. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Postpartum Depression | p | ||
|---|---|---|---|
| Yes | No | ||
| Lactation stages | 0.126 | ||
| 15–42 days postpartum | 161 (77.0) | 42 (23.0) | |
| >42 days postpartum | 535 (71.7) | 211 (28.3) | |
| Age (years) | 0.045 | ||
| <30 | 601 (71.8) | 236 (28.2) | |
| ≥30 | 92 (80.7) | 221 (19.3) | |
| Education experience | 0.276 | ||
| Senior school or below | 168 (70.0) | 72 (30.0) | |
| College and above | 525 (73.7) | 187 (26.3) | |
| Family average monthly income (Chinese yuan (CNY)) | 0.032 | ||
| <5000 | 303 (70.8) | 125 (29.2) | |
| 5000–10,000 | 272 (77.7) | 78 (22.3) | |
| >10,000 | 114 (68.3) | 53 (31.7) | |
| Number of family members | 0.052 | ||
| 3 | 233 (68.9) | 105 (31.1) | |
| 3–5 | 374 (73.9) | 132 (26.1) | |
| >5 | 89 (80.2) | 22 (19.8) | |
| Parity | 0.613 | ||
| 1 | 458 (72.4) | 175 (27.6) | |
| >2 | 235 (73.9) | 83 (26.1) | |
| Delivery mode | 0.479 | ||
| Vaginal delivery | 278 (71.6) | 110 (28.4) | |
| Cesarean delivery | 418 (73.7) | 129 (26.3) | |
| Parity | |||
| 1 | 449(64.5) | 247(35.5) | 0.074 |
| ≥2 | 183(70.7) | 76(29.3) | |
| Physical activities (MET hours/week) | 0.515 | ||
| <20 | 402 (73.5) | 145 (26.5) | |
| ≥20 | 282 (71.6) | 112 (28.4) | |
| Self-reported sleep quality | <0.001 | ||
| Good | 210 (79.5) | 54 (20.5) | |
| Fair | 333 (78.0) | 94 (22.0) | |
| Poor | 135 (61.4) | 85 (38.6) | |
| Very poor | 18 (40.9) | 26 (59.1) | |
| BMI | 0.841 | ||
| <18.9 | 38 (73.1) | 14 (26.9) | |
| 18.9–23.9 | 395 (72.2) | 152 (27.8) | |
| ≥24 | 259 (74.0) | 91 (26.0) | |
| Postpartum Depression | ||||||
|---|---|---|---|---|---|---|
| Yes | No | p | OR (95% CI) | AOR a (95% CI) | AOR b (95% CI) | |
| Overall postpartum practices | ||||||
| No | 359 (76.5) | 110 (23.5) | 0.012 | Ref. | Ref. | Ref. |
| Yes | 337 (69.3) | 149 (30.7) | 1.44 (1.08, 1.92) | 1.44 (1.08, 1.93) | 1.41 (1.04, 1.90) | |
| Non-dietary practices | ||||||
| No | 508 (74.4) | 175 (25.6) | 0.099 | Ref. | Ref. | Ref. |
| Yes | 188 (69.1) | 84 (30.9) | 1.30 (0.95, 1.77) | 1.35 (0.98, 1.84) | 1.26 (0.92, 1.75) | |
| Dietary practices | ||||||
| No | 459 (75.5) | 149 (24.5) | 0.016 | Ref. | Ref. | Ref. |
| Yes | 237 (68.3) | 110 (31.7) | 1.43 (1.07, 1.92) | 1.41 (1.05, 1.90) | 1.37 (1.01, 1.85) | |
| Postpartum Depression-Related Dietary Pattern | ||||
|---|---|---|---|---|
| Dietary Customs | Mean ± SD | p | OR (95% CI) | AOR a (95% CI) |
| No | 0.08 ± 0.99 | 0.001 | Ref. | Ref. |
| Yes | 0.14 ± 1.01 | 1.25 (1.10, 1.43) | 1.25 (1.10, 1.43) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, A.; Huo, S.; Tan, Y.; Yang, Y.; Szeto, I.M.-Y.; Zhang, Y.; Lan, H. The Association between Postpartum Practice and Chinese Postpartum Depression: Identification of a Postpartum Depression-Related Dietary Pattern. Nutrients 2022, 14, 903. https://doi.org/10.3390/nu14040903
Zhao A, Huo S, Tan Y, Yang Y, Szeto IM-Y, Zhang Y, Lan H. The Association between Postpartum Practice and Chinese Postpartum Depression: Identification of a Postpartum Depression-Related Dietary Pattern. Nutrients. 2022; 14(4):903. https://doi.org/10.3390/nu14040903
Chicago/Turabian StyleZhao, Ai, Shanshan Huo, Yuefeng Tan, Yucheng Yang, Ignatius Man-Yau Szeto, Yumei Zhang, and Hanglian Lan. 2022. "The Association between Postpartum Practice and Chinese Postpartum Depression: Identification of a Postpartum Depression-Related Dietary Pattern" Nutrients 14, no. 4: 903. https://doi.org/10.3390/nu14040903