
A Systematic Review of Psychobiotic Interventions in Children and Adolescents to Enhance Cognitive Functioning and Emotional Behavior

 , ,
, ,
Abstract
:1. Introduction
Targeting the Microbiota Gut–Brain Axis to Improve Developmental Outcomes
2. Objectives
3. Methods
3.1. Protocol
3.2. Eligibility Criteria
3.3. Search Strategy, Study Selection, and Data Extraction
3.4. Risk of Bias Assessment
4. Results
4.1. Stress/Anxiety
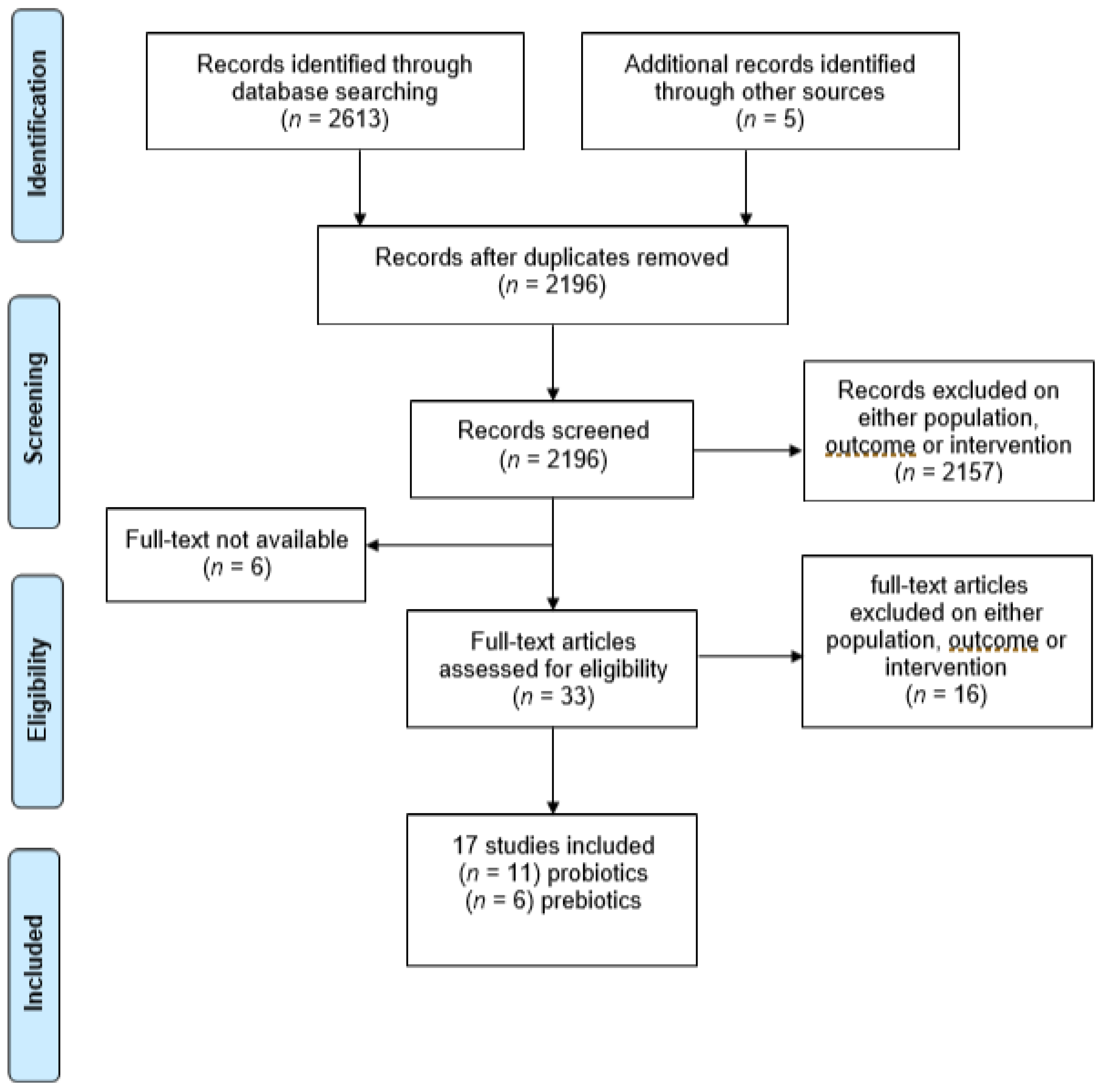
4.1.1. Study Records
4.1.2. Included Studies Characteristics
4.1.3. Quality of the Included Studies
4.1.4. Intervention Effects
4.2. Cognition
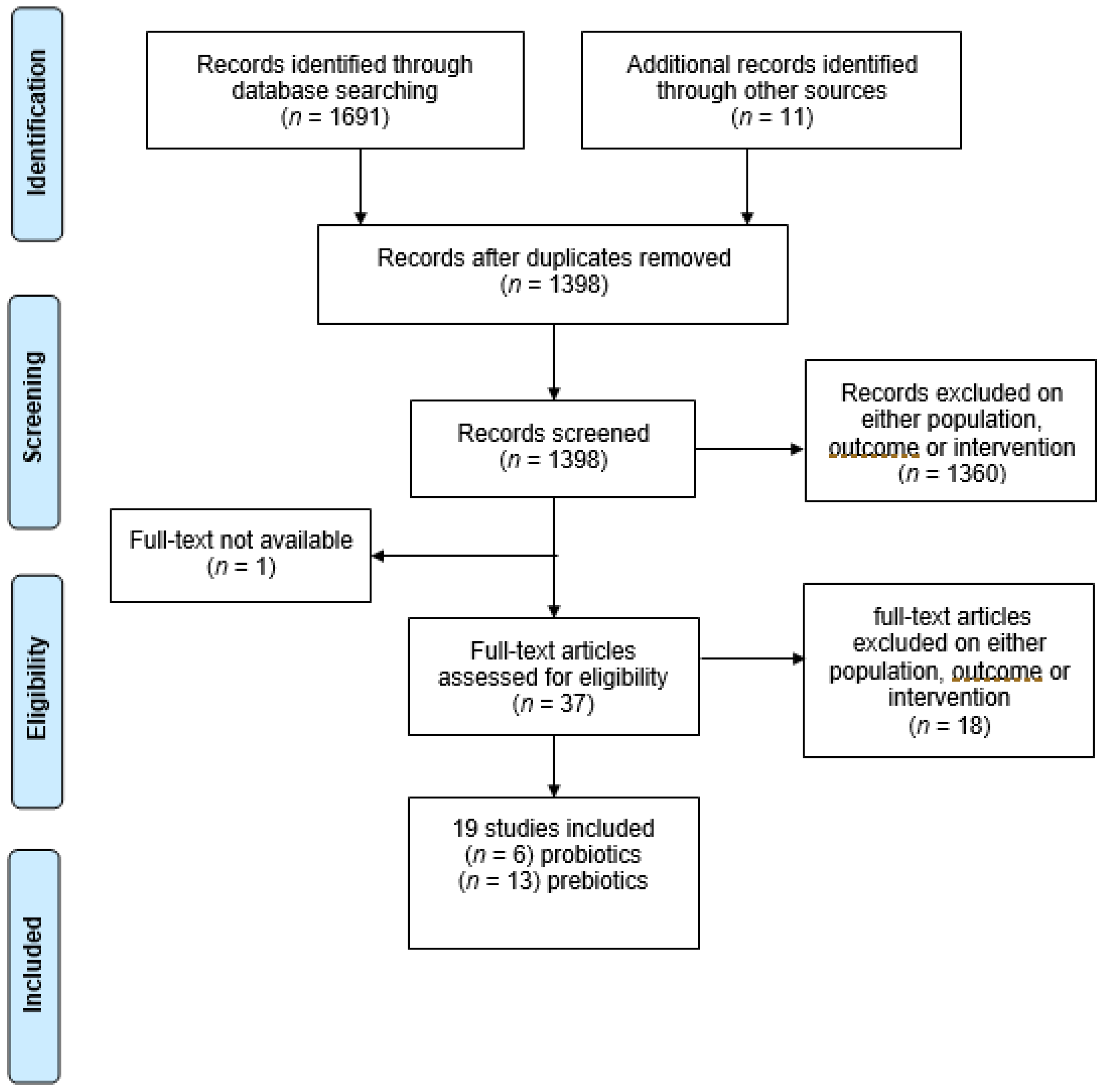
4.2.1. Study Records
4.2.2. Included Studies’ Characteristics
4.2.3. Quality of the Included Studies
4.2.4. Intervention Effects
4.3. Overall Results
5. Discussion
5.1. Anxiety and Stress Findings
5.2. Cognitive Findings
5.3. Towards a More Standardized Research Approach in the Field of Psychobiotic Interventions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADHD | Attention-deficit hyperactivity disorder |
| ASD | Autism spectrum disorder |
| BAI | Beck Anxiety Inventory |
| CFU | Colony-forming unit |
| CIs | Confidence intervals |
| DASS-42 | Depression Anxiety Stress Scale 42 |
| DHA | Docosahexaenoic acid |
| EPA | Eicosapentaenoic acid |
| FOS | Fructooligosaccharides |
| GABA | Gamma-aminobutyric acid |
| GBA | Gut–brain axis |
| GOS | Galactooligosaccharides |
| miRNA | Micro-RNA |
| mRNA | Messenger RNA |
| PGN | Peptidoglycan |
| PSWQ | Penn State Worry Questionnaire |
| PUFAs | Omega-3-polyunsaturated fatty acids |
| RoB-2 | Risk of bias tool for randomization trials |
| SCFAs | Short-chain fatty acids |
| STAI | State-Trait Anxiety Inventory |
| VAS | Visual Analogue Scale |
References
- Cryan, J.F.; Dinan, T.G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Luna, R.A.; Foster, J. Gut brain axis: Diet microbiota interactions and implications for modulation of anxiety and depression. Curr. Opin. Biotechnol. 2015, 32, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.A. Gut feelings: The emerging biology of gut–brain communication. Nat. Rev. Neurosci. 2011, 12, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Heijtz, R.D. Fetal, neonatal, and infant microbiome: Perturbations and subsequent effects on brain development and behavior. Semin. Fetal Neonatal Med. 2016, 21, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.C.; Olson, C.A.; Hsiao, E.Y. Interactions between the microbiota, immune and nervous systems in health and disease. Nat. Neurosci. 2017, 20, 145–155. [Google Scholar] [CrossRef]
- de Weerth, C. Do bacteria shape our development? Crosstalk between intestinal microbiota and HPA axis. Neurosci. Biobehav. Rev. 2017, 83, 458–471. [Google Scholar] [CrossRef]
- Methé, B.A.; Nelson, K.E.; Pop, M.; Creasy, H.H.; Giglio, M.G.; Huttenhower, C.; Gevers, D.; Petrosino, J.F.; Abubucker, S.; Mannon, P.J.; et al. A framework for human microbiome research. Nature 2012, 486, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Arevalo, P.; Van Insberghe, D.; Elsherbini, J.; Gore, J.; Polz, M.F. A Reverse Ecology Approach Based on a Biological Definition of Microbial Populations. Cell 2019, 178, 820–834.e14. [Google Scholar] [CrossRef]
- Berg, G.; Rybakova, D.; Fischer, D.; Cernava, T.; Vergès, M.-C.C.; Charles, T.; Chen, X.; Cocolin, L.; Eversole, K.; Corral, G.H.; et al. Microbiome definition re-visited: Old concepts and new challenges. Microbiome 2020, 8, 103. [Google Scholar] [CrossRef]
- Rosenberg, E.; Zilber-Rosenberg, I. The hologenome concept of evolution after 10 years. Microbiome 2018, 6, 78. [Google Scholar] [CrossRef]
- Zilber-Rosenberg, I.; Rosenberg, E. Role of microorganisms in the evolution of animals and plants: The hologenome theory of evolution. FEMS Microbiol. Rev. 2008, 32, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Margulis, L. Symbiosis as a Source of Evolutionary Innovation: Speciation and Morphogenesis. In Symbiogenesis and Symbionticism; Margulis, L., Fester, R., Eds.; MIT Press: Cambridge, MA, USA, 1991; pp. 1–14. [Google Scholar]
- Bravo, J.A.; Forsythe, P.; Chew, M.V.; Escaravage, E.; Savignac, H.M.; Dinan, T.G.; Bienenstock, J.; Cryan, J.F. Ingestion of Lactobacillus strain regulates emotional behavior and central GABA receptor expression in a mouse via the vagus nerve. Proc. Natl. Acad. Sci. USA 2011, 108, 16050–16055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnusson, K.; Hauck, L.; Jeffrey, B.; Elias, V.; Humphrey, A.; Nath, R.; Perrone, A.; Bermudez, L. Relationships between diet-related changes in the gut microbiome and cognitive flexibility. Neuroscience 2015, 300, 128–140. [Google Scholar] [CrossRef] [PubMed]
- Gensollen, T.; Iyer, S.S.; Kasper, D.L.; Blumberg, R.S. How colonization by microbiota in early life shapes the immune system. Science 2016, 352, 539–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudo, N.; Chida, Y.; Aiba, Y.; Sonoda, J.; Oyama, N.; Yu, X.-N.; Kubo, C.; Koga, Y. Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. J. Physiol. 2004, 558, 263–275. [Google Scholar] [CrossRef]
- Egrenham, S.; Clarke, G.; Cryan, J.F.; Dinan, T.G. Brain-Gut-Microbe Communication in Health and Disease. Front. Physiol. 2011, 2, 94. [Google Scholar] [CrossRef] [Green Version]
- Grossman, M. Neural and Hormonal Regulation of Gastrointestinal Function: An Overview. Annu. Rev. Physiol. 1979, 41, 27. [Google Scholar] [CrossRef]
- Mayer, E.A.; Knight, R.; Mazmanian, S.K.; Cryan, J.F.; Tillisch, K. Gut Microbes and the Brain: Paradigm Shift in Neuroscience. J. Neurosci. 2014, 34, 15490–15496. [Google Scholar] [CrossRef] [Green Version]
- Oldham, M.C.; Konopka, G.; Iwamoto, K.; Langfelder, P.; Kato, T.; Horvath, S.; Geschwind, D.H. Functional organization of the transcriptome in human brain. Nat. Neurosci. 2008, 11, 1271–1282. [Google Scholar] [CrossRef] [Green Version]
- Desbonnet, L.; Garrett, L.; Clarke, G.; Bienenstock, J.; Dinan, T.G. The probiotic Bifidobacteria infantis: An assessment of potential antidepressant properties in the rat. J. Psychiatr. Res. 2008, 43, 164–174. [Google Scholar] [CrossRef]
- Caputo, V.; Sinibaldi, L.; Fiorentino, A.; Parisi, C.; Catalanotto, C.; Pasini, A.; Cogoni, C.; Pizzuti, A. Brain Derived Neurotrophic Factor (BDNF) Expression Is Regulated by Micro, RNAs mi, R-26a and mi, R-26b Allele-Specific Binding. PLoS ONE 2011, 6, e28656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, S.H.; Pothoulakis, C.; Mayer, E.A. Principles and clinical implications of the brain–gut–enteric microbiota axis. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 306–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, Y.P.; Bernardi, A.; Frozza, R.L. The Role of Short-Chain Fatty Acids from Gut Microbiota in Gut-Brain Communication. Front. Endocrinol. 2020, 11, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiljar, M.; Merkler, D.; Trajkovski, M. The Immune System Bridges the Gut Microbiota with Systemic Energy Homeostasis: Focus on TLRs, Mucosal Barrier, and SCFAs. Front. Immunol. 2017, 8, 1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luczynski, P.; McVey Neufeld, K.-A.; Oriach, C.S.; Clarke, G.; Dinan, T.G.; Cryan, J.F. Growing up in a Bubble: Using Germ-Free Animals to Assess the Influence of the Gut Microbiota on Brain and Behavior. Int. J. Neuropsychopharmacol. 2016, 19, pyw020. [Google Scholar] [CrossRef]
- de Weerth, C.; Fuentes, S.; Puylaert, P.; de Vos, W.M. Intestinal Microbiota of Infants with Colic: Development and Specific Signatures. Pediatrics 2013, 131, e550–e558. [Google Scholar] [CrossRef] [Green Version]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef] [Green Version]
- Hollister, E.B.; Riehle, K.; Luna, R.A.; Weidler, E.M.; Rubio-Gonzales, M.; Mistretta, T.-A.; Raza, S.; Doddapaneni, H.V.; Metcalf, G.A.; Muzny, D.; et al. Structure and function of the healthy pre-adolescent pediatric gut microbiome. Microbiome 2015, 3, 36. [Google Scholar] [CrossRef] [Green Version]
- Heijtz, R.D.; Wang, S.; Anuar, F.; Qian, Y.; Björkholm, B.; Samuelsson, A.; Hibberd, M.L.; Forssberg, H.; Pettersson, S. Normal gut microbiota modulates brain development and behavior. Proc. Natl. Acad. Sci. USA 2011, 108, 3047–3052. [Google Scholar] [CrossRef] [Green Version]
- Burnet, P.W.; Cowen, P. Psychobiotics Highlight the Pathways to Happiness. Biol. Psychiatry 2013, 74, 708–709. [Google Scholar] [CrossRef]
- Lloyd-Price, J.; Mahurkar, A.; Rahnavard, G.; Crabtree, J.; Orvis, J.; Hall, A.B.; Brady, A.; Creasy, H.H.; McCracken, C.; Giglio, M.G.; et al. Strains, functions and dynamics in the expanded Human Microbiome Project. Nature 2017, 550, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Neufeld, K.-A.M.; Luczynski, P.; Oriach, C.S.; Dinan, T.G.; Cryan, J.F. What’s bugging your teen?—The microbiota and adolescent mental health. Neurosci. Biobehav. Rev. 2016, 70, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.H.; Grossmann, T.; Kadosh, K.C. Mapping functional brain development: Building a social brain through interactive specialization. Dev. Psychol. 2009, 45, 151–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, M.H. Interactive Specialization: A domain-general framework for human functional brain development? Dev. Cogn. Neurosci. 2011, 1, 7–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett, S.; Sebastian, C.; Kadosh, K.C.; Blakemore, S.-J. The social brain in adolescence: Evidence from functional magnetic resonance imaging and behavioural studies. Neurosci. Biobehav. Rev. 2011, 35, 1654–1664. [Google Scholar] [CrossRef] [Green Version]
- Dinan, T.G.; Stanton, C.; Cryan, J.F. Psychobiotics: A Novel Class of Psychotropic. Biol. Psychiatry 2013, 74, 720–726. [Google Scholar] [CrossRef]
- Tang, F.; Reddy, B.L.; Saier, M.H.S., Jr. Psychobiotics and Their Involvement in Mental Health. J. Mol. Microbiol. Biotechnol. 2014, 24, 211–214. [Google Scholar] [CrossRef] [Green Version]
- Gareau, M. Cognitive Function and the Microbiome. Int. Rev. Neurobiol. 2016, 131, 227–246. [Google Scholar]
- Boehm, G.; Jelinek, J.; Stahl, B.; Van Laere, K.; Knol, J.; Fanaro, S.; Moro, G.; Vigi, V. Prebiotics in Infant Formulas. J. Clin. Gastroenterol. 2004, 38, S76–S79. [Google Scholar] [CrossRef]
- Gibson, G.R.; Scott, K.P.; Rastall, R.A.; Tuohy, K.M.; Hotchkiss, A.; Dubert-Ferrandon, A.; Gareau, M.; Murphy, E.F.; Saulnier, D.; Loh, G.; et al. Dietary prebiotics: Current status and new definition. Food Sci. Technol. Bull. Funct. Foods 2010, 7, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Barile, D.; Rastall, R. Human milk and related oligosaccharides as prebiotics. Curr. Opin. Biotechnol. 2013, 24, 214–219. [Google Scholar] [CrossRef] [PubMed]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnstone, N.; Milesi, C.; Burn, O.; Bogert, B.V.D.; Nauta, A.; Hart, K.; Sowden, P.; Burnet, P.W.J.; Kadosh, K.C. Anxiolytic effects of a galacto-oligosaccharides prebiotic in healthy females (18–25 years) with corresponding changes in gut bacterial composition. Sci. Rep. 2021, 11, 8302. [Google Scholar] [CrossRef] [PubMed]
- Tillisch, K.; Labus, J.; Kilpatrick, L.; Jiang, Z.; Stains, J.; Ebrat, B.; Guyonnet, D.; Legrain-Raspaud, S.; Trotin, B.; Naliboff, B.; et al. Consumption of Fermented Milk Product with Probiotic Modulates Brain Activity. Gastroenterology 2013, 144, 1394–1401.e4. [Google Scholar] [CrossRef] [Green Version]
- Kadosh, K.C.; Basso, M.; Knytl, P.; Johnstone, N.; Lau, J.Y.F.; Gibson, G.R. Psychobiotic interventions for anxiety in young people: A systematic review and meta-analysis, with youth consultation. Transl. Psychiatry 2021, 11, 352. [Google Scholar] [CrossRef]
- Liu, X.; Cao, S.; Zhang, X. Modulation of Gut Microbiota–Brain Axis by Probiotics, Prebiotics, and Diet. J. Agric. Food Chem. 2015, 63, 7885–7895. [Google Scholar] [CrossRef]
- Eastwood, J.; Walton, G.; Van Hemert, S.; Williams, C.; Lamport, D. The effect of probiotics on cognitive function across the human lifespan: A systematic review. Neurosci. Biobehav. Rev. 2021, 128, 311–327. [Google Scholar] [CrossRef]
- Johnstone, N.; Kadosh, K.C. Why a developmental cognitive neuroscience approach may be key for future-proofing microbiota-gut-brain research. Behav. Brain Sci. 2019, 42, 73. [Google Scholar] [CrossRef]
- Murray, E.; Sharma, R.; Smith, K.B.; Mar, K.D.; Barve, R.; Lukasik, M.; Pirwani, A.F.; Malette-Guyon, E.; Lamba, S.; Thomas, B.J.; et al. Probiotic consumption during puberty mitigates LPS-induced immune responses and protects against stress-induced depression- and anxiety-like behaviors in adulthood in a sex-specific manner. Brain Behav. Immun. 2019, 81, 198–212. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions. Available online: www.training.cochrane.org/handbook (accessed on 14 December 2021).
- Thomas, J.; Graziosi, S.; Brunton, J.; Ghouze, Z.; O’Driscoll, P.; Bond, M. EPPI-Reviewer: Advanced Software for Systematic Reviews, Maps and Evidence Synthesis; UCL Social Research Institute: London, UK, 2020. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. Ro, B 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adikari, A.; Appukutty, M.; Kuan, G. Effects of Daily Probiotics Supplementation on Anxiety Induced Physiological Parameters among Competitive Football Players. Nutrients 2020, 12, 1920. [Google Scholar] [CrossRef] [PubMed]
- Chong, H.; Yusoff, N.A.; Hor, Y.Y.; Lew, L.C.; Jaafar, M.; Choi, S.-B.; Yusoff, M.; Wahid, N.; Bin Abdullah, M.F.I.L.; Zakaria, N.; et al. Lactobacillus plantarum DR7 alleviates stress and anxiety in adults: A randomised, double-blind, placebo-controlled study. Benef. Microbes 2019, 10, 355–373. [Google Scholar] [CrossRef] [PubMed]
- Culpepper, T.; Christman, M.; Nieves, J.C.; Specht, G.; Rowe, C.; Spaiser, S.; Ford, A.; Dahl, W.; Girard, S.; Langkamp-Henken, B. Bifidobacterium bifidum R0071 decreases stress-associated diarrhoea-related symptoms and self-reported stress: A secondary analysis of a randomised trial. Benef. Microbes 2016, 7, 327–336. [Google Scholar] [CrossRef]
- Hughes, C.; Davoodi-Semiromi, Y.; Colee, J.C.; Culpepper, T.; Dahl, W.J.; Mai, V.; Christman, M.C.; Langkamp-Henken, B. Galactooligosaccharide supplementation reduces stress-induced gastrointestinal dysfunction and days of cold or flu: A randomized, double-blind, controlled trial in healthy university students. Am. J. Clin. Nutr. 2011, 93, 1305–1311. [Google Scholar] [CrossRef] [Green Version]
- Karbownik, M.S.; Kręczyńska, J.; Kwarta, P.; Cybula, M.; Wiktorowska-Owczarek, A.; Kowalczyk, E.; Pietras, T.; Szemraj, J. Effect of Supplementation with Saccharomyces Boulardii on Academic Examination Performance and Related Stress in Healthy Medical Students: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2020, 12, 1469. [Google Scholar] [CrossRef] [PubMed]
- Kato-Kataoka, A.; Nishida, K.; Takada, M.; Suda, K.; Kawai, M.; Shimizu, K.; Kushiro, A.; Hoshi, R.; Watanabe, O.; Igarashi, T. Fermented milk containing Lactobacillus casei strain Shirota prevents the onset of physical symptoms in medical students under academic examination stress. Benef. Microbes 2016, 7, 153–156. [Google Scholar] [CrossRef]
- Kato-Kataoka, A.; Nishida, K.; Takada, M.; Kawai, M.; Kikuchi-Hayakawa, H.; Suda, K.; Ishikawa, H.; Gondo, Y.; Shimizu, K.; Matsuki, T.; et al. Fermented Milk Containing Lactobacillus casei Strain Shirota Preserves the Diversity of the Gut Microbiota and Relieves Abdominal Dysfunction in Healthy Medical Students Exposed to Academic Stress. Appl. Environ. Microbiol. 2016, 82, 3649–3658. [Google Scholar] [CrossRef] [Green Version]
- Kitaoka, K.; Uchida, B.K.; Okamoto, B.N.; Chikahisa, S.; Miyazaki, M.T.; Takeda, E.; Séi, H. Fermented Ginseng Improves the First-Night Effect in Humans. Sleep 2009, 32, 413–421. [Google Scholar] [CrossRef] [Green Version]
- Kelly, J.; Allen, A.P.; Temko, A.; Hutch, W.; Kennedy, P.J.; Farid, N.; Murphy, E.; Boylan, G.; Bienenstock, J.; Cryan, J.F.; et al. Lost in translation? The potential psychobiotic Lactobacillus rhamnosus (JB-1) fails to modulate stress or cognitive performance in healthy male subjects. Brain Behav. Immun. 2017, 61, 50–59. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, J.K.; Belury, M.A.; Andridge, R.; Malarkey, W.B.; Glaser, R. Omega-3 supplementation lowers inflammation and anxiety in medical students: A randomized controlled trial. Brain Behav. Immun. 2011, 25, 1725–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.-W.; Liong, M.T.; Chung, Y.-C.E.; Huang, H.-Y.; Peng, W.-S.; Cheng, Y.-F.; Lin, Y.-S.; Wu, Y.-Y.; Tsai, Y.-C. Effects of Lactobacillus plantarum PS128 on Children with Autism Spectrum Disorder in Taiwan: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2019, 11, 820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ba, B.E.M.; Bravender, T.D.; Harrison, T.M.; Lange, H.L.H.L.; Cottrill, C.B.; Abdel-Rasoul, M.; Bonny, A.E. A pilot randomized controlled trial of omega-3 fatty acid supplementation for the treatment of anxiety in adolescents with anorexia nervosa. Int. J. Eat. Disord. 2018, 51, 1367–1372. [Google Scholar] [CrossRef]
- Papalini, S.; Michels, F.; Kohn, N.; Wegman, J.; van Hemert, S.; Roelofs, K.; Arias-Vasquez, A.; Aarts, E. Stress matters: Randomized controlled trial on the effect of probiotics on neurocognition. Neurobiol. Stress 2019, 10, 100141. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, K.; Cowen, P.; Harmer, C.; Tzortzis, G.; Errington, S.; Burnet, P.W.J. Prebiotic intake reduces the waking cortisol response and alters emotional bias in healthy volunteers. Psychopharmacology 2015, 232, 1793–1801. [Google Scholar] [CrossRef] [Green Version]
- Tran, N.; Zhebrak, M.; Yacoub, C.; Pelletier, J.; Hawley, D. The gut-brain relationship: Investigating the effect of multispecies probiotics on anxiety in a randomized placebo-controlled trial of healthy young adults. J. Affect. Disord. 2019, 252, 271–277. [Google Scholar] [CrossRef]
- Capitão, L.P.; Baião, R.; Baek, H.K.; Kappelmann, N.; Sharman, R.; Harvey, C.-J.; Montgomery, P.; Burnet, P.W. Prebiotic Supplementation Does Not Affect Reading and Cognitive Performance in Children: A Randomised Placebo-Controlled Study. J. Psychopharmacol. 2020, 34, 148–152. [Google Scholar] [CrossRef]
- Nova, E.; Alvarez, A.; Marcos, A.; Warnberg, J.; Gómez–Martínez, S.; Alvarez, R.; Mateos, J.A.; Cobo, J.M. The effect of milk fermented by yogurt cultures plus Lactobacillus casei DN-114001 on the immune response of subjects under academic examination stress. Eur. J. Nutr. 2004, 43, 381–389. [Google Scholar] [CrossRef]
- Vijay, A.; Astbury, S.; Le Roy, C.; Spector, T.D.; Valdes, A.M. The prebiotic effects of omega-3 fatty acid supplementation: A six-week randomised intervention trial. Gut Microbes 2021, 13, 1863133. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, P.; Shin, C.Y. A comprehensive review of the therapeutic and pharmacological effects of ginseng and ginsenosides in central nervous system. J. Ginseng Res. 2013, 37, 8–29. [Google Scholar] [CrossRef] [Green Version]
- Bos, D.J.; Oranje, B.; Veerhoek, E.S.; Van Diepen, R.M.; Weusten, J.M.; Demmelmair, H.; Koletzko, B.; van der Velden, M.G.D.S.; Eilander, A.; Hoeksma, M.; et al. Reduced Symptoms of Inattention after Dietary Omega-3 Fatty Acid Supplementation in Boys with and without Attention Deficit/Hyperactivity Disorder. Neuropsychopharmacology 2015, 40, 2298–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capitão, L.P.; Forsyth, J.; Thomaidou, M.; Condon, M.D.; Harmer, C.J.; Burnet, P.W. A single administration of ‘microbial’ D-alanine to healthy volunteers augments reaction to negative emotions: A comparison with D-serine. J. Psychopharmacol. 2020, 34, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Cornu, C.; Mercier, C.; Ginhoux, T.; Masson, S.; Mouchet, J.; Nony, P.; Kassai, B.; Laudy, V.; Berquin, P.; Franc, N.; et al. A double-blind placebo-controlled randomised trial of omega-3 supplementation in children with moderate ADHD symptoms. Eur. Child Adolesc. Psychiatry 2018, 27, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Karr, J.E.; Grindstaff, T.R.; Alexander, J.E. Omega-3 polyunsaturated fatty acids and cognition in a college-aged population. Exp. Clin. Psychopharmacol. 2012, 20, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.O.; Jackson, P.A.; Elliott, J.M.; Scholey, A.B.; Robertson, B.C.; Greer, J.; Tiplady, B.; Buchanan, T.; Haskell, C.F. Cognitive and mood effects of 8 weeks’ supplementation with 400 mg or 1000 mg of the omega-3 essential fatty acid docosahexaenoic acid (DHA) in healthy children aged 10–12 years. Nutr. Neurosci. 2009, 12, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Milte, C.M.; Parletta, N.; Buckley, J.D.; Coates, A.M.; Young, R.; Howe, P. Eicosapentaenoic and docosahexaenoic acids, cognition, and behavior in children with attention-deficit/hyperactivity disorder: A randomized controlled trial. Nutrients 2012, 28, 670–677. [Google Scholar] [CrossRef]
- Milte, C.M.; Parletta, N.; Buckley, J.D.; Coates, A.M.; Young, R.; Howe, P.R.C. Increased Erythrocyte Eicosapentaenoic Acid and Docosahexaenoic Acid Are Associated with Improved Attention and Behavior in Children with ADHD in a Randomized Controlled Three-Way Crossover Trial. J. Atten. Disord. 2013, 19, 954–964. [Google Scholar] [CrossRef]
- Widenhorn-Müller, K.; Schwanda, S.; Scholz, E.; Spitzer, M.; Bode, H. Effect of supplementation with long-chain ω-3 polyunsaturated fatty acids on behavior and cognition in children with attention deficit/hyperactivity disorder (ADHD): A randomized placebo-controlled intervention trial. Prostaglandins Leukot. Essent. Fat. Acids 2014, 91, 49–60. [Google Scholar] [CrossRef]
- Portillo-Reyes, V.; Pérez-García, M.; Loya-Méndez, Y.; Puente, A.E. Clinical significance of neuropsychological improvement after supplementation with omega-3 in 8–12 years old malnourished Mexican children: A randomized, double-blind, placebo and treatment clinical trial. Res. Dev. Disabil. 2014, 35, 861–870. [Google Scholar] [CrossRef]
- Richardson, A.J.; Burton, J.R.; Sewell, R.P.; Spreckelsen, T.F.; Montgomery, P. Docosahexaenoic Acid for Reading, Cognition and Behavior in Children Aged 7–9 Years: A Randomized, Controlled Trial (The DOLAB Study). PLoS ONE 2012, 7, e43909. [Google Scholar] [CrossRef]
- Steenbergen, L.; Sellaro, R.; Van Hemert, S.; Bosch, J.A.; Colzato, L.S. A randomized controlled trial to test the effect of multispecies probiotics on cognitive reactivity to sad mood. Brain Behav. Immun. 2015, 48, 258–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vesco, A.T.; Young, A.S.; Arnold, L.E.; Fristad, M.A. Omega-3 supplementation associated with improved parent-rated executive function in youth with mood disorders: Secondary analyses of the omega 3 and therapy (OATS) trials. J. Child Psychol. Psychiatry 2017, 59, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Voigt, R.G.; Llorente, A.M.; Jensen, C.L.; Fraley, J.; Berretta, M.C.; Heird, W.C. A randomized, double-blind, placebo-controlled trial of docosahexaenoic acid supplementation in children with attention-deficit/hyperactivity disorder. J. Pediatr. 2001, 139, 189–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marx, W.; Scholey, A.; Firth, J.; D’cunha, N.M.; Lane, M.; Hockey, M.; Ashton, M.M.; Cryan, J.F.; O’neil, A.; Naumovski, N.; et al. Prebiotics, probiotics, fermented foods and cognitive outcomes: A meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 2020, 118, 472–484. [Google Scholar] [CrossRef] [PubMed]
- Faber, G.; Wolpert, M.; Kemmer, D. Common Measures for Mental Health Science: Laying the Foundations; NIH: London, UK, 2020. [Google Scholar]
- Patalay, P.; Fried, E.I. Editorial Perspective: Prescribing measures: Unintended negative consequences of mandating standardized mental health measurement. J. Child Psychol. Psychiatry 2021, 62, 1032–1036. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Intervention Type | Delivery Method | Active Compound | Dose | Frequency (Dose/Day) | Duration (Days) | Active/ Control | Mean Age | Sex (M/F) | Anxiety Measure | Effect WITHIN-AG | Effect BETWEEN-G | Stress Measure | Effect WITHIN-AG | Effect BETWEEN-G | Participants | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adikari et al., (2020) [55] | probiotic | liquid | Lactobacillus Casei Shirota | 3 × 1010 CFU | 1 | 56 | 10/9 | 19 | 19/0 | - | - | - | EDR | - | ns | football players | |
| HR | - | ns | |||||||||||||||
| Capitao et al., (2020) [70] | prebiotic | sachet | B-GOS | - | 1 | 84 | 17/18 | 8.84 | 24/11 | STAIC | ns | ns | salivary cortisol | - | ns | children with below-average literacy skills | |
| Chong et al., (2019) [56] | probiotics | sachet | Lactobacillus Plantarum DR7 | 1 × 109 CFU | 1 | 84 | 27/32 | 24.8 | - | DASS-42 anxiety | < | ↓ | PSS-10 | < | ns | healthy young adults | |
| DASS-42 stress | < | ↓ | |||||||||||||||
| Culpepper et al. (2016) [57] | probiotic | capsule | Lactobacillus helveticus R0052 | 3 × 109 CFU | 1 | 42 | 145 | 19.9 | 209/372 | - | - | - | self-reported stress | - | ↓ for B. Bifidum only, only in sleep deprived students | students e.s. | |
| Bifidobacterium longum ssp. infantis R0033 | 147 | ||||||||||||||||
| Bifidobacterium bifidum R0071 | 142 | ||||||||||||||||
| placebo | 147 | ||||||||||||||||
| Hughes et al. (2011) [58] | prebiotic | sachet | GOS | 0, 2500, 5000 mg | 1 | 56 | 279/140 | 19.9 | 207/212 | - | - | - | self-reported stress | - | ns | students e.s. | |
| Karbownik et al. (2020) [59] | probiotic | capsule | Saccharomyces boulardii | 5 × 109 CFU | 1 | 30 | 31/29 | 22.6 | 37/55 | STAI state | < | ns | salivary cortisol | + | ns | students e.s. | |
| salivary metanephrine | ns | ns | |||||||||||||||
| pulse rate | + | ↑ | |||||||||||||||
| Kato-Kataoka et al. (2016) [60] | probiotic | liquid | Lactobacillus casei Shirota | 100 × 109 CFU | 1 | 56 | 23/24 | 22.8 | 25/22 | STAI state | - | ns | visual analogue stress scale | - | ↓ | students e.s. | |
| salivary cortisol | - | ↓ | |||||||||||||||
| salivary alpha-amylase | - | ns | |||||||||||||||
| Kato-Kataoka et al. (2016) [61] | probiotic | liquid | Lactobacillus casei Shirota | 100 × 109 CFU | 1 | 56 | 24/23 | 22.9 | 26/21 | STAI state | - | ns | salivary cortisol | - | ns | students e.s. | |
| salivary immunoglobulin A | - | ns | |||||||||||||||
| Kitaoka et al. (2009) [62] | prebiotic | capsule | Fermented Ginseng | 205 mg | 9 | 8 | 8/8 | 20.7 | 16/0 | STAI total | < | - | salivary cortisol | ns | - | healthy subjects | |
| POMS | ns | - | salivary immunoglobulin A | ns | - | ||||||||||||
| Kelly et al. (2017) [63] | probiotic | capsule | Lactobacillus rhamnosus | 1 × 109 CFU | 1 | 28 | 15/14 | 24.6 | 29/0 | BAI | ns | ns | PSS-10 | ns | ns | healthy subjects, SECPT | |
| STAI trait | ns | ns | cortisol SECPT | - | ns | ||||||||||||
| STAI state | < | ns | self-reported stress SECPT | ns | ns | ||||||||||||
| Kiecolt-Glaser et al. (2011) [64] | prebiotic | capsule | omega-3 PUFAs | 2500 g | 1 | 84 | 34/34 | 23.7 | 38/30 | BAI | - | ↓ | - | - | - | students e.s. | |
| Liu et al. (2019) [65] | probiotic | capsule | Lactobacillus plantarum PS128 | 30 × 109 CFU | ns | 30 | 36/35 | 10.0 | 71/0 | CBCL | - | ns | - | - | - | ASD children | |
| Manos et al. (2018) [66] | prebiotic | capsule | omega-3-PUFAs | 782 mg | 4 | 84 | 10/8 | 14.7 | 0/18 | BAIT | < | ↑ | - | - | - | anorexic girls | |
| Marcos et al. (2004) [70] | probiotic | liquid | Lactobacillus delbrueckii bulgaricus | 1 × 109 CFU | 2 | 21 | 73/63 | 18–23 | 40/96 | STAI state | + | ns | serum cortisol | - | ns | students e.s. | |
| Streptococcus salivarius thermophilus | 10 × 109 CFU | STAI trait | ns | ||||||||||||||
| Lactobacillus casei DN114001 | 10 × 109 CFU | ||||||||||||||||
| Papalini et al. (2019) [67] | probiotic | powder | Bifidobacterium bifidum W23, Bifidobacterium lactis W51, Bifidobacterium lactis W52, Lactobacillus acidophilus W37, Lactobacillus brevis W63, Lactobacillus casei W56, Lactobacillus salivarius W24, Lactococcus lactis W19, Lactococcus lactis W58 | 2.5 × 109 CFU | 2 | 28 | 29/29 | 21.5 | 0/58 | - | - | - | VAS | + | ns | healthy subjects, SECPT | |
| cortisol | + | ns | |||||||||||||||
| alpha-amylase | + | ns | |||||||||||||||
| HR | + | ns | |||||||||||||||
| BP | + | ns | |||||||||||||||
| Schmidt et al. (2015) [68] | prebiotic | powder | FOS | 5500 mg | 1 | 21 | 15 | 23.7 | 22/23 | STAI state | - | ns | PSS-10 | - | ns | healthy subjects | |
| B-GOS | 15 | salivary cortisol | - | ↓ GOS only | |||||||||||||
| placebo | 15 | ||||||||||||||||
| Tran et al. (2019) [69] | probiotic | - | 18 species | 50 × 109 CFU (condition A) | 1 | 28 | 14 | 20.6 | 20/66 | BAI | - | ns BAI total | - | - | - | healthy students | |
| 10 species | 50 × 109 CFU (condition B) | 13 | - | ||||||||||||||
| 18 species | 15 × 109 CFU (condition D) | 15 | PSWQ | ↓50 × 109 CFU only | |||||||||||||
| 10 species | 10 × 109 CFU (condition E) | 15 | |||||||||||||||
| placebo | 11 | ||||||||||||||||
 | |||||||||||||||||
| Study | Intervention Type | Delivery Method | Active Compound | Dose | Frequency (Dose/Day) | Duration (Days) | Active/ Control | Mean Age | Sex (M/F) | Cognitive Tool | Cognitive Function | Effect WITHIN-G | Effect BETWEEN-G | Participants | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adikari et al. (2020) [55] | probiotic | liquid (orange juice) | Lactobacillus Casei Shirota | 3 × 1010 CFU | 1 | 56 | 10/9 | 19 | 19/0 | DVT-RT | sustained attention/vigilance/visual-motor tracking | + | ↓ | right-handed football players | |
| Bos et al. (2015) [74] | prebiotic | fortified margarine | DHA & EPA | 650 mg each | 1 | 112 | 19 ADHD PRO | 10.6 | 76/0 | CBCL-AP | attention | + | ↓(ADHDvsRG) ↓(PROvsPBO) | ADHD children either medication naïve or using metylphenidate | |
| 19 ADHD PBO | GO/NO-GO TASK | inhibitory control | ns | ns | |||||||||||
| 20 RG PRO | |||||||||||||||
| 18 RG PBO | |||||||||||||||
| Capitao et al. (2020) [75] | prebiotic | sachet | B-GOS | - | 1 | 84 | 17/18 | 8.84 | 24/11 | BAS-III | literacy | + | ns | children with below-average literacy skills | |
| CogTrack | memory retrieval speed | + | ns | ||||||||||||
| Cornu et al. (2018) [76] | prebiotic | capsules | DHA & EPA | 6–8 yo: 84 mg & 336 mg | 1 | 91 | 71/77 | 9.9 | 127/35 | Aloulette test | lexical age | - | ns | ADHD children | |
| 9–11 yo: 126 mg & 504 mg | KiTAP (6–10 yo)/TAP (11–15 yo) | distractibility (6–11 yo only) | - | ns | |||||||||||
| 12–15 yo: 168 mg & 672 mg | flexibility | - | ns | ||||||||||||
| inhibitory control (go/no-go RTs) | - | ↓ RTs | |||||||||||||
| Chong et al. (2019) [56] | probiotic | sachet | Lactobacillus plantarum DR7 | 1 × 109 CFU | 1 | 84 | 27/32 | 24.8 | - | CBB | psychomotor control | - | ns | stressed healthy subjects | |
| basic attention | - | ns | |||||||||||||
| visual learning & memory | - | ns | |||||||||||||
| working memory | - | ns | |||||||||||||
| executive function | - | ns | |||||||||||||
| social emotional cognition | - | ns | |||||||||||||
| associate learning | - | ns | |||||||||||||
| verbal learning and memory | - | ns | |||||||||||||
| Karr et al. (2012) [77] | prebiotic | capsules | DHA & EPA | 240 mg & 360 mg | 2 | 28 | 20 /21 | 20.1 | 12/29 | RAVLT | verbal learning and memory | ns | ns | college students | |
| SCWT | inhibitory control | ns | ns | ||||||||||||
| TMT | executive control | ns | ↑ | ||||||||||||
| Kelly et al. (2017) [63] | probiotic | capsules | Lactobacillus rhamnosus | 1 × 109 CFU | 1 | 28 | 15/14 | 24.6 | 29/0 | CANTAB | associate learning | + | ns | healthy subjects | |
| attention | + | ns | |||||||||||||
| visual speed processing | + | ns | |||||||||||||
| emotional attentional bias | ns | ns | |||||||||||||
| Kennedy et al. (2009) [78] | prebiotic | capsules | DHA | 200 mg | 2 (400 mg) | 56 | 28 | 10.8 | 44/42 | CDR | general cognitive functions | + | ↓word recognition speed in 400 mg pre&post breakfast ↑ in 1000 mg pre-breakfast | healthy children | |
| DHA | 200 mg | 5 (1000 mg) | 30 | internet battery | - | - | |||||||||
| PBO | 30 | ||||||||||||||
| Liu et al. (2019) [65] | probiotic | capsules | Lactobacillus plantarum PS128 | 3 × 1010 CFU | - | 30 | 36/35 | 10.01 | 71/0 | CBCL-AP | attention | - | ns | ASD children | |
| Milte et al. (2012) [79] | prebiotic | capsules | DHA & EPA | 108 mg & 1109 mg | 1 | 121 | 24 | 8.9 | 70/17 * | WIAT-III/WSCI-III | literacy | - | ns | ADHD | |
| DHA & EPA | 1032 mg & 264 mg | 1 | 19 | TEAC | attention and inhibition | - | ns | ||||||||
| safflower oil (control) | 1467 mg | 1 | 24 | ||||||||||||
| Milte et al. (2015) [80] | prebiotic | capsules | DHA & EPA | 108 mg & 1109 mg | 1 | 121*3 | 56 | 8.9 | 67/20 * | WIAT-III/WSCI-III | literacy | +(spelling) | ns | ADHD | |
| DHA & EPA | 1032 mg & 264 mg | 1 | 54 | TEAC | attention and inhibition | +(attention) | ns | ||||||||
| safflower oil (control) | 1467 mg | 1 | 57 | ||||||||||||
| Widenhorn-Müller et al. (2014) [81] | prebiotic | capsules | DHA & EPA | 600 mg & 120 mg | 1 | 112 | 46/49 | 8.9 | 74/21 | HAWIK-IV | working memory | - | ↓ | ADHD | |
| speed of information processing | - | ns | |||||||||||||
| KITAP/TAP | attention | - | ns | ||||||||||||
| CBCL AP | attention | NA | ns | ||||||||||||
| Papalini et al. (2019) [67] | probiotic | powder | Bifidobacterium bifidum W23, Bifidobacterium lactis W51, Bifidobacterium lactis W52, Lactobacillus acidophilus W37, Lactobacillus brevis W63, Lactobacillus casei W56, Lactobacillus salivarius W24, Lactococcus lactis W19, Lactococcus lactis W58 | 2.5 × 109 | 2 | 28 | 29/29 | 21.5 | 0/58 | emotional face-matching | emotional reactivity | + | ns | healthy subjects | |
| emotional face-word stroop | resolution of emotional conflicts | + | ns | ||||||||||||
| color-word stroop | cognitive inhibition | + | ns | ||||||||||||
| digit span backward test | working memory | +after stress | ↓(after stress) | ||||||||||||
| Portillo-Reyes et al. (2014) [82] | prebiotic | capsules | DHA & EPA | 60 mg & 90 mg | 3 | 91 | 30/20 | 9.2 | 29/21 | symbolic search | processing speed | + | ↓ | healthy children | |
| embedded figures test/visual closure | visuoperceptive integration | + | ↓ | ||||||||||||
| semantic fluency/comprehension instruction | language | +semantic fluency (fruit) | ns | ||||||||||||
| block design/TMT A | visuomotor coordination | +block design | ↓block design | ||||||||||||
| matrix reasoning/stroop colour word/TMT B/letter-number sequencing | executive functions | +letter-number seq, matrix reasoning, stroop | ↓matrix reasoning, stroop | ||||||||||||
| letter cancellation | attention | + | ns | ||||||||||||
| rey complex figure/word list | visual & verbal memory | +verbal recall & recognition | ns | ||||||||||||
| Richardson et al. (2012) [83] | prebiotic | capsules | DHA | 200 mg | 3 | 112 | 179/180 | 8.6 | 192/170 | BAS-II | reading | +very poor readers only | ↓poor and very poor readers only | healthy children | |
| DS-FW/DS-BW | working memory | ns | ↓ forward recall | ||||||||||||
| Schmidt et al. (2015) [68] | prebiotic | powder | FOS | 5500 mg | 1 | 21 | 15 | 23.7 | 22/23 | Attentional dot-probe task | attention | - | ↓GOS only, unmasked condition | healthy subjects | |
| B-GOS | 15 | facial expression recognition/emotional word recognition and recall | emotional cognition | - | ns | ||||||||||
| PBO | 15 | ||||||||||||||
| Steenbergen et al. (2015) [84] | probiotic | powder | Bifidobacterium bifidum W23, Bifidobacterium lactis W51, Bifidobacterium lactis W52, Lactobacillus acidophilus W37, Lactobacillus brevis W63, Lactobacillus casei W56, Lactobacillus salivarius W24, Lactococcus lactis W19, Lactococcus lactis W58 | 2.5 × 109 CFU | 2 | 28 | 20/20 | 19.9 | 8/32 | LEIDS-r | cognitive reactivity to sad mood | + | ↓particularly aggressive and ruminative thoughts | healthy subjects | |
| Vesco et al. (2018) [85] | prebiotic | capsules | DHA & EPA and others | 50 mg & 350 mg & 67 mg | 2 | 84 | 23 | 11.2 | 54/41 | BRIEF | Executive functions | + | ↓ | children with depression/mood disorders | |
| PUFAs + PEP | 22 | ||||||||||||||
| PEP + PBO | 26 | ||||||||||||||
| PBO | 24 | ||||||||||||||
| Voigt et al. (2000) [86] | prebiotic | capsules | DHA | 345 mg | 3 | 121 | 25/24 | 9.3 | 42/12 * | TOVA | sustained attention | + | ns | ADHD | |
| CCT | visual attention, sequencing, psychomotor speed, cognitive flexibility | ns | ns | ||||||||||||
 | |||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basso, M.; Johnstone, N.; Knytl, P.; Nauta, A.; Groeneveld, A.; Cohen Kadosh, K. A Systematic Review of Psychobiotic Interventions in Children and Adolescents to Enhance Cognitive Functioning and Emotional Behavior. Nutrients 2022, 14, 614. https://doi.org/10.3390/nu14030614
Basso M, Johnstone N, Knytl P, Nauta A, Groeneveld A, Cohen Kadosh K. A Systematic Review of Psychobiotic Interventions in Children and Adolescents to Enhance Cognitive Functioning and Emotional Behavior. Nutrients. 2022; 14(3):614. https://doi.org/10.3390/nu14030614
Chicago/Turabian StyleBasso, Melissa, Nicola Johnstone, Paul Knytl, Arjen Nauta, Andre Groeneveld, and Kathrin Cohen Kadosh. 2022. "A Systematic Review of Psychobiotic Interventions in Children and Adolescents to Enhance Cognitive Functioning and Emotional Behavior" Nutrients 14, no. 3: 614. https://doi.org/10.3390/nu14030614