
The Impact of Job-Demand-Control-Support on Leptin and Ghrelin as Biomarkers of Stress in Emergency Healthcare Workers
 , , , , , , ,
, , , , , , ,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Outcomes
2.3. Statistics
3. Results
3.1. Characteristics of the Population
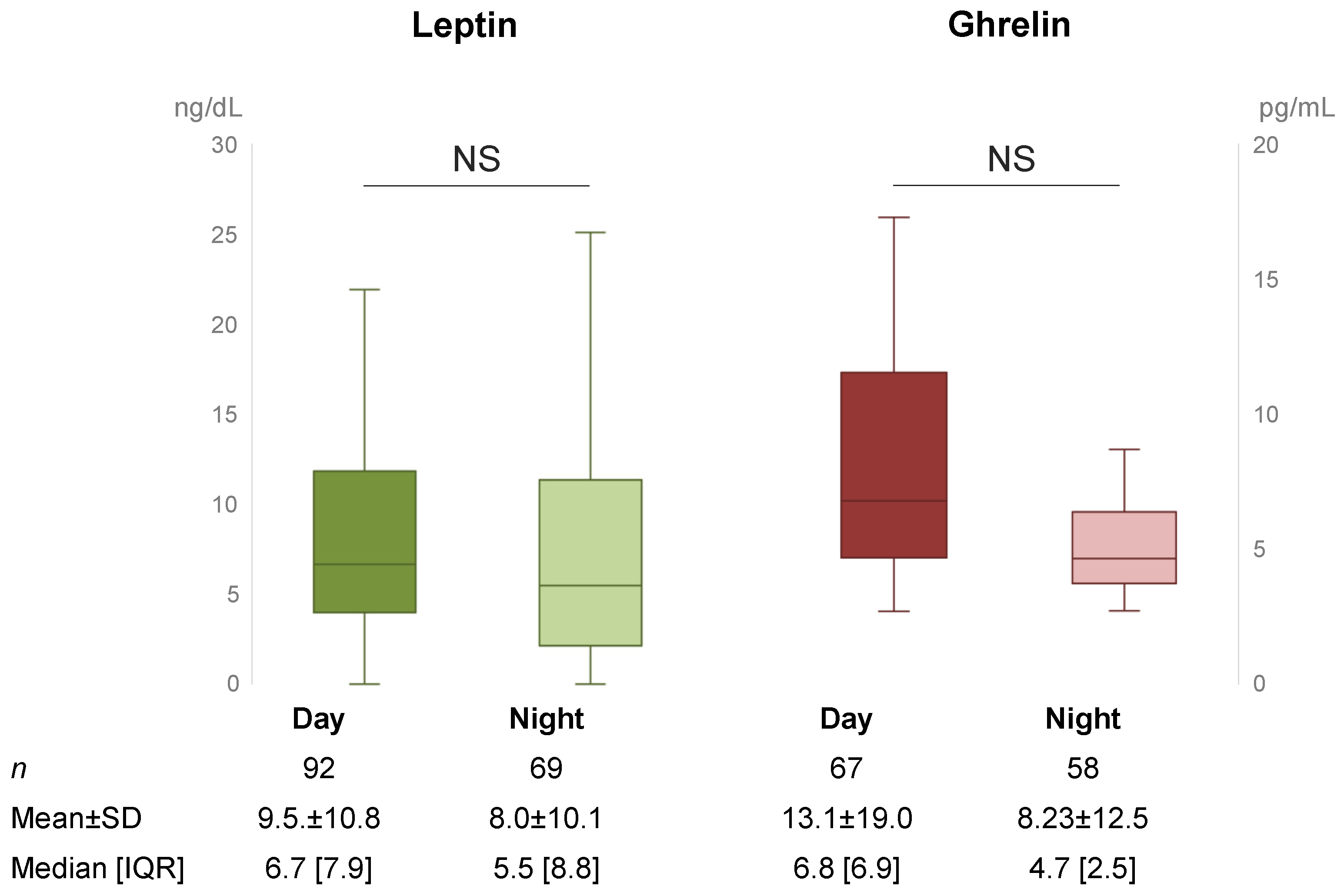
3.2. Assessment of Ghrelin and Leptin Levels
3.3. Impact of Stress, Night Shift, Sociodemographic, and Nutrition on Leptin and Ghrelin Levels
4. Discussion
4.1. The Impact of Night Shift and Stress
4.2. Impact of Food Intake and Sociodemographic Status
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dutheil, F.; Danini, B.; Bagheri, R.; Fantini, M.L.; Pereira, B.; Moustafa, F.; Trousselard, M.; Navel, V. Effects of a Short Daytime Nap on the Cognitive Performance: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10212. [Google Scholar] [CrossRef]
- Bouillon-Minois, J.-B.; Thivel, D.; Croizier, C.; Ajebo, É.; Cambier, S.; Boudet, G.; Adeyemi, O.J.; Ugbolue, U.C.; Bagheri, R.; Vallet, G.T.; et al. The Negative Impact of Night Shifts on Diet in Emergency Healthcare Workers. Nutrients 2022, 14, 829. [Google Scholar] [CrossRef] [PubMed]
- Bouillon-Minois, J.-B.; Raconnat, J.; Clinchamps, M.; Schmidt, J.; Dutheil, F. Emergency Department and Overcrowding During COVID-19 Outbreak; a Letter to Editor. Arch. Acad. Emerg. Med. 2021, 9, e28. [Google Scholar] [CrossRef] [PubMed]
- Bouillon-Minois, J.-B.; Schmidt, J.; Dutheil, F. SARS-CoV-2 Pandemic and Emergency Medicine: The Worst Is yet to Come. Am. J. Emerg. Med. 2020, 42, 246–247. [Google Scholar] [CrossRef]
- Karasek, R.A. Job Demands, Job Decision Latitude, and Mental Strain: Implications for Job Redesign. Adm. Sci. Q 1979, 24, 285–308. [Google Scholar] [CrossRef]
- Karasek, R.A. Job Decision Latitude, Job Design, and Coronary Heart Disease; Machine pacing and occupational stress; Taylor and Francis Ltd.: London, UK, 1981. [Google Scholar]
- Convention C171—Night Work Convention, 1990 (No. 171). Available online: https://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_INSTRUMENT_ID:312316 (accessed on 4 November 2021).
- Boivin, D.B.; Boudreau, P. Impacts of Shift Work on Sleep and Circadian Rhythms. Pathol. Biol. 2014, 62, 292–301. [Google Scholar] [CrossRef]
- Ganesan, S.; Magee, M.; Stone, J.E.; Mulhall, M.D.; Collins, A.; Howard, M.E.; Lockley, S.W.; Rajaratnam, S.M.W.; Sletten, T.L. The Impact of Shift Work on Sleep, Alertness and Performance in Healthcare Workers. Sci. Rep. 2019, 9, 4635. [Google Scholar] [CrossRef] [Green Version]
- Kosmadopoulos, A.; Kervezee, L.; Boudreau, P.; Gonzales-Aste, F.; Vujovic, N.; Scheer, F.A.J.L.; Boivin, D.B. Effects of Shift Work on the Eating Behavior of Police Officers on Patrol. Nutrients 2020, 12, 999. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.C.; Hoe, V.C.W.; Darus, A.; Bhoo-Pathy, N. Association between Night-Shift Work, Sleep Quality and Metabolic Syndrome. Occup. Environ. Med. 2018, 75, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Keski-Rahkonen, A.; Mustelin, L. Epidemiology of Eating Disorders in Europe: Prevalence, Incidence, Comorbidity, Course, Consequences, and Risk Factors. Curr. Opin. Psychiatry 2016, 29, 340–345. [Google Scholar] [CrossRef]
- Dutheil, F.; Chaplais, E.; Vilmant, A.; Courteix, D.; Duche, P.; Abergel, A.; Pfabigan, D.M.; Han, S.; Mobdillon, L.; Vallet, G.T.; et al. Stress Management in Obesity during a Thermal Spa Residential Programme (ObesiStress): Protocol for a Randomised Controlled Trial Study. BMJ Open 2019, 9, e027058. [Google Scholar] [CrossRef] [PubMed]
- Abdella, H.M.; El Farssi, H.O.; Broom, D.R.; Hadden, D.A.; Dalton, C.F. Eating Behaviours and Food Cravings; Influence of Age, Sex, BMI and FTO Genotype. Nutrients 2019, 11, E377. [Google Scholar] [CrossRef] [Green Version]
- Gifkins, J.; Johnston, A.; Loudoun, R. The Impact of Shift Work on Eating Patterns and Self-Care Strategies Utilised by Experienced and Inexperienced Nurses. Chronobiol. Int. 2018, 35, 811–820. [Google Scholar] [CrossRef] [Green Version]
- Padilla, H.M.; Wilson, M.; Vandenberg, R.J.; Davis, M.; Clark, M.A. Health Behavior among Working Adults: Workload and Exhaustion Are Associated with Nutrition and Physical Activity Behaviors That Lead to Weight Gain. J. Health Psychol. 2021, 26, 892–904. [Google Scholar] [CrossRef]
- Nishitani, N.; Sakakibara, H.; Akiyama, I. Eating Behavior Related to Obesity and Job Stress in Male Japanese Workers. Nutrition 2009, 25, 45–50. [Google Scholar] [CrossRef]
- Palla, L.; Almoosawi, S. Diurnal Patterns of Energy Intake Derived via Principal Component Analysis and Their Relationship with Adiposity Measures in Adolescents: Results from the National Diet and Nutrition Survey RP (2008–2012). Nutrients 2019, 11, 422. [Google Scholar] [CrossRef] [Green Version]
- Bonham, M.P.; Kaias, E.; Zimberg, I.; Leung, G.K.W.; Davis, R.; Sletten, T.L.; Windsor-Aubrey, H.; Huggins, C.E. Effect of Night Time Eating on Postprandial Triglyceride Metabolism in Healthy Adults: A Systematic Literature Review. J. Biol. Rhythms 2019, 34, 119–130. [Google Scholar] [CrossRef]
- Bali, A.; Jaggi, A.S. An Integrative Review on Role and Mechanisms of Ghrelin in Stress, Anxiety and Depression. Curr. Drug Targets 2016, 17, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Hansson, C.; Shirazi, R.H.; Näslund, J.; Vogel, H.; Neuber, C.; Holm, G.; Anckarsäter, H.; Dickson, S.L.; Eriksson, E.; Skibicka, K.P. Ghrelin Influences Novelty Seeking Behavior in Rodents and Men. PLoS ONE 2012, 7, e50409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummings, D.E. Ghrelin and the Short- and Long-Term Regulation of Appetite and Body Weight. Physiol. Behav. 2006, 89, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Nagaya, N.; Kojima, M.; Uematsu, M.; Yamagishi, M.; Hosoda, H.; Oya, H.; Hayashi, Y.; Kangawa, K. Hemodynamic and Hormonal Effects of Human Ghrelin in Healthy Volunteers. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2001, 280, R1483–R1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Münzberg, H.; Morrison, C.D. Structure, Production and Signaling of Leptin. Metabolism 2015, 64, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Gijón-Conde, T.; Graciani, A.; Guallar-Castillón, P.; Aguilera, M.T.; Rodríguez-Artalejo, F.; Banegas, J.R. Leptin Reference Values and Cutoffs for Identifying Cardiometabolic Abnormalities in the Spanish Population. Rev. Esp. Cardiol. 2015, 68, 672–679. [Google Scholar] [CrossRef] [Green Version]
- Bouillon-Minois, J.-B.; Trousselard, M.; Thivel, D.; Benson, A.C.; Schmidt, J.; Moustafa, F.; Bouvier, D.; Dutheil, F. Leptin as a Biomarker of Stress: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3350. [Google Scholar] [CrossRef] [PubMed]
- Bouillon-Minois, J.-B.; Trousselard, M.; Thivel, D.; Gordon, B.A.; Schmidt, J.; Moustafa, F.; Oris, C.; Dutheil, F. Ghrelin as a Biomarker of Stress: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 784. [Google Scholar] [CrossRef] [PubMed]
- Zefferino, R.; Di Gioia, S.; Conese, M. Molecular Links between Endocrine, Nervous and Immune System during Chronic Stress. Brain Behav. 2021, 11, e01960. [Google Scholar] [CrossRef]
- Pulopulos, M.M.; Baeken, C.; De Raedt, R. Cortisol Response to Stress: The Role of Expectancy and Anticipatory Stress Regulation. Horm. Behav. 2020, 117, 104587. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.L.; Tai, T.C.; Wong-Faull, D.C.; Claycomb, R.; Meloni, E.G.; Myers, K.M.; Carlezon, W.A.; Kvetnansky, R. Epinephrine: A Short- and Long-Term Regulator of Stress and Development of Illness: A Potential New Role for Epinephrine in Stress. Cell Mol. Neurobiol. 2012, 32, 737–748. [Google Scholar] [CrossRef]
- Dutheil, F.; Trousselard, M.; Perrier, C.; Lac, G.; Chamoux, A.; Duclos, M.; Naughton, G.; Mnatzaganian, G.; Schmidt, J. Urinary Interleukin-8 Is a Biomarker of Stress in Emergency Physicians, Especially with Advancing Age—The JOBSTRESS* Randomized Trial. PLoS ONE 2013, 8, e71658. [Google Scholar] [CrossRef] [PubMed]
- Bouillon-Minois, J.-B.; Trousselard, M.; Pereira, B.; Schmidt, J.; Clinchamps, M.; Thivel, D.; Ugbolue, U.C.; Moustafa, F.; Occelli, C.; Vallet, G.; et al. Protocol of the Study on Emergency Health Care Workers’ Responses Evaluated by Karasek Questionnaire: The SEEK-Study Protocol. Int. J. Environ. Res. Public Health 2021, 18, 4068. [Google Scholar] [CrossRef] [PubMed]
- Durand, A.-C.; Bompard, C.; Sportiello, J.; Michelet, P.; Gentile, S. Stress and Burnout among Professionals Working in the Emergency Department in a French University Hospital: Prevalence and Associated Factors. Work 2019, 63, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Bouillon-Minois, J.-B.; Roux, V.; Pereira, B.; Flannery, M.; Pelissier, C.; Occelli, C.; Schmidt, J.; Navel, V.; Dutheil, F. Stress among Emergency Health Care Workers on Nuclear or Radiation Disaster: A Preliminary State Survey. Int. J. Environ. Res. Public Health 2021, 18, 8384. [Google Scholar] [CrossRef]
- Dutheil, F.; Boudet, G.; Perrier, C.; Lac, G.; Ouchchane, L.; Chamoux, A.; Duclos, M.; Schmidt, J. JOBSTRESS Study: Comparison of Heart Rate Variability in Emergency Physicians Working a 24-Hour Shift or a 14-Hour Night Shift—A Randomized Trial. Int. J. Cardiol. 2012, 158, 322–325. [Google Scholar] [CrossRef]
- Aydin, S.; Halifeoglu, I.; Ozercan, I.H.; Erman, F.; Kilic, N.; Aydin, S.; Ilhan, N.; Ilhan, N.; Ozkan, Y.; Akpolat, N.; et al. A Comparison of Leptin and Ghrelin Levels in Plasma and Saliva of Young Healthy Subjects. Peptides 2005, 26, 647–652. [Google Scholar] [CrossRef] [PubMed]
- McHill, A.W.; Melanson, E.L.; Higgins, J.; Connick, E.; Moehlman, T.M.; Stothard, E.R.; Wright, K.P. Impact of Circadian Misalignment on Energy Metabolism during Simulated Nightshift Work. Proc. Natl. Acad. Sci. USA 2014, 111, 17302–17307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crispim, C.A.; Waterhouse, J.; Dâmaso, A.R.; Zimberg, I.Z.; Padilha, H.G.; Oyama, L.M.; Tufik, S.; de Mello, M.T. Hormonal Appetite Control Is Altered by Shift Work: A Preliminary Study. Metabolism 2011, 60, 1726–1735. [Google Scholar] [CrossRef] [Green Version]
- Scheer, F.A.J.L.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse Metabolic and Cardiovascular Consequences of Circadian Misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, J.; Wright, K.P. Influence of Weeks of Circadian Misalignment on Leptin Levels. Nat. Sci. Sleep 2010, 2, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molzof, H.E.; Peterson, C.M.; Thomas, S.J.; Gloston, G.F.; Johnson, R.L.; Gamble, K.L. Nightshift Work and Nighttime Eating Are Associated with Higher Insulin and Leptin Levels in Hospital Nurses. Front. Endocrinol. 2022, 13, 876752. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, A.G.; Crujeiras, A.B.; Casanueva, F.F.; Carreira, M.C. Leptin, Obesity, and Leptin Resistance: Where Are We 25 Years Later? Nutrients 2019, 11, 2704. [Google Scholar] [CrossRef] [PubMed]
- Myers, M.G.; Leibel, R.L.; Seeley, R.J.; Schwartz, M.W. Obesity and Leptin Resistance: Distinguishing Cause from Effect. Trends Endocrinol. Metab. 2010, 21, 643–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taheri, S.; Lin, L.; Austin, D.; Young, T.; Mignot, E. Short Sleep Duration Is Associated with Reduced Leptin, Elevated Ghrelin, and Increased Body Mass Index. PLoS Med. 2004, 1, e62. [Google Scholar] [CrossRef]
- Mullington, J.M.; Chan, J.L.; Van Dongen, H.P.A.; Szuba, M.P.; Samaras, J.; Price, N.J.; Meier-Ewert, H.K.; Dinges, D.F.; Mantzoros, C.S. Sleep Loss Reduces Diurnal Rhythm Amplitude of Leptin in Healthy Men. J. Neuroendocrinol. 2003, 15, 851–854. [Google Scholar] [CrossRef] [Green Version]
- Spiegel, K.; Tasali, E.; Penev, P.; Van Cauter, E. Brief Communication: Sleep Curtailment in Healthy Young Men Is Associated with Decreased Leptin Levels, Elevated Ghrelin Levels, and Increased Hunger and Appetite. Ann. Intern. Med. 2004, 141, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A. Soft Drink Consumption and Obesity: It Is All about Fructose. Curr. Opin. Lipidol. 2010, 21, 51–57. [Google Scholar] [CrossRef]
- Biercewicz, M.; Slusarz, R.; Kedziora-Kornatowska, K.; Filipska, K.; Bielawski, K.; Ruszkowska-Ciastek, B. Assessment of Leptin-to-Adiponectin Ratio in Prediction of Insulin Resistance and Nutrition Status in a Geriatric Female Population. J. Physiol. Pharmacol. 2020, 71, 35–46. [Google Scholar] [CrossRef]
- Langenberg, C.; Bergstrom, J.; Laughlin, G.A.; Barrett-Connor, E. Ghrelin and the Metabolic Syndrome in Older Adults. J. Clin. Endocrinol. Metab 2005, 90, 6448–6453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rigamonti, A.E.; Pincelli, A.I.; Corrà, B.; Viarengo, R.; Bonomo, S.M.; Galimberti, D.; Scacchi, M.; Scarpini, E.; Cavagnini, F.; Müller, E.E. Plasma Ghrelin Concentrations in Elderly Subjects: Comparison with Anorexic and Obese Patients. J. Endocrinol. 2002, 175, R1–R5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchesini, G.; Bianchi, G.; Lucidi, P.; Villanova, N.; Zoli, M.; De Feo, P. Plasma Ghrelin Concentrations, Food Intake, and Anorexia in Liver Failure. J. Clin. Endocrinol. Metab. 2004, 89, 2136–2141. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.M.; Wirth, R.; Troegner, J.; Erdmann, J.; Eberl, T.; Heppner, H.J.; Schusdziarra, V.; Sieber, C.C. Ghrelin, Anthropometry and Nutritional Assessment in Geriatric Hospital Patients. Z Gerontol. Geriatr. 2007, 40, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Al-Rawi, N.; Madkour, M.; Jahrami, H.; Salahat, D.; Alhasan, F.; BaHammam, A.; Faris, M.A.-I. Effect of Diurnal Intermittent Fasting during Ramadan on Ghrelin, Leptin, Melatonin, and Cortisol Levels among Overweight and Obese Subjects: A Prospective Observational Study. PLoS ONE 2020, 15, e0237922. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total n = 161 | Physician n = 57 | Paramedics n = 79 | Other n = 24 | |
|---|---|---|---|---|
| Age, years, mean ± SD | 37.4 ± 10.4 | 35.7 ± 10.4 | 39.5 ± 10.2 | 34.9 ± 10.3 |
| Sex, n (%) male | 68 (42.5) | 29 (50.9) | 28 (35.4) | 11 (45.8) |
| BMI, kg/m2, mean ± SD | 23.2 ± 4.4 | 22.9 ± 4.3 | 23.2 ± 3.6 | 23.7 ± 4.4 |
| Underweight, n (%) | 10 (6.2) | 3 (5.3) | 6 (7.6) | 1 (4.2) |
| Normal weight, n (%) | 107 (66.5) | 39 (68.4) | 53 (67.1) | 15 (62.5) |
| Overweight, n (%) | 36 (22.4) | 14 (24.6) | 17 (21.5) | 5 (20.8) |
| Obesity class 1, n (%) | 4 (2.5) | 0 | 1 (1.3) | 3 (12.5) |
| Obesity class 2, n (%) | 1 (0.6) | 0 | 1 (1.3) | 0 |
| Obesity class 3, n (%) | 3 (1.9) | 1 (1.8) | 1 (1.3) | 0 |
| Seniority, years, median [IQR] | ||||
| In the job | 6 [13] | 4 [8.5] | 11 [13] | 4.5 [8.5] |
| In the department | 3 [9] | 2 [4.5] | 5 [9] | 1 [6] |
| Physical activity, h/week, median [IQR] | 2 [4] | 2 [5] | 2 [4] | 2 [3] |
| Tea/coffee, cup/day, median [IQR] | 3 [3] | 4 [2] | 6 [12] | 5 [3.5] |
| Smoker, n (%) | 57 (35.6) | 17 (29.8) | 31 (39.7) | 9 (37.5) |
| Cig/day for smokers, median [IQR] | 6 [9] | 8 [5] | 6 [12] | 5 [3.5] |
| Family situation | ||||
| Married-engaged, n (%) | 108 (67.1) | 35 (61.4) | 63 (79.7) | 9 (37.5) |
| Single-divorced, n (%) | 53 (32.9) | 22 (38.6) | 16 (20.2) | 15 (62.5) |
| Kids at home, n (%) | 55 (41.7) | 16 (33.3) | 35 (53.0) | 4 (22.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bouillon-Minois, J.-B.; Outrey, J.; Pereira, B.; Adeyemi, O.J.; Sapin, V.; Bouvier, D.; Thivel, D.; de Saint-Vincent, S.; Ugbolue, U.C.; Baker, J.S.; et al. The Impact of Job-Demand-Control-Support on Leptin and Ghrelin as Biomarkers of Stress in Emergency Healthcare Workers. Nutrients 2022, 14, 5009. https://doi.org/10.3390/nu14235009
Bouillon-Minois J-B, Outrey J, Pereira B, Adeyemi OJ, Sapin V, Bouvier D, Thivel D, de Saint-Vincent S, Ugbolue UC, Baker JS, et al. The Impact of Job-Demand-Control-Support on Leptin and Ghrelin as Biomarkers of Stress in Emergency Healthcare Workers. Nutrients. 2022; 14(23):5009. https://doi.org/10.3390/nu14235009
Chicago/Turabian StyleBouillon-Minois, Jean-Baptiste, Justin Outrey, Bruno Pereira, Oluwaseun John Adeyemi, Vincent Sapin, Damien Bouvier, David Thivel, Sarah de Saint-Vincent, Ukadike Chris Ugbolue, Julien S. Baker, and et al. 2022. "The Impact of Job-Demand-Control-Support on Leptin and Ghrelin as Biomarkers of Stress in Emergency Healthcare Workers" Nutrients 14, no. 23: 5009. https://doi.org/10.3390/nu14235009