
Role of Inflammatory Factors in Mediating the Effect of Lipids on Nonalcoholic Fatty Liver Disease: A Two-Step, Multivariable Mendelian Randomization Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Resources for MR Analysis
2.3. Genetic IVs
2.4. Replicative Analysis
2.5. Mediation Analysis and MR Analysis
2.6. Sensitivity Analysis
3. Results
3.1. Selection of IVs
3.2. Total Effect of Lipids on NAFLD
3.3. Causal Effect of Inflammatory Factors on NAFLD
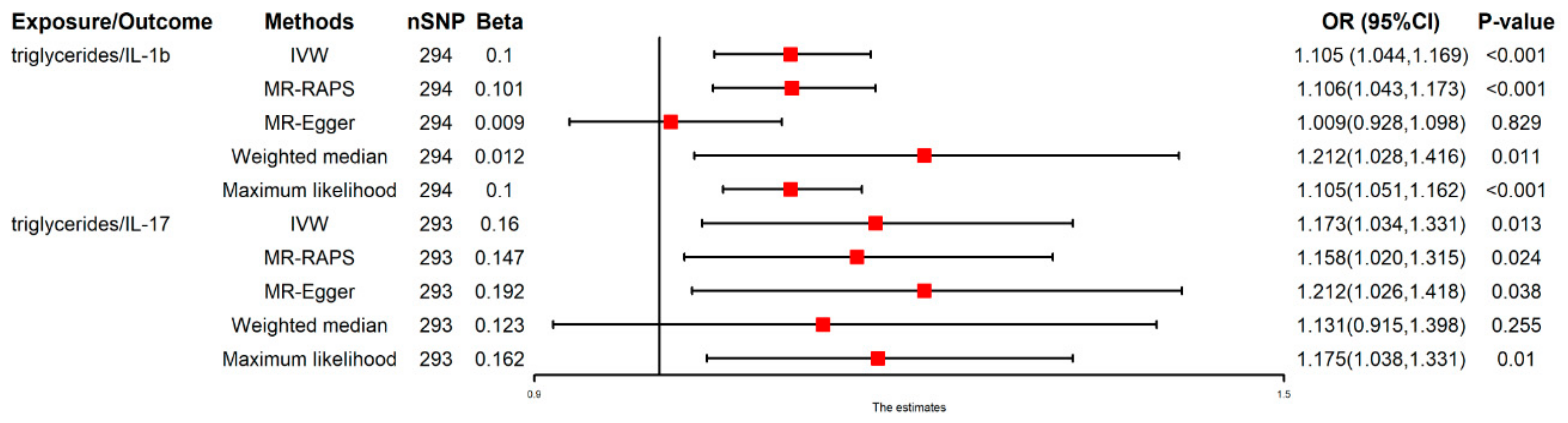
3.4. Casual Effect of TGs on IL-1β and IL-17
3.5. Mediated Effect and Proportion by IL-1β and IL-17
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, X.J.; Malhi, H. Nonalcoholic Fatty Liver Disease. Ann. Intern. Med. 2018, 169, itc65–itc80. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E. Nonalcoholic fatty liver disease: A systematic review. JAMA 2015, 313, 2263–2273. [Google Scholar] [CrossRef] [PubMed]
- El-Kassas, M.; Cabezas, J.; Coz, P.I.; Zheng, M.-H.; Arab, J.P.; Awad, A. Nonalcoholic Fatty Liver Disease: Current Global Burden. Semin. Liver Dis. 2022, 42, 401–412. [Google Scholar] [CrossRef]
- Muzurović, E.; Peng, C.C.; Belanger, M.J.; Sanoudou, D.; Mikhailidis, D.P.; Mantzoros, C.S. Nonalcoholic Fatty Liver Disease and Cardiovascular Disease: A Review of Shared Cardiometabolic Risk Factors. Hypertension 2022, 79, 1319–1326. [Google Scholar] [CrossRef]
- Souza, M.R.; Diniz, M.F.; de Medeiros-Filho, J.E.M.; de Araújo, M.S.T. Metabolic syndrome and risk factors for non-alcoholic fatty liver disease. Arq. Gastroenterol. 2012, 49, 89–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, Y.; Pan, X.; Luo, J.; Xiao, X.; Li, J.; Bestman, P.L.; Luo, M. Association of Inflammatory Cytokines With Non-Alcoholic Fatty Liver Disease. Front. Immunol. 2022, 13, 880298. [Google Scholar] [CrossRef]
- Davies, N.M.; Holmes, M.V.; Smith, G.D. Reading Mendelian randomisation studies: A guide, glossary, and checklist for clinicians. BMJ 2018, 362, k601. [Google Scholar] [CrossRef] [Green Version]
- Burgess, S.; Thompson, S.G. Avoiding bias from weak instruments in Mendelian randomization studies. Int. J. Epidemiol. 2011, 40, 755–764. [Google Scholar] [CrossRef] [Green Version]
- Richardson, T.G.; Sanderson, E.; Palmer, T.M.; Ala-Korpela, M.; Ference, B.A.; Smith, G.D.; Holmes, M.V. Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: A multivariable Mendelian randomisation analysis. PLoS Med. 2020, 17, e1003062. [Google Scholar] [CrossRef] [Green Version]
- Rusk, N. The UK Biobank. Nat. Methods 2018, 15, 1001. [Google Scholar] [CrossRef]
- Folkersen, L.; Gustafsson, S.; Wang, Q.; Hansen, D.H.; Hedman, Å.K.; Schork, A.; Page, K.; Zhernakova, D.V.; Wu, Y.; Peters, J.; et al. Genomic and drug target evaluation of 90 cardiovascular proteins in 30,931 individuals. Nat. Metab. 2020, 2, 1135–1148. [Google Scholar] [CrossRef] [PubMed]
- Ahola-Olli, A.V.; Würtz, P.; Havulinna, A.S.; Aalto, K.; Pitkänen, N.; Lehtimäki, T.; Kähönen, M.; Lyytikäinen, L.-P.; Raitoharju, E.; Seppälä, I.; et al. Genome-wide Association Study Identifies 27 Loci Influencing Concentrations of Circulating Cytokines and Growth Factors. Am. J. Hum. Genet. 2017, 100, 40–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Lee, S.; Kim, Y.; Lee, Y.; Kang, M.W.; Kim, K.; Kim, Y.C.; Han, S.S.; Lee, H.; Lee, J.P.; et al. Atrial fibrillation and kidney function: A bidirectional Mendelian randomization study. Eur. Heart J. 2021, 42, 2816–2823. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.R.; Sanderson, E.; Hammerton, G.; Richmond, R.C.; Smith, G.D.; Heron, J.; Taylor, A.E.; Davies, N.M.; Howe, L.D. Mendelian randomisation for mediation analysis: Current methods and challenges for implementation. Eur. J. Epidemiol. 2021, 36, 465–478. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.S.; Holmes, M.V.; Zheng, J.; Sanderson, E.; Carter, A.R. The impact of education inequality on rheumatoid arthritis risk is mediated by smoking and body mass index: Mendelian randomization study. Rheumatology 2022, 61, 2167–2175. [Google Scholar] [CrossRef] [PubMed]
- Varbo, A.; Benn, M.; Smith, G.D.; Timpson, N.J.; Tybjærg-Hansen, A.; Nordestgaard, B.G. Remnant cholesterol, low-density lipoprotein cholesterol, and blood pressure as mediators from obesity to ischemic heart disease. Circ. Res. 2015, 116, 665–673. [Google Scholar] [CrossRef] [Green Version]
- Holmes, M.V.; Ala-Korpela, M.; Smith, G.D. Mendelian randomization in cardiometabolic disease: Challenges in evaluating causality. Nat. Rev. Cardiol. 2017, 14, 577–590. [Google Scholar] [CrossRef] [Green Version]
- Hartwig, F.P.; Smith, G.D.; Bowden, J. Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. Int. J. Epidemiol. 2017, 46, 1985–1998. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.; Smith, G.D.; Haycock, P.C.; Burgess, S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet. Epidemiol. 2016, 40, 304–314. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.; Smith, G.D.; Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through Egger regression. Int. J. Epidemiol. 2015, 44, 512–525. [Google Scholar] [CrossRef]
- Zhao, Q.; Wang, J.; Hemani, G.; Bowden, J.; Small, D.S. Statistical inference in two-sample summary-data Mendelian randomization using robust adjusted profile score. Ann. Stat. 2020, 48, 1742–1769. [Google Scholar] [CrossRef]
- Choi, K.W.; Chen, C.-Y.; Stein, M.B.; Klimentidis, Y.C.; Wang, M.-J.; Koenen, K.C.; Smoller, J.W.; Wray, N.R.; Ripke, S.; Mattheisen, M.; et al. Assessment of Bidirectional Relationships Between Physical Activity and Depression Among Adults: A 2-Sample Mendelian Randomization Study. JAMA Psychiatry 2019, 76, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Burgess, S.; Thompson, S.G. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur. J. Epidemiol. 2017, 32, 377–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corona, G.; Monami, M.; Rastrelli, G.; Aversa, A.; Tishova, Y.; Saad, F.; Lenzi, A.; Forti, G.; Mannucci, E.; Maggi, M. Testosterone and metabolic syndrome: A meta-analysis study. J. Sex. Med. 2011, 8, 272–283. [Google Scholar] [CrossRef]
- Diehl, A.M.; Goodman, Z.; Ishak, K.G. Alcohollike liver disease in nonalcoholics. A clinical and histologic comparison with alcohol-induced liver injury. Gastroenterology 1988, 95, 1056–1062. [Google Scholar] [CrossRef]
- Kawano, Y.; Cohen, D.E. Mechanisms of hepatic triglyceride accumulation in non-alcoholic fatty liver disease. J. Gastroenterol. 2013, 48, 434–441. [Google Scholar] [CrossRef] [Green Version]
- Carr, R.M.; Oranu, A.; Khungar, V. Nonalcoholic Fatty Liver Disease: Pathophysiology and Management. Gastroenterol. Clin. N. Am. 2016, 45, 639–652. [Google Scholar] [CrossRef] [Green Version]
- Pierantonelli, I.; Svegliati-Baroni, G. Nonalcoholic Fatty Liver Disease: Basic Pathogenetic Mechanisms in the Progression From NAFLD to NASH. Transplantation 2019, 103, e1–e13. [Google Scholar] [CrossRef]
- Alves-Bezerra, M.; Cohen, D.E. Triglyceride Metabolism in the Liver. Compr. Physiol. 2017, 8, 1–8. [Google Scholar]
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef]
- Lopez-Castejon, G.; Brough, D. Understanding the mechanism of IL-1β secretion. Cytokine Growth Factor Rev. 2011, 22, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.; Wasiliew, P.; Kracht, M. Interleukin-1beta (IL-1beta) processing pathway. Sci. Signal. 2010, 3, cm2. [Google Scholar] [PubMed]
- Amatya, N.; Garg, A.V.; Gaffen, S.L. IL-17 Signaling: The Yin and the Yang. Trends Immunol. 2017, 38, 310–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omidian, Z.; Ahmed, R.; Giwa, A.; Donner, T.; Hamad, A.R.A. IL-17 and limits of success. Cell. Immunol. 2019, 339, 33–40. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Trait | Consortium | Ethnicity | Sample Size |
|---|---|---|---|
| NAFLD (n, %) | FinnGen Biobank | European | 218,792 |
| NAFLD (n, %) | UK Biobank | European | / |
| HDL cholesterol (mmol/L) | UK Biobank | European | 403,943 |
| LDL cholesterol (mmol/L) | UK Biobank | European | 440,546 |
| apolipoprotein B (mmol/L) | UK Biobank | European | 439,214 |
| apolipoprotein A-1 (mmol/L) | UK Biobank | European | 393,193 |
| triglycerides (mmol/L) | UK Biobank | European | 441,016 |
| Interleukin-1β(mmol/L) | SCALLOP consortium | European | 21,758 |
| Interleukin-18 (mmol/L) | SCALLOP consortium | European | 21,758 |
| Interleukin-16 (mmol/L) | YFS/FINRISK | European | 3,483 |
| Interleukin-6 (mmol/L) | SCALLOP consortium | European | 21,758 |
| Interleukin-17 (mmol/L) | SCALLOP consortium | European | 21,758 |
| Exposure Traits | Outcome Traits | Raw Estimates | Outlines Corrected Estimates | ||||
|---|---|---|---|---|---|---|---|
| N | Beta | p-Value | N | Beta | p-Value | ||
| LDL-C | NAFLD | 155 | −0.081 | 0.631 | 151 | −0.115 | 0.422 |
| HDL-C | NAFLD | 315 | −0.318 | 0.016 | 312 | −0.334 | 0.007 |
| apolipoprotein B | NAFLD | 179 | −0.052 | 0.721 | 176 | −0.088 | 0.502 |
| apolipoprotein A1 | NAFLD | 261 | −0.237 | 0.116 | 258 | −0.278 | 0.381 |
| triglycerides | NAFLD | 275 | 0.32 | 0.022 | 269 | 0.331 | 0.013 |
| IL-1β | NAFLD | 18 | 0.273 | 0.016 | NA | NA | NA |
| IL-18 | NAFLD | 7 | −0.228 | 0.293 | NA | NA | NA |
| IL-16 | NAFLD | NA | NA | NA | NA | NA | NA |
| IL-6 | NAFLD | 20 | −0.017 | 0.904 | NA | NA | NA |
| IL-17 | NAFLD | 8 | 0.384 | 0.021 | NA | NA | NA |
| triglycerides | IL-1β | 294 | 0.106 | 0.0002 | 293 | 0.108 | 0.0001 |
| triglycerides | IL-1β | 293 | 0.162 | 0.012 | 291 | 0.166 | 0.007 |
| Exposure | Outcome | Heterogeneity | Pleiotropy | |||
|---|---|---|---|---|---|---|
| Method | Cochran’s Q | p-Value | Egger-Intercept (95%CI) | p-Value | ||
| HDL cholesterol | NAFLD | IVW | 404.387 | <0.001 | 0.001 (−0.001,0.002) | 0.937 |
| LDL cholesterol | NAFLD | IVW | 238.420 | <0.001 | 0.016 (−0.021,0.037) | 0.069 |
| apolipoprotein B | NAFLD | IVW | 261.564 | <0.001 | 0.017 (−0.020,0.038) | 0.124 |
| apolipoprotein A1 | NAFLD | IVW | 399.391 | <0.001 | −0.005 (−0.018,0.008) | 0.525 |
| triglycerides | NAFLD | IVW | 397.854 | <0.001 | 0.003 (−0.009,0.015) | 0.641 |
| IL-1β | NAFLD | IVW | 14.263 | 0.579 | −0.030 (−0.090,0.030) | 0.447 |
| IL-18 | NAFLD | IVW | 1.038 | 0.959 | −0.040 (−0.140,0.060) | 0.485 |
| IL-16 | NAFLD | IVW | 0.403 | 0.525 | −0.030 (−0.130,0.070) | 0.697 |
| IL-6 | NAFLD | IVW | 17.814 | 0.468 | −0.015 (−0.075,0.045) | 0.632 |
| IL-17 | NAFLD | IVW | 3.729 | 0.810 | −0.081 (−0.181,0.019) | 0.208 |
| triglycerides | IL-1β | IVW | 362.882 | 0.003 | 0.004 (−0.001,0.009) | 0.173 |
| triglycerides | IL-17 | IVW | 302.256 | 0.313 | −0.001 (−0.005,0.003) | 0.676 |
| Exposure/Outcome | Adjusted Factors | Multivariate MR Analysis | Mediation Effect (%) | ||
|---|---|---|---|---|---|
| nSNP | OR (95%CI) | p-Value | |||
| triglycerides/NAFLD | None | 275 | 1.455 (1.110,1.924) | 0.009 | |
| triglycerides/NAFLD | Interleukin-1β | 287 | 1.214 (1.012,1.410) | 0.019 | 3.1 |
| triglycerides/NAFLD | Interleukin-17 | 276 | 1.250 (1.033,1.467) | 0.013 | 2.6 |
| triglycerides/NAFLD | Interleukin-1β, Interleukin-17 | 288 | 1.197 (0.794,1.600) | 0.224 | 14.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Zhou, H.; Jin, H.; Liu, K. Role of Inflammatory Factors in Mediating the Effect of Lipids on Nonalcoholic Fatty Liver Disease: A Two-Step, Multivariable Mendelian Randomization Study. Nutrients 2022, 14, 4434. https://doi.org/10.3390/nu14204434
Chen J, Zhou H, Jin H, Liu K. Role of Inflammatory Factors in Mediating the Effect of Lipids on Nonalcoholic Fatty Liver Disease: A Two-Step, Multivariable Mendelian Randomization Study. Nutrients. 2022; 14(20):4434. https://doi.org/10.3390/nu14204434
Chicago/Turabian StyleChen, Junhong, Hao Zhou, Hengwei Jin, and Kai Liu. 2022. "Role of Inflammatory Factors in Mediating the Effect of Lipids on Nonalcoholic Fatty Liver Disease: A Two-Step, Multivariable Mendelian Randomization Study" Nutrients 14, no. 20: 4434. https://doi.org/10.3390/nu14204434