
Breastfeeding Practices and Associated Factors in Shanghai: A Cross-Sectional Study
 , ,
, ,
Abstract
:
1. Introduction
2. Methods
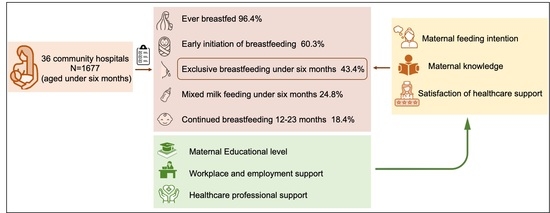
2.1. Study Design and Study Participants
2.2. Questionnaire, Data Collection and Management
2.3. Breastfeeding Indicators
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Breastfeeding Indicators
3.3. Determinants of Exclusive Breastfeeding
3.3.1. Maternal Educational Level and Feeding Intentions in Pregnancy (or the Prenatal Period)
3.3.2. Workplace and Employment
3.3.3. Health Professional Support
3.3.4. Marketing of Formula Milk and Exclusive Breastfeeding
4. Discussion
4.1. Current Situation of Breastfeeding Practices in Shanghai
4.2. Workplace and Employment
4.3. Health Professional Support
4.4. Marketing of Formula Milk
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Victora, C.G.; Horta, B.L.; Loret de Mola, C.; Quevedo, L.; Pinheiro, R.T.; Gigante, D.P.; Gonçalves, H.; Barros, F.C. Association between breastfeeding and intelligence, educational attainment, and income at 30 years of age: A prospective birth cohort study from Brazil. Lancet Glob. Health 2015, 3, e199–e205. [Google Scholar] [CrossRef] [Green Version]
- Rito, A.I.; Buoncristiano, M.; Spinelli, A.; Salanave, B.; Kunesova, M.; Hejgaard, T.; Solano, M.G.; Fijalkowska, A.; Sturua, L.; Hyska, J.; et al. Association between Characteristics at Birth, Breastfeeding and Obesity in 22 Countries: The WHO European Childhood Obesity Surveillance Initiative—COSI 2015/2017. Obes. Facts 2019, 12, 226–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babic, A.; Sasamoto, N.; Rosner, B.A.; Tworoger, S.S.; Jordan, S.J.; Risch, H.A.; Harris, H.R.; Rossing, M.A.; Doherty, J.A.; Fortner, R.T.; et al. Association Between Breastfeeding and Ovarian Cancer Risk. JAMA Oncol. 2020, 6, e200421. [Google Scholar] [CrossRef] [PubMed]
- Westerfield, K.L.; Koenig, K.; Oh, R. Breastfeeding: Common Questions and Answers. Am. Fam. Physician 2018, 98, 368–373. [Google Scholar]
- Park, Y.; Sinn, D.H.; Oh, J.H.; Goh, M.J.; Kim, K.; Kang, W.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; Koh, K.C.; et al. The Association Between Breastfeeding and Nonalcoholic Fatty Liver Disease in Parous Women: A Nation-wide Cohort Study. Hepatology 2021, 74, 2988–2997. [Google Scholar] [CrossRef]
- World Health Organization and the United Nations Children’s Fund (UNICEF). Indicators for Assessing Infant and Young Child Feeding Practices: Definitions and Measurement Methods; World Health Organization and the United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2021. [Google Scholar]
- Baker, P.; Melo, T.; Neves, P.A.; Machado, P.; Smith, J.; Piwoz, E.; Barros, A.J.D.; Victora, C.G.; McCoy, D. First-food systems transformations and the ultra-processing of infant and young child diets: The determinants, dynamics and consequences of the global rise in commercial milk formula consumption. Matern. Child Nutr. 2021, 17, e13097. [Google Scholar] [CrossRef]
- UNICEF. The State of The World’s Children 2019; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- Li, Q.; Tian, J.; Xu, F.; Binns, C. Breastfeeding in China: A Review of Changes in the Past Decade. Int. J. Environ. Res. Public Health 2020, 7, 8234. [Google Scholar] [CrossRef]
- Yang, Z.Y.; Lai, J.Q.; Yu, D.M.; Duan, Y.F.; Pang, X.H.; Jiang, S.; Bi, Y.; Wang, J.; Zhao, L.Y.; Yin, S.A. Breastfeeding rates in China: A cross-sectional survey and estimate of benefits of improvement. Lancet 2016, 388, 47. [Google Scholar] [CrossRef]
- Duan, Y.; Yang, Z.; Lai, J.; Yu, D.; Chang, S.; Pang, X.; Jiang, S.; Zhang, H.; Bi, Y.; Wang, J.; et al. Exclusive Breastfeeding Rate and Complementary Feeding Indicators in China: A National Representative Survey in 2013. Nutrients 2018, 10, 249. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Yang, Y.; Yin, X.; Li, J.; Fang, J.; Wang, X. Determinants of exclusive breastfeeding for the first six months in China: A cross-sectional study. Int. Breastfeed. J. 2021, 16, 40. [Google Scholar] [CrossRef]
- Li, J.; Nguyen, T.T.; Wang, X.; Mathisen, R.; Fang, J. Breastfeeding practices and associated factors at the individual, family, health facility and environmental levels in China. Matern. Child Nutr. 2020, 16, e13002. [Google Scholar] [CrossRef] [PubMed]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G.; Grp, L.B.S. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Wu, Y.; Marc, I.; Bouchard, L.; Ouyang, F.; Luo, Z.C.; Fan, J.; Dubois, L.; Mâsse, B.; Zhang, J.; Leung, P.C.K.; et al. Study protocol for the Sino-Canadian Healthy Life Trajectories Initiative (SCHeLTI): A multicentre, cluster-randomised, parallel-group, superiority trial of a multifaceted community-family-mother-child intervention to prevent childhood overweight and obesity. BMJ Open 2021, 4, e045192. [Google Scholar]
- United Nations Children’s Fund. Global UNICEF Global Databases: Infant and Young Child Feeding; United Nations Children’s Fund: Geneva, Switzerland, 2021. [Google Scholar]
- Xi, X.X. Reasons for China’s Changing Female Labor Force Participation Rate. Acsr. Adv. Comput. 2017, 76, 277–282. [Google Scholar]
- Navarro-Rosenblatt, D.; Garmendia, M.L. Maternity Leave and Its Impact on Breastfeeding: A Review of the Literature. Breastfeed. Med. 2018, 13, 589–597. [Google Scholar] [CrossRef]
- Maternity Leave for Working Mothers Has Been Extended from 98 to 158 Days. Available online: http://wsjkw.sh.gov.cn/xwfb/20211125/e7e60934b6d24dec9f86d035939888f6.html (accessed on 10 August 2022).
- Qiao, J.; Wang, Y.; Li, X.; Jiang, F.; Zhang, Y.; Ma, J.; Song, Y.; Ma, J.; Fu, W.; Pang, R.; et al. A Lancet Commission on 70 years of women’s reproductive, maternal, newborn, child, and adolescent health in China. Lancet 2021, 397, 2497–2536. [Google Scholar] [CrossRef]
- Baby-Friendly Hospitals in Shanghai up to April 2022. Available online: http://wsjkw.sh.gov.cn/fwjg/20180601/0012-55912.html (accessed on 10 August 2022).
- Huang, Y.; Bu, F.; Wang, J.; Fang, W. Breastfeeding Initiation and Related Factors in Postpartum Mothers in a District of Shanghai. Shanghai J. Prev. Med. 2022, 1–15. Available online: http://kns.cnki.net/kcms/detail/31.1635.R.20220801.1954.006.html (accessed on 10 August 2022).
- Li, L.L.; Song, H.Q.; Zhang, Y.; Li, H.; Li, M.; Jiang, H.; Yang, Y.J.; Wu, Y.; Gu, C.Y.; Yu, Y.L.; et al. Breastfeeding Supportive Services in Baby-Friendly Hospitals Positively Influenced Exclusive Breastfeeding Practice at Hospitalization Discharge and Six Months Postpartum. Int. J. Environ. Res. Public Health 2021, 18, 11430. [Google Scholar] [CrossRef]
- World Health Organization and the United Nations Children’s Fund (UNICEF). How the Marketing of Formula Milk Influences our Decisions on Infant Feeding; World Health Organization and the United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2022. [Google Scholar]
- Baker, P.; Smith, J.; Salmon, L.; Friel, S.; Kent, G.; Iellamo, A.; Dadhich, J.P.; Renfrew, M.J. Global trends and patterns of commercial milk-based formula sales: Is an unprecedented infant and young child feeding transition underway? Public Health Nutr. 2016, 19, 2540–2550. [Google Scholar] [CrossRef] [Green Version]
- Colombo, L.; Crippa, B.L.; Consonni, D.; Bettinelli, M.E.; Agosti, V.; Mangino, G.; Bezze, E.N.; Mauri, P.A.; Zanotta, L.; Roggero, P.; et al. Breastfeeding Determinants in Healthy Term Newborns. Nutrients 2018, 10, 48. [Google Scholar] [CrossRef] [Green Version]
- Xiao, X.; Loke, A.Y.; Zhu, S.N.; Gong, L.; Shi, H.M.; Ngai, F.W. “The sweet and the bitter”: Mothers’ experiences of breastfeeding in the early postpartum period: A qualitative exploratory study in China. Int. Breastfeed. J. 2020, 15, 12. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Maternal age at delivery | |
| 20–24 y | 110 (6.5) |
| 25–29 y | 578 (34.5) |
| 30–34 y | 694 (41.4) |
| ≥35 y | 295 (17.6) |
| Ethnicity | |
| Han | 1636 (97.6) |
| Minorities | 41 (2.4) |
| Marital status | |
| Married/co-habiting | 1656 (98.8) |
| Other | 21 (1.2) |
| Educational level | |
| Senior high or below | 241 (14.4) |
| Bachelor’s degree | 1209 (72.1) |
| Master’s or above | 213 (12.7) |
| Don’t know/refuse to answer | 14 (0.8) |
| Employment status | |
| Full-time employed | 1177 (70.2) |
| Work informally/Part-time employed | 97 (5.8) |
| Housewife | 403 (24.0) |
| Type of employee | |
| State civil servant | 231(18.1) |
| State-owned enterprise | 203(15.9) |
| Multinational company | 240(18.8) |
| Private enterprise | 375 (29.4) |
| Self-employed | 79 (6.2) |
| Others | 146 (11.5) |
| Annual household income | |
| <150,000 CNY | 682 (40.7) |
| 150,000–300,000 CNY | 514 (30.6) |
| >300,000 CNY | 288 (17.2) |
| Don’t know/refuse to answer | 193 (11.5) |
| Antenatal feeding intentions | |
| Exclusive breastfeeding | 1036 (61.8) |
| Mixed milk feeding | 513 (30.6) |
| Not breastfed | 16 (0.9) |
| No plan | 112 (6.7) |
| The first child | |
| Yes | 1290 (76.9) |
| No | 387(23.1) |
| Gender of child | |
| Boy | 859 (51.2) |
| Girl | 818 (48.8) |
| Delivery mode | |
| Vaginal birth | 1066 (63.6) |
| Caesarean section | 611 (36.4) |
| Gestational age | |
| Pre-term (28–36+6 gestational weeks) | 96 (5.7) |
| Full-term (≥37 gestational weeks) | 1581 (94.3) |
| Birth weight | |
| <2500 g | 74 (4.4) |
| 2500–3499 g | 1507 (89.9) |
| ≥4000 g | 96 (5.7) |
| BMS marketing massage received * | |
| Pre-conception | 474(28.3) |
| Pregnancy | 1602(95.5) |
| Postnatal | 1614(96.2) |
| Indicators | Percentage (%) | |
|---|---|---|
| 1 | Ever breastfed (EvBF) | 96.4 (2569/2665) |
| 2 | Early initiation of breastfeeding (EIBF) | 60.3 (1608/2665) |
| 3 | Exclusive breastfeeding under 6 months (EBF) | 43.4 (727/1677) |
| 0–1 month | 43.2 (235/544) | |
| 2–3 months | 47.3 (320/676) | |
| 4–5 months | 37.6 (172/457) | |
| 0–3 months | 45.5 (555/1220) | |
| 4 | Mixed milk feeding under six months (MixMF) | 24.8 (416/1677) |
| 0–1 month | 28.7 (156/544) | |
| 2–3 months | 21.8 (147/676) | |
| 4–5 months | 24.7 (113/457) | |
| 5 | Continued breastfeeding 12–23 months (CBF) | 18.4 (100/543) |
| 12–15 months | 25.3 (61/241) | |
| 16–19 months | 13.2 (26/197) | |
| 20–23 months | 12.4 (13/105) |
| Variable | Percentage of EBF | Univariable Model | |
| OR (95% CI) | p-Value | ||
| Maternal age at delivery, years | 0.546 | ||
| ≤24 | 40.91% | 1.02 (0.66, 1.50) | |
| 25–29 | 45.16% | 1.22 (0.92, 1.62) | |
| 30–34 | 43.52% | 1.14 (0.86, 1.53) | |
| ≥35 | 40.34% | 1.00 | |
| Educational level | <0.001 | ||
| Master’s or above | 51.17% | 2.56 (1.74,3.78) | |
| Bachelor’s degree | 45.08% | 2.00 (1.48,2.71) | |
| Senior high or below | 29.05% | 1.00 | |
| Employment status | 0.004 | ||
| Housewife | 43.18% | 0.94 (0.75, 1.18) | |
| Part-time employed | 26.80% | 0.45 (0.28, 0.72) | |
| Full-time employed | 44.77% | 1.00 | |
| Type of employee | 0.047 | ||
| State civil servant | 49.78% | 1.00 | |
| State-owned enterprise | 48.77% | 0.96 (0.66,1.40) | |
| Multinational company | 43.75% | 0.79 (0.55,1.13) | |
| Private enterprise | 38.73% | 0.64 (0.46,0.89) | |
| Self-employed | 37.50% | 0.61 (0.36,1.02) | |
| Others | 40.27% | 0.68 (0.45,1.03) | |
| Annual household income | <0.001 | ||
| >300,000 CNY | 50.00% | 1.70 (1.28,2.24) | |
| 150,000–300,000 CNY | 47.28% | 1.52 (1.21,1.92) | |
| <150,000 CNY | 37.10% | 1.00 | |
| Gestational age | 0.005 | ||
| Full-term | 44.21% | 1.92 (1.23, 3.02) | |
| Pre-term | 29.17% | 1.00 | |
| Delivery mode | 0.003 | ||
| Vaginal birth | 46.06% | 1.36 (1.11, 1.66) | |
| Caesarean section | 38.63% | 1.00 | |
| Paid maternity leave | 0.029 | ||
| ≥120 days | 47.07% | 1.35 (1.03,1.77) | |
| <119 days | 39.74% | 1.00 | |
| Antenatal feeding intention | <0.001 | ||
| Exclusive breastfeeding | 57.05% | 5.70 (4.44, 7.32) | |
| Mixed milk feeding | 18.90% | 1.00 | |
| Viewpoint on the statement “Breast milk is beneficial to children intellectual development” | <0.001 | ||
| Beneficial | 38.94% | 1.62 (1.07, 2.45) | |
| Beneficial with proper raising environment | 48.67% | 2.41 (1.61, 3.60) | |
| Not related | 28.24% | 1.00 | |
| Viewpoint on the statement “Lower risk of obesity and diabetes for breast milk” | <0.001 | ||
| Yes, I agree | 55.31% | 2.09 (1.65,2.65) | |
| Partly agree, Need further verification | 45.03% | 1.38 (1.09,1.76) | |
| I have never heard of it before | 37.19% | 1.00 | |
| Participation in breastfeeding classes | 0.021 | ||
| Yes | 45.78% | 1.26 (1.04, 1.53) | |
| No | 40.11% | 1.00 | |
| Overall satisfaction of information and support provided by healthcare system after delivery | 0.014 | ||
| Satisfied | 46.12% | 1.98 (1.15, 3.43) | |
| Not satisfied | 30.16% | 1.00 | |
| Initiated early breastfeeding within an hour after birth | <0.001 | ||
| Yes | 1.88 (1.54,2.30) | ||
| No | 1.00 | ||
| Advertisement state that “formula milk can make children sleep well and reduce crying at night” | 0.3250 | ||
| Will try | 36.56% | 1.38 (0.89,2.14) | |
| Will gather more information before making decisions | 42.65% | 1.29 (0.82,2.03) | |
| Won’t try | 44.33% | 1.00 | |
| Adjusted OR (95% CI) * | p-Value | |
|---|---|---|
| Antenatal feeding intention | <0.001 | |
| Exclusive breastfeeding | 4.87 (3.46, 6.84) | |
| Mixed milk feeding | 1.00 | |
| Viewpoint on the statement “lower risk of obesity and diabetes for breast milk” | 0.007 | |
| Yes, I agree | 1.56 (1.08,2.25) | |
| Partly agree, Need further verification | 1.31 (0.88,1.96) | |
| I have never heard of it before | 1.00 | |
| Overall satisfaction of information and support provided by healthcare system after delivery | 0.030 | |
| Satisfied | 2.56 (1.13, 5.80) | |
| Not satisfied | 1.00 |
| EBF | MixMF | Not Breastfed | p-Value | |
|---|---|---|---|---|
| % | % | % | ||
| Educational level | N1 = 724 | N2 = 416 | N3 = 534 | <0.0001 |
| Senior high or below | 70 (29.1) | 52 (21.6) | 119 (49.4) | |
| Bachelor’s degree | 545 (45.1) | 295 (24.4) | 369 (30.5) | |
| Master’s or above | 109 (51.2) | 68 (31.9) | 36 (16.9) |
| EBF | MixMF | Not Breastfed | p-Value | |
|---|---|---|---|---|
| % | % | % | ||
| Attitude toward benefits of breast milk and formula | 0.863 | |||
| Different | 600 (86.2) | 345 (85.2) | 412 (85.3) | |
| Almost the same | 96 (13.8) | 60 (14.8) | 71 (14.7) | |
| Viewpoint of relationship between breastfeeding and children intellectual development | <0.0001 | |||
| Beneficial | 250 (34.4) | 132 (31.7) | 260 (48.7) | |
| Beneficial with proper raising environment | 440 (60.5) | 237 (57.0) | 227 (42.5) | |
| Not related | 37 (5.1) | 47 (11.3) | 47 (8.8) | |
| Viewpoint of lower risk of obesity and diabetes for breastfed children | <0.0001 | |||
| I have never heard of it before | 331 (45.5) | 220 (52.9) | 339 (64.5) | |
| Need further verification | 172 (23.7) | 101 (24.3) | 109 (20.4) | |
| Yes, I agree | 224 (30.8) | 95 (22.8) | 86 (16.1) | |
| Attitude toward “Formula milk can make children sleep well and reduce crying at night” | <0.0001 | |||
| Will try | 34 (5.0) | 10 (2.5) | 49 (9.9) | |
| Will gather more information before making decisions | 186 (27.3) | 123 (30.8) | 133 (26.9) | |
| Won’t try | 461 (67.7) | 266 (66.7) | 313 (63.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hao, Y.; Wang, L.; Wang, C.; Peng, A.; Gao, W.; Marc, I.; Semenic, S.; Fraser, W.D.; Narayan, A.; Wu, Y.; et al. Breastfeeding Practices and Associated Factors in Shanghai: A Cross-Sectional Study. Nutrients 2022, 14, 4429. https://doi.org/10.3390/nu14204429
Hao Y, Wang L, Wang C, Peng A, Gao W, Marc I, Semenic S, Fraser WD, Narayan A, Wu Y, et al. Breastfeeding Practices and Associated Factors in Shanghai: A Cross-Sectional Study. Nutrients. 2022; 14(20):4429. https://doi.org/10.3390/nu14204429
Chicago/Turabian StyleHao, Yanhui, Lulu Wang, Caifeng Wang, Aiping Peng, Wei Gao, Isabelle Marc, Sonia Semenic, William D. Fraser, Anuradha Narayan, Yanting Wu, and et al. 2022. "Breastfeeding Practices and Associated Factors in Shanghai: A Cross-Sectional Study" Nutrients 14, no. 20: 4429. https://doi.org/10.3390/nu14204429