
Dietary Pattern Influences Gestational Weight Gain: Results from the ProcriAr Cohort Study—São Paulo, Brazil
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
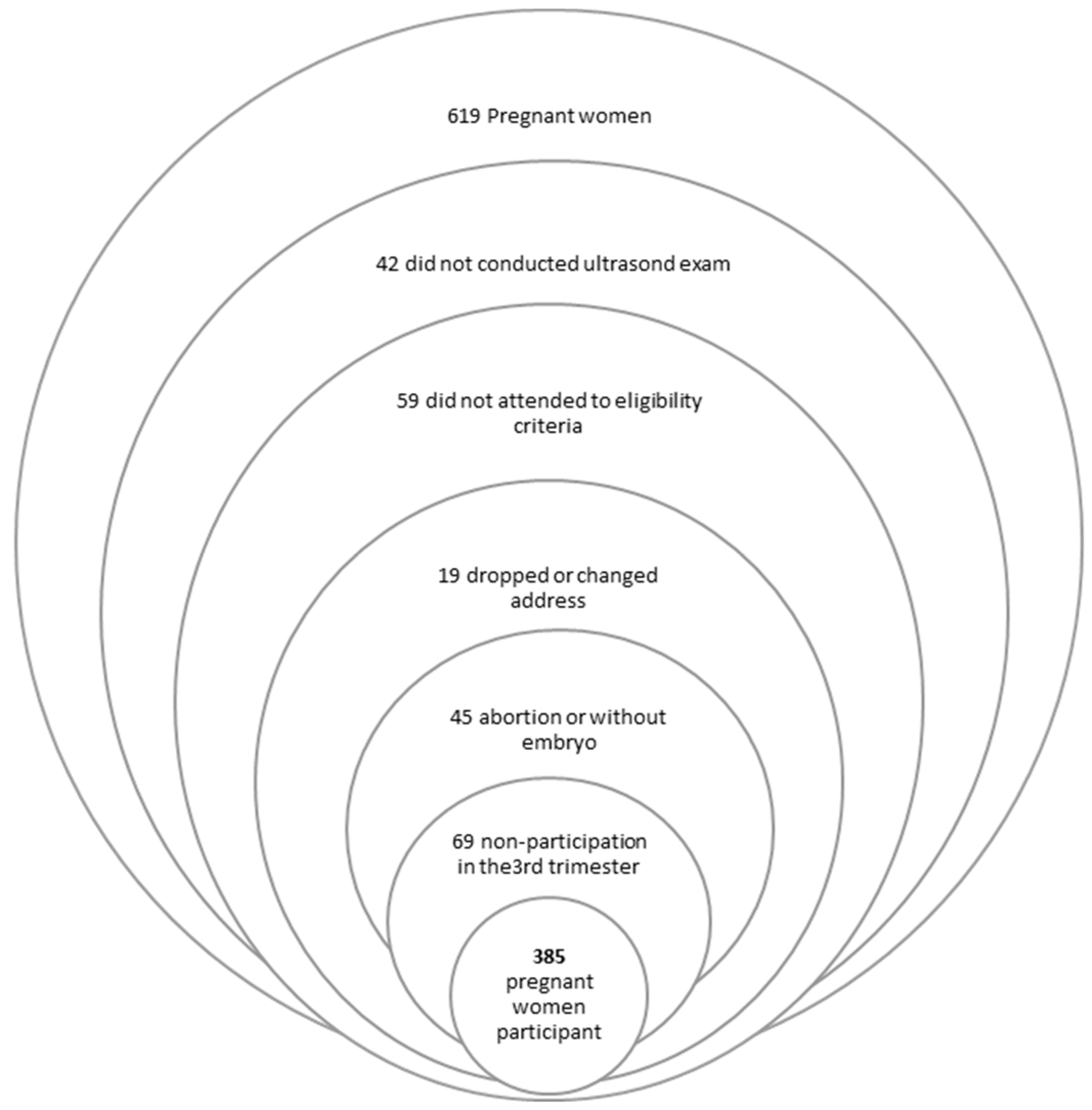
2.2. Characteristics of the Study Group
2.3. Nutritional Status
2.4. Dietary Intake Assessment
2.5. Principal Component Analysis
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine and National Research Council. Weight Gain During Pregnancy: Reexamining the Guidelines; The National Academies Press: Washington, DC, USA, 2009. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Siega-Riz, A.M.; Deierlein, A.; Stuebe, A. Implementation of the New Institute of Medicine Gestational Weight Gain Guidelines. J. Midwifery Women’s Health 2010, 55, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.J.; Bergström, A.; Jaddoe, V.W. Impact of Maternal Body Mass Index and Gestational Weight Gain on Pregnancy Complications: An Individual Participant Data Meta-Analysis of European, North American and Australian Cohorts. BJOG 2019, 126, 984–995. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.L.; Boyle, J.A.; Harrison, C.L.; Teede, H.J. Gestational Weight Gain Across Continents and Ethnicity: Systematic Review and Meta-Analysis of Maternal and Infant Outcomes in More than One Million Women. BMC Med. 2018, 16, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deputy, N.P.; Sharma, A.J.; Kim, S.Y.; Hinkle, S.N. Prevalence and Characteristics Associated with Gestational Weight Gain Adequacy. Obstet. Gynecol. 2015, 125, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Alberico, S.; Montico, M.; Barresi, V.; Monasta, L.; Businelli, C.; Soini, V.; Erenbourg, A.; Ronfani, L.; Maso, G. The Role of Gestational Diabetes, Pre-Pregnancy Body Mass Index, and Gestational Weight Gain on the Risk of Newborn Macrosomia: Results From a Prospective Multicentre Study. BMC Pregnancy Childbirth 2014, 14, 23. [Google Scholar] [CrossRef] [Green Version]
- Beyerlein, A.; Nehring, I.; Rzehak, P.; Heinrich, J.; Müller, M.J.; Plachta-Danielzik, S.; Wabitsch, M.; Weck, M.; Brenner, H.; Rothenbacher, D.; et al. Gestational Weight Gain and Body Mass Index in Children: Results From Three German Cohort Studies. PLoS ONE 2012, 7, e33205. [Google Scholar]
- Suliga, E.; Rokita, W.; Adamczyk-Gruszka, O.; Pazera, G.; Cieśla, E.; Głuszek, S. Factors Associated With Gestational Weight Gain: A Cross-Sectional Survey. BMC Pregnancy Childbirth 2018, 18, 465. [Google Scholar] [CrossRef]
- Godoy, A.C.; Nascimento, S.L.D.; Surita, F.G. A Systematic Review and Meta-Analysis of Gestational Weight Gain Recommendations and Related Outcomes in Brazil. Clinics 2015, 70, 758–764. [Google Scholar] [CrossRef]
- Stotland, N.E.; Cheng, Y.W.; Hopkins, L.M.; Caughey, A.B. Gestational Weight Gain and Adverse Neonatal Outcome Among Term Infants. Obstet. Gynecol. 2006, 108, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.R.; Hofferth, S.L. The Association Between Inadequate Gestational Weight Gain and Infant Mortality Among, U.S. Infants Born in 2002. Matern. Child Health J. 2012, 16, 119–124. [Google Scholar] [CrossRef]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain With Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef] [PubMed]
- McDowell, M.; Cain, M.A.; Brumley, J. Excessive Gestational Weight Gain. J. Midwifery Women’s Health 2019, 64, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodnar, L.M.; Siega-Riz, A.M.; Simhan, H.N.; Himes, K.P.; Abrams, B. Severe Obesity, Gestational Weight Gain, and Adverse Birth Outcomes. Am. J. Clin. Nutr. 2010, 91, 1642–1648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oken, E.; Taveras, E.M.; Kleinman, K.P.; Rich-Edwards, J.W.; Gillman, M.W. Gestational Weight Gain and Child Adiposity at Age 3 Years. Am. J. Obstet. Gynecol. 2007, 196, 322-e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, C.; Rogers, J.; Desai, M.; Ross, M.G. Fetal Programming of Adult Disease. Obstet. Gynecol. 2011, 117, 978–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vesco, K.K.; Sharma, A.J.; Dietz, P.M.; Rizzo, J.H.; Callaghan, W.M.; England, L.; Bruce, F.C.; Bachman, D.J.M.S.; Stevens, V.J.; Hornbrook, M.C. Newborn Size Among Obese Women With Weight Gain Outside the 2009 Institute of Medicine Recommendation. Obstet. Gynecol. 2011, 117, 812–818. [Google Scholar] [CrossRef]
- Lindberg, S.; Anderson, C.; Pillai, P.; Tandias, A.; Arndt, B.; Hanrahan, L. Prevalence and Predictors of Unhealthy Weight Gain in Pregnancy. WMJ 2016, 115, 233–237. [Google Scholar]
- Champion, M.L.; Harper, L.M. Gestational Weight Gain: Update on Outcomes and Interventions. Curr. Diabetes Rep. 2020, 20, 11. [Google Scholar] [CrossRef]
- Tielemans, M.J.; Garcia, A.H.; Peralta Santos, A.; Bramer, W.M.; Luksa, N.; Luvizotto, M.J.; Moreira, E.; Topi, G.; de Jonge, E.A.; Visser, T.L.; et al. Macronutrient Composition and Gestational Weight Gain: A Systematic Review. Am. J. Clin. Nutr. 2016, 103, 83–99. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B. Dietary Pattern Analysis: A New Direction in Nutritional Epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Englund-Ögge, L.; Brantsæter, A.L.; Sengpiel, V.; Haugen, M.; Birgisdottir, B.E.; Myhre, R.; Jacobsson, B. Maternal Dietary Patterns and Preterm Delivery: Results From a Large Prospective Cohort Study. BMJ 2014, 348, g1446. [Google Scholar] [CrossRef] [PubMed]
- Ancira-Moreno, M.; Vadillo-Ortega, F.; Rivera-Dommarco, J.Á.; Sánchez, B.N.; Pasteris, J.; Batis, C.; Castillo-Castrejón, M.; O’Neill, M.S. Gestational weight gain trajectories over pregnancy and their association with maternal diet quality: Results from the PRINCESA cohort. Nutrition 2019, 65, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Barchitta, M.; Favara, G.; La Rosa, M.C.; La Mastra, C.; Magnano San Lio, R.; Agodi, A. Maternal Dietary Patterns Are Associated with Pre-Pregnancy Body Mass Index and Gestational Weight Gain: Results from the “Mamma & Bambino” Cohort. Nutrients 2019, 11, 1308. [Google Scholar] [CrossRef] [Green Version]
- Pires, I.G.; Gonçalves, D.R. Consumo alimentar e ganho de peso de gestantes assistidas em unidades básicas de saúde. Braz. J. Health Rev. 2021, 4, 128–146. [Google Scholar] [CrossRef]
- dos Santos Araújo, E.; da Mota Santana, J.; Brito, S.M.; dos Santos, D.B. Consumo alimentar de gestantes atendidas em Unidades de Saúde. O Mundo Saúde 2016, 40, 28–37. [Google Scholar] [CrossRef]
- Hettfleisch, K.; Bernardes, L.S.; Carvalho, M.A.; Pastro, L.D.; Vieira, S.E.; Saldiva, S.R.; Saldiva, P.; Francisco, R.P. Short-term exposure to urban air pollution and influences on placental vascularization indexes. Environ. Health Perspect. 2017, 125, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, M.A.; Hettfleisch, K.; Rodrigues, A.S.; Benachi, A.; Vieira, S.E.; Saldiva, S.R.; Saldiva, P.H.; Francisco, R.P.; Bernardes, L.S. Association between exposure to air pollution during intrauterine life and cephalic circumference of the newborn. Environ. Sci. Pollut. Res. 2021, 28, 9701–9711. [Google Scholar] [CrossRef]
- Lohman, G.T.; Roche, F.A.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- WHO. Anthro Plus for Personal Computers Manual: Software For Assessing Growth of the World’s Children and Adolescents; WHO: Geneva, Switzerland, 2009; Available online: http://www.who.int/growthref/tools/en/ (accessed on 23 November 2021).
- Gilmore, L.A.; Redman, L.M. Weight Gain in Pregnancy and Application of the 2009 IOM Guidelines: Toward a Uniform Approach. Obesity 2015, 23, 507–511. [Google Scholar] [CrossRef] [Green Version]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method Reduces Bias in the Collection of Energy Intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, A.B.V.; Lacerda, E.M.A.; Benzecry, E.H.; Gomes, M.C.; Costa., V.M. Tabela Para Avaliação de Consumo em Medidas Caseiras, 4th ed.; Atheneu: São Paulo, Brazil, 2001. [Google Scholar]
- Fisberg, R.M.; Villar, B.S. Manual de receitas e medidas caseiras para cálculo de inquéritos alimentares: Manual elaborado para auxiliar o processamento de dados de inquéritos alimentares. In Manual de Receitas e Medidas Caseiras Para Cálculo de Inquéritos Alimentares: Manual Elaborado Para Auxiliar o Processamento de Dados de Inquéritos Alimentares; USP/FSP/HNT: São Paulo, Brazil, 2002. [Google Scholar]
- Nutrition Coordinating Center: Division of Epidemiology Nutrition Data System (NDS). Nutrition Data System for Research (NDS-R); University of Minnesota: Minneapolis, MN, USA, 1998. [Google Scholar]
- Harttig, U.; Haubrock, J.; Knüppel, S.; Boeing, H. The MSM program: Web-Based Statistics Package for Estimating Usual Dietary Intake Using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Análise Multivariada de Dados; Bookman Editora: Porto Alegre, Brazil, 2009. [Google Scholar]
- Restall, A.; Taylor, R.S.; Thompson, J.; Flower, D.; Dekker, G.A.; Kenny, L.C.; Poston, L.; McCowan, L.M. Risk Factors for Excessive Gestational Weight Gain in a Healthy, Nulliparous Cohort. J. Obes. 2014, 2014, 148391. [Google Scholar] [CrossRef] [PubMed]
- da Mota Santana, J.; de Oliveira Queiroz, V.A.; Brito, S.M.; Dos Santos, D.B.; Assis, A.M.O. Food Consumption Patterns During Pregnancy: A Longitudinal Study in a Region of the North East of Brazil. Nutr. Hosp. 2015, 32, 130–138. [Google Scholar] [PubMed]
- McGowan, C.A.; McAuliffe, F.M. Maternal Dietary Patterns and Associated Nutrient Intakes During Each Trimester of Pregnancy. Public Health Nutr. 2013, 16, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- [Recurso Eletrônico]; Ministério da Saúde: Brasilia—DF. Brazil. 2021. ISBN 978-65-5993-088-3. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/protocolos_guia_alimentar_fasciculo3.pdf (accessed on 21 December 2021).
- Cutler, G.J.; Flood, A.; Hannan, P.; Neumark-Sztainer, D. Major Patterns of Dietary Intake in Adolescents and Their Stability Over Time. J. Nutr. 2009, 139, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Neumann, A.I.; Martins, I.S.; Marcopito, L.F.; Araujo, E.A. Dietary patterns associated with risk factors for cardiovascular disease in a Brazilian city. Rev. Panam. Salud Publica 2007, 22, 329–339. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, J.A.; Hoffman, D.J.; Castro, T.G.; Saldiva, S.R.D.M.; Francisco, R.P.V.; Vieira, S.E.; Marchioni, D.M. Pre-Pregnancy Dietary Pattern is Associated With Newborn Size: Results From ProcriAr Study. Br. J. Nutr. 2021, 126, 903–912. [Google Scholar] [CrossRef]
- Lenders, C.M.; McElrath, T.F.; Scholl, T.O. Nutrition in Adolescent Pregnancy. Curr. Opin. Pediatr. 2000, 12, 291–296. [Google Scholar] [CrossRef]
- Lenz, A.; Olinto, M.T.; Dias-da-Costa, J.S.; Alves, A.L.; Balbinotti, M.; Pattussi, M.P.; Bassani, D.G. Socioeconomic, Demographic and Lifestyle Factors Associated With Dietary Patterns of Women Living in Southern Brazil. Cad. Saude Publica 2009, 25, 1297–1306. [Google Scholar] [CrossRef] [Green Version]
- Sturmer, J.; Franken, D.L.; Ternus, D.L.; Henn, R.L.; Dias-da-Costa, J.S.; Olinto, M.T.A.; Paniz, V.M.V. Dietary Pattern as a Predictor of Multimorbidity Patterns: A Population-Based Cross-Sectional Study With Women. Clin. Nutr. ESPEN 2022, 51, 452–460. [Google Scholar] [CrossRef]
- Wrottesley, S.V.; Pisa, P.T.; Norris, S.A. The Influence of Maternal Dietary Patterns on Body Mass Index and Gestational Weight Gain in Urban Black South African Women. Nutrients 2017, 9, 732. [Google Scholar] [CrossRef] [Green Version]
- Renée, L.; Eason, E.; Melzack, R. Nausea and vomiting during pregnancy: A prospective study of its frequency, intensity, and patterns of change. Am. J. Obstet. Gynecol. 2000, 182, 931–937. [Google Scholar]
- Le, Y.T.; Luu, M.N.; Mai, L.H.; Hoang, A.T.; Nguyen, T.T.; Quach, D.T. Prevalence and characteristics of gastroesophageal reflux disease in pregnant women. Rev. Gastroenterol. México 2022. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- DiPietro, J.A.; Millet, S.; Costigan, K.A.; Gurewitsch, E.; Caulfield, L.E. Psychosocial influences on weight gain attitudes and behaviors during pregnancy. J. Am. Diet. Assoc. 2003, 103, 1314–1319. [Google Scholar] [CrossRef]


{kind=link}
| Maternal Characteristics | No EGWG (%) | EGWG (%) | p-Value |
|---|---|---|---|
| 189(49.1) | 196(50.9) | ||
| Age at enrollment (y) a | 0.150 | ||
| <19 | 32(55.2) | 26(44.8) | |
| 19–34.9 | 135(46.4) | 156(53.6) | |
| ≥35 | 22(61.1) | 14(38.9) | |
| White Skin Color b | 0.778 | ||
| Yes | 74(50)) | 74(50) | |
| No | 115(48.5) | 122(51.5) | |
| Years of schooling b | 0.175 | ||
| <8 y | 95(52.8) | 85(47.2) | |
| ≥8 y | 94(45.8) | 111(54.2) | |
| Income b | 0.182 | ||
| ≤1 Basic wage | 30(57.7) | 22(42.3) | |
| >1 Basic wage | 159(47.8) | 174(52.2) | |
| Parity b | 0.590 | ||
| Primiparous | 91(50.6) | 89(49.4) | |
| Multiparous | 98(47.8) | 107(52.2) | |
| Marital status b | 0.051 | ||
| Single or divorced | 87(55.1) | 71(45.2) | |
| Married/partnered | 102(44.9) | 125(55.1) | |
| Physical activity b | 0.226 | ||
| No | 162(50.5) | 159(49.5) | |
| Yes | 27(42.2) | 37(57.8) | |
| Currently smoking b | 0.077 | ||
| No | 119(45.9) | 140(54.1) | |
| Yes/ex-smoking | 70(55.6) | 56(44.4) | |
| BMI categories a | <0.01 | ||
| <18.5 kg/m2 | 9(64.3) | 5(35.7) | |
| 18.5–24.9 kg/m2 | 112(58.1) | 81(41.9) | |
| 25.0–29.9 kg/m2 | 34(31.5) | 74(68.5) | |
| ≥30 kg/m2 | 34(48.6) | 36(51.4) | |
| Gestational Age in each trimester a | |||
| First, mean (SE) | 12.3 ± 0.06 | 12.4 ± 0.06 | 0.823 |
| Second, mean (SE) | 21.7 ± 0.07 | 21.6 ± 0.06 | 0.724 |
| Third, mean (SE) | 31.7 ± 0.07 | 31.8 ± 0.07 | 0.465 |
| Food Group | Vegetables and Fruits | Western | Traditional |
|---|---|---|---|
| Vegetables | 0.7520 | −0.1438 | 0.0616 |
| Oil and salad dressing | 0.6764 | 0.0841 | 0.2852 |
| Fruits | 0.5037 | −0.1020 | −0.1347 |
| Sweetened juices | 0.4320 | 0.0945 | −0.1136 |
| Salt | 0.4149 | 0.1366 | 0.1774 |
| Vinaigrette | 0.3685 | 0.1246 | 0.4032 |
| Unsweetened juices | 0.3152 | −0.0278 | −0.1238 |
| French bread | −0.2973 | 0.1165 | 0.4346 |
| Butter and Margarine | −0.2826 | −0.0352 | 0.4305 |
| Milk fat-reduced | 0.2722 | −0.0269 | −0.2680 |
| Lean meats | 0.2441 | −0.1395 | 0.1032 |
| Fruit smoothies and soy beverage | 0.2006 | −0.0021 | −0.1760 |
| White rice | 0.1991 | 0.0669 | 0.6856 |
| Crackers | 0.1813 | −0.1294 | −0.0731 |
| Sweetened tea | 0.1650 | −0.1273 | −0.1767 |
| Whole milk and yogurts | 0.1505 | 0.0075 | −0.1952 |
| Beans and lentils | 0.1480 | −0.1531 | 0.6758 |
| Mozzarella cheese | 0.1436 | 0.1777 | −0.0330 |
| Cereals and farofa | −0.1394 | −0.0001 | −0.1937 |
| Pork and frankfurters | 0.1393 | 0.4079 | 0.2532 |
| Soft drinks | −0.1185 | 0.6941 | 0.1113 |
| Wheat bread and brown rice | 0.1135 | −0.1457 | −0.2592 |
| Pasta | 0.1042 | 0.1802 | −0.1113 |
| Condiments | −0.1013 | 0.3320 | −0.0476 |
| Sweetened coffee | −0.0882 | −0.4299 | 0.2607 |
| Desserts and sweets | 0.0486 | 0.5700 | −0.0923 |
| Processed meat and snacks | −0.0336 | 0.6481 | −0.0620 |
| Fried beef, chicken, and eggs | 0.0332 | 0.0849 | 0.3496 |
| Potato and cassava boiled | 0.0286 | 0.1952 | 0.1108 |
| Chocolate powder | −0.0226 | 0.3654 | −0.2334 |
| Cookies and cakes | −0.0132 | 0.4723 | 0.0638 |
| Eigenvalue | 2.47 | 2.35 | 2.28 |
| Explained variance (%) | 7.99 | 7.59 | 7.39 |
| Mothers’ Characteristics | Set of R24h | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Vegetables/Fruits | Western | Traditional | |||||||
| Mean | SE | p | Mean | SE | p | Mean | SE | p | |
| Age a | 0.007 | <0.001 | 0.002 | ||||||
| < 19 years | −0.332 | 0.124 | 0.475 | 0.127 | 0.383 | 0.127 | |||
| 19 a 35 years | 0.044 | 0.060 | −0.044 | 0.057 | −0.051 | 0.059 | |||
| > 35 years | 0.172 | 0.117 | −0.407 | 0.148 | −0.206 | 0.148 | |||
| White Skin Color b | 0.632 | 0.145 | 0.041 | ||||||
| Yes | 0.018 | 0.077 | 0.114 | 0.089 | −0.159 | 0.082 | |||
| No | −0.012 | 0.067 | −0.071 | 0.061 | 0.099 | 0.064 | |||
| Schooling b | 0.054 | 0.603 | 0.003 | ||||||
| < 8 years | −0.123 | 0.073 | −0.028 | 0.076 | 0.134 | 0.067 | |||
| ≥ 8 years | 0.108 | 0.073 | 0.026 | 0.069 | −0.118 | 0.074 | |||
| Marital Status b | 0.095 | 0.001 | 0.004 | ||||||
| Single or divorced | −0.097 | 0.074 | 0.194 | 0.077 | 0.155 | 0.082 | |||
| Married /partnered | 0.067 | 0.069 | −0.135 | 0.066 | −0.108 | 0.064 | |||
| Income b | 0.427 | 0.141 | 0.940 | ||||||
| <1 Basic wage | −0.124 | 0.128 | −0.153 | 0.143 | 0.096 | 0.162 | |||
| ≥1 Basic wage | 0.019 | 0.055 | 0.024 | 0.054 | −0.001 | 0.053 | |||
| Primiparous b | 0.068 | <0.001 | 0.599 | ||||||
| No | 0.078 | 0.071 | −0.179 | 0.068 | 0.009 | 0.074 | |||
| Yes | −0.088 | 0.072 | 0.204 | 0.074 | −0.008 | 0.075 | |||
| Practice physical activity b | 0.048 | 0.858 | 0.293 | ||||||
| No | −0.043 | 0.055 | −0.002 | 0.057 | 0.023 | 0.054 | |||
| Yes | 0.218 | 0.125 | 0.009 | 0.114 | −0.115 | 0.143 | |||
| Smoking b | 0.426 | 0.186 | 0.041 | ||||||
| No | 0.036 | 0.060 | −0.057 | 0.059 | −0.072 | 0.060 | |||
| Yes | −0.076 | 0.094 | 0.117 | 0.096 | 0.149 | 0.092 | |||
| BMI at 1st trimester a | 0.542 | 0.021 | 0.013 | ||||||
| <18.5 kg/m² | −0.092 | 0.271 | 0.155 | 0.308 | 0.267 | 0.226 | |||
| 18.5–24.9 kg/m² | −0.044 | 0.069 | 0.131 | 0.070 | 0.121 | 0.075 | |||
| 25.0–29.9 kg/m² | 0.098 | 0.098 | −0.141 | 0.102 | −0.086 | 0.088 | |||
| ≥ 30.0 kg/m² | −0.012 | 0.127 | −0.175 | 0.107 | −0.253 | 0.116 | |||
| Excessive weight gain b | 0.328 | 0.869 | 0.249 | ||||||
| No | −0.052 | 0.069 | −0.013 | 0.069 | 0.075 | 0.075 | |||
| Yes | 0.051 | 0.074 | 0.013 | 0.074 | −0.072 | 0.069 | |||
| Excessive Weight Gain | β (SE) | OR | p | L95%CI | H95%CI |
|---|---|---|---|---|---|
| Brazilian Traditional | −0.192 (0.10) | 0.83 | 0.044 | 0.69 | 0.99 |
| Daily caloric intake (kcal) | 0.0004 (0.0001) | 1.00 | 0.010 | 1.00 | 1.00 |
| Underweight/normal weight | 1 | ||||
| Overweight at baseline | 0.627 (0.27) | 1.87 | 0.022 | 1.10 | 3.20 |
| Obese at baseline | −0.112 (0.32) | 0.89 | 0.728 | 0.48 | 1.68 |
| Age < 19 years | −0.671 (0.41) | 0.51 | 0.103 | 0.23 | 1.15 |
| Age 19−34.9 years | 1 | ||||
| Age ≥ 35 years | −0.704 (0.33) | 0.49 | 0.034 | 0.26 | 0.95 |
| Non-smoking | 1 | ||||
| Smoking | −0.917 (0.36) | 0.32 | 0.010 | 0.20 | 0.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saldiva, S.R.D.M.; De Arruda Neta, A.d.C.P.; Teixeira, J.A.; Peres, S.V.; Marchioni, D.M.L.; Carvalho, M.A.; Vieira, S.E.; Francisco, R.P.V. Dietary Pattern Influences Gestational Weight Gain: Results from the ProcriAr Cohort Study—São Paulo, Brazil. Nutrients 2022, 14, 4428. https://doi.org/10.3390/nu14204428
Saldiva SRDM, De Arruda Neta AdCP, Teixeira JA, Peres SV, Marchioni DML, Carvalho MA, Vieira SE, Francisco RPV. Dietary Pattern Influences Gestational Weight Gain: Results from the ProcriAr Cohort Study—São Paulo, Brazil. Nutrients. 2022; 14(20):4428. https://doi.org/10.3390/nu14204428
Chicago/Turabian StyleSaldiva, Silvia Regina Dias Medici, Adélia da Costa Pereira De Arruda Neta, Juliana Araujo Teixeira, Stela Verzinhasse Peres, Dirce Maria Lobo Marchioni, Mariana Azevedo Carvalho, Sandra Elisabete Vieira, and Rossana Pulcineli Vieira Francisco. 2022. "Dietary Pattern Influences Gestational Weight Gain: Results from the ProcriAr Cohort Study—São Paulo, Brazil" Nutrients 14, no. 20: 4428. https://doi.org/10.3390/nu14204428