

Alternative Healthy Eating Index-2010 and Incident Non-Communicable Diseases: Findings from a 15-Year Follow Up of Women from the 1973–78 Cohort of the Australian Longitudinal Study on Women’s Health

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
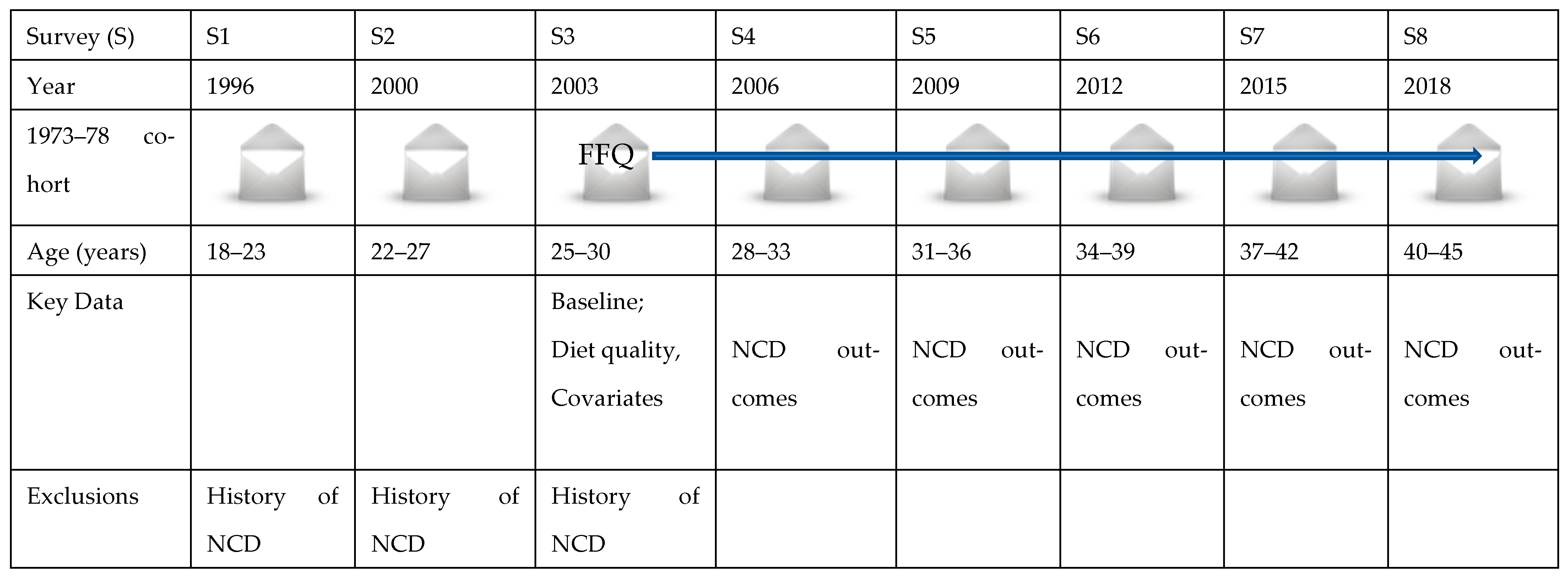
2.1. Study Population
2.2. Dietary Intake Assessment
2.3. Exposure Variable
2.4. Outcome Variables
2.5. Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- World Health Organization. Global Health Estimates 2020: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2019. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed on 9 August 2021).
- World Health Organization. World Health Statistics 2021: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-002705-3.
- Afshar, S.; Roderick, P.J.; Kowal, P.; Dimitrov, B.D.; Hill, A.G. Multimorbidity and the inequalities of global ageing: A cross-sectional study of 28 countries using the World Health Surveys. BMC Public Health 2015, 15, 776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCD Alliance. Non-Communicable Diseases: A Priortity for Women’s Health and Development; The NCD Alliance: Geneva, Switzerland, 2011. [Google Scholar]
- Taskforce on Women and NCDs. Women and Non-Communicable Diseases: A Call to Action. Available online: https://ncdalliance.org/sites/default/files/resource_files/Women%20and%20NCDs%20infographic_WEB_fv.pdf (accessed on 11 November 2021).
- Canoy, D.; Cairns, B.J.; Balkwill, A.; Wright, F.L.; Khalil, A.; Beral, V.; Green, J.; Reeves, G.; Collaborators, M.W.S. Hypertension in pregnancy and risk of coronary heart disease and stroke: A prospective study in a large UK cohort. Int. J. Cardiol. 2016, 222, 1012–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veerbeek, J.H.; Hermes, W.; Breimer, A.Y.; Van Rijn, B.B.; Koenen, S.V.; Mol, B.W.; Franx, A.; De Groot, C.J.; Koster, M.P. Cardiovascular disease risk factors after early-onset preeclampsia, late-onset preeclampsia, and pregnancy-induced hypertension. Hypertension 2015, 65, 600–606. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Wei, T.; Ni, W.; Zhang, A.; Zhang, J.; Xing, Y.; Xing, Q. Incidence and risk factors of gestational diabetes mellitus: A prospective cohort study in Qingdao, China. Front. Endocrinol. 2020, 11, 636. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.C.; Crilly, M.; Black, C.; Prescott, G.J.; Mercer, S.W. Defining and measuring multimorbidity: A systematic review of systematic reviews. Eur. J. Public Health 2019, 29, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Le Reste, J.Y.; Nabbe, P.; Manceau, B.; Lygidakis, C.; Doerr, C.; Lingner, H.; Czachowski, S.; Munoz, M.; Argyriadou, S.; Claveria, A. The European General Practice Research Network presents a comprehensive definition of multimorbidity in family medicine and long term care, following a systematic review of relevant literature. J. Am. Med. Dir. Assoc. 2013, 14, 319–325. [Google Scholar] [CrossRef]
- Harris, M.L.; Egan, N.; Forder, P.M.; Loxton, D. Increased chronic disease prevalence among the younger generation: Findings from a population-based data linkage study to inform chronic disease ascertainment among reproductive-aged Australian women. PLoS ONE 2021, 16, e0254668. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. The Health of Australia’s Females. Available online: https://www.aihw.gov.au/reports/men-women/female-health/contents/who-are (accessed on 31 August 2021).
- World Health Organization. Gender and Noncommunicable Diseases in Europe: Analysis of STEPS Data; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2020.
- Park, K. Park’s Textbook of Preventive and Social Medicine, 23rd ed.; Banarsidas Bhanot: Madhya Pradesh, India, 2015. [Google Scholar]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition, Physical Activity and Colorectal Cancer; World Cancer Research Fund International: London, UK, 2018; ISBN 978-1-912259-00-7. [Google Scholar]
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Waijers, P.M.C.M.; Feskens, E.J.M.; Ocke, M.C. A critical review of predefined diet quality scores. Br. J. Nutr. 2007, 97, 219–231. [Google Scholar] [CrossRef] [Green Version]
- Arvaniti, F.; Panagiotakos, D.B. Healthy indexes in public health practice and research: A review. Crit. Rev. Food Sci. Nutr. 2008, 48, 317–327. [Google Scholar] [CrossRef]
- Wirt, A.; Collins, C.E. Diet quality—What is it and does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Kourlaba, G.; Panagiotakos, D.B. Dietary quality indices and human health: A review. Maturitas 2009, 62, 1–8. [Google Scholar] [CrossRef]
- Hodge, A.; Bassett, J. What can we learn from dietary pattern analysis? Public Health Nutr. 2016, 19, 191–194. [Google Scholar] [CrossRef] [Green Version]
- Gerber, M. The comprehensive approach to diet: A critical review. J. Nutr. 2001, 131, 3051S–3055S. [Google Scholar] [CrossRef] [Green Version]
- Thorpe, M.G.; Kestin, M.; Riddell, L.J.; Keast, R.S.; McNaughton, S.A. Diet quality in young adults and its association with food-related behaviours. Public Health Nutr. 2013, 17, 1767–1775. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, T.E.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Patterson, R.E.; Haines, P.S.; Popkin, B.M. Diet quality index: Capturing a multidimensional behavior. J. Am. Diet. Assoc. 1994, 94, 57–64. [Google Scholar] [CrossRef]
- Haines, P.S.; Siega-Riz, A.M.; Popkin, B.M. The Diet Quality Index Revised: A measurement instrument for populations. J. Am. Diet. Assoc. 1999, 99, 697–704. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNaughton, S.A.; Ball, K.; Crawford, D.; Mishra, G.D. An index of diet and eating patterns is a valid measure of diet quality in an Australian population. J. Nutr. 2008, 138, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Siega-Riz, A.M.; Gordon-Larsen, P.; Cai, J.; Adair, L.S.; Zhang, B.; Popkin, B.M. Diet quality and its association with type 2 diabetes and major cardiometabolic risk factors among adults in China. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 987–1001. [Google Scholar] [CrossRef]
- Wong, J.E.; Haszard, J.J.; Howe, A.S.; Parnell, W.R.; Skidmore, P.M.L. Development of a Healthy Dietary Habits Index for New Zealand adults. Nutrients 2017, 9, 454. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Feskanich, D.; Stampfer, M.J.; Giovannucci, E.L.; Rimm, E.B.; Hu, F.B.; Spiegelman, D.; Hunter, D.J.; Colditz, G.A.; Willett, W.C. Diet quality and major chronic disease risk in men and women: Moving toward improved dietary guidance. Am. J. Clin. Nutr. 2002, 76, 1261–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, C.E.; Young, A.F.; Hodge, A. Diet quality is associated with higher nutrient intake and self-rated health in mid-aged women. J. Am. Coll. Nutr. 2008, 27, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Song, X.; Chen, G.-C.; Neelakantan, N.; van Dam, R.M.; Feng, L.; Yuan, J.-M.; Pan, A.; Koh, W.-P. Dietary pattern in midlife and cognitive impairment in late life: A prospective study in Chinese adults. Am. J. Clin. Nutr. 2019, 110, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M. Development of the Healthy Eating Index-2005. J. Am. Diet. Assoc. 2008, 108, 1896–1901. [Google Scholar] [CrossRef]
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the Healthy Eating Index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef] [Green Version]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- Reedy, J.; Lerman, J.; Herrick, K.; Shams-White, M.; Zimmer, M.; Mathieu, K.M.; Dodd, K.; Kahle, L.; Stoody, E.; Pannucci, T. Measuring Diet Quality Across the Lifespan: Introducing the New Healthy Eating Index-Toddlers-2020 and Healthy Eating Index-2020. Curr. Dev. Nutr. 2022, 6, 392. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morze, J.; Danielewicz, A.; Hoffmann, G.; Schwingshackl, L. Diet quality as assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and health outcomes: A second update of a systematic review and meta-analysis of cohort studies. J. Acad. Nutr. Diet. 2020, 120, 1998–2031.e1915. [Google Scholar] [CrossRef] [PubMed]
- Morze, J.; Danielewicz, A.; Przybyłowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur. J. Nutr. 2021, 60, 1561–1586. [Google Scholar] [CrossRef] [PubMed]
- Martín-Peláez, S.; Fito, M.; Castaner, O. Mediterranean diet effects on type 2 diabetes prevention, disease progression, and related mechanisms. a review. Nutrients 2020, 12, 2236. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean diet and cardiovascular health: A critical review. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Cowell, O.R.; Mistry, N.; Deighton, K.; Matu, J.; Griffiths, A.; Minihane, A.M.; Mathers, J.C.; Shannon, O.M.; Siervo, M. Effects of a Mediterranean diet on blood pressure: A systematic review and meta-analysis of randomized controlled trials and observational studies. J. Hypertens. 2021, 39, 729–739. [Google Scholar] [CrossRef]
- Shafiei, F.; Salari-Moghaddam, A.; Larijani, B.; Esmaillzadeh, A. Adherence to the Mediterranean diet and risk of depression: A systematic review and updated meta-analysis of observational studies. Nutr. Rev. 2019, 77, 230–239. [Google Scholar] [CrossRef]
- Soltani, S.; Jayedi, A.; Shab-Bidar, S.; Becerra-Tomás, N.; Salas-Salvadó, J. Adherence to the Mediterranean diet in relation to all-cause mortality: A systematic review and dose-response meta-analysis of prospective cohort studies. Adv. Nutr. 2019, 10, 1029–1039. [Google Scholar] [CrossRef]
- Altun, A.; Brown, H.; Szoeke, C.; Goodwill, A.M. The Mediterranean dietary pattern and depression risk: A systematic review. Neurol. Psychiatry Brain Res. 2019, 33, 1–10. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Fayosse, A.; Sabia, S.; Tabak, A.; Shipley, M.; Dugravot, A.; Kivimäki, M. Clinical, socioeconomic, and behavioural factors at age 50 years and risk of cardiometabolic multimorbidity and mortality: A cohort study. PLoS Med. 2018, 15, e1002571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hlaing-Hlaing, H.; Dolja-Gore, X.; Tavener, M.; James, E.L.; Hodge, A.M.; Hure, A.J. Diet quality and Incident non-communicable disease in the 1946–1951 cohort of the Australian Longitudinal Study on Women’s Health. Int. J. Environ. Res. Public Health 2021, 18, 11375. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, B.; Williams, J.; Rakovac, I.; Wickramasinghe, K.; Hennis, A.; Shin, H.-R.; Farmer, M.; Weber, M.; Berdzuli, N.; Borges, C. Life course approach to prevention and control of non-communicable diseases. BMJ 2019, 364, l257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Minsk Declaration: The Life-Course Approach in the Context of Health 2020; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2015.
- Smith, K.J.; McNaughton, S.A.; Gall, S.L.; Otahal, P.; Dwyer, T.; Venn, A.J. Associations between partnering and parenting transitions and dietary habits in young adults. J. Acad. Nutr. Diet. 2017, 117, 1210–1221. [Google Scholar] [CrossRef]
- Ball, K.; Jeffery, R.W.; Abbott, G.; McNaughton, S.A.; Crawford, D. Is healthy behavior contagious: Associations of social norms with physical activity and healthy eating. Int. J. Behav. Nutr. Phys. Act 2010, 7, 86. [Google Scholar] [CrossRef] [Green Version]
- Elstgeest, L.E.; Mishra, G.D.; Dobson, A.J. Transitions in living arrangements are associated with changes in dietary patterns in young women. J. Nutr. 2012, 142, 1561–1567. [Google Scholar] [CrossRef] [Green Version]
- Olson, C.M. Tracking of food choices across the transition to motherhood. J. Nutr. Educ. Behav. 2005, 37, 129–136. [Google Scholar] [CrossRef]
- Laroche, H.H.; Wallace, R.B.; Snetselaar, L.; Hillis, S.L.; Steffen, L.M. Changes in diet behavior when adults become parents. J. Acad. Nutr. Diet. 2012, 112, 832–839. [Google Scholar] [CrossRef] [Green Version]
- Berge, J.M.; Larson, N.; Bauer, K.W.; Neumark-Sztainer, D. Are parents of young children practicing healthy nutrition and physical activity behaviors? Pediatrics 2011, 127, 881–887. [Google Scholar] [CrossRef] [Green Version]
- Pegington, M.; French, D.P.; Harvie, M.N. Why young women gain weight: A narrative review of influencing factors and possible solutions. Obes. Rev. 2020, 21, e13002. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P. Obesity and cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef] [PubMed]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body fatness and cancer—viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [Green Version]
- Rowley, W.R.; Bezold, C.; Arikan, Y.; Byrne, E.; Krohe, S. Diabetes 2030: Insights from yesterday, today, and future trends. Popul. Health Manag. 2017, 20, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Institute of Health and Welfare. Australia’s Health 2020: In Brief; Australian Institute of Health and Welfare: Canberra, Australia, 2020; ISBN 978-1-76054-691-5. [Google Scholar]
- Dobson, A.J.; Hockey, R.; Brown, W.J.; Byles, J.E.; Loxton, D.J.; McLaughlin, D.P.; Tooth, L.R.; Mishr, G.D. Cohort profile update: Australian Longitudinal Study on Women’s Health. Int. J. Epidemiol. 2015, 44, 1547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loxton, D.; Tooth, L.; Harris, M.L.; Forder, P.M.; Dobson, A.; Powers, J.; Brown, W.; Byles, J.; Mishra, G. Cohort profile: The Australian longitudinal study on Women’s health (ALSWH) 1989–1995 cohort. Int. J. Epidemiol. 2018, 47, 391–392e. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, W.J.; Dobson, A.J.; Team, A.R. The Australian Longitudinal Study on Women’s Health: Study design and sample. N. S. W. Public Health Bull. 2000, 11, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Ireland, P.; Jolley, D.; Giles, G.; O’Dea, K.; Powles, J.; Rutishauser, I.; Wahlqvist, M.L.; Williams, J. Development of the Melbourne FFQ: A food frequency questionnaire for use in an Australian prospective study involving an ethnically diverse cohort. Asia Pac. J. Clin. Nutr. 1994, 3, 19–31. [Google Scholar] [PubMed]
- Hodge, A.; Patterson, A.J.; Brown, W.J.; Ireland, P.; Giles, G. The Anti Cancer Council of Victoria FFQ: Relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust. N. Z. J. Public Health 2000, 24, 576–583. [Google Scholar] [CrossRef]
- Lewis, J.; Milligan, G.C.; Hunt, A. Nuttab95: Nutrient Data Table for Use in Australia; Food Standards Australia New Zealand: Barton, Australia, 1995. [Google Scholar]
- Baldwin, J.N.; Forder, P.M.; Haslam, R.L.; Hure, A.J.; Loxton, D.J.; Patterson, A.J.; Collins, C.E. Change in diet quality over 12 years in the 1946–1951 cohort of the Australian Longitudinal Study on Women’s Health. Nutrients 2020, 12, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivappa, N.; Hebert, J.R.; Kivimaki, M.; Akbaraly, T. Alternative Healthy Eating Index 2010, Dietary Inflammatory Index and risk of mortality: Results from the Whitehall II cohort study and meta-analysis of previous Dietary Inflammatory Index and mortality studies. Br. J. Nutr. 2017, 118, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Hlaing-Hlaing, H.; Pezdirc, K.; Tavener, M.; James, E.L.; Hure, A. Diet quality indices used in Australian and New Zealand adults: A systematic review and critical appraisal. Nutrients 2020, 12, 3777. [Google Scholar] [CrossRef] [PubMed]
- Cristina, T.J.N.; Williams, J.A.S.; Parkinson, L.; Sibbritt, D.W.; Byles, J.E. Identification of diabetes, heart disease, hypertension and stroke in mid- and older-aged women: Comparing self-report and administrative hospital data records. Geriatr. Gerontol. Int. 2016, 16, 95–102. [Google Scholar] [CrossRef]
- Stavrou, E.; Vajdic, C.M.; Loxton, D.; Pearson, S.-A. The validity of self-reported cancer diagnoses and factors associated with accurate reporting in a cohort of older Australian women. Cancer Epidemiol. 2011, 35, e75–e80. [Google Scholar] [CrossRef] [PubMed]
- Australian Longitudinal Study on Women’s Health. ALSWH: Linked Data Overview. Available online: https://alswh.org.au/for-data-users/linked-data-overview/national-data/ (accessed on 26 February 2022).
- Hernán, M.A. The C-word: Scientific euphemisms do not improve causal inference from observational data. Am. J. Public Health 2018, 108, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection–a review and recommendations for the practicing statistician. Biom. J. 2018, 60, 431–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenland, S.; Pearl, J.; Robins, J.M. Causal diagrams for epidemiologic research. Epidemiology 1999, 10, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Textor, J.; Hardt, J.; Knüppel, S. DAGitty: A graphical tool for analyzing causal diagrams. Epidemiology 2011, 22, 745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tennant, P.W.; Murray, E.J.; Arnold, K.F.; Berrie, L.; Fox, M.P.; Gadd, S.C.; Harrison, W.J.; Keeble, C.; Ranker, L.R.; Textor, J. Use of directed acyclic graphs (DAGs) to identify confounders in applied health research: Review and recommendations. Int. J. Epidemiol. 2021, 50, 620–632. [Google Scholar] [CrossRef]
- Asghari, G.; Mirmiran, P.; Yuzbashian, E.; Azizi, F. A systematic review of diet quality indices in relation to obesity. Br. J. Nutr. 2017, 117, 1055–1065. [Google Scholar] [CrossRef] [Green Version]
- Peacock, A.S.; Bogossian, F.; McIntyre, H.D.; Wilkinson, S. A review of interventions to prevent type 2 diabetes after gestational diabetes. Women Birth 2014, 27, e7–e15. [Google Scholar] [CrossRef]
- Mongraw-Chaffin, M.L.; Peters, S.A.; Huxley, R.R.; Woodward, M. The sex-specific association between BMI and coronary heart disease: A systematic review and meta-analysis of 95 cohorts with 1 × 2 million participants. Lancet Diabetes Endocrinol. 2015, 3, 437–449. [Google Scholar] [CrossRef] [Green Version]
- Jackson, C.; Herber-Gast, G.-C.; Brown, W. Joint effects of physical activity and BMI on risk of hypertension in women: A longitudinal study. J. Obes. 2014, 2014, 271532. [Google Scholar] [CrossRef] [Green Version]
- Peters, U.; Dixon, A.E.; Forno, E. Obesity and asthma. J. Allergy Clin. Immunol. 2018, 141, 1169–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyrrell, J.; Mulugeta, A.; Wood, A.R.; Zhou, A.; Beaumont, R.N.; Tuke, M.A.; Jones, S.E.; Ruth, K.S.; Yaghootkar, H.; Sharp, S. Using genetics to understand the causal influence of higher BMI on depression. Int. J. Epidemiol. 2019, 48, 834–848. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Douglas, I.; Forbes, H.; dos-Santos-Silva, I.; Leon, D.A.; Smeeth, L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 5.24 million UK adults. Lancet 2014, 384, 755–765. [Google Scholar] [CrossRef] [Green Version]
- Gondek, D.; Bann, D.; Brown, M.; Hamer, M.; Sullivan, A.; Ploubidis, G.B. Prevalence and early-life determinants of mid-life multimorbidity: Evidence from the 1970 British birth cohort. BMC Public Health 2021, 21, 1319. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. The Active Australia Survey: A Guide and Manual for Implementation, Analysis and Reporting; Australian Institute of Health and Welfare: Canberra, Australia, 2003; ISBN 1740242580. [Google Scholar]
- Brown, W.J.; Burton, N.W.; Marshall, A.L.; Miller, Y.D. Reliability and validity of a modified self-administered version of the Active Australia physical activity survey in a sample of mid-age women. Aust. N. Z. J. Public Health 2008, 32, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Dolja-Gore, X.; Graves, A.; Gibson, R.; Wheway, V. ALSWH Data Dictionary Supplement: Section 6 Self-Reported Medications. Available online: https://alswh.org.au/wp-content/uploads/2020/08/DSSSection10Medications.pdf (accessed on 27 January 2022).
- Engels, J.M.; Diehr, P. Imputation of missing longitudinal data: A comparison of methods. J. Clin. Epidemiol. 2003, 56, 968–976. [Google Scholar] [CrossRef]
- Lalonde, T.L.; Wilson, J.R.; Yin, J. GMM logistic regression models for longitudinal data with time-dependent covariates and extended classifications. Stat. Med. 2014, 33, 4756–4769. [Google Scholar] [CrossRef] [PubMed]
- Hu, E.A.; Steffen, L.M.; Coresh, J.; Appel, L.J.; Rebholz, C.M. Adherence to the healthy eating index–2015 and other dietary patterns may reduce risk of cardiovascular disease, cardiovascular mortality, and all-cause mortality. J. Nutr. 2020, 150, 312–321. [Google Scholar] [CrossRef]
- Xu, Z.; Steffen, L.M.; Selvin, E.; Rebholz, C.M. Diet quality, change in diet quality and risk of incident CVD and diabetes. Public Health Nutr. 2020, 23, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Trebuchet, A.; Julia, C.; Fezeu, L.; Touvier, M.; Chaltiel, D.; Hercberg, S.; Galan, P.; Adjibade, M.; Kesse-Guyot, E. Prospective association between several dietary scores and risk of cardiovascular diseases: Is the Mediterranean diet equally associated to cardiovascular diseases compared to National Nutritional Scores? Am. Heart J. 2019, 217, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Cardiovascular Disease. Available online: https://www.aihw.gov.au/reports/heart-stroke-vascular-diseases/cardiovascular-health-compendium/contents/what-is-cardiovascular-disease (accessed on 24 July 2021).
- Wu, P.Y.; Huang, C.L.; Lei, W.S.; Yang, S.H. Alternative health eating index and the Dietary Guidelines from American Diabetes Association both may reduce the risk of cardiovascular disease in type 2 diabetes patients. J. Hum. Nutr. Diet. 2016, 29, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Neelakantan, N.; Naidoo, N.; Koh, W.-P.; Yuan, J.-M.; van Dam, R.M. The Alternative Healthy Eating Index is associated with a lower risk of fatal and nonfatal acute myocardial infarction in a Chinese adult population. J. Nutr. 2016, 146, 1379–1386. [Google Scholar] [CrossRef] [Green Version]
- Al-Ibrahim, A.A.; Jackson, R.T. Healthy Eating Index versus Alternate Healthy Index in relation to diabetes status and health markers in US adults: NHANES 2007–2010. Nutr. J. 2019, 18, 26. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, J.; Gaskin, E.; Ji, C.; Miller, M.A.; Cappuccio, F.P. The effect of plant-based dietary patterns on blood pressure: A systematic review and meta-analysis of controlled intervention trials. J. Hypertens. 2021, 39, 23–37. [Google Scholar] [CrossRef]
- Martini, D.; Godos, J.; Marventano, S.; Tieri, M.; Ghelfi, F.; Titta, L.; Lafranconi, A.; Trigueiro, H.; Gambera, A.; Alonzo, E. Nut and legume consumption and human health: An umbrella review of observational studies. Int. J. Food Sci. Nutr. 2021, 72, 871–878. [Google Scholar] [CrossRef]
- Colussi, G.; Catena, C.; Novello, M.; Bertin, N.; Sechi, L. Impact of omega-3 polyunsaturated fatty acids on vascular function and blood pressure: Relevance for cardiovascular outcomes. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Bédard, A.; Li, Z.; Ait-Hadad, W.; Camargo Jr, C.A.; Leynaert, B.; Pison, C.; Dumas, O.; Varraso, R. The role of nutritional factors in asthma: Challenges and opportunities for epidemiological research. Int. J. Environ. Res. Public Health 2021, 18, 3013. [Google Scholar] [CrossRef]
- Guilleminault, L.; Williams, E.J.; Scott, H.A.; Berthon, B.S.; Jensen, M.; Wood, L.G. Diet and asthma: Is it time to adapt our message? Nutrients 2017, 9, 1227. [Google Scholar] [CrossRef] [PubMed]
- Leynaert, B.; Le Moual, N.; Neukirch, C.; Siroux, V.; Varraso, R. Environmental risk factors for asthma developement. Presse Med. 2019, 48, 262–273. [Google Scholar] [CrossRef] [PubMed]
- Andrianasolo, R.M.; Hercberg, S.; Kesse-Guyot, E.; Druesne-Pecollo, N.; Touvier, M.; Galan, P.; Varraso, R. Association between dietary fibre intake and asthma (symptoms and control): Results from the French national e-cohort NutriNet-Santé. Br. J. Nutr. 2019, 122, 1040–1051. [Google Scholar] [CrossRef] [PubMed]
- Andrianasolo, R.M.; Hercberg, S.; Touvier, M.; Druesne-Pecollo, N.; Adjibade, M.; Kesse-Guyot, E.; Galan, P.; Varraso, R. Association between processed meat intake and asthma symptoms in the French NutriNet-Santé cohort. Eur. J. Nutr. 2020, 59, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Rava, M.; Bédard, A.; Dumas, O.; Garcia-Aymerich, J.; Leynaert, B.; Pison, C.; Le Moual, N.; Romieu, I.; Siroux, V. Cured meat intake is associated with worsening asthma symptoms. Thorax 2017, 72, 206–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeChristopher, L.R.; Tucker, K.L. Excess free fructose, high-fructose corn syrup and adult asthma: The Framingham Offspring Cohort. Br. J. Nutr. 2018, 119, 1157–1167. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Kesse-Guyot, E.; Dumas, O.; Garcia-Aymerich, J.; Leynaert, B.; Pison, C.; Moual, N.L.; Romieu, I.; Siroux, V.; Camargo Jr, C.A.; et al. Longitudinal study of diet quality and change in asthma symptoms in adults, according to smoking status. Br. J. Nutr. 2017, 117, 562–571. [Google Scholar] [CrossRef] [Green Version]
- Andrianasolo, R.M.; Kesse-Guyot, E.; Adjibade, M.; Hercberg, S.; Galan, P.; Varraso, R. Associations between dietary scores with asthma symptoms and asthma control in adults. Eur. Respir. J. 2018, 52, 1702572. [Google Scholar] [CrossRef] [Green Version]
- Varraso, R.; Chiuve, S.E.; Fung, T.T.; Barr, R.G.; Hu, F.B.; Willett, W.C.; Camargo, C.A. Alternate Healthy Eating Index 2010 and risk of chronic obstructive pulmonary disease among US women and men: Prospective study. BMJ 2015, 350, h286. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.-Y.; Jerschow, E.; Forno, E.; Hua, S.; Mossavar-Rahmani, Y.; Perreira, K.M.; Sotres-Alvarez, D.; Afshar, M.; Punjabi, N.M.; Thyagarajan, B. Dietary patterns, asthma, and lung function in the Hispanic Community Health Study/Study of Latinos. Ann. Am. Thorac. Soc. 2020, 17, 293–301. [Google Scholar] [CrossRef]
- Lavalette, C.; Adjibade, M.; Srour, B.; Sellem, L.; Fiolet, T.; Hercberg, S.; Latino-Martel, P.; Fassier, P.; Deschasaux, M.; Kesse-Guyot, E. Cancer-specific and general nutritional scores and cancer risk: Results from the prospective NutriNet-Sante cohort. Cancer Res. 2018, 78, 4427–4435. [Google Scholar] [CrossRef]
- Wirfält, E.; Drake, I.; Wallström, P. What do review papers conclude about food and dietary patterns? Food Nutr. Res. 2013, 57, 20523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, M.L.; Willett, W.C. Evaluating adherence to recommended diets in adults: The Alternate Healthy Eating Index. Public Health Nutr. 2006, 9, 152–157. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, S.; Harmon, B.E.; Boushey, C.J.; Morimoto, Y.; Wilkens, L.R.; Le Marchand, L.; Kröger, J.; Schulze, M.B.; Kolonel, L.N.; Maskarinec, G. A priori-defined diet quality indexes and risk of type 2 diabetes: The Multiethnic Cohort. Diabetologia 2015, 58, 98–112. [Google Scholar] [CrossRef] [Green Version]
- Cespedes, E.M.; Hu, F.B.; Tinker, L.; Rosner, B.; Redline, S.; Garcia, L.; Hingle, M.; Van Horn, L.; Howard, B.V.; Levitan, E.B. Multiple healthful dietary patterns and type 2 diabetes in the Women’s Health Initiative. Am. J. Epidemiol. 2016, 183, 622–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, G.-C.; Koh, W.-P.; Neelakantan, N.; Yuan, J.-M.; Qin, L.-Q.; van Dam, R.M. Diet quality indices and risk of type 2 diabetes mellitus: The Singapore Chinese Health Study. Am. J. Epidemiol. 2018, 187, 2651–2661. [Google Scholar] [CrossRef]
- Rahe, C.; Unrath, M.; Berger, K. Dietary patterns and the risk of depression in adults: A systematic review of observational studies. Eur. J. Nutr. 2014, 53, 997–1013. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lv, M.-R.; Wei, Y.-J.; Sun, L.; Zhang, J.-X.; Zhang, H.-G.; Li, B. Dietary patterns and depression risk: A meta-analysis. Psychiatry Res. 2017, 253, 373–382. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, J.K. Stress, food, and inflammation: Psychoneuroimmunology and nutrition at the cutting edge. Psychosom. Med. 2010, 72, 365. [Google Scholar] [CrossRef] [Green Version]
- Hu, D.; Cheng, L.; Jiang, W. Sugar-sweetened beverages consumption and the risk of depression: A meta-analysis of observational studies. J. Affect. Disord. 2019, 245, 348–355. [Google Scholar] [CrossRef]
- Nucci, D.; Fatigoni, C.; Amerio, A.; Odone, A.; Gianfredi, V. Red and processed meat consumption and risk of depression: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 6686. [Google Scholar] [CrossRef]
- Saneei, P.; Hajishafiee, M.; Keshteli, A.H.; Afshar, H.; Esmaillzadeh, A.; Adibi, P. Adherence to Alternative Healthy Eating Index in relation to depression and anxiety in Iranian adults. Br. J. Nutr. 2016, 116, 335–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Villegas, A.; Henríquez-Sánchez, P.; Ruiz-Canela, M.; Lahortiga, F.; Molero, P.; Toledo, E.; Martínez-González, M.A. A longitudinal analysis of diet quality scores and the risk of incident depression in the SUN Project. BMC Med. 2015, 13, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adjibade, M.; Lemogne, C.; Julia, C.; Hercberg, S.; Galan, P.; Assmann, K.E.; Kesse-Guyot, E. Prospective association between adherence to dietary recommendations and incident depressive symptoms in the French NutriNet-Santé cohort. Br. J. Nutr. 2018, 120, 290–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Z.; Ruel, G.; Dal Grande, E.; Pilkington, R.; Taylor, A.W. Soft drink consumption and multimorbidity among adults. Clin. Nutr. ESPEN 2015, 10, e71–e76. [Google Scholar] [CrossRef]
- Jeong, D.; Kim, J.; Lee, H.; Kim, D.-Y.; Lim, H. Association of cardiometabolic multimorbidity pattern with dietary factors among adults in South Korea. Nutrients 2020, 12, 2730. [Google Scholar] [CrossRef]
- Pereira, B.P.; Bortolotto, C.C.; Tomasi, E.; Gonzalez, M.C.; Gomes, A.P.; Gonçalves, H.; Bielemann, R.M. Food consumption and multimorbidity among non-institutionalized elderly people in Pelotas, 2014: A cross-sectional study. Epidemiol. E Serviços De Saúde 2020, 29, e2019050. [Google Scholar] [CrossRef]
- Ruel, G.; Shi, Z.; Zhen, S.; Zuo, H.; Kröger, E.; Sirois, C.; Lévesque, J.-F.; Taylor, A.W. Association between nutrition and the evolution of multimorbidity: The importance of fruits and vegetables and whole grain products. Clin. Nutr. 2014, 33, 513–520. [Google Scholar] [CrossRef]
- Wikström, K.; Lindström, J.; Harald, K.; Peltonen, M.; Laatikainen, T. Clinical and lifestyle-related risk factors for incident multimorbidity: 10-year follow-up of Finnish population-based cohorts 1982–2012. Eur. J. Intern. Med. 2015, 26, 211–216. [Google Scholar] [CrossRef]
- Dekker, L.H.; de Borst, M.H.; Meems, L.M.; de Boer, R.A.; Bakker, S.J.; Navis, G.J. The association of multimorbidity within cardio-metabolic disease domains with dietary patterns: A cross-sectional study in 129,369 men and women from the Lifelines cohort. PLoS ONE 2019, 14, e0220368. [Google Scholar] [CrossRef] [Green Version]
- Freisling, H.; Viallon, V.; Lennon, H.; Bagnardi, V.; Ricci, C.; Butterworth, A.S.; Sweeting, M.; Muller, D.; Romieu, I.; Bazelle, P. Lifestyle factors and risk of multimorbidity of cancer and cardiometabolic diseases: A multinational cohort study. BMC Med. 2020, 18, 5. [Google Scholar] [CrossRef] [Green Version]
- Kyprianidou, M.; Panagiotakos, D.; Faka, A.; Kambanaros, M.; Makris, K.C.; Christophi, C.A. Adherence to the Mediterranean diet in Cyprus and its relationship to multi-morbidity: An epidemiological study. Public Health Nutr. 2021, 24, 4546–4555. [Google Scholar] [CrossRef] [PubMed]
- Al Ramadhani, R.M.; Nagle, C.M.; Ibiebele, T.I.; Grant, P.; Friedlander, M.; DeFazio, A.; Webb, P.M. Pre-and post-diagnosis diet quality and ovarian cancer survival. Cancer Epidemiol. Biomark. Prev. 2021, 30, 229–232. [Google Scholar] [CrossRef]
- Shang, X.; Scott, D.; Hodge, A.; Khan, B.; Khan, N.; English, D.; Giles, G.G.; Ebeling, P.; Sanders, K. Dietary quality is associated with abdominal aortic calcification: A mean of 18-year longitudinal study in community-dwelling older adults. J. Nutr. Health Aging 2017, 21, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.H.; Conley, M.; Reeves, M.M.; Campbell, K.L.; Kelly, J.T. Evaluating the impact of goal setting on improving diet quality in chronic kidney disease. Front. Nutr. 2021, 8, 627753. [Google Scholar] [CrossRef]
- Hodge, A.M.; Karim, M.N.; Hébert, J.R.; Shivappa, N.; Milne, R.L.; De Courten, B. Diet scores and prediction of general and abdominal obesity in the Melbourne Collaborative Cohort study. Public Health Nutr. 2021, 24, 6157–6168. [Google Scholar] [CrossRef] [PubMed]
- Dugué, P.A.; Hodge, A.M.; Brinkman, M.T.; Bassett, J.K.; Shivappa, N.; Hebert, J.R.; Hopper, J.L.; English, D.R.; Milne, R.L.; Giles, G.G. Association between selected dietary scores and the risk of urothelial cell carcinoma: A prospective cohort study. Int. J. Cancer 2016, 139, 1251–1260. [Google Scholar] [CrossRef] [Green Version]
- Powers, J.; Loxton, D. The impact of attrition in an 11-year prospective longitudinal study of younger women. Ann. Epidemiol. 2010, 20, 318–321. [Google Scholar] [CrossRef]
- Irani, F.; Coquoz, E.; von Wolff, M.; Bitterlich, N.; Stute, P. Awareness of non-communicable diseases in women: A cross-sectional study. Arch. Gynecol. Obstet. 2022, 306, 801–810. [Google Scholar] [CrossRef]
- Bista, B.; Dhungana, R.R.; Chalise, B.; Pandey, A.R. Prevalence and determinants of non-communicable diseases risk factors among reproductive aged women of Nepal: Results from Nepal Demographic Health Survey 2016. PLoS ONE 2020, 15, e0218840. [Google Scholar] [CrossRef] [Green Version]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef]
- Olendzki, B.; Procter-Gray, E.; Magee, M.F.; Youssef, G.; Kane, K.; Churchill, L.; Ockene, J.; Li, W. Racial differences in misclassification of healthy eating based on food frequency questionnaire and 24-hour dietary recalls. J. Nutr. Health Aging 2017, 21, 787–798. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| AHEI-2010 Quintiles | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Q1 (n = 1635) | Q2 (n = 1572) | Q3 (n = 1582) | Q4 (n = 1636) | Q5 (n = 1592) | p-Value § |
| Age (years) [mean (sd)] | 27.5 (1.5) | 27.6 (1.5) | 27.5 (1.5) | 27.6 (1.5) | 27.6 (1.4) | 0.02 ** |
| Marital status [n (%)] | <0.001 ** | |||||
| Never married | 415 (25.5) | 487 (31.1) | 557 (35.3) | 630 (38.6) | 734 (46.3) | |
| Married/de facto | 1141 (70.1) | 1028 (65.6) | 974 (61.7) | 939 (57.5) | 810 (51.1) | |
| Separated/divorced/widowed | 72 (4.4) | 52 (3.3) | 47 (3.0) | 64 (3.9) | 42 (2.6) | |
| Area of residence [n (%)] | <0.001 ** | |||||
| Major cities | 810 (49.6) | 835 (53.2) | 868 (55.0) | 992 (60.7) | 1002 (63.2) | |
| Inner regional | 499 (30.5) | 435 (27.7) | 430 (27.2) | 388 (23.7) | 388 (24.4) | |
| Outer regional/rural | 325 (19.9) | 300 (19.1) | 281 (17.8) | 254 (15.6) | 197 (12.4) | |
| Education [n (%)] | <0.001 ** | |||||
| No formal education | 21 (1.3) | 22 (1.4) | 21 (1.3) | 11 (0.7) | 9 (0.6) | |
| High school level | 582 (36.1) | 507 (32.7) | 452 (29.0) | 375 (23.3) | 289 (18.4) | |
| Diploma | 449 (27.9) | 414 (26.7) | 398 (25.6) | 402 (25.0) | 340 (21.7) | |
| University degree | 558 (34.7) | 607 (39.2) | 685 (44.1) | 821 (51.0) | 929 (59.3) | |
| Occupation [n (%)] | <0.001 ** | |||||
| No paid employment | 393 (24.2) | 354 (22.6) | 269 (17.1) | 257 (15.9) | 195 (12.3) | |
| Paid employment | 1228 (75.8) | 1210 (77.4) | 1304 (82.9) | 1364 (84.1) | 1385 (87.7) | |
| Income stress [n (%)] | <0.001 ** | |||||
| Easy | 885 (54.3) | 884 (56.4) | 904 (57.4) | 1031 (63.2) | 1036 (65.2) | |
| Difficult | 746 (45.7) | 683 (43.6) | 670 (42.6) | 600 (36.8) | 552 (34.8) | |
| Physical activity [n (%)] | <0.001 ** | |||||
| None/sedentary | 204 (12.7) | 167 (10.8) | 129 (8.3) | 101 (6.3) | 56 (3.6) | |
| Low | 625 (38.9) | 578 (37.3) | 510 (32.7) | 482 (29.8) | 375 (23.8) | |
| Moderate | 359 (22.3) | 355 (22.9) | 380 (24.2) | 414 (25.6) | 381 (24.2) | |
| High | 420 (26.1) | 450 (29.0) | 543 (34.8) | 618 (38.3) | 761 (48.4) | |
| Taking prescribed medicine [n (%)] | 0.22 | |||||
| No | 1170 (72.7) | 1107 (71.5) | 1134 (72.7) | 1206 (74.6) | 1171 (74.5) | |
| Yes | 440 (27.3) | 442 (28.5) | 425 (27.3) | 411 (25.4) | 401 (25.5) | |
| Survey | S4 | S5 | S6 | S7 | S8 |
|---|---|---|---|---|---|
| NCD | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) |
| CHD | n = 11 | n = 17 | n = 29 | n = 42 | n = 69 |
| S4 (n = 6871) a | S5 (n = 6127) a | S6 (n = 6017) a | S7 (n = 5452) a | S8 (n = 5394) a | |
| Univariate | 1.0 (0.1–7.0) | 3.9 (0.4–34.6) | 1.2 (0.3–4.3) | 2.7 (0.6–13.6) | 1.1 (0.5–2.5) |
| HT | n = 77 | n = 231 | n = 346 | n = 433 | n = 556 |
| S4 (n = 6871) a | S5 (n = 6127) a | S6 (n = 6017) a | S7 (n = 5452) a | S8 (n = 5394) a | |
| Univariate | 0.9 (0.4–1.8) | 0.7 (0.4–1.1) | 0.7 (0.5–1.0) | 0.6 (0.4–0.9) * | 0.7 (0.5–0.9) * |
| S4 (n = 6608) b | S5 (n = 5905) b | S6 (n = 5814) b | S7 (n = 5268) b | S8 (n = 5214) b | |
| Multivariate c | 1.0 (0.5–2.3) | 0.7 (0.4–1.2) | 0.7 (0.5–1.0) | 0.7 (0.5–1.1) | 0.8 (0.6–1.1) |
| Asthma | n = 662 | n = 559 | n = 558 | n = 464 | n = 478 |
| S4 (n = 6871) a | S5 (n = 6127) a | S6 (n = 6017) a | S7 (n = 5452) a | S8 (n = 5394) a | |
| Univariate | 0.76 (0.59–0.99) * § ¥ | 0.8 (0.6–1.0) | 0.8 (0.6–1.1) | 0.9 (0.6–1.2) | 0.9 (0.6–1.1) |
| S4 (n = 6621) b | S5 (n = 5914) b | S6 (n = 5824) b | S7 (n = 5279) b | S8 (n = 5226) b | |
| Multivariate d | 0.75 (0.57–0.99) * § ¥ | 0.8 (0.6–1.0) | 0.8 (0.6–1.1) | 0.8 (0.6–1.1) | 0.8 (0.6–1.1) |
| Multivariate d+ | 0.8 (0.6–1.1) | 0.8 (0.6–1.1) | 0.9 (0.7–1.2) | 0.9 (0.6–1.2) | 0.8 (0.6–1.2) |
| Cancer (excludes skin cancer) | n = 68 | n = 100 | n = 148 | n = 200 | n = 274 |
| S4 (n = 6871) a | S5 (n = 6127) a | S6 (n = 6017) a | S7 (n = 5452) a | S8 (n = 5394) a | |
| Univariate | 1.3 (0.6–2.8) | 1.5 (0.7–2.9) | 1.1 (0.6–1.8) | 1.0 (0.6–1.6) | 0.9 (0.6–1.3) |
| S4 (n = 6621) b | S5 (n = 5866) b | S6 (n = 5785) b | S7 (n = 5279) b | S8 (n = 5226) b | |
| Multivariate | 1.4 (0.6–3.1) | 1.4 (0.7–3.0) | 1.1 (0.6–2.0) | 0.9 (0.5–1.5) | 0.85 (0.6–1.3) |
| DM | n = 24 | n = 62 | n = 110 | n = 136 | n = 167 |
| S4 (n = 6871) a | S5 (n = 6127) a | S6 (n = 6017) a | S7 (n = 5452) a | S8 (n = 5394) a | |
| Univariate | 0.8 (0.2–3.0) | 1.4 (0.5–3.6) | 0.8 (0.4–1.6) | 0.7 (0.4–1.4) | 0.6 (0.3–1.1) |
| S4 (n = 6560) b | S5 (n = 5905) b | S6 (n = 5814) b | S7 (n = 5268) b | S8 (n = 5214) b | |
| Multivariate e | 0.9 (0.2–4.0) | 1.5 (0.5–4.5) | 0.8 (0.4–1.6) | 0.7 (0.3–1.4) | 0.6 (0.3–1.3) |
| Depression and/or anxiety | n = 999 | n = 1106 | n = 1199 | n = 1058 | n = 1024 |
| S4 (n = 6871) a | S5 (n = 6127) a | S6 (n = 6017) a | S7 (n = 5452) a | S8 (n = 5394) a | |
| Univariate | 1.0 (0.8–1.2) | 1.0 (0.8–1.2) | 1.0 (0.8–1.2) | 0.9 (0.8–1.2) | 0.9 (0.8–1.2) |
| S4 (n = 6621) b | S5 (n = 5914) b | S6 (n = 5824) b | S7 (n = 5279) b | S8 (n = 5226) b | |
| Multivariate f | 1.0 (0.8–1.3) | 1.0 (0.8–1.2) | 1.1 (0.9–1.4) | 1.0 (0.8–1.3) | 1.0 (0.8–1.3) |
| Multimorbidity | n = 198 | n = 253 | n = 360 | n = 346 | n = 413 |
| S4 (n = 6871) a | S5 (n = 6127) a | S6 (n = 6017) a | S7 (n = 5452) a | S8 (n = 5394) a | |
| Univariate | 0.9 (0.6–1.5) | 0.9 (0.6–1.4) | 0.9 (0.6–1.2) | 1.0 (0.7–1.4) | 0.9 (0.6–1.2) |
| S4 (n = 6621) b | S5 (n = 5914) b | S6 (n = 5824) b | S7 (n = 5279) b | S8 (n = 5226) b | |
| Multivariate f | 1.1 (0.7–1.8) | 0.9 (0.6–1.4) | 0.9 (0.6–1.3) | 1.0 (0.7–1.5) | 0.8 (0.6–1.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hlaing-Hlaing, H.; Dolja-Gore, X.; Tavener, M.; James, E.L.; Hure, A.J. Alternative Healthy Eating Index-2010 and Incident Non-Communicable Diseases: Findings from a 15-Year Follow Up of Women from the 1973–78 Cohort of the Australian Longitudinal Study on Women’s Health. Nutrients 2022, 14, 4403. https://doi.org/10.3390/nu14204403
Hlaing-Hlaing H, Dolja-Gore X, Tavener M, James EL, Hure AJ. Alternative Healthy Eating Index-2010 and Incident Non-Communicable Diseases: Findings from a 15-Year Follow Up of Women from the 1973–78 Cohort of the Australian Longitudinal Study on Women’s Health. Nutrients. 2022; 14(20):4403. https://doi.org/10.3390/nu14204403
Chicago/Turabian StyleHlaing-Hlaing, Hlaing, Xenia Dolja-Gore, Meredith Tavener, Erica L. James, and Alexis J. Hure. 2022. "Alternative Healthy Eating Index-2010 and Incident Non-Communicable Diseases: Findings from a 15-Year Follow Up of Women from the 1973–78 Cohort of the Australian Longitudinal Study on Women’s Health" Nutrients 14, no. 20: 4403. https://doi.org/10.3390/nu14204403