
Increasing Fruit and Vegetable Intake of Primary School Children in a Quasi-Randomized Trial: Evaluation of the Three-Year School-Based Multicomponent Intervention

Abstract
:1. Introduction
2. Materials and Methods
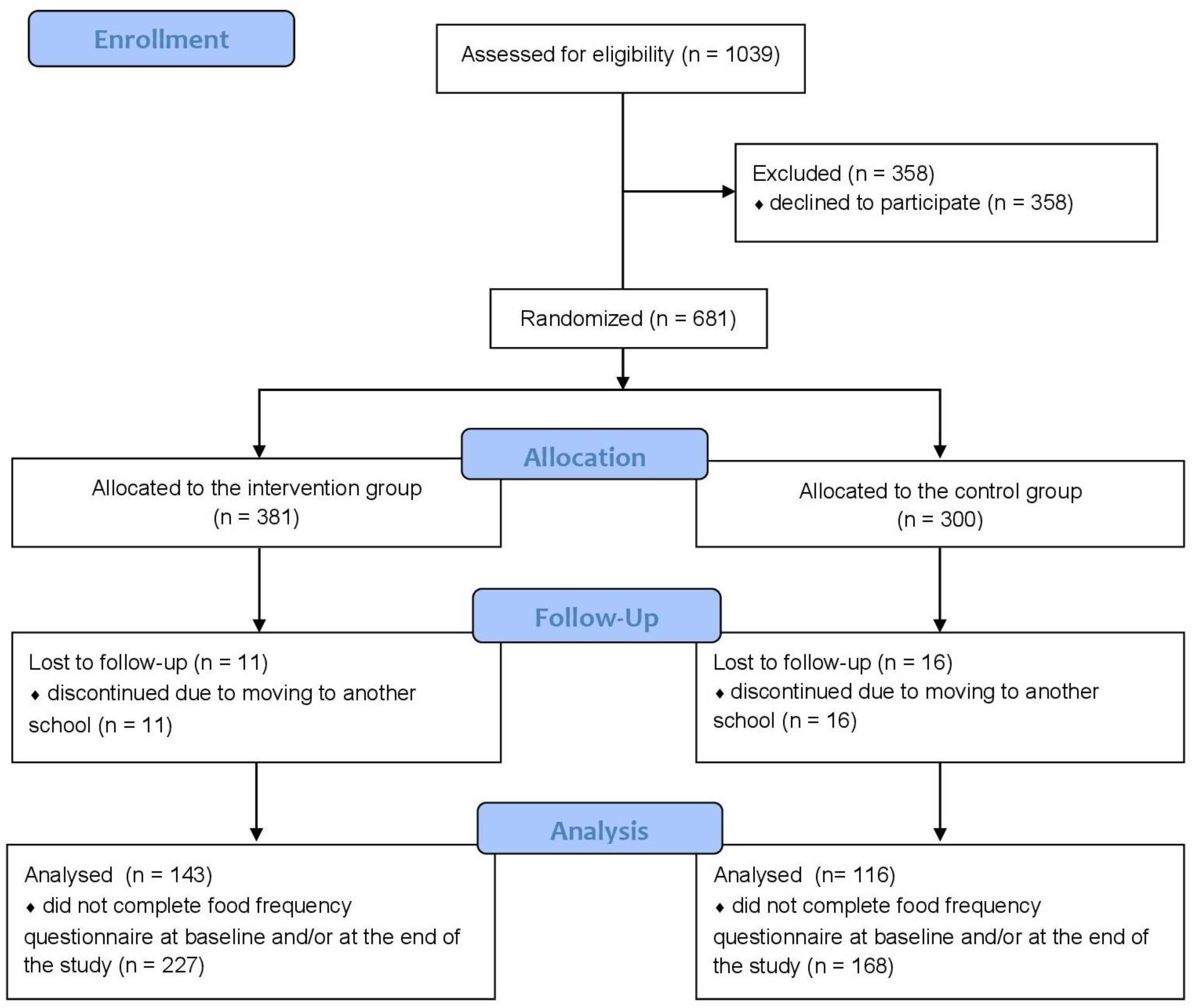
2.1. Study Design and Settings
2.2. Participants
2.3. Intervention
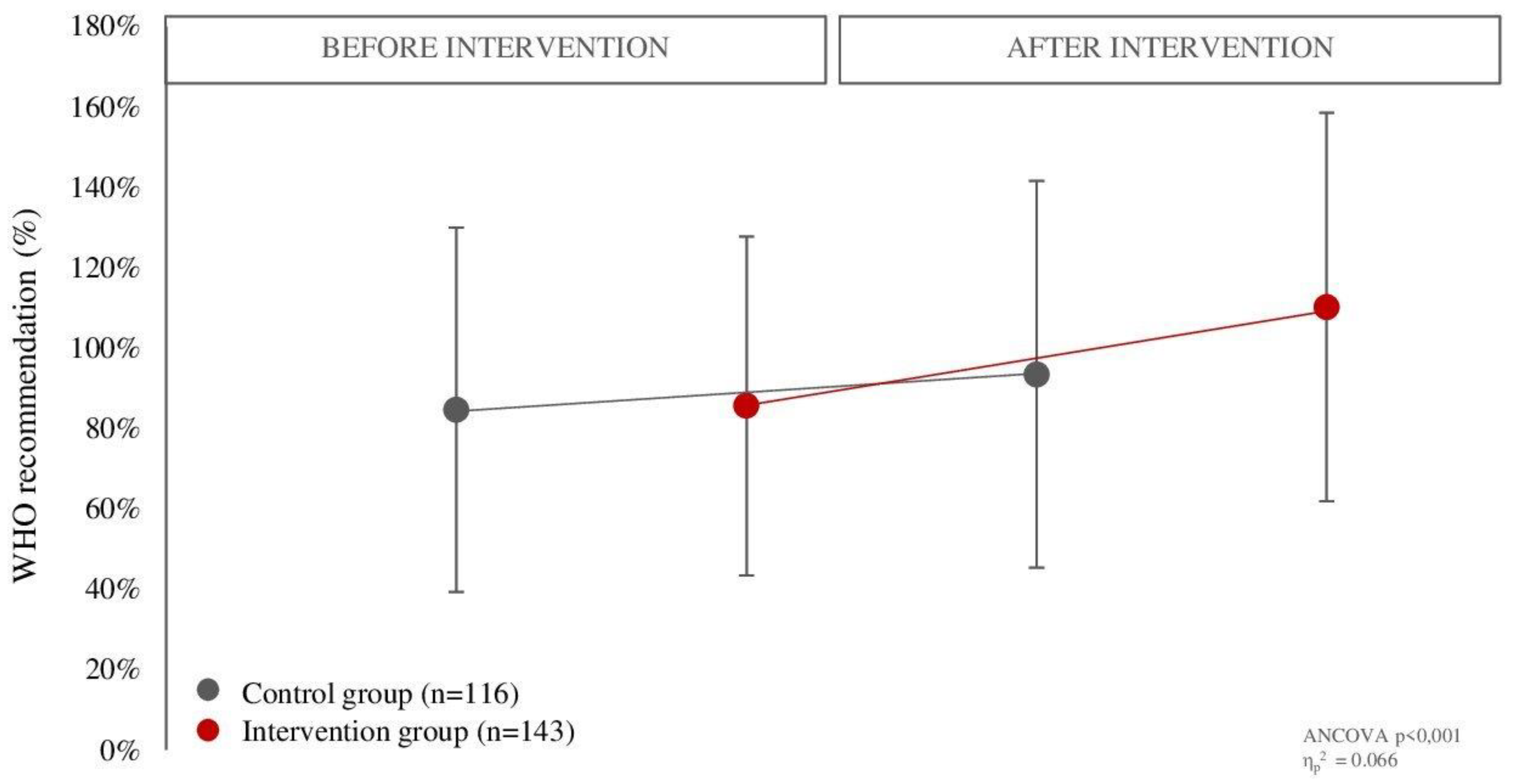
2.4. Assessment of Fruit and Vegetable Intake
2.5. Anthropometric Data
2.6. Physical Activity Level
2.7. General Questionnaire
2.8. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases: Report of Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Slavin, J.L.; Lloyd, B. Health benefits of fruits and vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijnhoven, T.M.; van Raaij, J.M.; Yngve, A.; Sjöberg, A.; Kunešová, M.; Duleva, V.; Petrauskiene, A.; Rito, A.I.; Breda, J. WHO European Childhood Obesity Surveillance Initiative: Health-risk behaviours on nutrition and physical activity in 6–9-year-old schoolchildren. Public Health Nutr. 2015, 18, 3108–3124. [Google Scholar] [CrossRef] [Green Version]
- Food and Agriculture Organization and World Health Organization. Sustainable Healthy Diets—Guiding Principles; Food and Agriculture Organization of the United Nations, World Health Organization: Rome, Italy, 2019. [Google Scholar]
- World Health Organization. WHO European Childhood Obesity Surveillance Initiative: Overweight and Obesity among 6–9-Year-Old Children. Report of the Third Round of Data Collection 2012–2013; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Mihrshahi, S.; Myton, R.; Partridge, S.R.; Esdaile, E.; Hardy, L.L.; Gale, J. Sustained low consumption of fruit and vegetables in Australian children: Findings from the Australian National Health Surveys. Health Promot. J. Aust. 2019, 30, 83–87. [Google Scholar] [CrossRef] [Green Version]
- Wambogo, E.A.; Ansai, N.; Ahluwalia, N.; Ogden, C.L. Fruit and vegetable consumption among children and adolescents in the United States, 2015–2018. NHC Data Brief 2020, 391, 1–8. [Google Scholar]
- Al-Jawaldeh, A.; Taktouk, M.; Nasreddine, L. Food consumption patterns and nutrient intakes of children and adolescents in the Eastern Mediterranean Region: A call for policy action. Nutrients 2020, 12, 3345. [Google Scholar] [CrossRef]
- Van Cauwenberghe, E.; Maes, L.; Spittaels, H.; van Lenthe, F.J.; Brug, J.; Oppert, J.-M.; De Bourdeaudhuij, I. Effectiveness of school-based interventions in Europe to promote healthy nutrition in children and adolescents: Systematic review of published and ‘grey’ literature. Br. J. Nutr. 2010, 103, 781–797. [Google Scholar] [CrossRef]
- Appleton, K.M.; Hemingway, A.; Saulais, L.; Dinnella, C.; Monteleone, E.; Depezay, L.; Morizet, D.; Armando Perez-Cueto, F.J.; Bevan, A.; Hartwell, H. Increasing vegetable intakes: Rationale and systematic review of published interventions. Eur. J. Nutr. 2016, 55, 869–896. [Google Scholar] [CrossRef] [Green Version]
- Blanchette, L.; Brug, J. Determinants of fruit and vegetable consumption among 6-12-year-old children and effective interventions to increase consumption. J. Hum. Nutr. Diet. 2005, 18, 431–443. [Google Scholar] [CrossRef] [PubMed]
- Knai, C.; Pomerleau, J.; Lock, K.; McKee, M. Getting children to eat more fruit and vegetables: A systematic review. Prev. Med. (Baltim.) 2006, 42, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.E.L.; Christian, M.S.; Cleghorn, C.L.; Greenwood, D.C.; Cade, J.E. Systematic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 y. Am. J. Clin. Nutr. 2012, 96, 889–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Noguera, M.; Tort, S.; Martínez-Zapata, M.J.; Bonfill, X. Primary school interventions to promote fruit and vegetable consumption: A systematic review and meta-analysis. Prev. Med. (Baltim.) 2011, 53, 3–9. [Google Scholar] [CrossRef]
- Diep, C.S.; Chen, T.-A.; Davies, V.F.; Baranowski, J.C.; Baranowski, T. Influence of behavioral theory on fruit and vegetable intervention effectiveness among children: A meta-analysis. J. Nutr. Educ. Behav. 2014, 46, 506–546. [Google Scholar] [CrossRef]
- Contento, I.R. Nutrition Education: Linking Research, Theory and Practice, 3rd ed.; Jones and Bartlett Learning: Burlington, UK, 2016. [Google Scholar]
- Hayes, D.; Contento, I.R.; Weekly, C. Position of the Academy of Nutrition and Dietetics, Society for Nutrition Education and Behavior, and School Nutrition Association: Comprehensive Nutrition Programs and Services in Schools. J. Nutr. Educ. Behav. 2018, 50, 433–439.e1. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.; Buoncristiano, M.; Nardone, P.; Rito, A.I.; Spinelli, A.; Hejgaard, T.; Kierkegaard, L.; Nurk, E.; Kunešová, M.; Musić Milanović, S.; et al. A Snapshot of European Children’s Eating Habits: Results from the Fourth Round of the WHO European Childhood Obesity Surveillance Initiative (COSI). Nutrients 2020, 12, 2481. [Google Scholar] [CrossRef] [PubMed]
- Ilić, A.; Bituh, M.; Brečić, R.; Colić Barić, I. Relationship between plate waste and food preferences among primary school students aged 7–10 years. J. Nutr. Educ. Behav. 2022, 54, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Hrvatska, R.; Športa, O.I. Državni pedagoški standard osnovnoškolskog sustava odgoja i obrazovanja. Nar. Novine 2008, 63. [Google Scholar]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [Green Version]
- Capak, K.; Colić, I.; Sanja, B.; Milanović, M.; Petrović, G.; Pucarin-Cvetković, J.; Jureša, V.; Pavić, I.; Iva, Š.; Franelić, P.; et al. Nacionalne Smjernice za Prehranu Učenika u Osnovnim Školama; Ministartsvo zdravstva Republike Hrvatske: Zagreb, Croatia, 2013. [Google Scholar]
- Ilić, A.; Bituh, M.; Brečić, R.; Colić Barić, I. Do School Menus in Zagreb Municipality Offer Enough Fruits and Vegetables? In Central European Congress on Food; Brka, M., Sarić, Z., Oručević Žuljević, S., Omanović-Mikličanin, E., Taljić, I., Biber, L., Mujčinović, A., Eds.; Springer: Cham, Switzerland, 2022; pp. 252–261. [Google Scholar]
- Ilić, A.; Rumbak, I.; Marić, L.; Karlović, T.; Brečić, R.; Colić Barić, I.; Bituh, M. The proportion of differently processed foods in the diet of Croatian school-aged children and its impact on daily energy and nutrient intake. Croat. J. Food Sci. Tecnol. 2022, 14, 15. [Google Scholar] [CrossRef]
- Čačić Kenjerić, D.; Sokolići, D. Food, nutrition, and health in Croatia. In Nutritional and Health Aspects of Food in the Balkans; Gostin, A.I., Bogueva, D., Kakurinov, V., Eds.; Academic Press: London, UK, 2021; pp. 91–106. [Google Scholar]
- Boyel, M.A. Community Nutrition in Action—A Entrepreneurial Approach, 7th ed.; Cengage Learnig: Boston, MA, USA, 2016. [Google Scholar]
- Bronfenbrenner, U.; Morris, P.A. The bioecological model of human development. In Handbook of Child Psychology: Theoretical Models of Human Development; Lerner, R.M., Damon, W., Eds.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2006; pp. 793–828. [Google Scholar]
- Wardle, J.; Herrera, M.L.; Cooke, L.; Gibson, E.L. Modifying children’s food preferences: The effects of exposure and reward on acceptance of an unfamiliar vegetable. Eur. J. Clin. Nutr. 2003, 57, 341–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brug, J.; Tak, N.I.; Te Velde, S.J.; Bere, E.; De Bourdeaudhuij, I. Taste preferences, liking and other factors related to fruit and vegetable intakes among schoolchildren: Results from observational studies. Br. J. Nutr. 2008, 29, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Touyz, L.M.; Wakefield, C.E.; Grech, A.M.; Quinn, V.F.; Costa, D.S.J.; Zhang, F.F.; Cohn, R.J.; Sajeev, M.; Cohen, J. Parent-targeted home-based interventions for increasing fruit and vegetable intake in children: A systematic review and meta-analysis. Nutr. Rev. 2018, 76, 154–173. [Google Scholar] [CrossRef] [PubMed]
- Ilić, A.; Rumbak, I.; Brečić, R.; Colić Barić, I.; Bituh, M. Relative validity and reproducibility of a semi-quantitative food frequency questionnaire to assess fruit and vegetable consumption in school-aged children. Front. Nutr. 2022, 9, 934295. [Google Scholar] [CrossRef] [PubMed]
- Agudo, A. Measuring intake of fruit and vegetables. In Proceedings of the Joint FAO/WHO Workshop on Fruit and Vegetables for Health, Kobe, Japan, 1–3 September 2004; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Blössner, M.; Siyam, A.; Borghi, E.; Onyanngo, A.; de Onis, M. WHO AnthroPlus for Personal Computers Manual: Software for Assessing Growth of the World’s Children and Adolescents 2009; Work Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Kowalski, K.C.; Croocker, P.R.E.; Donen, R.M. The Physical Activity Questionnaire for Older Children (PAQ-C) and Adolescents (PAQ-A) Manual; College of Kinesiology, University of Saskatchewan: Saskatoon, SK, Canada, 2004. [Google Scholar]
- Vidaković Samaržija, D.; Mišigoj-Duraković, M. Reliability of Croatian version of the questionnaire for assessment of overall level of physical activity of younger school children. Hrvat. Športskomed. Vjesn. 2013, 28, 24–32. [Google Scholar]
- Wolfson, A.R.; Carskadon, M.A. Sleep schedules and daytime functioning in adolescents. Child Dev. 1998, 69, 875–887. [Google Scholar] [CrossRef] [PubMed]
- Erna, L.; Garaulet, M.; Ortega, F.B.; Ruiz, J.R.; Rey-Ló Pez, J.P.; Béghin, L.; Manios, Y.; Cuenca-García, M.; Plada, M.; Diethelm, K.; et al. Short sleep duration is associated with increased obesity markers in European adolescents: Effect of physical activity and dietary habits. HELENA study Int. J. Obes. 2011, 35, 1308–1317. [Google Scholar]
- Roman-Viñas, B.; Chaput, J.-P.; Katzmarzyk, P.T.; Fogelholm, M.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; Onywera, V.; Sarmiento, O.L.; et al. Proportion of children meeting recommendations for 24-hour movement guidelines and associations with adiposity in a 12-country study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 123. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, R.; Kehoe, L.; Flynn, A.; Walton, J. The role of fruit and vegetables in the diets of children in Europe: Current state of knowledge on dietary recommendations, intakes and contribution to energy and nutrient intakes. Proc. Nutr. Soc. 2020, 79, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Irish Universities Nutrition Alliance. National Children’s Food Survey II Main Report 2019; Irish University Nutrition: Dublin, Ireland, 2019. [Google Scholar]
- Leclercq, C.; Arcella, D.; Piccinelli, R.; Sette, S.; Le Donne, C. The Italian National Food Consumption Survey INRAN-SCAI 2005–06: Main results in terms of food consumption. Public Health Nutr. 2009, 12, 2504–2532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, A.N.; Christensen, T.; Matthiessen, J.; Knudsen, V.K.; Rosenlund-Sørensen, M.; Biltoft-Jensen, A.; Hinsch, H.J.; Ygil, K.H.; Kørup, K.; Saxholt, E.; et al. Danish National Survey of Dietary Dietary Habits and Physical Activity (DANSDA) (2011–2013); National Food Institute, Technical University of Denmark: Søborg, Denmark, 2014. [Google Scholar]
- Rossum, C.T.M.; Buurma-Rethans, E.J.M.; Vennemann, F.B.C.; Beukers, M.; Brants, H.A.M.; de Boer, E.O.M. The Diet of the Dutch. Results of the First Two Years of the Dutch National Food Consumption Survey 2012–2016; The Netherlands National Institute for Public Health and the Environment: Bilthoven, The Netherlands, 2016. [Google Scholar]
- Public Health England. National Diet and Nutrition Survey Results from Years 7 and 8 (Combined) of the Rolling Programme (2014/2015 to 2015/2016); Public Health England and the Food Standards Agency: London, UK, 2018. [Google Scholar]
- Partearroyo, T.; Samaniego-Vaesken, M.D.L.; Ruiz, E.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Current food consumption amongst the Spanish ANIBES Study Population. Nutrients 2019, 11, 2663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Agriculture. Dietary Guidelines for Americans 2020–2025. Make Every Bit Count with the Dietary Guidelines, 9th ed.; U.S. Department of Agriculture: Washington, DC, USA, 2020. [Google Scholar]
- Rasmussen, M.; Krolner, R.; Klepp, K.-I.; Lytle, L.; Brug, J.; Bere, E.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part I: Quantitative studies. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 22. [Google Scholar] [CrossRef] [Green Version]
- Godrich, S.L.; Davies, C.R.; Darby, J.; Devine, A. Which ecological determinants influence Australian children’s fruit and vegetable consumption? Health Promot. Int. 2016, 33, 229–238. [Google Scholar] [CrossRef]
- Haß, J.; Hartmann, M. What determines the fruit and vegetables intake of primary school children?—An analysis of personal and social determinants. Appetite 2018, 120, 82–91. [Google Scholar]
- Hurley, J.C.; Bruening, M.; Ohri-Vachaspati, P.; Adams, M.A. Demographic relationships to students’ fruit and vegetable intake. Am. J. Health Behav. 2018, 42, 60–69. [Google Scholar] [CrossRef]
- De Menezes, M.C.; Diez Roux, A.V.; Souza Lopes, A.C. Fruit and vegetable intake: Influence of perceived food environment and self-efficacy. Appetite 2018, 127, 249–256. [Google Scholar] [CrossRef]
- Helsel, B.C.; Liang, J.; Williams, J.E.; Griffin, S.F.; Spitler, H. Family and friend influences on fruit and vegetable intake in elementary aged children. J. Community Health 2019, 44, 932–940. [Google Scholar] [CrossRef]
- Fismen, A.; Buoncristiano, M.; Williams, J.; Helleve, A.; Abdrakhmanova, S.; Bakacs, M.; Bergh, I.H.; Boymatova, K.; Duleva, V.; Fijałkowska, A.; et al. Socioeconomic differences in food habits among 6- to 9-year-old children from 23 countries—WHO European Childhood Obesity Surveillance Initiative (COSI 2015/2017). Obes. Rev. 2021, 22, e13211. [Google Scholar] [CrossRef]
- Field, A.E.; Gillman, M.W.; Rosner, B.; Rockett, H.R.; Colditz, G.A. Association between fruit and vegetable intake and change in body mass index among a large sample of children and adolescents in the United States. Int. J. Obes. 2003, 27, 821–826. [Google Scholar] [CrossRef] [Green Version]
- Manz, K.; Mensink, G.B.M.; Finger, J.D.; Haftenberger, M.; Brettschneider, A.-K.; Lage Barbosa, C.; Krug, S.; Schienkiewitz, A. Associations between physical activity and food intake among children and adolescents: Results of KiGGS wave 2. Nutrients 2019, 11, 1060. [Google Scholar] [CrossRef] [Green Version]
- Börnhorst, C.; Wijnhoven, T.M.A.; Kunešová, M.; Yngve, A.; Rito, A.I.; Lissner, L.; Duleva, V.; Petrauskiene, A.; Breda, J. WHO European Childhood Obesity Surveillance Initiative: Associations between sleep duration, screen time and food consumption frequencies. BMC Public Health 2015, 15, 442. [Google Scholar] [CrossRef] [Green Version]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Screen time and its effect on dietary habits and lifestyle among schoolchildren. Cent. Eur. J. Public Health 2020, 28, 260–266. [Google Scholar] [CrossRef]
- Chaput, J.-P.; Katzmarzyk, P.T.; LeBlanc, A.G.; Tremblay, M.S.; Barreira, T.V.; Broyles, S.T.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; et al. Associations between sleep patterns and lifestyle behaviors in children: An international comparison. Int. J. Obes. Suppl. 2015, 5, S59–S65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savoie-Roskos, M.R.; Wengreen, H.; Durward, C. Increasing fruit and vegetable intake among children and youth through gardening-based interventions: A systematic review. J. Acad. Nutr. Diet. 2017, 117, 240–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlton, K.; Comerford, T.; Deavin, N.; Walton, K. Characteristics of successful primary school-based experiential nutrition programmes: A systematic literature review. Public Health Nutr. 2021, 24, 4642–4662. [Google Scholar] [CrossRef]
- World Health Organization. Food and Nutrition Policy for Schools: A Tool for the Development of School Nutrition Programmes in the European Region; WHO Regional Office for Europe: Copenhagen, Dsenmark, 2006. [Google Scholar]
- Heyman, M.B.; Abrams, S.A.; Heitlinger, L.A.; deCastro Cabana, M.; Gilger, M.A.; Gugig, R.; Hill, I.D.; Lightdale, J.R.; Daniels, S.R.; Corkins, M.R.; et al. Fruit juice in infants, children, and adolescents: Current recommendations. Pediatrics 2017, 139, e20170967. [Google Scholar] [CrossRef] [Green Version]
- Middleton, G.; Evans, A.B.; Keegan, R.; Bishop, D.; Evans, D. The importance of parents and teachers as stakeholders in school-based healthy eating programs. In Health Education: Parental and Educators’ Perspectives, Current Practices and Need Assessments. Health Care Issues, Costs and Access; NOVA Science Publishers: New York, NY, USA, 2014. [Google Scholar]
- Horne, P.J.; Tapper, K.; Lowe, C.F.; Hardman, C.A.; Jackson, M.C.; Woolner, J. Increasing children’s fruit and vegetable consumption: A peer-modelling and rewards-based intervention. Eur. J. Clin. Nutr. 2004, 58, 1649–1660. [Google Scholar] [CrossRef]
- Hashemi, S.Z.; Mehdi Hazavehei, S.M.; Shahabadi, S. Improving fruit and vegetable consumption in elementary school students: A systematic review of interventions. Int. J. Child Health Nutr. 2013, 2, 201–211. [Google Scholar] [CrossRef]
- Laureati, M.; Bergamaschi, V.; Pagliarini, E. School-based intervention with children. Peer-modeling, reward and repeated exposure reduce food neophobia and increase liking of fruits and vegetables. Appetite 2014, 83, 26–32. [Google Scholar] [CrossRef]
- Sharps, M.; Robinson, E. Encouraging children to eat more fruit and vegetables: Health vs. descriptive social norm-based messages. Appetite 2016, 100, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Chung, L.M.Y.; Fong, S.S.M. Appearance alteration of fruits and vegetables to increase their appeal to and consumption by school-age children: A pilot study. Health. Psychol. Open 2018, 5, 205510291880267. [Google Scholar] [CrossRef] [Green Version]
- Bennett, G.; Young, E.; Butler, I.; Coe, S. The impact of lockdown during the COVID-19 outbreak on dietary habits in various population groups: A scoping review. Front. Nutr. 2021, 8, 626432. [Google Scholar] [CrossRef]
- Burkart, S.; Parker, H.; Weaver, R.G.; Beets, M.W.; Jones, A.; Adams, E.L.; Chaput, J.; Armstrong, B. Impact of the COVID-19 pandemic on elementary schoolers’ physical activity, sleep, screen time and diet: A quasi-experimental interrupted time series study. Pediatr. Obes. 2022, 17, 12846. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.F.; Murphy, S.; Chaplin, K.; Lyons, R.A.; Atkinson, M.; Moore, L. Impacts of the Primary School Free Breakfast Initiative on socio-economic inequalities in breakfast consumption among 9–11-year-old schoolchildren in Wales. Public Health Nutr. 2014, 17, 1280–1289. [Google Scholar] [CrossRef] [Green Version]
- Vik, F.N.; Van Lippevelde, W.; Øverby, N.C. Free school meals as an approach to reduce health inequalities among 10–12- year-old Norwegian children. BMC Public Health 2019, 19, 951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agencija za plaćanja u poljoprivredi ribarstvu i ruralnom razvoju Školska Shema. Available online: https://www.apprrr.hr/skolska-shema-2020-2021/ (accessed on 28 April 2021).
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Livingstone, M.B.E.; Robson, P.J.; Wallace, J.M.W. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92, S213–S222. [Google Scholar] [CrossRef] [Green Version]
- Fahey, M.T.; Sasaki, S.; Kobayashi, M.; Akabane, M.; Tsugane, S. Seasonal misclassification error and magnitude of true between-person variation in dietary nutrient intake: A random coefficients analysis and implications for the Japan Public Health Center (JPHC) Cohort Study. Public Health Nutr. 2003, 6, 385–391. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total Sample | Control | Intervention | p Value 2 |
|---|---|---|---|---|
| Participants (n) | 259 | 116 | 143 | |
| Age (yr.) | 7.7 ± 0.4 | 7.7 ± 0.3 | 7.7 ± 0.4 | 0.476 |
| Sex (%): | ||||
| Boys | 49.8 | 49.1 | 50.3 | 0.846 |
| Girls | 50.2 | 50.9 | 49.7 | |
| Body height (cm) | 135.5 ± 5.9 | 135.4 ± 6.2 | 135.5 ± 5.7 | 0.818 |
| Body height for age z-score | 0.9 ± 1.0 | 0.9 ± 1.1 | 0.9 ± 0.9 | 0.989 |
| Body weight (kg) | 31.6 ± 6.6 | 30.7 ± 5.9 | 32.2 ± 7.0 | 0.129 |
| Body weight for age z-score | 0.8 ± 1.1 | 0.7 ± 1.1 | 0.9 ± 1.1 | 0.089 |
| Body mass index (kgm−2) | 17.7 ± 2.7 | 16.6 ± 2.3 | 17.4 ± 2.9 | 0.060 |
| Body mass index for age z-score | 0.4 ± 1.2 | 0.2 ± 1.1 | 0.6 ± 1.2 | 0.034 |
| Physical activity level | 3.1 ± 0.6 | 3.1 ± 0.7 | 3.1 ± 0.6 | 0.754 |
| Sleep time (min/day) | 585.2 ± 33.3 | 580.9 ± 34.2 | 589.1 ± 32.2 | 0.098 |
| Screen time (min/day) | 137.9 ± 69.9 | 141.8 ± 76.8 | 134.3 ± 63.2 | 0.992 |
| Household income (%): | ||||
| <5000.00 kn (664.92 €) | 2.2 | 3.4 | 1.0 | 0.750 |
| 5000.00–8000.00 kn (664.93–1063.87 €) | 6.6 | 5.7 | 7.3 | |
| 8000.01–14,000.00 kn (1063.88–1861.77 €) | 35.0 | 34.5 | 35.4 | |
| 14,000.01–18,000.00 kn (1861.78–2393.70 €) | 21.9 | 19.5 | 24.0 | |
| ≥18,000.01 kn (≥2393.71 €) | 34.4 | 36.8 | 32.3 |
| Food Groups | Sex 1 | Body Mass Index for Age z-Score 2 | Physical Activity Level 2 | Sleep Time 2 | Screen Time 2 | Household Income 3 |
|---|---|---|---|---|---|---|
| Fruit: | ||||||
| Fruit | 0.096 | 0.054 | 0.114 | 0.048 | −0.014 | 0.125 * |
| Fruit and fruit juices | 0.077 | 0.029 | 0.126 | 0.042 | 0.027 | 0.097 |
| Vegetables: | ||||||
| Vegetables | 0.043 | 0.005 | 0.166 * | 0.092 | 0.068 | 0.056 |
| Vegetables and vegetable juices | 0.034 | 0.013 | 0.177 * | 0.099 | 0.068 | 0.057 |
| Vegetables, vegetable juices and dry legumes | 0.035 | 0.011 | 0.167 * | 0.098 | 0.066 | 0.061 |
| Fruit and vegetables: | ||||||
| Fruit and vegetables | 0.093 | 0.045 | 0.138 * | 0.077 | 0.040 | 0.103 |
| Fruit, fruit juices, vegetables and vegetable juices | 0.073 | 0.028 | 0.142 * | 0.072 | 0.062 | 0.107 |
| Fruit, fruit juices, vegetables, vegetable juices and dry legumes | 0.059 | 0.026 | 0.139 * | 0.072 | 0.064 | 0.108 |
| Food Groups | Before Intervention | After Intervention | p Value 2 | ηp2 | ||
|---|---|---|---|---|---|---|
| Control Group (n = 116) | Intervention Group (n = 143) | Control Group (n = 116) | Intervention Group (n = 143) | |||
| Fruit: | ||||||
| Fruit | 188.6 ± 141.4 (162.9–219.9) | 171.7 ± 123.5 (149.7–193.2) | 211.2 ± 144.4 (181.5–238.4) | 216.2 ± 143.1 (193.3–240.9) | 0.099 | 0.011 |
| Fruit and fruit juices | 198.6 ± 139.2 (173.8–224.4) | 198.6 ± 139.2 (186.2–231.7) | 213.4 ± 136.0 (184.6–241.5) | 280.3 ± 168.5 (255.0–306.2) | 0.001 | 0.040 |
| Vegetables: | ||||||
| Vegetables | 134.5 ± 82.2 (121.7–146.5) | 119.9 ± 53.3 109.0–113.4) | 142.6 ± 84.7 (128.9–156.9) | 147.0 ± 68.9 (134.1–159.3) | 0.010 | 0.026 |
| Vegetables and vegetable juices | 137.1 ± 85.4 (123.5–149.7) | 122.7 ± 57.7 (111.3–134.9) | 145.2 ± 87.4 (131.1–159.9) | 149.8 ± 70.5 (136.6–162.5) | 0.014 | 0.023 |
| Vegetables, vegetable juices and dry legumes | 174.9 ± 135.8 (154.6–191.2) | 127.3 ± 60.5 (112.5–145.4) | 206.8 ± 151.5 (186.3–228.5) | 155.6 ± 72.9 (136.1–174.1) | 0.580 | 0.001 |
| Fruit and vegetables: | ||||||
| Fruit and vegetables | 320.3 ± 177.8 (289.9–349.8) | 291.5 ± 149.4 (264.9–318.8) | 354.6 ± 187.5 (321.9–386.4) | 362.8 ± 165.4 (334.2–392.3) | 0.011 | 0.023 |
| Fruit, fruit juices, vegetables and vegetable juices | 350.2 ± 187.5 (317.4–381.7) | 332.1 ± 164.9 (303.6–361.6) | 382.6 ± 196.8 (347.1–417.3) | 430.1 ± 186.7 (398.8–642.1) | <0.001 | 0.078 |
| Fruit, fruit juices, vegetables, vegetable juices and dry legumes | 313.5 ± 188.4 (282.4–347.2) | 336.7 ± 166.7 (306.5–364.7) | 321.8 ± 224.4 (283.9–359.1) | 435.9 ± 187.2 (402.3–470.0) | 0.002 | 0.074 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilić, A.; Rumbak, I.; Brečić, R.; Barić, I.C.; Bituh, M. Increasing Fruit and Vegetable Intake of Primary School Children in a Quasi-Randomized Trial: Evaluation of the Three-Year School-Based Multicomponent Intervention. Nutrients 2022, 14, 4197. https://doi.org/10.3390/nu14194197
Ilić A, Rumbak I, Brečić R, Barić IC, Bituh M. Increasing Fruit and Vegetable Intake of Primary School Children in a Quasi-Randomized Trial: Evaluation of the Three-Year School-Based Multicomponent Intervention. Nutrients. 2022; 14(19):4197. https://doi.org/10.3390/nu14194197
Chicago/Turabian StyleIlić, Ana, Ivana Rumbak, Ružica Brečić, Irena Colić Barić, and Martina Bituh. 2022. "Increasing Fruit and Vegetable Intake of Primary School Children in a Quasi-Randomized Trial: Evaluation of the Three-Year School-Based Multicomponent Intervention" Nutrients 14, no. 19: 4197. https://doi.org/10.3390/nu14194197