
A Proinflammatory Diet Is Associated with Higher Risk of Peripheral Artery Disease

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Exposure
2.3. Covariates
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
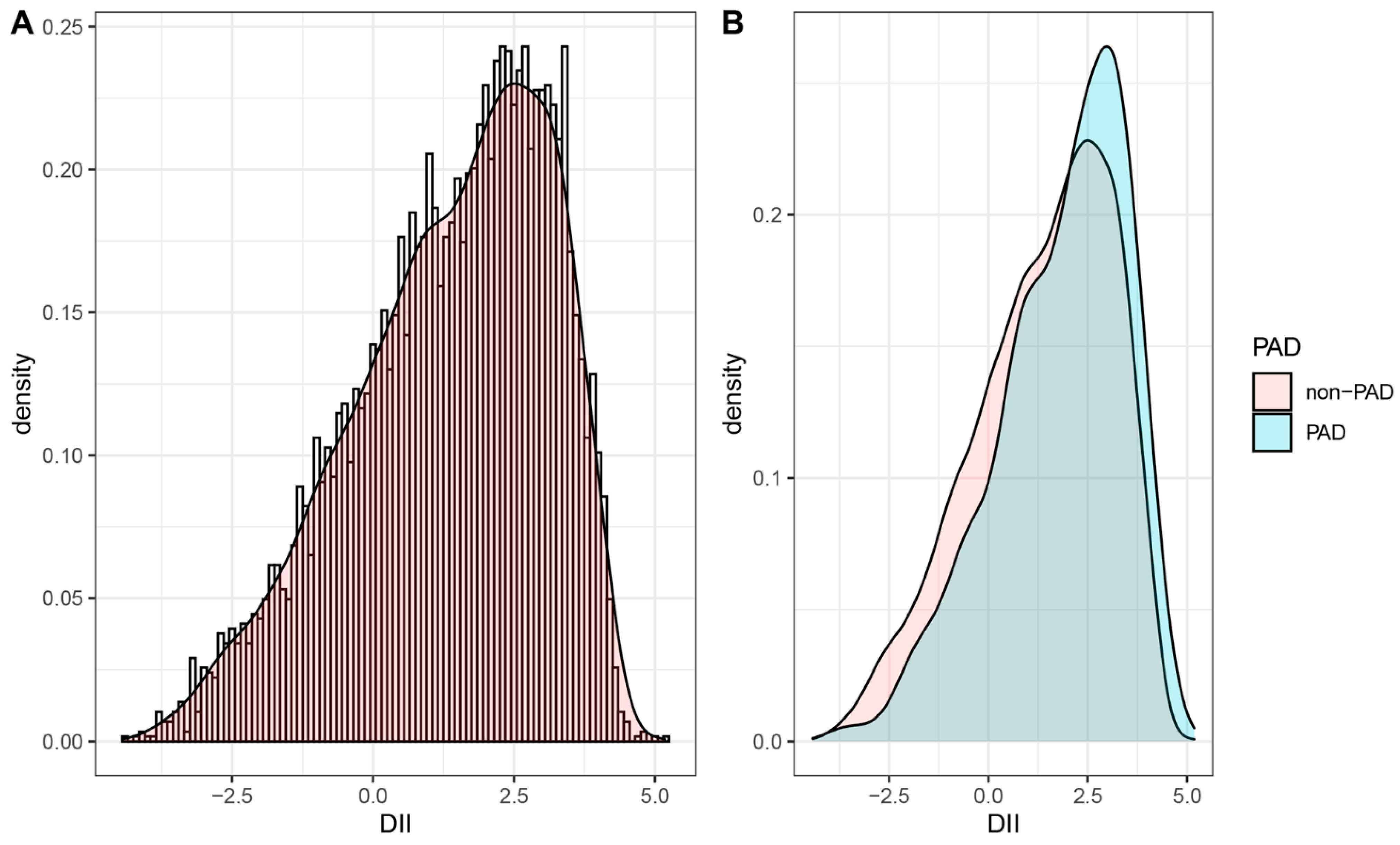
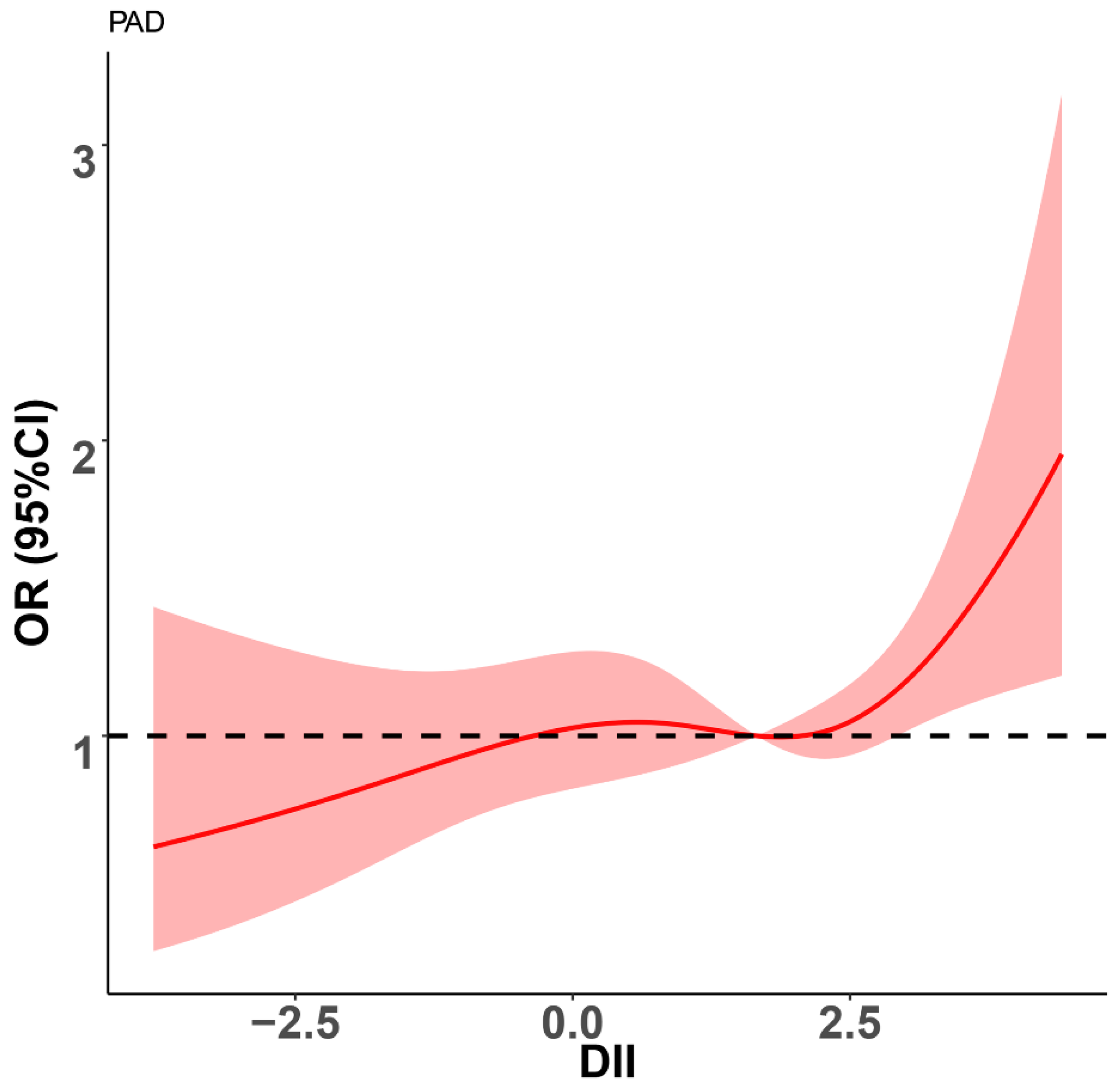
3.2. Association between DII and PAD
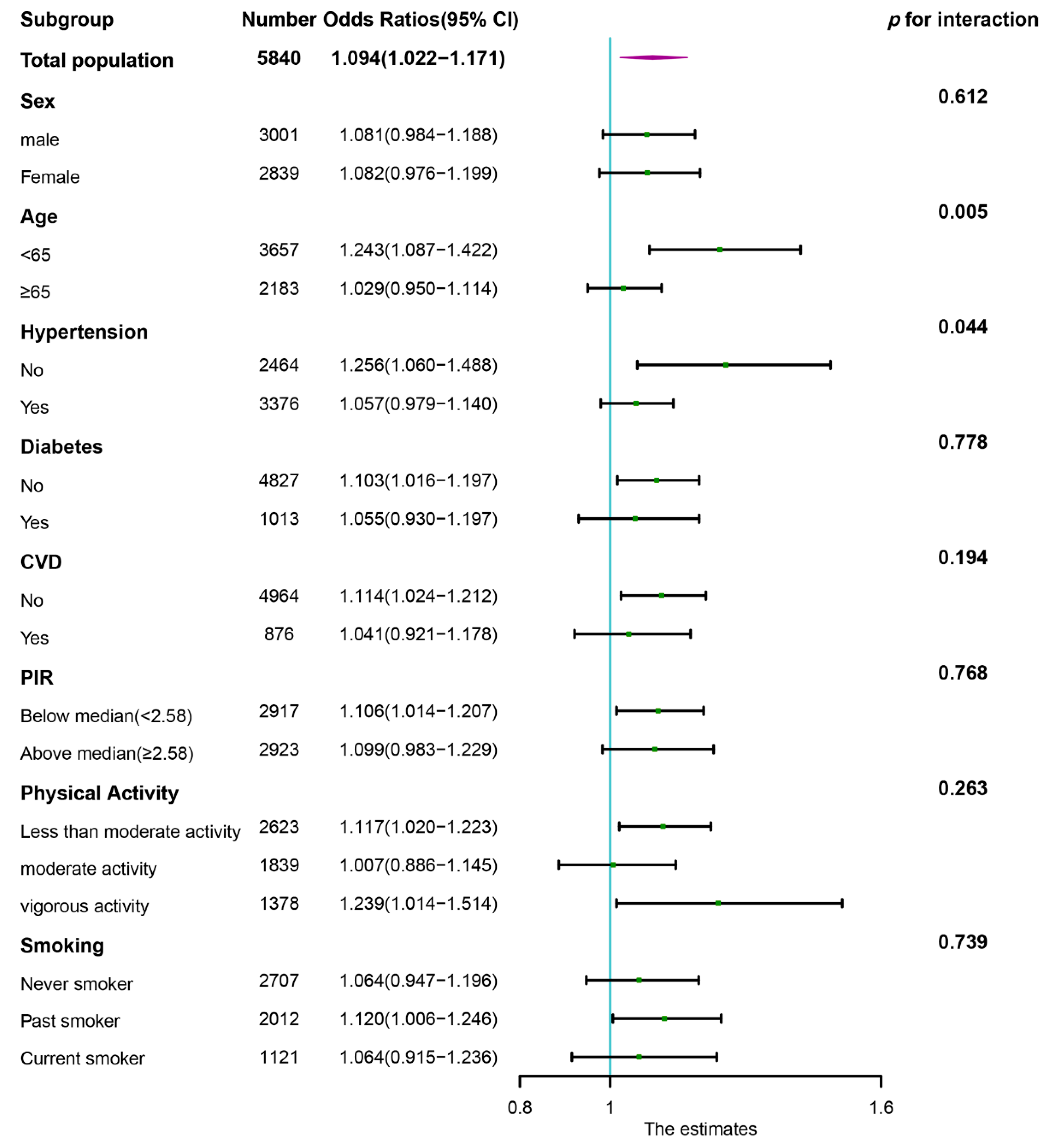
3.3. Stratification Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brevetti, G.; Giugliano, G.; Brevetti, L.; Hiatt, W.R. Inflammation in peripheral artery disease. Circulation 2010, 122, 1862–1875. [Google Scholar] [CrossRef] [PubMed]
- Shu, J.; Santulli, G. Update on peripheral artery disease: Epidemiology and evidence-based facts. Atherosclerosis 2018, 275, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Belch, J.J.F.; Baumgartner, I.; Giovas, P.; Hoffmann, U. Morbidity and mortality associated with atherosclerotic peripheral artery disease: A systematic review. Atherosclerosis 2020, 293, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Sigvant, B.; Lundin, F.; Wahlberg, E. The Risk of Disease Progression in Peripheral Arterial Disease is Higher than Expected: A Meta-Analysis of Mortality and Disease Progression in Peripheral Arterial Disease. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 395–403. [Google Scholar] [CrossRef]
- Loffredo, L.; Marcoccia, A.; Pignatelli, P.; Andreozzi, P.; Borgia, M.C.; Cangemi, R.; Chiarotti, F.; Violi, F. Oxidative-stress-mediated arterial dysfunction in patients with peripheral arterial disease. Eur. Heart J. 2007, 28, 608–612. [Google Scholar] [CrossRef]
- Ridker, P.M.; Cushman, M.; Stampfer, M.J.; Tracy, R.P.; Hennekens, C.H. Plasma concentration of C-reactive protein and risk of developing peripheral vascular disease. Circulation 1998, 97, 425–428. [Google Scholar] [CrossRef]
- Tzoulaki, I.; Murray, G.D.; Lee, A.J.; Rumley, A.; Lowe, G.D.; Fowkes, F.G. C-reactive protein, interleukin-6, and soluble adhesion molecules as predictors of progressive peripheral atherosclerosis in the general population: Edinburgh Artery Study. Circulation 2005, 112, 976–983. [Google Scholar] [CrossRef]
- Krzyzanowska, K.; Mittermayer, F.; Krugluger, W.; Schnack, C.; Hofer, M.; Wolzt, M.; Schernthaner, G. Asymmetric dimethylarginine is associated with macrovascular disease and total homocysteine in patients with type 2 diabetes. Atherosclerosis 2006, 189, 236–240. [Google Scholar] [CrossRef]
- Ding, N.; Yang, C.; Ballew, S.H.; Kalbaugh, C.A.; McEvoy, J.W.; Salameh, M.; Aguilar, D.; Hoogeveen, R.C.; Nambi, V.; Selvin, E.; et al. Fibrosis and Inflammatory Markers and Long-Term Risk of Peripheral Artery Disease: The ARIC Study. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2322–2331. [Google Scholar] [CrossRef]
- Selvaggio, S.; Abate, A.; Brugaletta, G.; Musso, C.; Di Guardo, M.; Di Guardo, C.; Vicari, E.S.D.; Romano, M.; Luca, S.; Signorelli, S.S. Platelet-to-lymphocyte ratio, neutrophil-to-lymphocyte ratio and monocyte-to-HDL cholesterol ratio as markers of peripheral artery disease in elderly patients. Int. J. Mol. Med. 2020, 46, 1210–1216. [Google Scholar] [CrossRef]
- Hayfron-Benjamin, C.F.; Mosterd, C.; Maitland-van der Zee, A.H.; van Raalte, D.H.; Amoah, A.G.B.; Agyemang, C.; van den Born, B.J. Inflammation and its associations with aortic stiffness, coronary artery disease and peripheral artery disease in different ethnic groups: The HELIUS Study. EClinicalMedicine 2021, 38, 101012. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Brann, L.; Shivappa, N.; Hébert, J.R. Dietary inflammatory index is positively associated with serum high-sensitivity C-reactive protein in a Korean adult population. Nutrition 2019, 63–64, 155–161. [Google Scholar] [CrossRef]
- Shivappa, N.; Hébert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, R.; Odjidja, E.N.; Scott, D.; Shivappa, N.; Hébert, J.R.; Hodge, A.; de Courten, B. The dietary inflammatory index, obesity, type 2 diabetes, and cardiovascular risk factors and diseases. Obes. Rev. 2022, 23, e13349. [Google Scholar] [CrossRef] [PubMed]
- Syed Soffian, S.S.; Mohammed Nawi, A.; Hod, R.; Ja’afar, M.H.; Isa, Z.M.; Chan, H.K.; Hassan, M.R.A. Meta-Analysis of the Association between Dietary Inflammatory Index (DII) and Colorectal Cancer. Nutrients 2022, 14, 1555. [Google Scholar] [CrossRef]
- Hayati, Z.; Jafarabadi, M.A.; Pirouzpanah, S. Dietary inflammatory index and breast cancer risk: An updated meta-analysis of observational studies. Eur. J. Clin. Nutr. 2022, 76, 1073–1087. [Google Scholar] [CrossRef]
- Shivappa, N.; Godos, J.; Hébert, J.R.; Wirth, M.D.; Piuri, G.; Speciani, A.F.; Grosso, G. Dietary Inflammatory Index and Cardiovascular Risk and Mortality-A Meta-Analysis. Nutrients 2018, 10, 200. [Google Scholar] [CrossRef]
- Chen, C.; Yang, T.; Wang, C. The Dietary Inflammatory Index and Early COPD: Results from the National Health and Nutrition Examination Survey. Nutrients 2022, 14, 2841. [Google Scholar] [CrossRef]
- Xiao, Y.; Huang, W. Association of Dietary Inflammatory Index with Depression and Suicidal Ideation in Older Adult: Results From the National Health and Nutrition Examination Surveys 2005–2018. Front Psychiatry 2022, 13, 944154. [Google Scholar] [CrossRef]
- Shakya, P.R.; Melaku, Y.A.; Shivappa, N.; Hébert, J.R.; Adams, R.J.; Page, A.J.; Gill, T.K. Dietary inflammatory index (DII®) and the risk of depression symptoms in adults. Clin. Nutr. 2021, 40, 3631–3642. [Google Scholar] [CrossRef]
- Jia, G.; Wu, C.C.; Su, C.H. Dietary inflammatory index and metabolic syndrome in US children and adolescents: Evidence from NHANES 2001–2018. Nutr. Metab. 2022, 19, 39. [Google Scholar] [CrossRef]
- Motamedi, A.; Askari, M.; Mozaffari, H.; Homayounfrar, R.; Nikparast, A.; Ghazi, M.L.; Nejad, M.M.; Alizadeh, S. Dietary Inflammatory Index in relation to Type 2 Diabetes: A Meta-Analysis. Int. J. Clin. Pract. 2022, 2022, 9953115. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Qiu, S.; Bian, H.; Tian, B.; Wang, H.; Tu, X.; Cai, B.; Jin, K.; Zheng, X.; Yang, L.; et al. Association between Dietary Inflammatory Index and kidney stones in US adults: Data from the National Health and Nutrition Examination Survey (NHANES) 2007–2016. Public Health Nutr. 2021, 24, 6113–6121. [Google Scholar] [CrossRef]
- Wolbert, L.; Kreutzburg, T.; Zyriax, B.C.; Adegbola, A.; Westenhöfer, J.; Jagemann, B.; Alexander Neumann, F.; Preuß, M.; Debus, E.S.; Rieß, H.C.; et al. A cross-sectional survey study on the nutrition patterns of patients with peripheral artery disease. Vasa 2022, 51, 239–246. [Google Scholar] [CrossRef]
- Wan, D.; Li, V.; Banfield, L.; Azab, S.; de Souza, R.J.; Anand, S.S. Diet and Nutrition in Peripheral Artery Disease: A Systematic Review. Can. J. Cardiol. 2022, 38, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, A.Z.; Davis, R.B.; Mukamal, K.J. Nutrient intake and peripheral artery disease in adults: Key considerations in cross-sectional studies. Clin. Nutr. 2014, 33, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Heffron, S.P.; Rockman, C.B.; Adelman, M.A.; Gianos, E.; Guo, Y.; Xu, J.F.; Berger, J.S. Greater Frequency of Fruit and Vegetable Consumption Is Associated with Lower Prevalence of Peripheral Artery Disease. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1234–1240. [Google Scholar] [CrossRef]
- Qu, C.J.; Teng, L.Q.; Liu, X.N.; Zhang, Y.B.; Fang, J.; Shen, C.Y. Dose-Response Relationship between Physical Activity and the Incidence of Peripheral Artery Disease in General Population: Insights from the National Health and Nutrition Examination Survey 1999–2004. Front. Cardiovasc. Med. 2021, 8, 730508. [Google Scholar] [CrossRef]
- Jones, M.R.; Apelberg, B.J.; Samet, J.M.; Navas-Acien, A. Smoking, menthol cigarettes, and peripheral artery disease in U.S. adults. Nicotine Tob. Res. 2013, 15, 1183–1189. [Google Scholar] [CrossRef]
- Berger, J.S.; Eraso, L.H.; Xie, D.; Sha, D.; Mohler, E.R., 3rd. Mean platelet volume and prevalence of peripheral artery disease, the National Health and Nutrition Examination Survey, 1999–2004. Atherosclerosis 2010, 213, 586–591. [Google Scholar] [CrossRef] [Green Version]
- Zalawadiya, S.K.; Veeranna, V.; Panaich, S.S.; Afonso, L. Red cell distribution width and risk of peripheral artery disease: Analysis of National Health and Nutrition Examination Survey 1999–2004. Vasc. Med. 2012, 17, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Liu, H.; Deng, Q.; Sun, C.; He, W.; Zheng, W.; Tang, R.; Li, W.; Xie, Q. Association between Dietary Inflammatory Index and Heart Failure: Results from NHANES (1999–2018). Front. Cardiovasc. Med. 2021, 8, 702489. [Google Scholar] [CrossRef]
- Qin, Z.; Chang, K.; Liao, R.; Jiang, L.; Yang, Q.; Su, B. Greater Dietary Inflammatory Potential Is Associated with Higher Likelihood of Abdominal Aortic Calcification. Front. Cardiovasc. Med. 2021, 8, 720834. [Google Scholar] [CrossRef] [PubMed]
- Min, J.Y.; Cho, J.S.; Lee, K.J.; Park, J.B.; Park, S.G.; Kim, J.Y.; Min, K.B. Potential role for organochlorine pesticides in the prevalence of peripheral arterial diseases in obese persons: Results from the National Health and Nutrition Examination Survey 1999–2004. Atherosclerosis 2011, 218, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Selvin, E.; Köttgen, A.; Coresh, J. Kidney function estimated from serum creatinine and cystatin C and peripheral arterial disease in NHANES 1999–2002. Eur. Heart J. 2009, 30, 1918–1925. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Kimiagar, M.; Mehrabi, Y.; Azadbakht, L.; Hu, F.B.; Willett, W.C. Dietary patterns and markers of systemic inflammation among Iranian women. J. Nutr. 2007, 137, 992–998. [Google Scholar] [CrossRef]
- Soltani, S.; Chitsazi, M.J.; Salehi-Abargouei, A. The effect of dietary approaches to stop hypertension (DASH) on serum inflammatory markers: A systematic review and meta-analysis of randomized trials. Clin. Nutr. 2018, 37, 542–550. [Google Scholar] [CrossRef]
- Shivappa, N.; Hebert, J.R.; Marcos, A.; Diaz, L.E.; Gomez, S.; Nova, E.; Michels, N.; Arouca, A.; González-Gil, E.; Frederic, G.; et al. Association between dietary inflammatory index and inflammatory markers in the HELENA study. Mol. Nutr. Food Res. 2017, 61, 1600707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di, X.; Han, W.; Liu, C.W.; Ni, L.; Zhang, R. A systematic review and meta-analysis on the association between C-reactive protein levels and adverse limb events after revascularization in patients with peripheral arterial disease. J. Vasc. Surg. 2021, 74, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Kremers, B.; Wübbeke, L.; Mees, B.; Ten Cate, H.; Spronk, H.; Ten Cate-Hoek, A. Plasma Biomarkers to Predict Cardiovascular Outcome in Patients with Peripheral Artery Disease: A Systematic Review and Meta-Analysis. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2018–2032. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Mantrana, I.; Selma-Royo, M.; Alcantara, C.; Collado, M.C. Shifts on Gut Microbiota Associated to Mediterranean Diet Adherence and Specific Dietary Intakes on General Adult Population. Front. Microbiol. 2018, 9, 890. [Google Scholar] [CrossRef] [PubMed]
- Nova, E.; Gómez-Martinez, S.; González-Soltero, R. The Influence of Dietary Factors on the Gut Microbiota. Microorganisms 2022, 10, 1368. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Gao, Y.; Chen, W.; Hu, Q.; He, Z.; Wang, X.; Li, D.; Lin, R. Dietary variety relates to gut microbiota diversity and abundance in humans. Eur. J. Nutr. 2022, 1–14. [Google Scholar] [CrossRef]
- Bolte, L.A.; Vich Vila, A.; Imhann, F.; Collij, V.; Gacesa, R.; Peters, V.; Wijmenga, C.; Kurilshikov, A.; Campmans-Kuijpers, M.J.E.; Fu, J.; et al. Long-term dietary patterns are associated with pro-inflammatory and anti-inflammatory features of the gut microbiome. Gut 2021, 70, 1287–1298. [Google Scholar] [CrossRef]
- Jonsson, A.L.; Bäckhed, F. Role of gut microbiota in atherosclerosis. Nat. Rev. Cardiol. 2017, 14, 79–87. [Google Scholar] [CrossRef]
- Gui, D.D.; Luo, W.; Yan, B.J.; Ren, Z.; Tang, Z.H.; Liu, L.S.; Zhang, J.F.; Jiang, Z.S. Effects of gut microbiota on atherosclerosis through hydrogen sulfide. Eur. J. Pharmacol. 2021, 896, 173916. [Google Scholar] [CrossRef]
- Duttaroy, A.K. Role of Gut Microbiota and Their Metabolites on Atherosclerosis, Hypertension and Human Blood Platelet Function: A Review. Nutrients 2021, 13, 144. [Google Scholar] [CrossRef]
- Roncal, C.; Martínez-Aguilar, E.; Orbe, J.; Ravassa, S.; Fernandez-Montero, A.; Saenz-Pipaon, G.; Ugarte, A.; Estella-Hermoso de Mendoza, A.; Rodriguez, J.A.; Fernández-Alonso, S.; et al. Trimethylamine-N-Oxide (TMAO) Predicts Cardiovascular Mortality in Peripheral Artery Disease. Sci. Rep. 2019, 9, 15580. [Google Scholar] [CrossRef] [Green Version]
- Senthong, V.; Wang, Z.; Fan, Y.; Wu, Y.; Hazen, S.L.; Tang, W.H. Trimethylamine N-Oxide and Mortality Risk in Patients with Peripheral Artery Disease. J. Am. Heart Assoc. 2016, 5, e004237. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, L.; Ivanov, V.; Ciobanu, N.; Deseatnicova, E.; Gutu, E.; Mudrea, L.; Ivanov, M.; Nocella, C.; Cammisotto, V.; Orlando, F.; et al. Is There an Association between Atherosclerotic Burden, Oxidative Stress, and Gut-Derived Lipopolysaccharides? Antioxid. Redox Signal. 2020, 33, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Brandsma, E.; Kloosterhuis, N.J.; Koster, M.; Dekker, D.C.; Gijbels, M.J.J.; van der Velden, S.; Ríos-Morales, M.; van Faassen, M.J.R.; Loreti, M.G.; de Bruin, A.; et al. A Proinflammatory Gut Microbiota Increases Systemic Inflammation and Accelerates Atherosclerosis. Circ. Res. 2019, 124, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Pande, R.L.; Creager, M.A. Socioeconomic inequality and peripheral artery disease prevalence in US adults. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 532–539. [Google Scholar] [CrossRef]
- Fanaroff, A.C.; Yang, L.; Nathan, A.S.; Khatana, S.A.M.; Julien, H.; Wang, T.Y.; Armstrong, E.J.; Treat-Jacobson, D.; Glaser, J.D.; Wang, G.; et al. Geographic and Socioeconomic Disparities in Major Lower Extremity Amputation Rates in Metropolitan Areas. J. Am. Heart Assoc. 2021, 10, e021456. [Google Scholar] [CrossRef]
- Otto, C.M. Marital status and cardiovascular disease risk. Heart 2018, 104, 1893–1894. [Google Scholar] [CrossRef]
- Cha, S.; Grace, S.L.; Han, K.; Kim, B.; Paik, N.J.; Won-Seok, K. Effect of physical activity and tobacco use on mortality and morbidity in patients with peripheral arterial disease after revascularisation: A Korean nationwide population-based cohort study. Eur. J. Vasc. Endovasc. Surg. 2022. [Google Scholar] [CrossRef]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef]
- Calcaterra, V.; Vandoni, M.; Rossi, V.; Berardo, C.; Grazi, R.; Cordaro, E.; Tranfaglia, V.; Carnevale Pellino, V.; Cereda, C.; Zuccotti, G. Use of Physical Activity and Exercise to Reduce Inflammation in Children and Adolescents with Obesity. Int. J. Environ. Res. Public Health 2022, 19, 6908. [Google Scholar] [CrossRef]
- da Rocha, A.L.; Pinto, A.P.; Kohama, E.B.; Pauli, J.R.; de Moura, L.P.; Cintra, D.E.; Ropelle, E.R.; da Silva, A.S.R. The proinflammatory effects of chronic excessive exercise. Cytokine 2019, 119, 57–61. [Google Scholar] [CrossRef]
- Cheng, A.J.; Jude, B.; Lanner, J.T. Intramuscular mechanisms of overtraining. Redox Biol. 2020, 35, 101480. [Google Scholar] [CrossRef] [PubMed]
- Sahl, R.E.; Andersen, P.R.; Gronbaek, K.; Morville, T.H.; Rosenkilde, M.; Rasmusen, H.K.; Poulsen, S.S.; Prats, C.; Dela, F.; Helge, J.W. Repeated Excessive Exercise Attenuates the Anti-Inflammatory Effects of Exercise in Older Men. Front. Physiol. 2017, 8, 407. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 5840) | Q1 (n = 1462) | Q2 (n = 1465) | Q3 (n = 1461) | Q4 (n = 1452) | p-Value |
|---|---|---|---|---|---|---|
| Age (years) | 59.78 ± 12.96 | 59.16 ± 12.98 | 59.44 ± 13.03 | 60.13 ± 12.92 | 60.4 ± 12.88 | 0.023 |
| Sex, male, n (%) | 3001 (51.39%) | 948 (64.84%) | 794 (54.20%) | 680 (46.54%) | 579 (39.88%) | <0.001 |
| Hypertension, n (%) | 3376 (57.81%) | 796 (54.45%) | 825 (56.31%) | 896 (61.33%) | 859 (59.16%) | 0.001 |
| Diabetes, n (%) | 1013 (17.35%) | 229 (15.66%) | 244 (16.66%) | 274 (18.75%) | 266 (18.32%) | 0.096 |
| MS, n (%) | <0.001 | |||||
| Married/Living with partner | 3895 (66.70%) | 1067 (72.98%) | 1006 (68.67%) | 929 (63.59%) | 893 (61.50%) | |
| Widowed/Divorced/Separated | 1615 (27.65%) | 319 (21.82%) | 373 (25.46%) | 443 (30.32%) | 480 (33.06%) | |
| Never married | 330 (5.65%) | 76 (5.20%) | 86 (5.87%) | 89 (6.09%) | 79 (5.44%) | |
| Education level, n (%) | <0.001 | |||||
| Less than high school | 1875 (32.11%) | 360 (24.62%) | 437 (29.83%) | 498 (34.09%) | 580 (39.94%) | |
| High school diploma or GED | 1376 (23.56%) | 316 (21.61%) | 343 (23.41%) | 344 (23.55%) | 373 (25.69%) | |
| More than high school | 2589 (44.33%) | 786 (53.76%) | 685 (46.76%) | 619 (42.37%) | 499 (34.37%) | |
| Physical activity, n (%) | <0.001 | |||||
| Less than moderate | 2623 (44.91%) | 519 (35.50%) | 612 (41.77%) | 705 (48.25%) | 787 (54.20%) | |
| Moderate | 1839 (31.49%) | 484 (33.11%) | 497 (33.92%) | 439 (30.05%) | 419 (28.86%) | |
| Vigorous | 1378 (23.60%) | 459 (31.40%) | 356 (24.30%) | 317 (21.70%) | 246 (16.94%) | |
| Race, n (%) | <0.001 | |||||
| Mexican American | 1205 (20.63%) | 307 (21.00%) | 299 (20.41%) | 283 (19.37%) | 316 (21.76%) | |
| Non-Hispanic white | 3261 (55.84%) | 873 (59.71%) | 851 (58.09%) | 806 (55.17%) | 731 (50.34%) | |
| Non-Hispanic black | 980 (16.78%) | 180 (12.31%) | 200 (13.65%) | 285 (19.51%) | 315 (21.69%) | |
| Other Hispanic | 228 (3.90%) | 56 (3.83%) | 64 (4.37%) | 52 (3.56%) | 56 (3.86%) | |
| Other races | 166 (2.84%) | 46 (3.15%) | 51 (3.48%) | 35 (2.40%) | 34 (2.34%) | |
| Hypotensive drugs, n (%) | 1531 (26.22%) | 389 (26.61%) | 381 (26.01%) | 406 (27.79%0 | 355 (24.45%) | 0.225 |
| Hypoglycemic drugs, n (%) | 612 (10.48%) | 146 (9.99%) | 144 (9.83%) | 160 (10.95%) | 162 (11.16%) | 0.553 |
| CVD, n (%) | 876 (15.00%) | 198 (13.54%) | 208 (14.20%) | 210 (14.37%) | 260 (17.91%) | 0.004 |
| Smoking, n (%) | <0.001 | |||||
| Never smoker | 2707 (46.35%) | 706 (48.29%) | 689 (47.03%) | 672 (46.00%) | 640 (44.08%) | |
| Past smoker | 2012 (34.45%) | 570 (38.99%) | 498 (33.99%) | 495 (33.88%) | 449 (30.92%) | |
| Current smoker | 1121 (19.20%) | 186 (12.72%) | 278 (18.98%) | 294 (20.12%) | 363 (25.00%) | |
| PIR | 2.80 ± 1.61 | 3.14 ± 1.61 | 2.94 ± 1.61 | 2.68 ± 1.59 | 2.46 ± 1.56 | <0.001 |
| BMI, kg/m2 | 28.43 ± 5.45 | 28.07 ± 5.23 | 28.37 ± 5.40 | 28.66 ± 5.53 | 28.61 ± 5.62 | 0.014 |
| ASBP, mmHg | 131.04 ± 20.66 | 129.13 ± 19.21 | 131.04 ± 20.61 | 132.04 ± 21.33 | 131.98 ± 21.33 | 0.002 |
| ADBP, mmHg | 72.91 ± 12.37 | 73.44 ± 11.68 | 72.75 ± 12.45 | 72.62 ± 13.08 | 72.83 ± 12.23 | 0.267 |
| Total cholesterol, mg/dL | 209.35 ± 41.68 | 207.68 ± 39.01 | 207.16 ± 39.98 | 211.95 ± 44.13 | 210.62 ± 43.24 | 0.009 |
| HDL, mmol/L | 52.69 ± 16.23 | 52.52 ± 16.44 | 52.38 ± 15.72 | 52.83 ± 16.52 | 53.03 ± 16.26 | 0.690 |
| CRP, mg/dL | 0.47 ± 0.87 | 0.38 ± 0.69 | 0.46 ± 0.74 | 0.48 ± 1.03 | 0.58 ± 0.95 | <0.001 |
| eGFR, mL/min/1.73 m2 | 83.61 ± 20.02 | 84.96 ± 18.57 | 83.59 ± 19.80 | 83.00 ± 20.91 | 82.88 ± 20.68 | 0.131 |
| HbA1c, % | 5.77 ± 1.12 | 5.69 ± 1.04 | 5.77 ± 1.17 | 5.80 ± 1.14 | 5.80 ± 1.11 | <0.001 |
| PAD, n (%) | 435 (7.45%) | 70 (4.79%) | 102 (6.96%) | 113 (7.73%) | 150 (10.33%) | <0.001 |
| DII | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Continuous | 1.190 (1.120–1.265) | <0.001 | 1.168 (1.095–1.246) | <0.001 | 1.094 (1.022–1.171) | 0.010 |
| Categorical | ||||||
| Quartile 1 (≤−0.7680) | Reference | Reference | Reference | |||
| Quartile 2 (−0.7680–0.5475) | 1.488 (1.088–2.036) | 0.013 | 1.474 (1.066–2.038) | 0.019 | 1.231 (0.880–1.722) | 0.224 |
| Quartile 3 (0.5475–1.6080) | 1.667 (1.226–2.267) | 0.001 | 1.531 (1.112–2.109) | 0.009 | 1.156 (0.828–1.613) | 0.395 |
| Quartile 4 (>1.6080) | 2.291 (1.708–3.073) | <0.001 | 2.106 (1.546–2.869) | <0.001 | 1.543 (1.116–2.133) | 0.009 |
| DII | ||
|---|---|---|
| r | p-Value | |
| Age | 0.035 | 0.007 |
| PIR | −0.167 | <0.001 |
| ASBP | 0.042 | 0.002 |
| ADBP | −0.013 | 0.333 |
| HDL | 0.01 | 0.437 |
| TC | 0.034 | 0.009 |
| CRP | 0.140 | <0.001 |
| HbA1c | 0.083 | <0.001 |
| eGFR | −0.027 | 0.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, H.; Zhou, J.; Huang, Y.; Feng, X.; Dang, P.; Li, G.; Yuan, Z. A Proinflammatory Diet Is Associated with Higher Risk of Peripheral Artery Disease. Nutrients 2022, 14, 3490. https://doi.org/10.3390/nu14173490
Fan H, Zhou J, Huang Y, Feng X, Dang P, Li G, Yuan Z. A Proinflammatory Diet Is Associated with Higher Risk of Peripheral Artery Disease. Nutrients. 2022; 14(17):3490. https://doi.org/10.3390/nu14173490
Chicago/Turabian StyleFan, Heze, Juan Zhou, Yuzhi Huang, Xueying Feng, Peizhu Dang, Guoliang Li, and Zuyi Yuan. 2022. "A Proinflammatory Diet Is Associated with Higher Risk of Peripheral Artery Disease" Nutrients 14, no. 17: 3490. https://doi.org/10.3390/nu14173490