
Role of Dairy Foods, Fish, White Meat, and Eggs in the Prevention of Colorectal Cancer: A Systematic Review of Observational Studies in 2018–2022


Abstract
:1. Introduction
2. Methods
2.1. Search Strategy

2.2. Review Process and Selection Criteria
2.3. Study Quality Assessment
2.4. Data Extraction
3. Results and Discussion
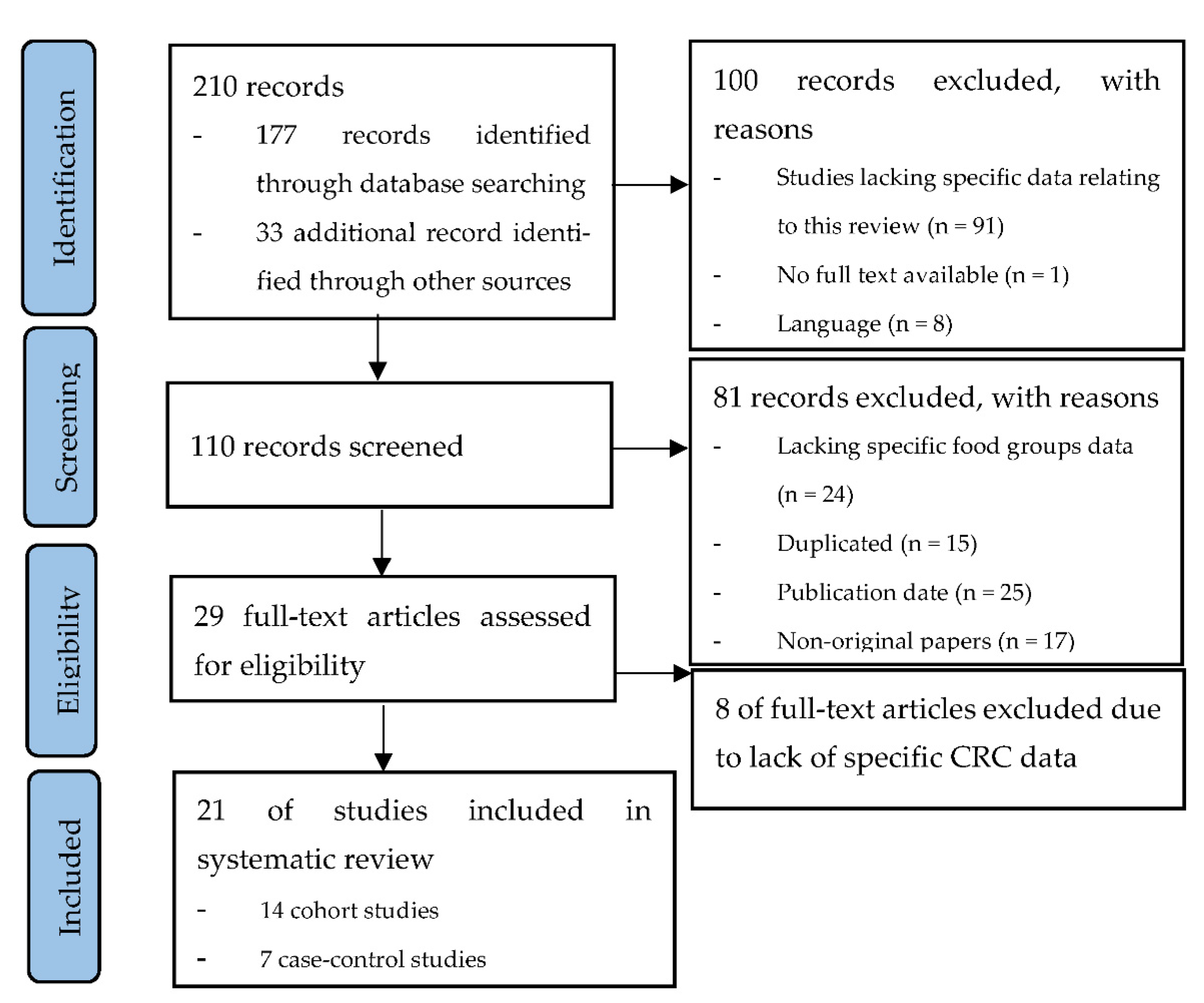
3.1. Study Selection
3.2. Study Characteristics about Milk and Dairy Products
3.3. Dairy Products
3.3.1. Total Dairy Products in Overall and by Fat Content
3.3.2. Total Milk, Whole, and Low-Fat Milk
3.3.3. Yogurt and Other Fermented Dairy Products
3.3.4. Cheese
3.3.5. Other Dairy Products: Butter, Sugary Dairy Products, Cream, and Ice Cream
3.4. Study Characteristics about Fish, White Meat, and Eggs
3.5. Fish, White Meat, and Eggs
3.5.1. Fish
3.5.2. White Meat
3.5.3. Eggs
3.6. Strengths and Limitations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLO-BOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [PubMed]
- Roquette, R.; Painho, M.; Nunes, B. Geographical patterns of the incidence and mortality of colorectal cancer in mainland Portugal municipalities (2007–2011). BMC Cancer 2019, 19, 512. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Levi, F.; Rosato, V.; Bertuccio, P.; Lucchini, F.; Negri, E.; La Vecchia, C. Recent trends in colorectal cancer mortality in Europe. Int. J. Cancer 2011, 129, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Thanikachalam, K.; Khan, G. Colorectal Cancer and Nutrition. Nutrients 2019, 11, 164. [Google Scholar] [CrossRef] [Green Version]
- Kuipers, E.J.; Grady, W.M.; Lieberman, D.; Seufferlein, T.; Sung, J.J.; Boelens, P.G.; van de Velde, C.J.J.; Watanabe, T. Colorectal cancer. Nat. Rev. Dis. Primers 2015, 1, 15065. [Google Scholar] [CrossRef] [Green Version]
- Center, M.M.; Jemal, A.; Smith, R.A.; Ward, E. Worldwide Variations in Colorectal Cancer. CA Cancer J. Clin. 2009, 59, 366–378. [Google Scholar] [CrossRef] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition, Physical Activity and Colorectal Cancer. 2017. Available online: https://www.wcrf.org/sites/default/files/Colorectal-cancer-report.pdf (accessed on 1 May 2022).
- Couto, E.; Boffetta, P.; Lagiou, P.; Ferrari, P.; Buckland, G.; Overvad, K.; Dahm, C.; Tjonneland, A.; Olsen, A.; Clavelchapelon, F.; et al. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br. J. Cancer 2011, 104, 1493–1499. [Google Scholar] [CrossRef] [Green Version]
- Farinetti, A.; Zurlo, V.; Manenti, A.; Coppi, F.; Mattioli, A.V. Mediterranean diet and colorectal cancer: A systematic review. Nutrition 2017, 43–44, 83–88. [Google Scholar] [CrossRef]
- Chartier, L.C.; Howarth, G.S.; Mashtoub, S. Combined nutraceuticals: A novel approach to colitis-associated colorectal cancer? Nutr. Cancer 2019, 71, 199–206. [Google Scholar] [CrossRef]
- Iannone, M.; Mare, R.; Paolino, D.; Gagliardi, A.; Froiio, F.; Cosco, D.; Fresta, M. Characterization and in vitro anticancer properties of chitosan-microencapsulated flavan-3-ols-rich grape seed extracts. Int. J. Biol. Macromol. 2017, 104, 1039–1045. [Google Scholar] [CrossRef]
- Barrubés, L.; Babio, N.; Becerra-Tomás, N.; Rosique-Esteban, N.; Salas-Salvadó, J. Association Between Dairy Product Con-sumption and Colorectal Cancer Risk in Adults: A Systematic Review and Meta-Analysis of Epidemiologic Studies. Adv. Nutr. 2019, 10, S190–S211. [Google Scholar] [CrossRef] [PubMed]
- Spencer, E.A.; Key, T.J.; Appleby, P.N.; Dahm, C.; Keogh, R.H.; Fentiman, I.S.; Akbaraly, T.; Brunner, E.; Burley, V.; Cade, J.; et al. Meat, poultry and fish and risk of colorectal cancer: Pooled analysis of data from the UK dietary cohort consortium. Cancer Causes Control 2010, 21, 1417–1425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Preterre, A.L.; Iqbal, K.; Bechthold, A.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; et al. Food groups and risk of colorectal cancer. Int. J. Cancer 2017, 142, 1748–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietary Guidelines Advisory Committee. 2020. Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services. U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA. Available online: https://www.dietaryguidelines.gov/sites/default/files/2020-07/ScientificReport_of_the_2020DietaryGuidelinesAdvisoryCommittee_first-print.pdf (accessed on 15 June 2022).
- National Health and Medical Research Council 2013. Australian Dietary Guidelines. Canberra: National Health and Medical Research Council. Available online: https://www.eatforhealth.gov.au/sites/default/files/content/n55_australian_dietary_guidelines.pdf (accessed on 15 June 2022).
- Wells, G.A.; Shea, B.; O’Connell, D.; Pereson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa Hospital Research Institute, 2011. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 31 May 2022).
- Bakken, T.; Braaten, T.; Olsen, A.; Hjartåker, A.; Lund, E.; Skeie, G. Milk and risk of colorectal, colon and rectal cancer in the Norwegian Women and Cancer (NOWAC) Cohort Study. Br. J. Nutr. 2018, 119, 1274–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrubés, L.; Babio, N.; Mena-Sánchez, G.; Toledo, E.; Ramírez-Sabio, J.B.; Estruch, R.; Ros, E.; Fitó, M.; Arós, F.; Fiol, M.; et al. PREvención con DIeta MEDiterránea Study Investigators. Dairy product consumption and risk of colorectal cancer in an older mediter-ranean population at high cardiovascular risk. Int. J. Cancer 2018, 143, 1356–1366. [Google Scholar] [CrossRef] [Green Version]
- Vulcan, A.; Ericson, U.; Manjer, J.; Ohlsson, B. A colorectal cancer diet quality index is inversely associated with colorectal cancer in the Malmö diet and cancer study. Eur. J. Cancer Prev. 2019, 28, 463–471. [Google Scholar] [CrossRef]
- Um, C.Y.; Prizment, A.; Hong, C.P.; Lazovich, D.; Bostick, R.M. Associations of Calcium, Vitamin D, and Dairy Product Intakes with Colorectal Cancer Risk among Older Women: The Iowa Women’s Health Study. Nutr. Cancer 2019, 71, 739–748. [Google Scholar] [CrossRef]
- Bradbury, K.E.; Murphy, N.; Key, T.J. Diet and colorectal cancer in UK Biobank: A prospective study. Int. J. Epidemiol. 2019, 49, 246–258. [Google Scholar] [CrossRef] [Green Version]
- Michels, K.B.; Willett, W.C.; Vaidya, R.; Zhang, X.; Giovannucci, E. Yogurt consumption and colorectal cancer incidence and mortality in the Nurses’ Health Study and the Health Professionals Follow-Up Study. Am. J. Clin. Nutr. 2020, 112, 1566–1575. [Google Scholar] [CrossRef]
- Nilsson, L.M.; Winkvist, A.; Esberg, A.; Jansson, J.-H.; Wennberg, P.; van Guelpen, B.; Johansson, I. Dairy Products and Cancer Risk in a Northern Sweden Population. Nutr. Cancer 2020, 72, 409–420. [Google Scholar] [CrossRef] [Green Version]
- Papadimitriou, N.; Bouras, E.; Brandt, P.A.V.D.; Muller, D.C.; Papadopoulou, A.; Heath, A.K.; Critselis, E.; Gunter, M.J.; Vineis, P.; Ferrari, P.; et al. A Prospective Diet-Wide Association Study for Risk of Colorectal Cancer in EPIC. Clin. Gastroenterol. Hepatol. 2021, 20, 864–873.e13. [Google Scholar] [CrossRef] [PubMed]
- Deschasaux-Tanguy, M.; Barrubés Piñol, L.; Sellem, L.; Debras, C.; Srour, B.; Chazelas, E.; Wendeu-Foyet, G.; Hercberg, S.; Galan, P.; Kesse-Guyot, E.; et al. Dairy product consumption and risk of cancer: A short report from the NutriNet-Santé prospective cohort study. Int. J. Cancer 2022, 150, 1978–1986. [Google Scholar] [CrossRef] [PubMed]
- Kakkoura, M.G.; Du, H.; Guo, Y.; Yu, C.; Yang, L.; Pei, P.; Chen, Y.; Sansome, S.; Chan, W.C.; Yang, X.; et al. Dairy consumption and risks of total and site-specific cancers in Chinese adults: An 11-year prospective study of 0.5 million people. BMC Med. 2022, 20, 134. [Google Scholar] [CrossRef] [PubMed]
- Aglago, E.K.; Huybrechts, I.; Murphy, N.; Casagrande, C.; Nicolas, G.; Pischon, T.; Fedirko, V.; Severi, G.; Boutron-Ruault, M.-C.; Fournier, A.; et al. Consumption of Fish and Long-chain n-3 Polyunsaturated Fatty Acids Is Associated With Reduced Risk of Colorectal Cancer in a Large European Cohort. Clin. Gastroenterol. Hepatol. 2020, 18, 654–666.e6. [Google Scholar] [CrossRef]
- Knuppel, A.; Papier, K.; Fensom, G.K.; Appleby, P.N.; A Schmidt, J.; Tong, T.Y.N.; Travis, R.C.; Key, T.J.; Perez-Cornago, A. Meat intake and cancer risk: Prospective analyses in UK Biobank. Int. J. Epidemiol. 2020, 49, 1540–1552. [Google Scholar] [CrossRef]
- Mejborn, H.; Møller, S.P.; Thygesen, L.C.; Biltoft-Jensen, A. Dietary Intake of Red Meat, Processed Meat, and Poultry and Risk of Colorectal Cancer and All-Cause Mortality in the Context of Dietary Guideline Compliance. Nutrients 2020, 13, 32. [Google Scholar] [CrossRef]
- Wang, F.; Chandler, P.D.; Zeleznik, O.A.; Wu, K.; Wu, Y.; Yin, K.; Song, R.; Avila-Pacheco, J.; Clish, C.B.; Meyerhardt, J.A.; et al. Plasma Metabolite Profiles of Red Meat, Poultry, and Fish Consumption, and Their Associations with Colorectal Cancer Risk. Nutrients 2022, 14, 978. [Google Scholar] [CrossRef]
- Alegria-Lertxundi, I.; Aguirre, C.; Bujanda, L.; Fernández, F.J.; Polo, F.; Ordovás, J.M.; Etxezarraga, M.C.; Zabalza, I.; Larzabal, M.; Portillo, I.; et al. Food groups, diet quality and colorectal cancer risk in the Basque Country. World J. Gastroenterol. 2020, 26, 4108–4125. [Google Scholar] [CrossRef]
- Zhang, X.; Fang, Y.J.; Feng, X.L.; Abulimiti, A.; Huang, C.Y.; Luo, H.; Zhang, N.Q.; Chen, Y.M.; Zhang, C.X. Higher intakes of dietary vitamin D, calcium and dairy products are inversely associated with the risk of colorectal cancer: A case-control study in China. Br. J. Nutr. 2020, 123, 699–711. [Google Scholar] [CrossRef]
- Collatuzzo, G.; Seyyedsalehi, M.S.; Rezaeianzadeh, A.; Marzban, M.; Rashidian, H.; Hadji, M.; Kamangar, F.; Etemadi, A.; Pukkala, E.; Zendehdel, K.; et al. Consumption of Yoghurt and Other Dairy Products and Risk of Colorectal Cancer in Iran: The IROPICAN Study. Nutrients 2022, 14, 2506. [Google Scholar] [CrossRef]
- Deoula, M.S.; El Kinany, K.; Huybrechts, I.; Gunter, M.J.; Hatime, Z.; Boudouaya, H.A.; Benslimane, A.; Nejjari, C.; El Abkari, M.; Badre, W.; et al. Consumption of meat, traditional and modern processed meat and colorectal cancer risk among the Moroccan population: A large-scale case-control study. Int. J. Cancer 2020, 146, 1333–1345. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lee, J.; Woo, H.D.; Kim, D.W.; Oh, J.H.; Chang, H.J.; Sohn, D.K.; Shin, A.; Kim, J. Dietary mercury intake and colo-rectal cancer risk: A case-control study. Clin. Nutr. 2020, 39, 2106–2113. [Google Scholar] [CrossRef]
- Shen, W.; Sun, J.; Li, Z.; Yao, F.; Lin, K.; Jiao, X. Food intake and its effect on the species and abundance of intestinal flora in colorectal cancer and healthy individuals. Korean J. Intern. Med. 2021, 36, 568–583. [Google Scholar] [CrossRef] [PubMed]
- Franchi, C.; Ardoino, I.; Bosetti, C.; Negri, E.; Serraino, D.; Crispo, A.; Giacosa, A.; Fattore, E.; Dolci, A.; Bravi, F.; et al. Inverse Association between Canned Fish Consumption and Colorectal Cancer Risk: Analysis of Two Large Case-Control Studies. Nutrients 2022, 14, 1663. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.R.; Abar, L.; Chan, D.S.M.; Vingeliene, S.; Polemiti, E.; Stevens, C.; Greenwood, D.; Norat, T. Foods and beverages and colorectal cancer risk: A systematic review and meta-analysis of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project. Ann. Oncol. 2017, 28, 1788–1802. [Google Scholar] [CrossRef]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Proyect Expert Report 2018. Meat, Fish and Dairy Products and the Risk of Cancer. Available online: https://www.wcrf.org/diet-activity-and-cancer/risk-factors/meat-fish-dairy-and-cancer-risk/ (accessed on 1 June 2022).
- Murphy, N.; Norat, T.; Ferrari, P.; Jenab, M.; Bueno-De-Mesquita, B.; Skeie, G.; Olsen, A.; Tjonneland, A.; Dahm, C.; Overvad, K.; et al. Consumption of Dairy Products and Colorectal Cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC). PLoS ONE 2013, 8, e72715. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.C.; Bergkvist, L.; Wolk, A. High-fat dairy food and conjugated linoleic acid intakes in relation to colorectal cancer incidence in the Swedish Mammography Cohort. Am. J. Clin. Nutr. 2005, 82, 894–900. [Google Scholar] [CrossRef]
- Lee, S.-A.; Shu, X.O.; Yang, G.; Li, H.; Gao, Y.-T.; Zheng, W. Animal Origin Foods and Colorectal Cancer Risk: A Report From the Shanghai Women’s Health Study. Nutr. Cancer 2009, 61, 194–205. [Google Scholar] [CrossRef]
- Park, S.-Y.; Murphy, S.P.; Wilkens, L.R.; Nomura, A.M.; Henderson, B.E.; Kolonel, L.N. Calcium and Vitamin D Intake and Risk of Colorectal Cancer: The Multiethnic Cohort Study. Am. J. Epidemiol. 2007, 165, 784–793. [Google Scholar] [CrossRef]
- Kesse, E.; Boutron-Ruault, M.; Norat, T.; Riboli, E.; Clavel-Chapelon, F. E3N Group Dietary calcium, phosphorus, vitamin D, dairy products and the risk of colorectal adenoma and cancer among French women of the E3N-EPIC prospective study. Int. J. Cancer 2005, 117, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.C.; Bergkvist, L.; Rutegård, J.; Giovannucci, E.; Wolk, A. Calcium and dairy food intakes are inversely associated with colorectal cancer risk in the Cohort of Swedish Men. Am. J. Clin. Nutr. 2006, 83, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Tantamango-Bartley, Y.; Knutsen, S.F.; Jaceldo-Siegl, K.; Fan, J.; Mashchak, A.; Fraser, G.E. Independent associations of dairy and calcium intakes with colorectal cancers in the Adventist Health Study-2 cohort. Public Health Nutr. 2017, 20, 2577–2586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simons, C.C.J.M.; Leurs, L.J.; Weijenberg, M.P.; Schouten, L.J.; Goldbohm, R.A.; van den Brandt, P.A. Fluid Intake and Colorectal Cancer Risk in the Netherlands Cohort Study. Nutr. Cancer 2010, 62, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Frattini, M.; Balestra, D.; Suardi, S.; Oggionni, M.; Alberici, P.; Radice, P.; Costa, A.; Daidone, M.G.; Leo, E.; Pilotti, S.; et al. Different Genetic Features Associated with Colon and Rectal Carcinogenesis. Clin. Cancer Res. 2004, 10, 4015–4021. [Google Scholar] [CrossRef] [Green Version]
- Kapiteijn, E.; Liefers, G.J.; Los, L.C.; Kranenbarg, E.-K.; Hermans, J.; Tollenaar, R.A.; Moriya, Y.; Van De Velde, C.J.; Van Krieken, J.H. Mechanisms of oncogenesis in colon versus rectal cancer. J. Pathol. 2001, 195, 171–178. [Google Scholar] [CrossRef]
- Huncharek, M.; Muscat, J.; Kupelnick, B. Colorectal Cancer Risk and Dietary Intake of Calcium, Vitamin D, and Dairy Products: A Meta-Analysis of 26,335 Cases From 60 Observational Studies. Nutr. Cancer 2009, 61, 47–69. [Google Scholar] [CrossRef]
- Vargas, A.J.; Thompson, P.A. Diet and Nutrient Factors in Colorectal Cancer Risk. Nutr. Clin. Pract. 2012, 27, 613–623. [Google Scholar] [CrossRef]
- Zhang, X.; Keum, N.; Wu, K.; Smith-Warner, S.A.; Ogino, S.; Chan, A.T.; Fuchs, C.S.; Giovannucci, E.L. Calcium intake and colorectal cancer risk: Results from the nurses’ health study and health professionals follow-up study. Int. J. Cancer 2016, 139, 2232–2242. [Google Scholar] [CrossRef] [Green Version]
- Cho, E.; Smith-Warner, S.A.; Spiegelman, D.; Beeson, W.L.; van den Brandt, P.A.; Colditz, G.; Folsom, A.R.; Fraser, G.E.; Freudenheim, J.L.; Giovannucci, E.; et al. Dairy Foods, Calcium, and Colorectal Cancer: A Pooled Analysis of 10 Cohort Studies. J. Natl. Cancer Inst. 2004, 96, 1015–1022, Erratum in: J. Natl. Cancer Inst. 2004, 96, 1724. [Google Scholar] [CrossRef] [Green Version]
- Peters, R.K.; Pike, M.C.; Garabrant, D.; Mack, T.M. Diet and colon cancer in Los Angeles County, California. Cancer Causes Control 1992, 3, 457–473. [Google Scholar] [CrossRef]
- Pala, V.; Sieri, S.; Berrino, F.; Vineis, P.; Sacerdote, C.; Palli, D.; Masala, G.; Panico, S.; Mattiello, A.; Tumino, R.; et al. Yogurt consumption and risk of colorectal cancer in the Italian European prospective investigation into cancer and nutrition cohort. Int. J. Cancer 2011, 129, 2712–2719. [Google Scholar] [CrossRef] [PubMed]
- USDA Agricultural Research Service, Beltsville Human Nutrition Research Center. MyPyramid Equivalents Product Downloads. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/mypyramid-equivalents-product-downloads/ (accessed on 17 October 2021).
- Beydoun, M.A.; Gary, T.L.; Caballero, B.H.; Lawrence, R.S.; Cheskin, L.J.; Wang, Y. Ethnic differences in dairy and related nutrient consumption among US adults and their association with obesity, central obesity, and the metabolic syndrome. Am. J. Clin. Nutr. 2008, 87, 1914–1925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahbandeh, M.U.S. Per Capita Consumption of Yogurt 2000–2018 Statista; 24 September 2019. Available online: https://www.statista.com/statistics/184309/per-capita-consumption-of-yogurt-in-the-us-since-2000/ (accessed on 17 May 2022).
- Trichia, E.; Luben, R.; Khaw, K.T.; Wareham, N.J.; Imamura, F.; Forouhi, N.G. The associations of longitudinal changes in consumption of total and types of dairy products and markers of metabolic risk and adiposity: Findings from the European Investigation into Cancer and Nutrition (EPIC)-Norfolk study, United Kingdom. Am. J. Clin. Nutr. 2020, 111, 1018–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuda, H.; Kozu, T.; Iinuma, G.; Ohashi, Y.; Saito, Y.; Saito, D.; Akasu, T.; Alexander, D.B.; Futakuchi, M.; Fukamachi, K.; et al. Cancer prevention by bovine lactoferrin: From animal studies to human trial. BioMetals 2010, 23, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Alcalá, L.M.; Castro-Gómez, M.P.; Pimentel, L.L.; Fontecha, J. Milk fat components with potential anticancer ac-tivity-a review. Biosci. Rep. 2017, 37, BSR20170705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leeuwendaal, N.K.; Stanton, C.; O’Toole, P.W.; Beresford, T.P. Fermented Foods, Health and the Gut Microbiome. Nutrients 2022, 14, 1527. [Google Scholar] [CrossRef]
- Ou, J.; DeLany, J.P.; Zhang, M.; Sharma, S.; O’Keefe, S.J. Association between low colonic short-chain fatty acids and high bile acids in high colon cancer risk populations. Nutr. Cancer 2012, 64, 34–40. [Google Scholar] [CrossRef]
- Ajouz, H.; Mukherji, D.; Shamseddine, A. Secondary bile acids: An underrecognized cause of colon cancer. World J. Surg. Oncol. 2014, 12, 164. [Google Scholar] [CrossRef] [Green Version]
- Chazelas, E.; Deschasaux, M.; Srour, B.; Kesse-Guyot, E.; Julia, C.; Alles, B.; Druesne-Pecollo, N.; Galan, P.; Hercberg, S.; Latino-Martel, P.; et al. Food additives: Distribution and co-occurrence in 126,000 food products of the French market. Sci. Rep. 2020, 10, 3980. [Google Scholar] [CrossRef] [Green Version]
- Caini, S.; Chioccioli, S.; Pastore, E.; Fontana, M.; Tortora, K.; Caderni, G.; Masala, G. Fish Consumption and Colorectal Cancer Risk: Meta-Analysis of Prospective Epidemiological Studies and Review of Evidence from Animal Studies. Cancers 2022, 14, 640. [Google Scholar] [CrossRef]
- Zhang, C.-J.; Chen, P.-F. High Consumption of Fish Tends to Be Inversely Associated with the Risk of Colorectal Cancer. Clin. Gastroenterol. Hepatol. 2020, 18, 751–753. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Jiang, Y.; Fischer, S.M. Prostaglandin E3 metabolism and cancer. Cancer Lett. 2014, 348, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, B.S. Studies with the azoxymethane-rat preclinical model for assessing colon tumor development and chemoprevention. Environ. Mol. Mutagen. 2004, 44, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Chan, A.T. Environmental Factors, Gut Microbiota, and Colorectal Cancer Prevention. Clin. Gastroenterol. Hepatol. 2019, 17, 275–289. [Google Scholar] [CrossRef] [PubMed]
- Piazzi, G.; Prossomariti, A.; Baldassarre, M.; Montagna, C.; Vitaglione, P.; Fogliano, V.; Biagi, E.; Candela, M.; Brigidi, P.; Balbi, T.; et al. A Mediterranean Diet Mix Has Chemopreventive Effects in a Murine Model of Colorectal Cancer Modulating Apoptosis and the Gut Microbiota. Front. Oncol. 2019, 9, 140. [Google Scholar] [CrossRef] [Green Version]
- Irún, P.; Lanas, A.; Piazuelo, E. Omega-3 Polyunsaturated Fatty Acids and Their Bioactive Metabolites in Gastrointestinal Malignancies Related to Unresolved Inflammation. A Review. Front. Pharmacol. 2019, 10, 852. [Google Scholar] [CrossRef]
- Wennberg, M.; Tornevi, A.; Johansson, I.; Hörnell, A.; Norberg, M.; Bergdahl, I.A. Diet and lifestyle factors associated with fish consumption in men and women: A study of whether gender differences can result in gender-specific confounding. Nutr. J. 2012, 11, 101. [Google Scholar] [CrossRef] [Green Version]
- Tani, S.; Kawauchi, K.; Atsumi, W.; Matsuo, R.; Ashida, T.; Imatake, K.; Suzuki, Y.; Yagi, T.; Takahashi, A.; Matsumoto, N.; et al. Association among daily fish intake, white blood cell count, and healthy lifestyle behaviors in an apparently healthy Japanese population: Implication for the anti-atherosclerotic effect of fish consumption. Heart Vessels 2021, 36, 924–933. [Google Scholar] [CrossRef]
- Zaheer, K. An Updated Review on Chicken Eggs: Production, Consumption, Management Aspects and Nutritional Benefits to Human Health. Food Nutr. Sci. 2015, 6, 1208–1220. [Google Scholar] [CrossRef] [Green Version]
- Rao, A.V.; Rao, L.G. Carotenoids and human health. Pharmacol. Res. 2007, 55, 207–216. [Google Scholar] [CrossRef]
- Lyon, P.; Strippoli, V.; Fang, B.; Cimmino, L. B Vitamins and One-Carbon Metabolism: Implications in Human Health and Disease. Nutrients 2020, 12, 2867. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, A.P.; Gehrke, C.W.; Kuo, K.C.; Ehrlich, M. Reduced genomic 5-methylcytosine content in human colonic neoplasia. Cancer Res. 1988, 48, 1159–1161. [Google Scholar] [PubMed]
- Aune, D.; De Stefani, E.; Ronco, A.L.; Boffetta, P.; Deneo-Pellegrini, H.; Acosta, G.; Mendilaharsu, M. Egg consumption and the risk of cancer: A multisite case-control study in Uruguay. Asian Pac. J. Cancer Prev. 2009, 10, 869–876. [Google Scholar] [PubMed]


{kind=link}
| Study, Year (Ref.) | Study Cohort, Country (Age, y) | No. Participants (M/W) | No. Incident Cases | Follow-Up Length, y | Exposure | HR (95%CI) | Adjustments to HR | NOS Quality Score |
|---|---|---|---|---|---|---|---|---|
| Bakken et al., 2018 [18] | Norway: NOWAC Cohort Study (median, 51) | 81,675 W | 872 CRC (617 CC, 255 RC) | 6 | Total milk: >240 g/day vs. never/seldom | CRC: 0.85 (0.69, 1.05) CC: 0.80 (0.62, 1.03) RC: 0.97 (0.67, 1.42) | Age as the time scale and adjusted for BMI, smoking, processed meat, red meat, hard white cheese, yogurt, fibre from foods, alcohol, and energy intake | 6 |
| Barrubés et al., 2018 [19] | Spain: PREDIMED trial (55–80) | 7216 M&W | 97 CRC | 6 | Total dairy products: 564 g/day vs. 206 g/day | CRC: 0.55 (0.31, 0.99) | Stratified by recruitment centre. Adjusted for the intervention group, sex, age, leisure time PA, smoking status, family history of cancer, education level, history of diabetes, use of aspirin treatment, and cumulative average consumption of vegetables, fruits, legumes, cereals, fish, meat, olive oil and nuts, and alcohol | 7 |
| Whole-fat dairy products: 114 g/day vs. 0 g/day | CRC: 1.01 (0.62, 1.64) | |||||||
| Low-fat dairy products: 495 g/day vs. 67 g/day | CRC: 0.62 (0.36, 1,07) | |||||||
| Total yogurt: 128 g/day vs. 8 g/day | CRC: 0.94 (0.56, 1.59) | |||||||
| Low-fat yogurt: 122 g/day vs. 1 g/day | CRC: 1.06 (0.65, 1.73) | |||||||
| Whole-fat yogurt. 45 g/day vs. 0 g/day | CRC: 0.86 (0.51, 1.46) | |||||||
| Cheese: 44 g/day vs. 11 g/day | CRC: 1.23 (0.74, 2.06) | |||||||
| Total milk: 449 g/day vs. 117 g/day | CRC: 0.63 (0.36, 1.10) | |||||||
| Low-fat milk: 407 g/day vs. 15 g/day | CRC: 0.54 (0.32, 0.92) | |||||||
| Whole milk: 60 g/day vs. 0 g/day | CRC: 1.06 (0.64, 1.75) | |||||||
| Concentrated full-fat dairy products: 45 g/day vs. 11 g/day | CRC: 1.11 (0.66, 1.86) | |||||||
| Sugar-enriched dairy products: 14 g/day vs. 0 g/day | CRC: 0.98 (0.55, 1.75) | |||||||
| Fermented dairy products: 166 g/day vs. 36 g/day | CRC: 0.90 (0.53, 1.53) | |||||||
| Vulcan et al., 2018 [20] | Sweden: Malmö Diet and Cancer Cohort Study (cases, 60,6+/−7,0; non-cases, 58,0+/−7,6) | 10,966/16,955 | 923 CRC (590 CC, 317 RC, 16 SCRC) | 18 | Total dairy products: Q5 vs. Q1 | CRC: 0.77 (0.62, 0.96) CC: 0.81 (0.61, 1.06) RC: 0.66 (0.46, 0.94) | Sex, age, method version, season, total energy, education, PA, and BMI | 6 |
| Um et al., 2019 [21] | USA: Iowa Women’s Health Study (55–69) | 35,221 W | 1731 CRC (971 PCC, 760 DCC) | 26 | Total dairy products: Q5 vs. Q1 | PCC: 0.87 (0.69, 1.10) DCC: 0.69 (0.53, 0.90) | Age, family history of CRC, BMI, smoking, alcohol, PA, HRT use (W), total energy intake, vitamin D, magnesium, fruit and vegetable intake, red and processed meat intake, dietary oxidative balance score, and supplemental calcium | 7 |
| Bradbury et al., 2020 [22] | UK: UK Biobank Cohort Study (40–69) | 219,329/256,252 | 2609 CRC | 5.7 | Milk: ≥300 mL/day vs. never | CRC: 0.93 (0.87, 1.01) | Stratified by age, sex, geographical region, and socio-economic status. Adjusted for education, smoking status, waist circumference, height, PA, alcohol intake, family history of CRC, aspirin or ibuprofen use, use of vitamin D and folate supplements, and for W: parity, menopause, OCA, and HRT use | 6 |
| Cheese: ≥5 times/week vs. <once/week | CRC: 1.09 (0.96, 1.23) | |||||||
| Michels et al. 2020 [23] | USA: NHS and HPFS (mean at baseline: M 52.3 and W 45.7) | 43,269/83,054 | 2666 CCR * (1965 CC, 579 RC) | 26 M, 32 W | Yogurt: never or <1 serving/mo vs. >1 servings/week | CRC: 0.89 (0.80, 1.00) CC: 0.87 (0.76, 0.99) PCC: 0.84 (0.70, 0.99) DCC: 0.91 (0.74, 1.12) RC: 0.95 (0.76, 1.21) | Age, 2-year follow-up cycle, family history of CRC, history of lower gastrointestinal endoscopy, BMI, height, PA, pack-years of smoking before age 30, current multivitamin use, regular aspirin or NSAIDs use, total caloric intake, alcohol consumption, and energy-adjusted intakes of folate, calcium, vitamin D, total fibre, unprocessed red meat, and processed meat, and for W: parity and age at first birth, menopausal status, age at menopause and HRT | 6 |
| Nilsson et al., 2020 [24] | Sweden: VIP and MONICA (25–75) | 53,157/52,734 | 1381 CRC | 20 | Non-fermented milk: Q5 vs. Q1 | CRC (M): 0.87 (0.67, 1.14) CRC (W): 0.88 (0.68, 1.14) | Age, screening year, dairy product category, BMI, civil status, education level, PA in leisure time, smoking status, recruitment cohort (VIP or MONICA), and Qs of fruit and vegetables, alcohol, and energy intake | 8 |
| Fermented milk: Q5 vs. Q1 | CRC (M): 0.98 (0.77, 1.25) CRC (W): 0.90 (0.70, 1.15) | |||||||
| Butter: Q5 vs. Q1 | CRC (M): 0.99 (0.76, 1.28) CRC (W): 0.82 (0.62, 1.08) | |||||||
| Cheese: Q5 vs. Q1 | CRC (M): 0.86 (0.67, 1.10) CRC (W): 0.82 (0.63, 1.07) | |||||||
| Papadimitriou et al., 2021 [25] | Europe: EPIC (35–70) | 112,170/274,622 | 5069 CRC | 14.1 | Milk (standardized continuous variable) | CRC: 0.96 (0.93, 0.99) | Total energy intake, smoking status, BMI, PA, diabetes history, education status, age sex, and recruitment centre | 8 |
| Cheese (standardized continuous variable) | CRC: 0.95 (0.92, 0.99) | |||||||
| Yogurt (standardized continuous variable) | CRC: 0.98 (0.95, 1.01) | |||||||
| Deschasaux-Tanguy et al. 2022 [26] | France: NutriNet-Santé Cohort Study (42.2+/−14.5) | 21,572/79,707 | 182 CRC | 10 | Total dairy products: continuous per 1 serving increment | CRC: 1.05 (0.93, 1.19) | Age, sex, height, BMI, baseline type 2 diabetes, prevalent hypertriglyceridemia, hypercholesterolemia, energy intake without alcohol, sugar intake, sodium intake, fruits and vegetables intake, whole foods, red and processed meat consumption, non-dairy calcium intake, non-dairy SFA intake, alcohol intake, number of 24 h dietary records, smoking status, educational level, PA and family history of cancer | 6 |
| Milk: continuous per 1 serving increment | CRC: 0.92 (0.74, 1.15) | |||||||
| Yogurt: continuous per 1 serving increment | CRC: 0.90 (0.67, 1.19) | |||||||
| Cheese: continuous per 1 serving increment | CRC: 1.10 (0.9, 1.30) | |||||||
| Fromage blanc: continuous per 1 serving increment | CRC: 1.39 (1.09, 1.77) | |||||||
| Fermented dairy products: continuous per 1 serving increment | CRC: 1.10 (0.96, 1.27) | |||||||
| Sugary dairy dessert: continuous per 1 serving increment | CRC: 1.58 (1.01, 2.46) | |||||||
| Kakkoura et al. 2022 [27] | China: China Kadoorie Biobank Study (35–74) | 205,000/295,000 | 3350 CRC | 10.8 | Total dairy products: never/rarely intake | CRC: 1.00 (0.94, 1.06) | Stratified by age-at-risk, sex, and individual regions. Adjusted for education, income, smoking, alcohol consumption, total PA, family history of cancer, fresh fruit consumption, soy consumption, and BMI | 8 |
| Monthly intake | CRC: 1.10 (1.00, 1.21) | |||||||
| Regular intake | CRC: 1.09 (1.01, 1.18) | |||||||
| Per 50 g/day of usual intake | CRC: 1.08 (1.00, 1.17) |
| Study, Year (Ref.) | Country (Age, y) | No. Cases and Endpoint | Sex, No. of Cases (M/W) | No. Controls and Type | Exposure | OR (95% CI) | Adjustments to OR | NOS Quality Score |
|---|---|---|---|---|---|---|---|---|
| Alegria-Lertxundi et al., 2020 [32] | Spain (50–69) | 308 CRC (74 PCC, 234 DCC) | 204/104 | 308 C | Milk/dairy products: T3 vs. T1 | CRC: 1.80 (0.95, 3.42) | Age, sex, BMI, energy intake, physical exercise level, smoking status and intensity of smoking, Deprivation Index, and Predictive Risk Modelling, including all the mean food groups (red and processed meat, fish, eggs, fibre-containing foods, nuts, fat, sweets and added sugar, and alcoholic beverage) | 7 |
| Fresh cheese: T3 vs. T1 | CRC: 0.92 (0.58, 1.46) | |||||||
| Other cheeses: T3 vs. T1 | CRC: 1.87 (1.11, 3.16) | |||||||
| Zhang et al., 2020 [33] | China (30–75) | 2380 CRC (1476 CC, 828 RC, and 76 SCRC) | 1356/102 | 2389 H | Total dairy products: T3 vs. T1 | CRC: 0.32 (0.27, 0.39) CRC (M): 0.30 (0.23, 0.38) CRC (W): 0.36 (0.27, 0.47) CC: 0.31 (0.25, 0.38) RC: 0.35 (0.27, 0.45) | Age, sex, marital status, residence, educational level, occupation, income level, occupational activity, household and recreational PA, smoking status, alcohol drinking, family history of cancer, BMI, total energy intake, vegetable, fruit, red meat, and dietary fibre intake, and for W: age at menarche | 7 |
| Milk, drink vs. not drink | CRC: 0.52 (0.45, 0.59) CRC (M): 0.49 (0.41, 0.59) CRC (W): 0.56 (0.46, 0.88) CC: 0.53 (0.46, 0.62) RC: 0.53 (0.44, 0.64) | |||||||
| Collatuzzo et al., 2022 [34] | Iran (controls, 57.2+/−11.5; cases, 58.6+/−12.4) | 865 CRC a (434 CC, 404 RC) | 497/368 | 3205 C | Total dairy products: T3 vs. T1 | CRC: 1.06 (0.85, 1.32) CC: 1.00 (0.75, 1.34) PCC: 0.98 (0.61, 1.58) DCC: 0.96 (0.62, 1.47) RC: 1.06 (0.78, 1.44) | Sex, age, BMI, smoking, opium, province, aspirin, SES, PA, use of red and processed meat, fat intake, fibre intake | 5 |
| Yogurt: T3 vs. T1 | CRC: 0.96 (0.77, 1.20) CC: 0.78 (0.58, 1.06) PCC: 0.43 (0.27, 0.70) DCC: 0.81 (0.52, 1.26) RC: 1.07 (0.80, 1.45) | |||||||
| Milk: T3 vs. T1 | CRC: 0.98 (0.79, 1.21) CC: 1.06 (0.80, 1.41) PCC: 1.18 (0.74, 1.88) DCC: 1.30 (0.87, 1.96) RC: 0.97 (0.72, 1.31) | |||||||
| Dough: T3 vs. T1 | CRC: 1.26 (0.98, 1.61) CC: 1.15 (0.83, 1.60) PCC: 1.52 (0.88, 2.61) DCC: 1.06 (0.65, 1.73) RC: 1.36 (0.96, 1.91) | |||||||
| Kashk: T3 vs. T1 | CRC: 1.03 (0.81, 1.31) CC: 1.09 (0.79, 1.49) PCC: 0.90 (0.52, 1.58) DCC: 0.91 (0.57, 1.44) RC: 1.01 (0.73, 1.40) | |||||||
| Cheese: T3 vs. T1 | CRC: 1.08 (0.81, 1.44) CC: 1.08 (0.74, 1.56) PCC: 0.78 (0.40, 1.49) DCC: 1.20 (0.70, 2.05) RC: 0.96 (0.63, 1.47) | |||||||
| Cream: T3 vs. T1 | CRC: 1.33 (1.08, 1.64) CC: 1.37 (1.03, 1.81) PCC: 1.68 (1.08, 2.61) DCC: 0.93 (0.60, 1.43) RC: 1.20 (0.90, 1.60) | |||||||
| Ice cream: T3 vs. T1 | CRC: 0.86 (0.62, 1.21) CC: 0.75 (0.48, 1.17) PCC: 1.48 (0.68, 3.22) DCC: 0.44 (0.23, 0.85) RC: 0.98 (0.61, 1.55) | |||||||
| Other milk products: T3 vs. T1 | CRC: 1.00 (0.73, 1.37) CC: 0.99 (0.65, 1.50) PCC: 1.04 (0.53, 2.03) DCC: 1.07 (0.60, 1.92) RC: 0.96 (0.63, 1.47) |
| Food Type | Cohort Studies | Case-Control studies | ||
|---|---|---|---|---|
| No. of Total Studies (Ref.) | No. of Studies (Ref.), Type of Association, Food Subtype a, CRC Overall or Subsites Risk b | No. of Total Studies (Ref.) | No. of Studies (Ref.), Type of Association, Food Subtype a, CRC Overall or Subsites Risk b | |
| Total dairy products in overall | 5 [19,20,21,26,27] | 3 [19,20,21], inverse, CRC | 3 [32,33,34] | 1 [33], inverse, CRC |
| Total dairy products by fat content | 1 [19] | |||
| Total milk in overall | 5 [18,19,22,24,26] | 2 [33,34] | 1 [33], inverse, CRC | |
| Total milk by fat content | 1 [19] | 1 [19], inverse, low-fat milk, CRC | ||
| Yogurt and other fermented dairy products | 4 [19,23,24,26] | 1 [23], inverse, CC | 1 [34] | |
| Cheese | 4 [19,22,24,26] | 1 [26], positive, “fromage blanc”, CRC | 2 [32,34] | 1 [32], positive, high-fat cheese, CRC |
| Other dairy products | 3 [19,24,26] | 1 [26], positive, sugary dairy products, CRC | 1 [34] | 1 [34], positive, cream, CRC, CC, PCC; inverse, ice cream, DCC |
| Study, Year (Ref.) | Study Cohort, Country (Age, y) | No. Participants (M/W) | No. Incident Cases (M/W) | Follow-Up Length, y | Exposure | HR (95%CI) | Adjustments to HR | NOS Quality Score |
|---|---|---|---|---|---|---|---|---|
| Aglago et al., 2020 [28] | EPIC, 10 European countries (cases, 57.3+/−7.9; controls, 51.2+/−9.95) | 142,241/333,919 | 2719/3572 | 14.9 | Total fish and shellfish: Q5 vs. Q1 | CRC: 0.88 (0.80, 0.96) CC: 0.89 (0.79, 1.00) RC: 0.88 (0.75, 1.04) PCC: 0.93 (0.79, 1.11) DCC: 0.89 (0.75, 1.07) | Stratified by age, sex, and centre. Adjusted for BMI, height, PA, smoking, education, and intakes of energy, alcohol, red and processed meat, fibre, and dairy products | 7 |
| Oily fish: Q5 vs. Q1 | CRC: 0.90 (0.82, 0.98) CC: 0.89 (0.80, 0.99) RC: 0.91 (0.78, 1.06) PCC: 0.81 (0.70, 0.95) DCC: 1.03 (0.87, 1.21) | |||||||
| Non-oily fish: Q5 vs. Q1 | CRC: 0.91 (0.83, 1.00) CC: 0.90 (0.80, 1.01) RC: 0.96 (0.82, 1.13) PCC: 0.95 (0.80, 1.12) DCC: 0.85 (0.71, 1.01) | |||||||
| Bradbury et al., 2020 [22] | UK Biobank Cohort Study, UK (40–69) | 219,329/256,252 | 2609 | 5.7 | Total fish: ≥3 times/week vs. <once/week | CRC: 0.95 (0.80, 1.13) | Stratified by age, sex, geographical region, and SES. Adjusted for education, smoking status, waist circumference, height, PA, alcohol intake, family history of CRC, aspirin or ibuprofen use, use of vitamin D and folate supplements and for W: parity, menopause, OCA and HRT use | 6 |
| Poultry: ≥2 times/week vs. never | CRC: 0.96 (0.79, 1.18) | |||||||
| Knuppel et al., 2020 [29] | UK Biobank Cohort Study, UK (37–73) | 218,498/256,498 | 28,955 | 6.9 | Poultry: per 30 g/day | CRC: 1.02 (0.91, 1.14) CC: 1.01 (0.88, 1.15) RC: 1.02 (0.85, 1.24) RC (M): 1.27 (1.00, 1.62) RC (W): 0.72 (0.52, 0.98) | Stratified for sex, age group, region; and adjusted for age, ethnicity, deprivation, qualification, employment, living with a spouse or partner, height, smoking, PA, alcohol intake, total fruit and vegetable intake, estimated cereal fibre intake, BMI, and for W: menopausal status, parity, HRT and OCA use | 7 |
| Mejborn et al., 2021 [30] | The Danish National Survey on Diet and Physical Activity cohort study, Denmark (>50) | 3033/3249 | 127 CRC | 8.7 | Poultry: ≥16 g/day vs. <16 g/day | CRC: 1.62 (1.13, 2.31) | Sex, educational attainment, ethnicity, smoking, PA, alcohol, BMI, and total energy intake | 7 |
| Wang et al., 2022 [31] | NHS, NHSII, and HPFS, USA (M, 40–75; W, 25–42) | 527/4742 | 404 CC, 122 RC | 30 | Total fish: 1 SD, MPS Oily fish: 1 SD, MPS Canned tuna fish: 1 SD, MPS | CRC: OR, 0.86 (0.78, 0.96) CRC: OR, 0.86 (0.77, 0.96) CRC: OR, 0.87 (0.78, 0.97) | BMI, family history of CRC, endoscopy, multivitamin use, aspirin use, smoking, PA, total energy intake, alcohol intake, and modified AHEI (in NHS/HPFS) | 6 |
| Poultry: 1 SD, MPS | CRC: OR, 0.94 (0.85, 1.05) |
| Study, Year (Ref.) | Country (Age, y) | No. Cases and Endpoint | Sex, No. of Cases (M/W) | No. Controls and Type | Exposure | OR (95% CI) | Adjustments to OR | NOS Quality Score |
|---|---|---|---|---|---|---|---|---|
| Deoula et al., 2019 [35] | Morocco (≥18) | 1453 CRC | 716/737 | 1453 C | White meat: >308 g/week vs. ≤308 g/week | CRC: 1.07 (0.96, 1.19) CRC (M): 1.08 (0.92, 1.26) CRC (W): 1.15 (0.93, 1.42) CC: 1.13 (0.97, 1.31) CC (M): 1.13 (0.91, 1.41) CC (W): 1.01 (0.80, 1.26) RC: 1.01 (0.86, 1.18) RC (M): 1.03 (0.82, 1.28) RC (W): 1.08 (0.92, 1.25) | Age, residence, education level, monthly income, PA intensity, smoking status, BMI, NSAIDs, total energy intake, calcium, dietary fibre, family history of CRC, dairy product, fruits, vegetable, fish, and alcohol consumption | 6 |
| Turkey: >51 g/week vs. ≤51 g/week | CRC: 0.89 (0.80, 1.01) CRC (M): 0.94 (0.75, 1.18) CC: 0.92 (0.79, 1.08) CC (M): 0.90 (0.72, 1.13) RC: 0.85 (0.72, 1.01) RC (M): 0.92 (0.79, 1.08) | |||||||
| Poultry: >196 g/week vs. ≤196 g/week | CRC: 1.10 (0.99, 1.23) CRC (M): 1.15 (0.98, 1.35) CRC (W): 1.08 (0.92, 1.26) CC: 1.15 (0.98, 1.34) CC (M): 1.27 (1.01, 1.59) CC (W): 1.10 (0.88, 1.37) RC: 1.05 (0.89, 1.22) RC (M): 1.05 (0.84, 1.31) RC (W): 1.08 (0.86, 1.36) | |||||||
| Kim et al., 2019 [36] | Republic of Korea (cases, 56.6+/−9.7; controls, 56.1+/−9.1) | 923 CRC | 625/298 | 1846 C | Total fish and shellfish: T3 vs. T1 | CRC: 1.04 (0.82, 1.32) CRC (M): 0.99 (0.74, 1.32) CRC (W): 1.25 (0.81, 1.94) | Total energy intake, BMI, first-degree family history of CRC, occupation, educational level, monthly income, marital status, regular exercise, and alcohol consumption | 6 |
| Alegria-Lertxundi et al., 2020 [32] | Spain (50–69) | 308 CRC (234 DCC, 74 PCC) | 204/104 | 308 C | Eggs: T3 vs. T1 | CRC: 1.26 (0.71, 2.23) | Age, sex, BMI, energy intake, physical exercise level, smoking status and intensity of smoking, Deprivation Index, and Predictive Risk Modelling, including all the mean food groups (red and processed meat, fibre-containing foods, nuts, fat, sweets and added sugar, and alcoholic beverage) | 7 |
| Total fish: T3 vs. T1 Oily fish: T3 vs. T1 Non-oily fish: T3 vs. T1 | CRC: 1.25 (0.68, 2.29) CRC: 0.53 (0.27, 0.99) CRC: 1.29 (0.74–2.25) | |||||||
| Shen et al., 2021 [37] | China (cases, 60.3+/−13.4; controls, 59.6+/−12.9) | 100 CRC | 54/46 | 100 C | Eggs: ≥280 g/week vs. <280 g/week | CRC: 0.26 (0.10, 0.69) | Age, BMI | 4 |
| White meat: >500 g/week vs. ≤500 g/week | CRC: 0.86 (0.30, 2.46) | |||||||
| Franchi et al., 2022 [38] | Italy (50–69) | 2419 CRC (727 DCC, 373 PCC) | 1432/987 | 4723 H | Total fish (canned and non-canned) vs. no fish | CRC: 0.69 (0.58, 0.81) | Centre, study, sex, age, BMI, education, family history of CRC, PA at work, smoking habits, alcohol consumption, vegetable and fruit consumption, and energy intake | 5 |
| Non-canned fish vs. no fish | CRC: 0.88 (0.77, 1.00) | |||||||
| Only canned fish vs. no fish | CRC: 0.77 (0.62, 0.97) | |||||||
| Canned fish: ≥2 servings/week vs. <1 serving/week | CRC: 0.86 (0.51, 0.85) CC: 0.66 (0.49, 0.90) RC: 0.65 (0.44, 0.95) | The same as in the previous row plus fish consumption |
| Food Type | Cohort Studies | Case-Control Studies | ||
|---|---|---|---|---|
| No. of Total Studies (Ref.) | No. of Studies (ref.), Type of Association, CRC Overall or Subsites Risk a | No. of Total Studies (Ref.) | No. of Studies (Ref.), Type of Association, CRC Overall or Subsites Risk a | |
| Total fish | 3 [22,28,31] | 2 [28,31], inverse, CRC and CC | 3 [32,36,38] | 1 [38], inverse, CRC |
| Oily fish | 2 [28,31] | 2 [28,31], inverse, CRC, CC, and PCC | 1 [32] | 1 [32], inverse, CRC |
| Non-oily fish | 1 [28] | 1 [28], inverse, CRC, CC, and DCC | 1 [32] | |
| Canned fish | 1 [31] | 1 [31], inverse, CRC | 1 [38] | 1 [38], inverse, CRC |
| White meat | 1 [37] | 1 [35] | ||
| Poultry | 4 [22,29,30,31] | 1 [29], inverse, RC (W); positive, RC (M) | 1 [35] | 1 [35], positive, CC (M) |
| Turkey | 1 [35] | |||
| Egg | 2 [32,37] | 1 [37], inverse, CRC | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alegria-Lertxundi, I.; Bujanda, L.; Arroyo-Izaga, M. Role of Dairy Foods, Fish, White Meat, and Eggs in the Prevention of Colorectal Cancer: A Systematic Review of Observational Studies in 2018–2022. Nutrients 2022, 14, 3430. https://doi.org/10.3390/nu14163430
Alegria-Lertxundi I, Bujanda L, Arroyo-Izaga M. Role of Dairy Foods, Fish, White Meat, and Eggs in the Prevention of Colorectal Cancer: A Systematic Review of Observational Studies in 2018–2022. Nutrients. 2022; 14(16):3430. https://doi.org/10.3390/nu14163430
Chicago/Turabian StyleAlegria-Lertxundi, Iker, Luis Bujanda, and Marta Arroyo-Izaga. 2022. "Role of Dairy Foods, Fish, White Meat, and Eggs in the Prevention of Colorectal Cancer: A Systematic Review of Observational Studies in 2018–2022" Nutrients 14, no. 16: 3430. https://doi.org/10.3390/nu14163430