
Weight Change across Adulthood in Relation to Non-Alcoholic Fatty Liver Disease among Non-Obese Individuals

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
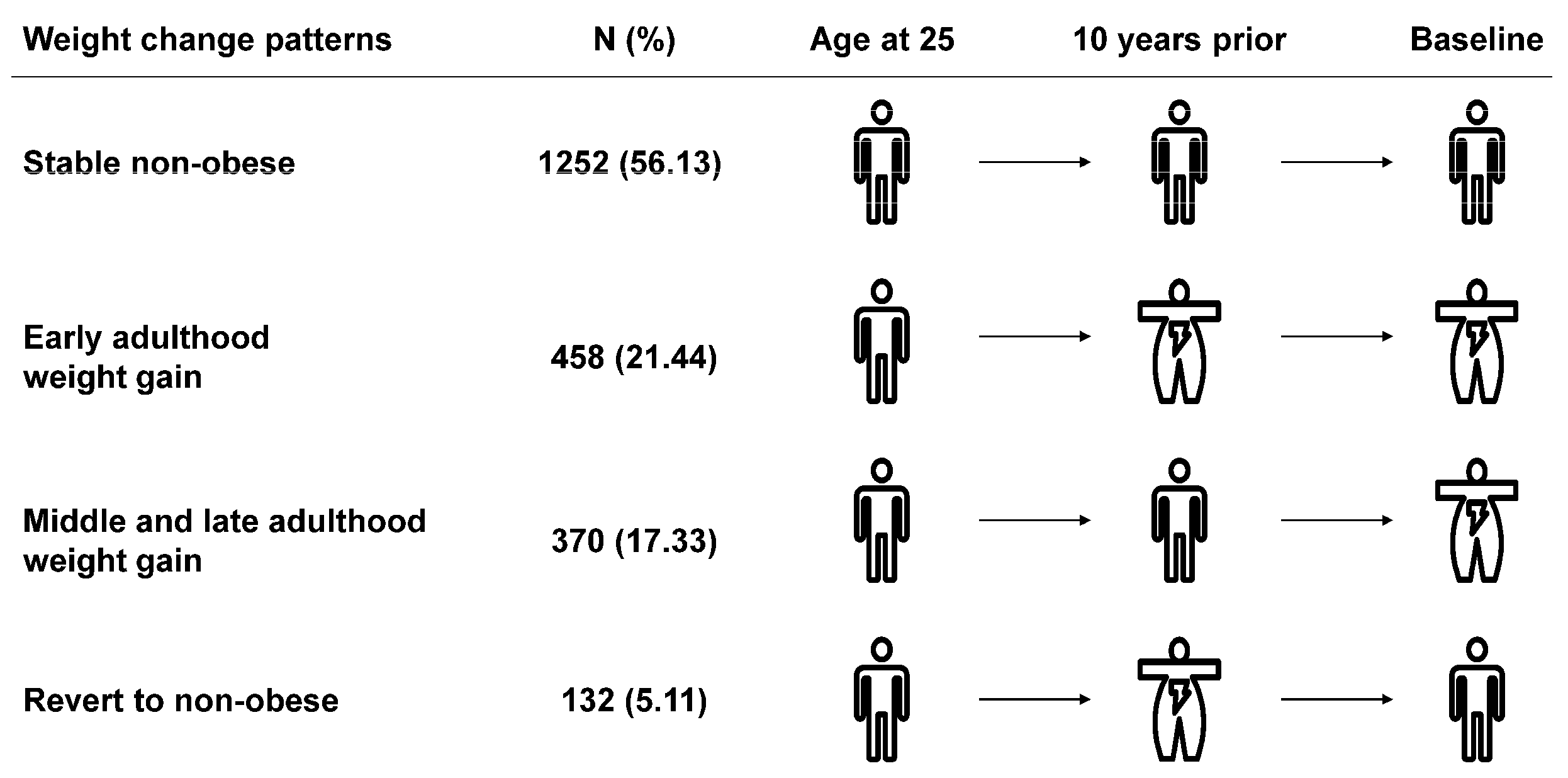
2.2. Measurement of Exposure: Weight Change Patterns
2.3. Measurement of Outcome: Fatty Liver
2.4. Covariates
2.5. Statistical Analysis
2.5.1. Baseline Description
2.5.2. Association Analysis
2.5.3. Calculation of Population Attributable Fraction (PAF)
2.5.4. Sensitivity Analysis
3. Results
3.1. Baseline Characteristics
3.2. Relations of Weight Change Patterns with NAFLD
3.3. Assessment of the Public Health Impact of Weight Change in Populations
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.; Tacke, F.; Arrese, M.; Chander Sharma, B.; Mostafa, I.; Bugianesi, E.; Wai-Sun Wong, V.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.M. Non-alcoholic fatty liver disease—A global public health perspective. J. Hepatol. 2019, 70, 531–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62 (Suppl. S1), S47–S64. [Google Scholar] [CrossRef] [Green Version]
- Adams, L.A.; Anstee, Q.M.; Tilg, H.; Targher, G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut 2017, 66, 1138–1153. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Liu, D.W.; Yan, H.Y.; Wang, Z.Y.; Zhao, S.H.; Wang, B. Obesity is an independent risk factor for non-alcoholic fatty liver disease: Evidence from a meta-analysis of 21 cohort studies. Obes. Rev. 2016, 17, 510–519. [Google Scholar] [CrossRef]
- Williams, C.D.; Stengel, J.; Asike, M.I.; Torres, D.M.; Shaw, J.; Contreras, M.; Landt, C.L.; Harrison, S.A. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: A prospective study. Gastroenterology 2011, 140, 124–131. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Corey, K.E.; Lim, J.K. AGA Clinical Practice Update on Lifestyle Modification Using Diet and Exercise to Achieve Weight Loss in the Management of Nonalcoholic Fatty Liver Disease: Expert Review. Gastroenterology 2021, 160, 912–918. [Google Scholar] [CrossRef]
- Kwon, Y.M.; Oh, S.W.; Hwang, S.S.; Lee, C.; Kwon, H.; Chung, G.E. Association of nonalcoholic fatty liver disease with components of metabolic syndrome according to body mass index in Korean adults. Am. J. Gastroenterol. 2012, 107, 1852–1858. [Google Scholar] [CrossRef]
- Kim, D.; Kim, W.R. Nonobese Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2017, 15, 474–485. [Google Scholar] [CrossRef] [Green Version]
- Yamada, G.; Hagiwara, Y.; Kimura, T.; Takeuchi, Y.; Oba, K.; Masuda, K.; Matsuyama, Y. Impact of Body Weight Gain on the Incidence of Nonalcoholic Fatty Liver Disease in Nonobese Japanese Individuals. Am. J. Gastroenterol. 2021, 116, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Manson, J.E.; Yuan, C.; Liang, M.H.; Grodstein, F.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Associations of Weight Gain From Early to Middle Adulthood with Major Health Outcomes Later in Life. JAMA 2017, 318, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.F.; Leitzmann, M.F.; Ballard-Barbash, R.; Albanes, D.; Harris, T.B.; Hollenbeck, A.; Kipnis, V. Body mass and weight change in adults in relation to mortality risk. Am. J. Epidemiol. 2014, 179, 135–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabbrini, E.; Sullivan, S.; Klein, S. Obesity and nonalcoholic fatty liver disease: Biochemical, metabolic, and clinical implications. Hepatology 2010, 51, 679–689. [Google Scholar] [CrossRef]
- Kim, M.N.; Lo, C.H.; Corey, K.E.; Liu, P.H.; Ma, W.; Zhang, X.; Jovani, M.; Song, M.; Chan, A.T.; Simon, T.G. Weight gain during early adulthood, trajectory of body shape and the risk of nonalcoholic fatty liver disease: A prospective cohort study among women. Metabolism 2020, 113, 154398. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). About the National Health and Nutrition Examination Survey. 2017. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_13_14/NHANES_Overview_Brochure.pdf (accessed on 5 January 2022).
- Stokes, A.; Collins, J.M.; Grant, B.F.; Scamuffa, R.F.; Hsiao, C.W.; Johnston, S.S.; Ammann, E.M.; Manson, J.E.; Preston, S.H. Obesity Progression Between Young Adulthood and Midlife and Incident Diabetes: A Retrospective Cohort Study of U.S. Adults. Diabetes Care 2018, 41, 1025–1031. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Ye, Y.; Zhang, Y.; Pan, X.F.; Pan, A. Weight change across adulthood in relation to all cause and cause specific mortality: Prospective cohort study. BMJ 2019, 367, l5584. [Google Scholar] [CrossRef] [Green Version]
- Karlas, T.; Petroff, D.; Sasso, M.; Fan, J.G.; Mi, Y.Q.; de Ledinghen, V.; Kumar, M.; Lupsor-Platon, M.; Han, K.H.; Cardoso, A.C.; et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. J. Hepatol. 2017, 66, 1022–1030. [Google Scholar] [CrossRef]
- Eddowes, P.J.; Sasso, M.; Allison, M.; Tsochatzis, E.; Anstee, Q.M.; Sheridan, D.; Guha, I.N.; Cobbold, J.F.; Deeks, J.J.; Paradis, V.; et al. Accuracy of FibroScan Controlled Attenuation Parameter and Liver Stiffness Measurement in Assessing Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1717–1730. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Li, X.; Wang, Z.; Bancks, M.P.; Carnethon, M.R.; Greenland, P.; Feng, Y.Q.; Wang, H.; Zhong, V.W. Trends in Prevalence of Diabetes and Control of Risk Factors in Diabetes Among US Adults, 1999–2018. JAMA 2021, 326, 1–13. [Google Scholar] [CrossRef]
- Muntner, P.; Hardy, S.T.; Fine, L.J.; Jaeger, B.C.; Wozniak, G.; Levitan, E.B.; Colantonio, L.D. Trends in Blood Pressure Control Among US Adults with Hypertension, 1999–2000 to 2017–2018. JAMA 2020, 324, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Decker, S.L.; Kostova, D.; Kenney, G.M.; Long, S.K. Health status, risk factors, and medical conditions among persons enrolled in Medicaid vs uninsured low-income adults potentially eligible for Medicaid under the Affordable Care Act. JAMA 2013, 309, 2579–2586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockhill, B.; Newman, B.; Weinberg, C. Use and misuse of population attributable fractions. Am. J. Public Health 1998, 88, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zelber-Sagi, S.; Lotan, R.; Shlomai, A.; Webb, M.; Harrari, G.; Buch, A.; Nitzan Kaluski, D.; Halpern, Z.; Oren, R. Predictors for incidence and remission of NAFLD in the general population during a seven-year prospective follow-up. J. Hepatol. 2012, 56, 1145–1151. [Google Scholar] [CrossRef]
- VanWagner, L.B.; Khan, S.S.; Ning, H.; Siddique, J.; Lewis, C.E.; Carr, J.J.; Vos, M.B.; Speliotes, E.; Terrault, N.A.; Rinella, M.E.; et al. Body mass index trajectories in young adulthood predict non-alcoholic fatty liver disease in middle age: The CARDIA cohort study. Liver Int. 2018, 38, 706–714. [Google Scholar] [CrossRef]
- Du, S.; Wang, C.; Jiang, W.; Li, C.; Li, Y.; Feng, R.; Sun, C. The impact of body weight gain on nonalcoholic fatty liver disease and metabolic syndrome during earlier and later adulthood. Diabetes Res. Clin. Pract. 2016, 116, 183–191. [Google Scholar] [CrossRef]
- Montonen, J.; Boeing, H.; Schleicher, E.; Fritsche, A.; Pischon, T. Association of changes in body mass index during earlier adulthood and later adulthood with circulating obesity biomarker concentrations in middle-aged men and women. Diabetologia 2011, 54, 1676–1683. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Wang, T.; Yin, X.; Sun, Y.; Seow, W.J. Association of Weight Loss from Early to Middle Adulthood and Incident Hypertension Risk Later in Life. Nutrients 2020, 12, 2622. [Google Scholar] [CrossRef]
- Liu, M.; Zhang, Z.; Zhou, C.; He, P.; Zhang, Y.; Li, H.; Li, Q.; Liu, C.; Wang, B.; Li, J.; et al. Relationship of Weight Change Patterns From Young to Middle Adulthood With Incident Cardiovascular Diseases. J. Clin. Endocrinol. Metab. 2021, 106, e812–e823. [Google Scholar] [CrossRef]
- Kvaerner, A.S.; Hang, D.; Giovannucci, E.L.; Willett, W.C.; Chan, A.T.; Song, M. Trajectories of body fatness from age 5 to 60 y and plasma biomarker concentrations of the insulin-insulin-like growth factor system. Am. J. Clin. Nutr. 2018, 108, 388–397. [Google Scholar] [CrossRef]
- Shoelson, S.E.; Herrero, L.; Naaz, A. Obesity, inflammation, and insulin resistance. Gastroenterology 2007, 132, 2169–2180. [Google Scholar] [CrossRef] [PubMed]
- Boden, G.; Shulman, G.I. Free fatty acids in obesity and type 2 diabetes: Defining their role in the development of insulin resistance and beta-cell dysfunction. Eur. J. Clin. Investig. 2002, 32 (Suppl. S3), 14–23. [Google Scholar] [CrossRef] [PubMed]
- Cho, I.Y.; Chang, Y.; Sung, E.; Kang, J.H.; Shin, H.; Wild, S.H.; Byrne, C.D.; Ryu, S. Weight Change and the Development of Nonalcoholic Fatty Liver Disease in Metabolically Healthy Overweight Individuals. Clin. Gastroenterol. Hepatol. 2021, 20, E505–E507. [Google Scholar] [CrossRef]
- Koutoukidis, D.A.; Jebb, S.A.; Tomlinson, J.W.; Cobbold, J.F.; Aveyard, P. Association of Weight Changes With Changes in Histological Features and Blood Markers in Nonalcoholic Steatohepatitis. Clin. Gastroenterol. Hepatol. 2021, 20, E538–E547. [Google Scholar] [CrossRef] [PubMed]
- Koutoukidis, D.A.; Koshiaris, C.; Henry, J.A.; Noreik, M.; Morris, E.; Manoharan, I.; Tudor, K.; Bodenham, E.; Dunnigan, A.; Jebb, S.A.; et al. The effect of the magnitude of weight loss on non-alcoholic fatty liver disease: A systematic review and meta-analysis. Metabolism 2021, 115, 154455. [Google Scholar] [CrossRef] [PubMed]
- De Rubeis, V.; Bayat, S.; Griffith, L.E.; Smith, B.T.; Anderson, L.N. Validity of self-reported recall of anthropometric measures in early life: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 1426–1440. [Google Scholar] [CrossRef]
- Stokes, A.; Ni, Y. Validating a summary measure of weight history for modeling the health consequences of obesity. Ann. Epidemiol. 2016, 26, 821–826.e2. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Weight Change Patterns | |||||
|---|---|---|---|---|---|---|
| Total (n = 2212, 100%) | Stable Non-Obese (n = 1252, 56.13%) | Early Adulthood Weight Gain (n = 458, 21.44%) | Middle and Late Adulthood Weight Gain (n = 370, 17.33%) | Revert to Non-Obese (n = 132, 5.11%) | p Value | |
| Age, years, mean ± SE | 55.74 ± 0.47 | 55.24 ± 0.50 | 58.25 ± 0.90 | 52.58 ± 0.89 | 61.43 ± 1.30 | <0.001 |
| Sex, n (%) | 0.009 | |||||
| Male | 1056 (46.22) | 611 (44.03) | 223 (56.10) | 148 (38.12) | 74 (56.23) | |
| Female | 1156 (53.78) | 641 (55.97) | 235 (43.90) | 222 (61.88) | 58 (43.77) | |
| BMI, kg/m2, mean ± SE | ||||||
| At age 25 years | 22.85 ± 0.12 | 21.77 ± 0.12 | 25.05 ± 0.31 | 23.56 ± 0.21 | 23.17 ± 0.36 | <0.001 |
| 10 years prior | 27.38 ± 0.21 | 24.20 ± 0.07 | 34.65 ± 0.30 | 27.10 ± 0.16 | 33.17 ± 0.66 | <0.001 |
| At baseline | 29.11 ± 0.28 | 25.16 ± 0.14 | 35.95 ± 0.42 | 33.92 ± 0.16 | 27.47 ± 0.24 | <0.001 |
| Absolute weight change from age 25 years old to baseline, kg, mean ± SE | 15.72 ± 0.56 | 7.95 ± 0.42 | 28.66 ± 0.95 | 26.68 ± 0.71 | 9.52 ± 1.42 | <0.001 |
| Waist circumference, cm, mean ± SE | 100.32 ± 0.76 | 90.91 ± 0.40 | 117.87 ± 1.04 | 109.78 ± 0.65 | 98.13 ± 0.84 | <0.001 |
| Race and ethnicity, n (%) | <0.001 | |||||
| Non-Hispanic White | 727 (64.00) | 381 (61.52) | 181 (71.55) | 115 (61.73) | 50 (67.34) | |
| Non-Hispanic Black | 533 (11.03) | 248 (9.24) | 144 (12.39) | 117 (15.93) | 24 (8.42) | |
| Non-Hispanic Asian | 385 (6.90) | 330 (10.49) | 14 (1.16) | 32 (3.63) | 9 (2.58) | |
| Hispanic | 460 (13.54) | 245 (14.29) | 86 (9.14) | 89 (15.41) | 40 (17.44) | |
| Other | 107 (4.53) | 48 (4.46) | 33 (5.76) | 17 (3.30) | 9 (4.23) | |
| Education, n (%) | 0.158 | |||||
| Less than high school | 416 (10.85) | 230 (11.36) | 81 (8.46) | 68 (10.83) | 37 (15.41) | |
| High school or equivalent | 498 (25.63) | 265 (23.55) | 100 (24.34) | 96 (32.51) | 37 (30.64) | |
| College or above | 1293 (63.52) | 754 (65.10) | 277 (67.19) | 205 (56.66) | 57 (53.95) | |
| Family income–poverty ratio level, n (%) | 0.169 | |||||
| 0–1.0 | 303 (10.06) | 159 (9.21) | 63 (7.71) | 65 (15.04) | 16 (11.88) | |
| 1.1–3.0 | 838 (33.00) | 472 (32.40) | 183 (32.10) | 132 (34.18) | 51 (39.15) | |
| >3.0 | 806 (56.94) | 480 (58.39) | 157 (60.19) | 130 (50.78) | 39 (48.97) | |
| Marital status, n (%) | 0.352 | |||||
| Married | 1293 (64.95) | 786 (67.45) | 245 (62.35) | 191 (61.68) | 71 (59.47) | |
| Separated | 581 (23.47) | 286 (21.35) | 154 (27.86) | 103 (24.53) | 38 (24.76) | |
| Never married | 335 (11.58) | 178 (11.20) | 59 (9.80) | 75 (13.78) | 23 (15.77) | |
| Alcohol consumption, n (%) | 0.005 | |||||
| Non-drinker | 747 (27.84) | 428 (29.48) | 167 (27.98) | 97 (18.39) | 55 (41.72) | |
| Low to moderate drinker | 1340 (72.16) | 737 (70.52) | 274 (72.02) | 259 (81.61) | 70 (58.28) | |
| Smoking status, n (%) | 0.113 | |||||
| Never smoker | 1284 (59.21) | 752 (60.44) | 242 (54.74) | 216 (60.30) | 74 (60.85) | |
| Former smoker | 335 (12.71) | 195 (13.05) | 51 (9.45) | 62 (13.19) | 27 (20.90) | |
| Current smoker | 593 (28.08) | 305 (26.51) | 165 (35.81) | 92 (26.50) | 31 (18.25) | |
| Leisure time physical activity level, n (%) | 0.003 | |||||
| 0 times/week | 1199 (45.91) | 633 (41.16) | 275 (49.85) | 207 (54.60) | 84 (51.96) | |
| 1–2 times/week | 707 (38.06) | 421 (38.55) | 135 (40.34) | 122 (36.03) | 29 (29.90) | |
| ≥3 times/week | 304 (16.04) | 196 (20.28) | 48 (9.82) | 41 (9.37) | 19 (18.14) | |
| Healthy eating index score, n (%) | 0.021 | |||||
| Quarter 1 | 381 (20.38) | 174 (15.79) | 106 (25.25) | 76 (27.94) | 25 (23.57) | |
| Quarter 2 | 484 (25.60) | 257 (24.54) | 115 (28.51) | 79 (26.24) | 33 (22.40) | |
| Quarter 3 | 514 (24.30) | 291 (25.85) | 107 (23.95) | 92 (22.67) | 24 (14.58) | |
| Quarter 4 | 667 (29.72) | 422 (33.83) | 108 (22.29) | 99 (23.16) | 38 (39.45) | |
| Chronic diseases, n (%) | ||||||
| Diabetes | 488 (15.31) | 188 (8.254) | 174 (32.15) | 77 (13.46) | 49 (28.35) | <0.001 |
| Hypertension | 1013 (39.03) | 478 (30.92) | 281 (52.56) | 174 (42.63) | 80 (57.13) | <0.001 |
| Dyslipidemia | 812 (34.13) | 433 (31.06) | 202 (44.02) | 120 (30.09) | 57 (39.15) | 0.035 |
| Weight Change Patterns | ||||
|---|---|---|---|---|
| Stable Non-Obese | Early Adulthood Weight Gain | Middle and Late Adulthood Weight Gain | Revert to Non-Obese | |
| Number of NAFLD | 355 | 298 | 226 | 45 |
| Age adjusted incidence rate (%) | 23.82 (19.66, 27.98) | 67.20 (58.75, 75.64) | 54.57 (46.82, 62.31) | 37.40 (27.85, 46.95) |
| Model 1, RR (95% CI) | 1.00 (ref) | 2.77 (2.21, 3.49) | 2.33 (1.78, 3.05) | 1.37 (0.95, 1.98) |
| Model 2, RR (95% CI) | 1.00 (ref) | 2.23 (1.73, 2.88) | 1.98 (1.45, 2.71) | 1.09 (0.70, 1.68) |
| Model 3, RR (95% CI) | 1.00 (ref) | 2.19 (1.64, 2.91) | 1.92 (1.40, 2.62) | 1.01 (0.62, 1.64) |
| Hypothesis | Weight Change Pattern | RR (95% CI) | p Value |
|---|---|---|---|
| Risk raise | Stable non-obese | 1.00 (ref) | |
| Early or middle and late adulthood weight gain | 2.07 (1.60, 2.67) | <0.001 | |
| Risk elimination | Early adulthood weight gain | 1.00 (ref) | |
| Revert to non-obese | 0.48 (0.37, 0.61) | <0.001 |
| Scenario | Definition | PAF (%), 95% CI of Non-Obese Population | PAF (%), 95% CI of Total Population |
|---|---|---|---|
| Weight loss | If those who gained weight from early adulthood could have lost weight in later adulthood (“early adulthood weight gain” group vs. “revert to non-obese” group). | 18.98 (14.18, 22.74) | 16.27 (12.16, 19.50) |
| Weight maintenance | If those who gained weight could have maintained non-obese during adulthood (“early or middle and late adulthood weight gain” group vs. “stable non-obese” group). | 31.18 (22.69, 37.76) | 26.74 (19.45, 32.38) |
| Partial prevention | If the total population maintained non-obese (BMI < 30 kg/m2) across adulthood (“stable non-obese” vs. other counterparts). | 31.10 (21.19, 38.76) | 26.67 (18.17, 33.23) |
| Comprehensive prevention | If the total population had a normal BMI (BMI < 25 kg/m2) across adulthood (“stable normal” vs. other counterparts). | 73.32 (55.03, 82.05) | 73.09 (55.62, 82.93) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, Y.; Xu, X.; Tian, T.; Yu, C.; Ge, X.; Gao, J.; Lu, J.; Ge, Z.; Jiang, T.; Jiang, Y.; et al. Weight Change across Adulthood in Relation to Non-Alcoholic Fatty Liver Disease among Non-Obese Individuals. Nutrients 2022, 14, 2140. https://doi.org/10.3390/nu14102140
Ding Y, Xu X, Tian T, Yu C, Ge X, Gao J, Lu J, Ge Z, Jiang T, Jiang Y, et al. Weight Change across Adulthood in Relation to Non-Alcoholic Fatty Liver Disease among Non-Obese Individuals. Nutrients. 2022; 14(10):2140. https://doi.org/10.3390/nu14102140
Chicago/Turabian StyleDing, Yuqing, Xin Xu, Ting Tian, Chengxiao Yu, Xinyuan Ge, Jiaxin Gao, Jing Lu, Zijun Ge, Tao Jiang, Yue Jiang, and et al. 2022. "Weight Change across Adulthood in Relation to Non-Alcoholic Fatty Liver Disease among Non-Obese Individuals" Nutrients 14, no. 10: 2140. https://doi.org/10.3390/nu14102140