
Anthropometric Measurements, Sociodemographics, and Lifestyle Behaviors among Saudi Adolescents Living in Riyadh Relative to Sex and Activity Energy Expenditure: Findings from the Arab Teens Lifestyle Study 2 (ATLS-2)


Abstract
:1. Introduction
2. Methods
2.1. Ethical Approval
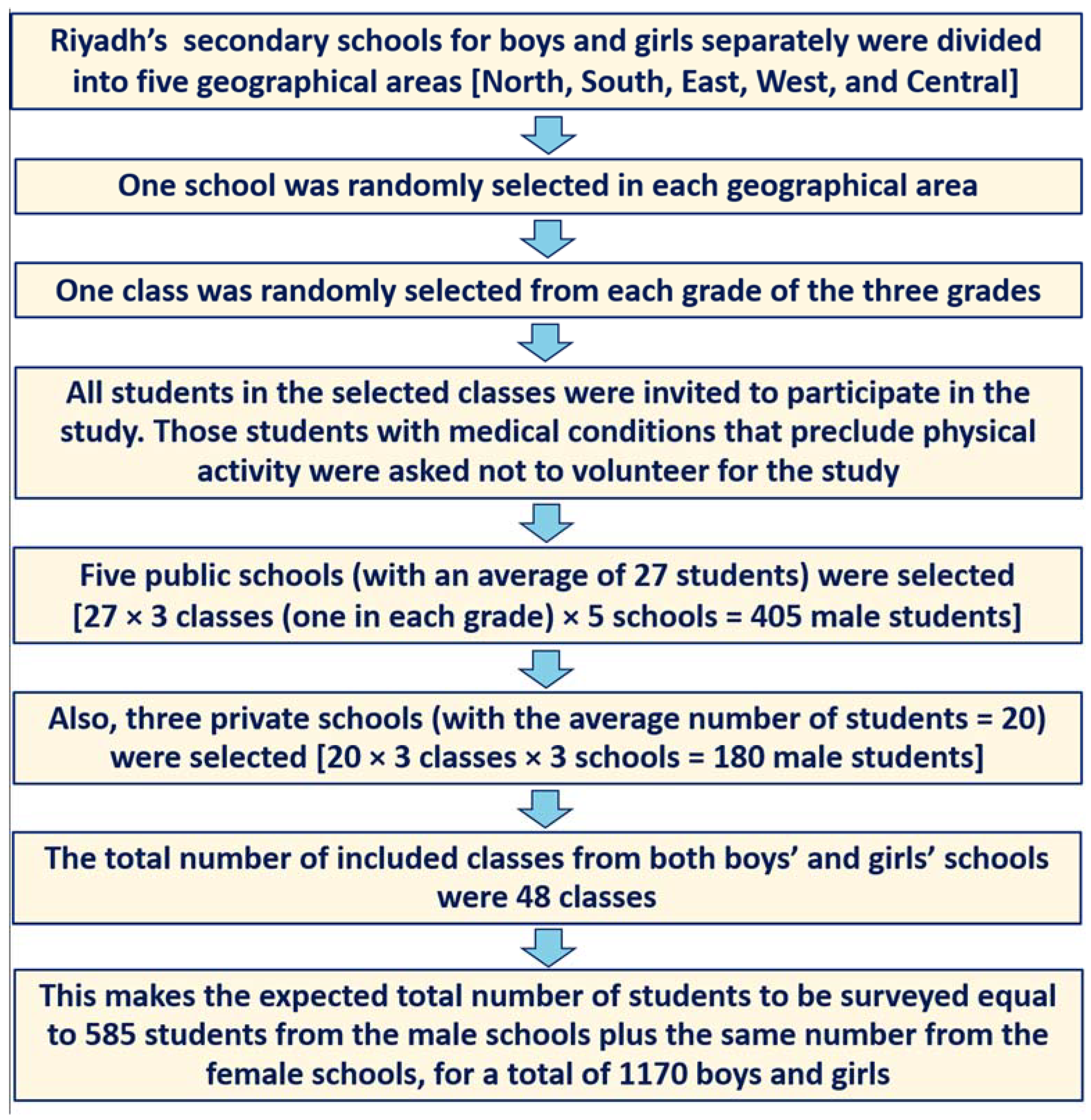
2.2. Participants and Selection Procedures
2.3. Anthropometric Measurements, Demographics, and Socioeconomic Status
2.4. Assessment of Lifestyle Behaviors
2.4.1. Physical Activity
2.4.2. Sedentary Behaviors and Sleep Duration
2.4.3. Dietary Habits
2.5. Data and Statistical Analyses
3. Results
4. Discussion
Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, B.; Robinson, R.; Till, S. Physical activity and health in adolescence. Clin. Med. 2015, 15, 267–272. [Google Scholar] [CrossRef] [Green Version]
- Viner, R.M.; Ross, R.; Hardy, R.; Kuh, D.; Power, C.; Johnson, A.; Wellings, K.; McCambridge, J.; Cole, T.; Kelly, Y.; et al. Life course epidemiology: Recognising the importance of adolescence. J. Epidemiol. Community Health 2015, 69, 719–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallio, P.; Pahkala, K.; Heinonen, O.J.; Tammelin, T.; Hirvensalo, M.; Telama, R.; Juonala, M.; Magnussen, C.G.; Rovio, S.; Helajärvi, H.; et al. Physical inactivity from youth to adulthood and risk of impaired glucose metabolism. Med. Sci. Sports Exerc. 2018, 50, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M. Physical inactivity in Saudi Arabia revisited: A systematic review of inactivity prevalence and perceived barriers to active living. Int. J. Health Sci. 2018, 12, 50–64. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6257875/ (accessed on 15 November 2021).
- Al-Hazzaa, H.M.; Abahussain, N.; Al-Sobayel, H.; Qahwaji, D.; Musaiger, A.O. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 140. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Strategy on Diet, Physical Activity and Health. WHA57.17; WHO: Geneva, Switzerland, 2004; Available online: https://www.who.int/dietphysicalactivity/strategy/eb11344/strategy_english_web.pdf (accessed on 20 October 2021).
- World Health Organization. Global Action Plan on Physical Activity 2018–2030; WHO: Geneva, Switzerland, 2018; pp. 1–101. Available online: http://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf?ua=1 (accessed on 5 September 2021).
- World Health Organization. Saudi Arabia Country Cooperation Strategy 2011–2016; WHO: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/handle/10665/113227 (accessed on 20 October 2021).
- Saudi Arabia Ministry of Health. Transformation Strategy. Available online: https://www.moh.gov.sa/en/Ministry/vro/Documents/Healthcare-Transformation-Strategy.pdf (accessed on 20 October 2021).
- Saudi Vision 2030. National Transformation Program 2020. Available online: http://vision2030.gov.sa/en (accessed on 28 July 2021).
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behavior; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 25 August 2021).
- De Meester, F.; Van Dyck, D.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G. Changes in physical activity during the transition from primary to secondary school in Belgian children: What is the role of the school environment? BMC Public Health 2014, 14, 261. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Brazo-Sayavera, J.; Aubert, S.; Barnes, J.D.; González, S.A.; Tremblay, M.S. Gender differences in physical activity and sedentary behavior: Results from over 200,000 Latin-American children and adolescents. PLoS ONE 2021, 16, e0255353. [Google Scholar] [CrossRef]
- de Looze, M.; Elgar, F.J.; Currie, C.; Kolip, P.; Stevens, G.W.J.M. Gender inequality and sex differences in physical fighting, physical activity, and injury among adolescents across 36 countries. J. Adolesc. Health 2019, 64, 657–663. [Google Scholar] [CrossRef] [Green Version]
- Rosselli, M.; Ermini, E.; Tosi, B.; Boddi, M.; Stefani, L.; Toncelli, L.; Modesti, P.A. Gender differences in barriers to physical activity among adolescents. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1582–1589. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M.; Alahmadi, M.A.; Al-Sobayel, H.I.; Abahussain, N.A.; Qahwaji, D.; Musaiger, A.O. Patterns and determinants of physical activity among Saudi youth. J. Phys. Act. Health 2014, 11, 1202–1211. [Google Scholar] [CrossRef]
- Alsobayel, H.; Al-Hazzaa, H.M.; Abahussain, N.; Qahwaji, D.; Musaiger, A.O. Gender differences in leisure-time versus non-leisure-time physical activity among Saudi adolescents. Ann. Agric. Environ. Med. 2015, 22, 334–348. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M.; Albawardi, N.M. Activity energy expenditure, screen time and dietary habits relative to gender among Saudi youth: Interactions of gender with obesity status and selected lifestyle behaviours. Asia Pac. J. Clin. Nutr. 2019, 28, 389–400. [Google Scholar] [CrossRef]
- AlTamimi, A.A.; Albawardi, N.M.; AlMarzooqi, M.A.; Aljubairi, M.; Al-Hazzaa, H.M. Lifestyle Behaviors and Socio-Demographic Factors Associated with Overweight or Obesity Among Saudi Females Attending Fitness Centers. Diabetes Metab. Syndr. Obes. 2020, 13, 2613–2622. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M.; Albawardi, N.M. Obesity, lifestyle behaviors, and dietary habits of Saudi adolescents living in Riyadh (ATLS-2 project): Revisited after a ten-year period. Life 2021, 11, 1078. [Google Scholar] [CrossRef]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- McCarthy, H.D.; Ashwell, M. A study of central fatness using waist-to-height ratios in UK children and adolescents over two decades supports the simple message—‘Keep your waist circumference to less than half your height’. Int. J. Obes. 2006, 30, 988–992. [Google Scholar] [CrossRef] [Green Version]
- Taylor, R.W.; Jones, I.E.; Williams, S.M.; Goulding, A. Evaluation of waist circumference, waist-to-hip ratio, and the conicity index as screening tools for high trunk fat mass, as measured by dual-energy X-ray absorptiometry, in children aged 3–19 y. Am. J. Clin. Nutr. 2000, 72, 490–495. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M.; Musaiger, A.O.; ATLS Research Group. Arab Teens Lifestyle Study (ATLS): Objectives, design, methodology and implications. Diabetes Metab. Syndr. Obes. 2011, 4, 417–426. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Musaiger, A.O. Convergent validity of the Arab Teens Lifestyle Study (ATLS) physical activity questionnaire. Int. J. Environ. Res. Public Health 2011, 8, 3810–3820. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M.; Al-Ahmadi, M.A. Self-reported questionnaire for the assessment of physical activity in youth 15–25 years: Development, reliability and construct validity. Arab J. Food Nutr. 2003, 4, 279–291. Available online: https://www.researchgate.net/publication/273401034_A_Self-reported_questionnaire_for_the_assessment_of_physical_activity_in_youth_15-25_years_Development_reliability_and_construct_validity (accessed on 4 December 2021).
- Butte, N.F.; Watson, K.B.; Ridley, K.; Zakeri, I.F.; McMurray, R.G.; Pfeiffer, K.A.; Crouter, S.E.; Herrmann, S.D.; Bassett, D.R.; Long, A.; et al. A Youth Compendium of Physical Activities: Activity Codes and Metabolic Intensities. Med. Sci. Sports Exerc. 2018, 50, 246–256. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Carson, V.; Chaput, J.-P.; Gorber, S.C.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–50. Available online: http://www.sleephealthjournal.org/article/S2352-7218%2815%2900015-7/fulltext (accessed on 20 October 2021). [CrossRef] [PubMed]
- Musaiger, A.O.; Bader, Z.; Al-Roomi, K.; D’Souza, R. Dietary and lifestyle habits amongst adolescents in Bahrain. Food Nutr. Res. 2011, 55, 7122. [Google Scholar] [CrossRef] [Green Version]
- Bahathig, A.A.; Abu Saad, H.; Nor Yusop, N.B.; Shukri, N.H.; Essam El-Din, M.M. Relationship between Physical Activity, Sedentary Behavior, and Anthropometric Measurements among Saudi Female Adolescents: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 8461. [Google Scholar] [CrossRef] [PubMed]
- Watson, K.B.; Dai, S.; Paul, P.; Carlson, S.A.; Carroll, D.D.; Fulton, J. The attributable proportion of specific leisure-time physical activities to total leisure activity volume among US adults, National Health and Nutrition Examination Survey 1999–2006. J. Phys. Act Health. 2016, 13, 1192–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jago, R.; Edwards, M.J.; Sebire, S.J.; Bird, E.L.; Tomkinson, K.; Kesten, J.M.; Banfield, K.; May, T.; Cooper, A.R.; Blair, P.S.; et al. Bristol Girls Dance Project: A cluster randomised controlled trial of an after-school dance programme to increase physical activity among 11- to 12-year-old girls. Public Health Res. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Ishii, K.; Shibata, A.; Adachi, M.; Nonoue, K.; Oka, K. Gender and grade differences in objectively measured physical activity and sedentary behavior patterns among Japanese children and adolescents: A cross-sectional study. BMC Public Health 2015, 15, 1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guimarães, R.F.; Mathieu, M.E.; Reid, R.E.R.; Henderson, M.; Barnett, T.A. Physical activity, screen time, and sleep trajectories from childhood to adolescence: The influence of sex and body weight status. J. Phys. Act. Health 2021, 18, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.R.; Goodman, A.; Page, A.S.; Sherar, L.B.; Esliger, D.W.; van Sluijs, E.M.; Andersen, L.B.; Anderssen, S.; Cardon, G.; Davey, R.; et al. Objectively measured physical activity and sedentary time in youth: The International children’s accelerometry database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 113. [Google Scholar] [CrossRef] [Green Version]
- Sirard, J.R.; Pfeiffer, K.A.; Pate, R.R. Motivational factors associated with sports program participation in middle school students. J. Adolesc. Health 2006, 38, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, C.S. Sex-dependent differences in voluntary physical activity. J. NeuroSci. Res. 2017, 95, 279–290. [Google Scholar] [CrossRef] [Green Version]
- Barnekow-Bergkvist, M.; Hedberg, G.; Janlert, U.; Jansson, E. Physical activity pattern in men and women at the ages of 16 and 34 and development of physical activity from adolescence to adulthood. Scand. J. Med. Sci. Sports 1996, 6, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Jabour, A.M.; Rehman, W.; Idrees, S.; Thanganadar, H.; Hira, K.; Alarifi, M.A. The adoption of mobile health applications among University students in health colleges. J. Multidiscip. Healthc. 2021, 14, 1267–1273. [Google Scholar] [CrossRef]
- Pate, R.R.; Flynn, J.I.; Dowda, M. Policies for promotion of physical activity and prevention of obesity in adolescence. J. Exerc. Sci. Fit. 2016, 14, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Schafer, M.; Whitehouse, E. State Policies on Physical Activity in Schools. 2017. Available online: http://knowledgecenter.csg.org/kc/system/files/CR_activity_school.pdf (accessed on 5 September 2021).
- Robinson, L.E.; Wadsworth, D.D.; Webseter, E.K.; Bassett, D.R., Jr. School reform: The role of physical education policy in physical activity of elementary school children in Alabama’s Black Belt region. Am. J. Health Behav. 2014, 28 (Suppl. 3), S72–S76. [Google Scholar] [CrossRef] [PubMed]
- An, R.; Ji, M.; Clarke, C.; Guan, C. Impact of State Laws Governing Physical Education on Attendance Among US High School Students, 2003 to 2017. Am. J. Health Promot. 2019, 33, 1144–1151. [Google Scholar] [CrossRef]
- Sallis, J.F.; Conway, T.L.; Cain, K.L.; Carlson, J.A.; Frank, L.D.; Kerr, J.; Glanz, K.; Chapman, J.E.; Saelens, B.E. Neighborhood built environment and socioeconomic status in relation to physical activity, sedentary behavior, and weight status of adolescents. Prev. Med. 2018, 110, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Rittsteiger, L.; Hinz, T.; Oriwol, D.; Wäsche, H.; Santos-Hövener, C.; Woll, A. Sports participation of children and adolescents in Germany: Disentangling the influence of parental socioeconomic status. BMC Public Health 2021, 21, 1446. [Google Scholar] [CrossRef] [PubMed]
- Gordon-Larsen, P.; Nelson, M.C.; Page, P.; Popkin, B.M. Inequality in the built environment underlies key health disparities in physical activity and obesity. Pediatrics 2006, 117, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobstein, T.; Baur, L.; Uauy, R.; IASO International Obesity Task Force. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, 4–104. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M. Prevalence and trends in obesity among school boys in Central Saudi Arabia between 1988 and 2005. Saudi Med. J. 2007, 28, 1569–1574. Available online: https://www.researchgate.net/publication/5929529_Prevalence_and_trends_in_obesity_among_school_boys_in_Central_Saudi_Arabia_between_1988_and_2005 (accessed on 8 November 2021).
- Moradi-Lakeh, M.; El Bcheraoui, C.; Tuffaha, M.; Daoud, F.; Al Saeedi, M.; Basulaiman, M.; Memish, Z.A.; Al Mazroa, M.A.; Al Rabeeah, A.A.; Mokdad, A.H. The health of Saudi youths: Current challenges and future opportunities. BMC Fam. Pract. 2016, 17, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belcher, B.R.; Berrigan, D.; Dodd, K.W.; Emken, B.A.; Chou, C.P.; Spruijt-Metz, D. Physical activity in US youth: Effect of race/ethnicity, age, gender, and weight status. Med. Sci. Sports Exerc. 2010, 42, 2211–2221. [Google Scholar] [CrossRef] [Green Version]
- Burns, R.D.; Bai, Y.; Fu, Y.; Brusseau, T.A. Associations of adolescent lifestyle behaviors with body mass index within a nationally representative sample of US adolescents: A quantile regression analysis. Public Health 2020, 179, 51–58. [Google Scholar] [CrossRef]
- Riddoch, C.J.; Leary, S.D.; Ness, A.R.; Blair, S.N.; Deere, K.; Mattocks, C.; Griffiths, A.; Smith, G.D.; Tilling, K. Prospective associations between objective measures of physical activity and fat mass in 12–14 year old children: The Avon longitudinal study of parents and children (ALSPAC). BMJ 2009, 339, b4544. [Google Scholar] [CrossRef] [Green Version]
- McMurray, R.G.; Harrell, J.S.; Levine, A.A.; Gansky, S.A. Childhood obesity elevates blood pressure and total cholesterol independent of physical activity. Int. J. Obes. Relat. Metab. Disord. 1995, 19, 881–886. [Google Scholar]
- Amiri, P.; Naseri, P.; Vahedi-Notash, G.; Jalali-Farahani, S.; Mehrabi, Y.; Hamzavi-Zarghani, N.; Azizi, F.; Hadaegh, F.; Khalili, D. Trends of low physical activity among Iranian adolescents across urban and rural areas during 2006–2011. Sci. Rep. 2020, 10, 21318. [Google Scholar] [CrossRef]
- ten Velde, T.G.; Plasqui, G.; Dorenbos, E.; Winkens, B.; Vreugdenhil, A. Objectively measured physical activity and sedentary time in children with overweight, obesity and morbid obesity: A cross-sectional analysis. BMC Public Health 2021, 21, 1558. [Google Scholar] [CrossRef]
- Yang, L.; Cao, C.; Kantor, E.D.; Nguyen, L.H.; Zheng, X.; Park, Y.; Giovannucci, E.L.; Matthews, C.E.; Colditz, G.A.; Cao, Y.; et al. Trends in Sedentary Behavior among the US Population, 2001–2016. JAMA 2019, 321, 1587–1597. [Google Scholar] [CrossRef] [PubMed]
- Dalene, K.E.; Anderssen, S.A.; Andersen, L.B.; Steene-Johannessen, J.; Ekelund, U.; Hansen, B.H.; Kolle, E. Secular and longitudinal physical activity changes in population-based samples of children and adolescents. Scand. J. Med. Sci. Sports 2018, 28, 161–171. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; On Behalf of Sbrn Terminology Consensus Project Participants. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Brage, S.; Froberg, K.; Harro, M.; Anderssen, S.A.; Sardinha, L.B.; Riddoch, C.; Andersen, L.B. TV viewing physical activity are independently associated with metabolic risk in children: The European Youth Heart Study. PLoS Med. 2006, 3, e488. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Colley, R.C.; Saunders, T.J.; Healy, G.N.; Owen, N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gomez, D.; Rey-López, J.P.; Chillón, P.; Gómez-Martínez, S.; Vicente-Rodríguez, G.; Martín-Matillas, M.; Garcia-Fuentes, M.; Delgado, M.; Moreno, L.A.; Veiga, O.L.; et al. Excessive TV viewing and cardiovascular disease risk factors in adolescents. The AVENA cross-sectional study. BMC Public Health 2010, 10, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, K.D.; Howe, L.D.; Basterfield, L.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.K.; Adamson, A.J.; Reilly, J.J.; Janssen, X. Longitudinal study of the associations between change in sedentary behavior and change in adiposity during childhood and adolescence: Gateshead Millennium Study. Int. J. Obes. 2017, 41, 1042–1047. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.; Lee, E.; Rosenbaum, S.; Khan, S.R.; Tremblay, M.S. Dose-dependent and joint associations between screen time, physical activity, and mental wellbeing in adolescents: An international observational study. Lancet Child Adolesc. Health 2021, 5, 729–738. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Abahussain, N.A.; Qahwaji, D.M.; Alahmadi, M.A.; Musaiger, A.O. Association of dietary habits with levels of physical activity and screen time among adolescents living in Saudi Arabia. J. Hum. Nutr. Diet. 2014, 27 (Suppl. 2), 204–213. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Musaiger, A.O.; Abahussain, N.A.; Al-Sobayel, H.I.; Qahwaji, D.M. Lifestyle correlates of self-reported sleep duration among Saudi adolescents: A multicentre school-based cross-sectional study. Child Care Health Dev. 2014, 40, 533–542. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Musaiger, A.O.; Abahussain, N.; Al-Sobayel, H.; Qahwaji, D. Prevalence of short sleep duration and its association with obesity among Saudi adolescents. Ann. Thorac. Med. 2012, 7, 133–139. [Google Scholar] [CrossRef]
- Brand, S.; Gerber, M.; Beck, J.; Hatzinger, M.; Pühse, U.; Holsboer-Trachsler, E. High exercise levels are related to favorable sleep patterns and psychological functioning in adolescents: A comparison of athletes and controls. J. Adolesc. Health 2010, 46, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Foti, K.E.; Eaton, D.K.; Lowry, R.; McKnight-Ely, L.R. Sufficient sleep, physical activity, and sedentary behaviors. Am. J. Prev. Med. 2011, 41, 596–602. [Google Scholar] [CrossRef] [PubMed]
- McKnight-Eily, L.R.; Eaton, D.K.; Lowry, R.; Croft, J.B.; Presley-Cantrell, L.; Perry, G.S. Relationships between hours of sleep and health-risk behaviors in US adolescent students. Prev. Med. 2011, 53, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Labayen, I.; Kwak, L.; Harro, J.; Oja, L.; Veidebaum, T.; Sjöström, M. Sleep duration and activity levels in Estonian and Swedish children and adolescents. Eur. J. Appl. Physiol. 2011, 111, 2615–2623. [Google Scholar] [CrossRef]
- Youngstedt, S.D.; Perlis, M.L.; O’Brien, P.M.; Palmer, C.R.; Smith, M.T.; Orff, H.J.; Kripke, D.F. No association of sleep with total daily physical activity in normal sleepers. Physiol. Behav. 2003, 78, 395–401. [Google Scholar] [CrossRef]
- Kim, Y.; Umeda, M.; Lochbaum, M.; Sloan, R.A. Examining the day-to-day bidirectional associations between physical activity, sedentary behavior, screen time, and sleep health during school days in adolescents. PLoS ONE 2020, 15, e0238721. [Google Scholar] [CrossRef] [PubMed]
- Martinez, S.M.; Tschann, J.M.; McCulloch, C.E.; Sites, E.; Butte, N.F.; Gregorich, S.E.; Penilla, C.; Flores, E.; Pasch, L.; Greenspan, L.; et al. Temporal associations between circadian sleep and activity patterns in Mexican American children. Sleep Health 2019, 5, 201–207. [Google Scholar] [CrossRef]
- Youngstedt, S.D. Effects of exercise on sleep. Clin. Sports Med. 2005, 24, 355–365. [Google Scholar] [CrossRef]


{kind=link}
| Variable | All n = 1261 | Male n = 660 | Female n = 601 | p-Value * |
|---|---|---|---|---|
| Age (year) | 16.4 ± 0.95 | 16.4 ± 0.94 | 16.3 ± 0.96 | 0.050 |
| Body weight (kg) | 65.6 ± 20.9 | 73.2 ± 23.1 | 57.3 ± 14.3 | <0.001 |
| Body height (cm) | 163.6 ± 8.9 | 169.7 ± 6.8 | 157.0 ± 5.5 | <0.001 |
| Body mass index (kg/m2) | 24.3 ± 6.6 | 25.3 ± 7.4 | 23.2 ± 5.4 | <0.001 |
| Waist circumference (cm) | 77.5 ± 16.5 | 83.6 ± 17.5 | 70.7 ± 12.4 | <0.001 |
| Waist-to-height ratio (W/Ht-R (%)) | 0.47 ± 0.09 | 0.49 ± 0.09 | 0.45 ± 0.08 | <0.001 |
| Body shape index ** | 0.73 ± 0.07 | 0.75 ± 0.06 | 0.70 ± 0.06 | <0.001 |
| Overweight + obesity (%) *** | 40.5 | 47.3 | 32.8 | <0.001 |
| School type (%) | 0.001 | |||
| Public | 74.9 | 78.8 | 70.5 | |
| Private | 25.1 | 21.2 | 29.5 | |
| Father’s education (%) | 0.038 | |||
| Intermediate or less (≤9 years) | 14.3 | 16.7 | 11.6 | |
| High school | 28.2 | 28.9 | 27.4 | |
| University degree | 40.9 | 38.0 | 44.1 | |
| Postgraduate degree | 16.6 | 16.4 | 16.9 | |
| Mother’s education (%) | 0.584 | |||
| Intermediate or less (≤9 years) | 21.5 | 20.0 | 23.0 | |
| High school | 29.2 | 29.7 | 28.7 | |
| University degree | 39.1 | 39.4 | 38.7 | |
| Postgraduate degree | 10.2 | 10.9 | 9.6 | |
| Family income (%) **** | <0.001 | |||
| SAR 10,000 or less | 17.4 | 20.2 | 13.9 | |
| SAR 10,001–20,000 | 42.2 | 48.1 | 34.9 | |
| SAR 20,001–30,000 | 16.4 | 16.4 | 24.3 | |
| SAR 30,001+ | 20.5 | 15.3 | 26.9 |
| Variable | Criterion * | Proportion (%) | p-Value ** | ||
|---|---|---|---|---|---|
| All | Male | Female | |||
| Overweight or obesity | BMI > cut-offs | 40.5 | 47.3 | 32.8 | <0.001 |
| Abdominal obesity (W/Ht-R) | >0.50 | 31.7 | 40.9 | 21.4 | <0.001 |
| Screen time | >2 h/day | 89.7 | 89.0 | 90.5 | 0.363 |
| >3 h/day | 80.6 | 79.0 | 82.4 | 0.128 | |
| Nocturnal sleep duration | <8 h/night | 69.1 | 73.6 | 64.3 | <0.001 |
| PA in Metabolic equivalent | <1680 METs-min/week | 53.4 | 58.0 | 48.5 | 0.001 |
| <2520 METs-min/week | 66.8 | 69.8 | 63.4 | 0.004 | |
| Breakfast intake at home | Non-daily | 65.7 | 66.6 | 64.7 | 0.492 |
| Vegetable intake | Non-daily | 73.2 | 75.2 | 71.0 | 0.097 |
| Fruit intake | Non-daily | 84.2 | 84.1 | 84.2 | 0.970 |
| Milk/dairy products | Non-daily | 62.4 | 61.7 | 63.1 | 0.624 |
| Sugar sweetened drink intake | ≥3 day/week | 57.5 | 62.5 | 52.1 | 0.001 |
| Fast food intake | ≥3 day/week | 48.6 | 52.0 | 44.4 | 0.013 |
| French fries/potato chips intake | ≥3 day/week | 44.5 | 42.7 | 46.6 | 0.225 |
| Cake/donuts intake | ≥3 day/week | 40.6 | 37.4 | 44.1 | 0.039 |
| Chocolates/candy intake | ≥3 day/week | 56.0 | 50.4 | 62.2 | <0.001 |
| Variable | All (n = 1189) | Male (n = 591) | Female (n = 598) | p Value * |
|---|---|---|---|---|
| Walking (METs-min/week) | 350.9 ± 14.8 | 334.9 ± 20.3 | 366.6 ± 21.6 | 0.286 |
| Stair Stepping (METs-min/week) | 86.6 ± 0.93 | 85.3 ± 1.4 | 87.9 ± 1.3 | 0.145 |
| Jogging (METs-min/week) | 363.0 ± 20.9 | 409.7 ± 32.3 | 317.1 ± 26.8 | 0.027 |
| Cycling (METs-min/week) | 64.0 ± 7.0 | 89.7 ± 12.9 | 38.7 ± 5.6 | <0.001 |
| Swimming (METs-min/week) | 119.4 ± 11.8 | 149.5 ± 20.1 | 89.7 ± 12.6 | 0.012 |
| Martial art (METs-min/week) | 39.5 ± 7.2 | 25.7 ± 9.6 | 53.1 ± 10.7 | 0.057 |
| Resistance training (METs-min/week) | 101.3 ± 10.7 | 113.8 ± 17.5 | 88.9 ± 12.3 | 0.244 |
| Household (METs-min/week) | 275.4 ± 14.7 | 198.3 ± 16.4 | 351.2 ± 23.9 | <0.001 |
| Dancing (METs-min/week) | 351.7 ± 21.8 | 15.2 ± 4.5 | 700.5 ± 39.0 | <0.001 |
| Moderate-intensity sports (METs-min/week) | 155.2 ± 10.6 | 206.3 ± 18.2 | 104.9 ± 10.9 | <0.001 |
| Vigorous-intensity sports (METs-min/week) | 498.0 ± 29.7 | 735.5 ± 51.6 | 264.6 ± 26.9 | <0.001 |
| Sum of all moderate-intensity physical activity (min/week) | 298.1 ± 8.8 | 218.4 ± 9.5 | 376.6 ± 14.0 | <0.001 |
| Sum of all vigorous-intensity physical activity (min/week) | 169.3 ± 6.6 | 213.7 ± 10.9 | 125.6 ± 7.1 | <0.001 |
| METs-min/week from moderate-intensity physical activity ** | 1134.1 ± 35.2 | 756.2 ± 33.4 | 1520.1 ± 58.0 | <0.001 |
| METs-min/week from vigorous-intensity physical activity *** | 1271.8 ± 49.3 | 1609.2 ± 81.5 | 936.4 ± 52.5 | <0.001 |
| METs-min/week from total physical activity | 2406.3 ± 67.0 | 2365.4 ± 99.3 | 2456.8 ± 90.3 | 0.463 |
| Activity levels (%): Low (<1680 METS-min/week) | 53.4 | 58.0 | 48.5 | 0.004 |
| Moderate (1680–2519 METs-min/week) | 13.4 | 11.8 | 14.9 | |
| High (≥2520 METs-min/week) | 33.3 | 30.2 | 36.6 |
| Variable | Activity Energy Expenditure Levels | p-Value * | |
|---|---|---|---|
| Low Active (<1680 METs-min/week) | High Active (≥1680 METs-min/week) | ||
| School type (%) | 0.514 | ||
| Public | 53.9 | 46.1 | |
| Private | 51.8 | 48.2 | |
| Father’s education (%) | 0.071 | ||
| Intermediate or less | 15.1 | 14.1 | |
| High school | 26.5 | 30.3 | |
| University degree | 43.2 | 36.9 | |
| Postgraduate degree | 15.1 | 18.8 | |
| Mother’s education (%) | 0.510 | ||
| Intermediate or less | 20.9 | 23.0 | |
| High school | 30.8 | 27.7 | |
| University degree | 38.9 | 38.3 | |
| Postgraduate degree | 9.5 | 11.0 | |
| Family income (%) ** | 0.834 | ||
| SAR 10,000 or less | 17.3 | 18.1 | |
| SAR 10,001–20,000 | 42.9 | 40.4 | |
| SAR 20,001–30,000 | 20.0 | 19.9 | |
| SAR 30,001+ | 19.8 | 21.5 | |
| Overweight or obesity (%) | 0.354 | ||
| Non-overweight/non-obesity | 58.7 | 61.3 | |
| Overweight/obesity | 41.3 | 38.7 | |
| Screen time (%) | 0.239 | ||
| ≤3 h/day | 18.5 | 21.2 | |
| >3 h/day | 80.5 | 78.8 | |
| Sleep duration | 0.681 | ||
| <8 h/night | 68.6 | 69.7 | |
| ≥8 h/night | 31.4 | 30.3 | |
| Breakfast intake (%) | <0.001 | ||
| Non-daily intake | 70.7 | 60.0 | |
| Daily intake | 29.3 | 40.0 | |
| Vegetable intake (%) | <0.001 | ||
| Non-daily intake | 78.5 | 66.8 | |
| Daily intake | 21.5 | 33.2 | |
| Fruit intake (%) | 0.001 | ||
| Non-daily intake | 87.3 | 80.2 | |
| Daily intake | 12.7 | 19.8 | |
| Milk/dairy products intake (%) | 0.095 | ||
| Non-daily intake | 64.4 | 59.8 | |
| Daily intake | 35.6 | 40.2 | |
| Sugar sweetened drink intake (%) | 0.089 | ||
| 1–2 days/week | 39.8 | 46.0 | |
| 3–4 days/week | 22.3 | 19.2 | |
| 5+ days/week | 37.9 | 34.8 | |
| Fast food intake (%) | 0.537 | ||
| 1–2 days/week | 51.3 | 52.4 | |
| 3–4 days/week | 27.5 | 28.8 | |
| 5+ days/week | 21.2 | 18.8 | |
| French fries/potato chips intake (%) | 0.674 | ||
| 1–2 days/week | 54.4 | 56.8 | |
| 3–4 days/week | 24.6 | 22.9 | |
| 5+ days/week | 21.0 | 20.3 | |
| Cake/donuts intake (%) | 0.414 | ||
| 1–2 days/week | 60.6 | 57.7 | |
| 3–4 days/week | 19.9 | 19.7 | |
| 5+ days/week | 19.5 | 22.6 | |
| Chocolates/candy intake (%) | 0.086 | ||
| 1–2 days/week | 46.4 | 40.9 | |
| 3–4 days/week | 22.6 | 22.6 | |
| 5+ days/week | 31.0 | 36.5 | |
| Variable | Sex | Activity Levels (n = 1108) | p-Value * | |
|---|---|---|---|---|
| Low Active | High Active | |||
| Age (years) | Male | 16.4 ± 0.94 | 16.3 ± 0.95 | Activity levels: 0.493 Gender: 0.336 Activity levels by gender interaction: 0.995 |
| Female | 16.4 ± 0.98 | 16.4 ± 0.91 | ||
| All | 16.4 ± 0.96 | 16.3 ± 0.93 | ||
| Body weight (kg) | Male | 73.5 ± 23.2 | 71.3 ± 21.4 | Activity levels: 0.988 Gender: <0.001 Activity levels by gender interaction: 0.052 |
| Female | 56.0 ± 13.4 | 58.1 ± 14.8 | ||
| All | 65.4 ± 21.3 | 64.2 ± 19.3 | ||
| BMI (kg/m2) | Male | 25.4 ± 7.5 | 24.7 ± 6.9 | Activity levels: 0.868 Gender: <0.001 Activity levels by gender interaction: 0.077 |
| Female | 22.7 ± 5.2 | 23.5 ± 5.5 | ||
| All | 24.1 ± 6.6 | 24.1 ± 6.2 | ||
| Waist circumference (cm) | Male | 83.8 ± 18.3 | 82.7 ± 15.9 | Activity levels: 0.647 Gender: <0.001 Activity levels by gender interaction: 0.466 |
| Female | 70.5 ± 13.2 | 70.8 ± 12.0 | ||
| All | 77.6 ± 17.4 | 76.3 ± 15.1 | ||
| Body shape index | Male | 0.7 ± 0.07 | 0.75 ± 0.05 | Activity levels: 0.247 Gender: <0.001 Activity levels by gender interaction: 0.029 |
| Female | 0.71 ± 0.7 | 0.69 ± 0.06 | ||
| All | 0.73 ± 0.07 | 0.72 ± 0.6 | ||
| Screen time (hours/day) | Male | 5.2 ± 2.4 | 4.9 ± 2.6 | Activity levels: 0.418 Gender: <0.001 Activity levels by gender interaction: 0.309 |
| Female | 5.7 ± 2.7 | 5.7 ± 2.9 | ||
| All | 5.4 ± 2.5 | 5.3 ± 2.8 | ||
| Sleep duration (hours/night) | Male | 7.1 ± 1.6 | 6.9 ± 1.5 | Activity levels: 0.096 Gender: <0.001 Activity levels by gender interaction: 0.551 |
| Female | 7.5 ± 1.7 | 7.4 ± 1.8 | ||
| All | 7.3 ± 1.7 | 7.1 ± 1.7 | ||
| Breakfast intake (day/week) | Male | 3.58 ± 2.7 | 4.32 ± 2.7 | Activity levels: <0.001 Gender: 0.300 Activity levels by gender interaction: 0.308 |
| Female | 3.57 ± 2.9 | 3.97 ± 2.9 | ||
| All | 3.58 ± 2.8 | 4.13 ± 2.8 | ||
| Vegetable intake (day/week) | Male | 3.57 ± 2.3 | 4.48 ± 2.3 | Activity levels: <0.001 Gender: 0.386 Activity levels by gender interaction: 0.792 |
| Female | 3.48 ± 2.5 | 4.30 ± 2.5 | ||
| All | 3.53 ± 2.4 | 4.38 ± 2.4 | ||
| Fruit intake (day/week) | Male | 2.97 ± 2.3 | 3.64 ± 2.3 | Activity levels: <0.001 Gender: 0.043 Activity levels by gender interaction: 0.484 |
| Female | 2.60 ± 2.2 | 3.46 ± 2.4 | ||
| All | 2.80 ± 2.3 | 3.54 ± 2.3 | ||
| Milk/dairy products intake (day/week) | Male | 4.37 ± 2.5 | 4.91 ± 2.3 | Activity levels: 0.019 Gender: 0.001 Activity levels by gender interaction: 0.256 |
| Female | 4.04 ± 2.6 | 4.24 ± 2.8 | ||
| All | 4.21 ± 2.6 | 4.55 ± 2.6 | ||
| Sugar sweetened drink intake (day/week) | Male | 3.8 ± 2.5 | 3.53 ± 2.5 | Activity levels: 0.173 Gender: 0.016 Activity levels by gender interaction: 0.666 |
| Female | 3.37 ± 2.5 | 3.20 ± 2.6 | ||
| All | 3.60 ± 2.5 | 3.36 ± 2.5 | ||
| Fast food intake (day/week) | Male | 2.88 ± 1.9 | 2.94 ± 1.9 | Activity levels: 0.436 Gender: 0.275 Activity levels by gender interaction: 0.196 |
| Female | 2.89 ± 1.9 | 2.63 ± 1.9 | ||
| All | 2.89 ± 1.9 | 2.77 ± 1.9 | ||
| French fries/potato chips intake (day/week) | Male | 2.52 ± 1.9 | 2.46 ± 2.0 | Activity levels: 0.344 Gender: 0.003 Activity levels by gender interaction: 0.636 |
| Female | 2.94 ± 2.0 | 2.76 ± 2.1 | ||
| All | 2.72 ± 2.0 | 2.62 ± 2.1 | ||
| Cake/donuts intake (day/week) | Male | 2.22 ± 2.0 | 2.30 ± 2.1 | Activity levels: 0.187 Gender: <0.001 Activity levels by gender interaction: 0.506 |
| Female | 2.71 ± 2.1 | 2.95 ± 2.2 | ||
| All | 2.45 ± 2.1 | 2.65 ± 2.2 | ||
| Chocolates/candy intake (day/week) | Male | 2.8 ± 2.1 | 3.10 ± 2.2 | Activity levels: 0.064 Gender: <0.001 Activity levels by gender interaction: 0.851 |
| Female | 3.68 ± 2.4 | 3.91 ± 2.5 | ||
| All | 3.22 ± 2.3 | 3.53 ± 2.4 | ||
| Variable | High Versus Low Active * | |||
|---|---|---|---|---|
| aOR | (95% CI) | SEE | p-Value | |
| Age (younger age = ref) | 0.947 | 0.8–251.087 | 0.071 | 0.439 |
| Sex (female = ref) | 0.763 | 0.577–1.009 | 0.143 | 0.058 |
| Father education (low education = ref) | 1.022 | 0.865–1.208 | 0.085 | 0.797 |
| Mother education (low education = ref) | 0.966 | 0.818–1.141 | 0.085 | 0.686 |
| Family income (low income = ref) | 0.965 | 0.834–1.116 | 0.074 | 0.628 |
| Overweight or obesity (Overweight/obesity = ref) | 1.00 | |||
| Non-overweight/non-obesity | 1.069 | 0.733–1.559 | 0.192 | 0.728 |
| Waist-to-height ratio (<0.50 = ref) | 1.00 | |||
| ≥0.50 | 1.195 | 0.798–1.790 | 0.206 | 0.386 |
| Screen time (low screen time = ref) | 1.00 | |||
| High screen time | 1.145 | 0.823–1.593 | 0.168 | 0.421 |
| Sleep duration (insufficient sleep = ref) | 1.00 | |||
| Sufficient sleep | 1.141 | 0.856–1.520 | 0.146 | 0.368 |
| Breakfast intake (daily intake = ref) | 1.00 | |||
| Non-daily intake | 0.615 | 0.463–0.817 | 0.145 | 0.001 |
| Vegetable intake (daily intake = ref) | 1.00 | |||
| Non-daily intake | 0.555 | 0.403–0.764 | 0.164 | <0.001 |
| Fruit intake (daily intake = ref) | 1.00 | |||
| Non-daily intake | 0.784 | 0.536–1.149 | 0.195 | 0.212 |
| Milk/dairy products intake (daily intake = ref) | 1.00 | |||
| Non-daily intake | 1.081 | 0.813–1.437 | 0.145 | 0.591 |
| Sugar sweetened drink intake (daily intake = ref) | 1.00 | |||
| Non-daily intake | 1.110 | 0.795–1.550 | 0.170 | 0.539 |
| Fast food intake (daily intake = ref) | 1.00 | |||
| Non-daily intake | 1.147 | 0.658–2.001 | 0.284 | 0.628 |
| French fries/potato chips intake (daily intake = ref) | 1.00 | |||
| Non-daily intake | 1.356 | 0.782–2.353 | 0.281 | 0.278 |
| Cake/donuts intake (daily intake = ref) | 1.00 | |||
| Non-daily intake | 0.757 | 0.452–1.267 | 0.263 | 0.290 |
| Chocolates/candy intake (daily intake = ref) | 1.00 | |||
| Non-daily intake | 0.882 | 0.584–1.334 | 0.211 | 0.553 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Hazzaa, H.M.; Alothman, S.A.; Alghannam, A.F.; Almasud, A.A. Anthropometric Measurements, Sociodemographics, and Lifestyle Behaviors among Saudi Adolescents Living in Riyadh Relative to Sex and Activity Energy Expenditure: Findings from the Arab Teens Lifestyle Study 2 (ATLS-2). Nutrients 2022, 14, 110. https://doi.org/10.3390/nu14010110
Al-Hazzaa HM, Alothman SA, Alghannam AF, Almasud AA. Anthropometric Measurements, Sociodemographics, and Lifestyle Behaviors among Saudi Adolescents Living in Riyadh Relative to Sex and Activity Energy Expenditure: Findings from the Arab Teens Lifestyle Study 2 (ATLS-2). Nutrients. 2022; 14(1):110. https://doi.org/10.3390/nu14010110
Chicago/Turabian StyleAl-Hazzaa, Hazzaa M., Shaima A. Alothman, Abdullah F. Alghannam, and Alaa A. Almasud. 2022. "Anthropometric Measurements, Sociodemographics, and Lifestyle Behaviors among Saudi Adolescents Living in Riyadh Relative to Sex and Activity Energy Expenditure: Findings from the Arab Teens Lifestyle Study 2 (ATLS-2)" Nutrients 14, no. 1: 110. https://doi.org/10.3390/nu14010110