
Human Leukocyte Antigen (HLA) Typing Study Identifies Maternal DQ2 Susceptibility Alleles among Infertile Women: Potential Associations with Autoimmunity and Micronutrients

 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Clinical Records Collection from the Study Cohort
2.3. Serum Determinations of Micronutrients
2.4. Genotyping of HLA-DQ2 and -DQ8 Alleles
2.5. Serology for CD
2.6. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Micronutrients Status
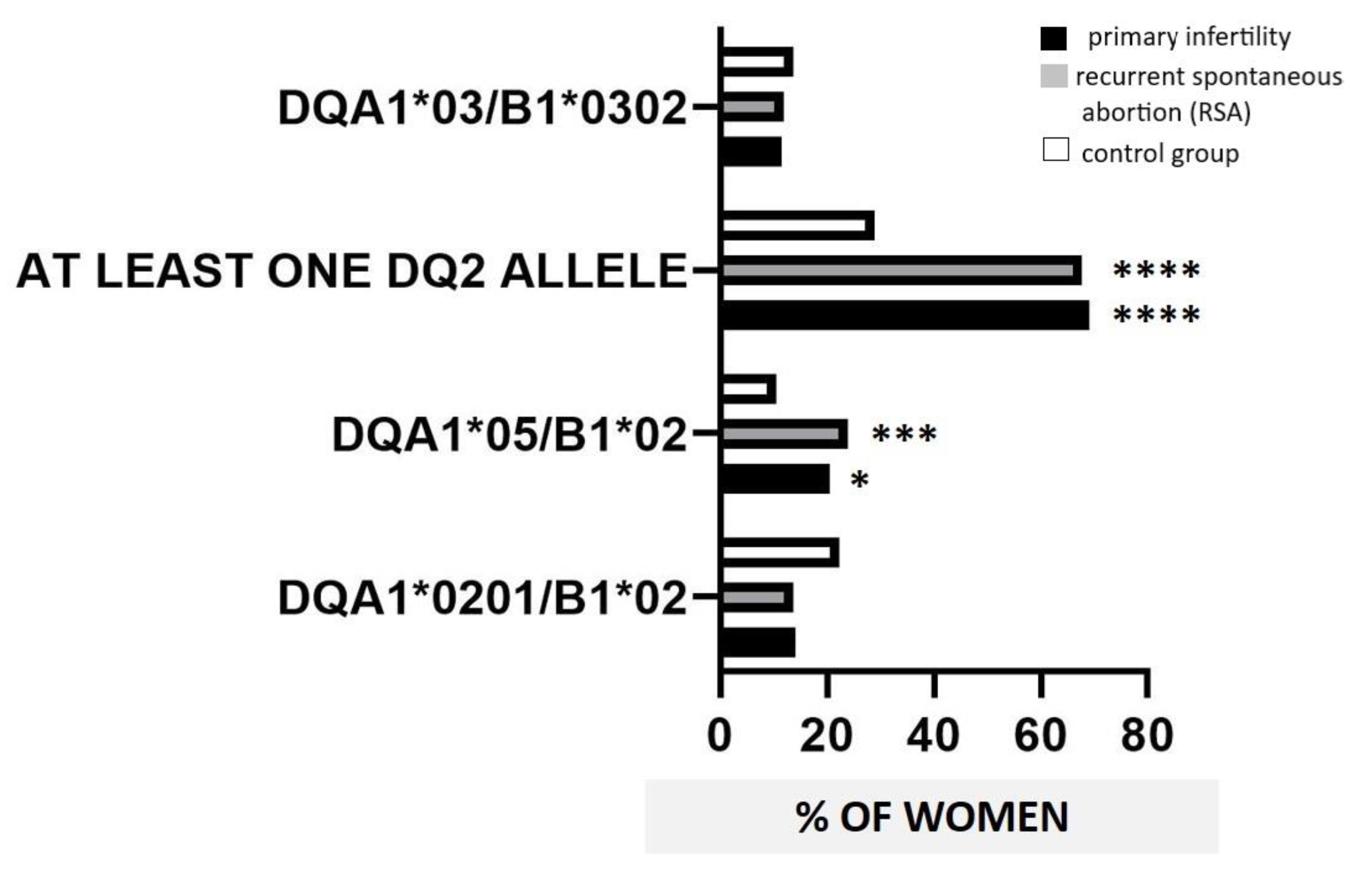
3.3. HLA-DQ2/-DQ8 Distribution
3.4. HLA-DQ2/-DQ8 Distribution and AIDs
3.5. HLA-DQ2/-DQ8 Positivity and CD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colley, E.; Hamilton, S.; Smith, P.; Morgan, N.V.; Coomarasamy, A.; Allen, S. Potential genetic causes of miscarriage in euploid pregnancies: A systematic review. Hum. Reprod. Update 2019, 25, 452–472. [Google Scholar] [CrossRef]
- Triggianese, P.; Perricone, C.; Perricone, R.; De Carolis, C. Prolactin and natural killer cells: Evaluating the neuroendocrine-immune axis in women with primary infertility and recurrent spontaneous abortion. Am. J. Reprod. Immunol. 2015, 73, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.B.; Jeelall, Y.; Pennell, C.E.; Hart, R.; McLean-Tooke, A.; Lucas, M. The role of immunological testing and intervention in reproductive medicine: A fertile collaboration? Am. J. Reprod. Immunol. 2018, 79, e12784. [Google Scholar] [CrossRef]
- De Carolis, S.; Moresi, S.; Rizzo, F.; Monteleone, G.; Tabacco, S.; Salvi, S.; Garufi, C.; Lanzone, A. Autoimmunity in obstetrics and autoimmune diseases in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2019, 60, 66–67. [Google Scholar] [CrossRef]
- Triggianese, P.; Perricone, C.; Chimenti, M.S.; De Carolis, C.; Perricone, R. Innate Immune System at the Maternal-Fetal Interface: Mechanisms of Disease and Targets of Therapy in Pregnancy Syndromes. Am. J. Reprod. Immunol. 2016, 76, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Perricone, C.; de Carolis, C.; Perricone, R. Pregnancy and autoimmunity: A common problem. Best Pract. Res. Clin. Rheumatol. 2012, 26, 47–60. [Google Scholar] [CrossRef]
- Negro, R. Levothyroxine before conception in women with thyroid antibodies: A step forward in the management of thyroid disease in pregnancy. Thyroid Res. 2019, 12, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.J.; Li, C.W.; Hammerstad, S.S.; Stefan, M.; Tomer, Y. Immunogenetics of autoimmune thyroid diseases: A comprehensive review. J. Autoimmun. 2015, 64, 82–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aversa, T.; Corica, D.; Zirilli, G.; Pajno, G.B.; Salzano, G.; De Luca, F.; Wasniewska, M. Phenotypic Expression of Autoimmunity in Children with Autoimmune Thyroid Disorders. Front. Endocrinol. 2019, 10, 476. [Google Scholar] [CrossRef] [Green Version]
- Farina, F.; Picascia, S.; Pisapia, L.; Barba, P.; Vitale, S.; Franzese, A.; Mozzillo, E.; Gianfrani, C.; Del Pozzo, G. HLA-DQA1 and HLA-DQB1 Alleles, Conferring Susceptibility to Celiac Disease and Type 1 Diabetes, are More Expressed ThanNon-Predisposing Alleles and are Coordinately Regulated. Cells 2019, 8, 751. [Google Scholar] [CrossRef] [Green Version]
- Castaño, M.; Gómez-Gordo, R.; Cuevas, D.; Núñez, C. Systematic Review and Meta-Analysis of Prevalence of Coeliac Disease in Women with Infertility. Nutrients 2019, 11, 1950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.M.; Lebwohl, B.; Wang, J.; Lee, S.K.; Murray, J.A.; Sauer, M.V.; Green, P.H.R. Increased prevalence of celiac disease in patients with unexplained infertility in the United States. J. Reprod. Med. 2011, 56, 199–203. [Google Scholar] [PubMed]
- Balestrieri, P.; Ribolsi, M.; Guarino, M.P.L.; Emerenziani, S.; Altomare, A.; Cicala, M. Nutritional Aspects in Inflammatory Bowel Diseases. Nutrients 2020, 12, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisshof, R.; Chermesh, I. Micronutrient deficiencies in inflammatory bowel disease. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Martín-Masot, R.; Nestares, M.T.; Diaz-Castro, J.; López-Aliaga, I.; Alférez, M.J.M.; Moreno-Fernandez, J.; Maldonado, J. Multifactorial Etiology of Anemia in Celiac Disease and Effect of Gluten-Free Diet: A Comprehensive Review. Nutrients 2019, 11, 2557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Luo, D.; Wang, Q.; Ma, Y.; Ping, L.; Wu, T.; Tang, J.; Peng, D.; Ping, Z. Serum homocysteine and folate concentrations in early pregnancy and subsequent events of adverse pregnancy outcome: The Sichuan Homocysteine study. BMC Pregnancy Childbirth 2020, 20, 176. [Google Scholar] [CrossRef]
- Infante, M.; Buoso, A.; Pieri, M.; Lupisella, S.; Nuccetelli, M.; Bernardini, S.; Fabbri, A.; Iannetta, M.; Andreoni, M.; Colizzi, V.; et al. Low Vitamin D Status at Admission as a Risk Factor for Poor Survival in Hospitalized Patients with COVID-19: An Italian Retrospective Study. J. Am. Coll. Nutr. 2021, 18, 1–16. [Google Scholar] [CrossRef]
- Triggianese, P.; Watad, A.; Cedola, F.; Perricone, C.; Amital, H.; Giambini, I.; Perricone, R.; Shoenfeld, Y.; De Carolis, C. Vitamin D deficiency in an Italian cohort of infertile women. Am. J. Reprod. Immunol. 2017, 78, e12733. [Google Scholar] [CrossRef]
- Rayman, M.P. Multiple nutritional factors and thyroid disease, with particular reference to autoimmune thyroid disease. Proc. Nutr. Soc. 2019, 78, 34–44. [Google Scholar] [CrossRef] [Green Version]
- Miettinen, M.E.; Kinnunen, L.; Harjutsalo, V.; Aimonen, K.; Surcel, H.M.; Lamberg-Allardt, C.; Tuomilehto, J. Association of serum 25-hydroxyvitamin D concentration with HLA-B, -DRB1 and -DQB1 genetic polymorphisms. Eur. J. Clin. Nutr. 2017, 71, 128–131. [Google Scholar] [CrossRef]
- Andreoli, L.; Bertsias, G.K.; Agmon-Levin, N.; Brown, S.; Cervera, R.; Costedoat-Chalumeau, N.; Doria, A.; Fischer-Betz, R.; Forger, F.; Moraes-Fontes, M.F.; et al. EULAR recommendations for women’s health and the management of family planning, assisted reproduction, pregnancy and menopause in patients with systemic lupus erythematosus and/or antiphospholipid syndrome. Ann. Rheum Dis. 2017, 76, 476–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triggianese, P.; Conigliaro, P.; Chimenti, M.S.; Barbato, C.; Greco, E.; Kroegler, B.; De Carolis, C.; Perricone, R. Systemic Sclerosis: Exploring the Potential Interplay between Thyroid Disorders and Pregnancy Outcome in an Italian Cohort. Isr. Med. Assoc. J. 2017, 19, 473–477. [Google Scholar] [PubMed]
- Perricone, C.; De Carolis, C.; Giacomelli, R.; Zaccari, G.; Cipriani, P.; Bizzi, E.; Perricone, R. High levels of NK cells in the peripheral blood of patients affected with anti-phospholipid syndrome and recurrent spontaneous abortion: A potential new hypothesis. Rheumatology 2007, 46, 1574–1578. [Google Scholar] [CrossRef] [Green Version]
- Triggianese, P.; Perricone, C.; Conigliaro, P.; Chimenti, M.S.; Perricone, R.; De Carolis, C. Peripheral blood natural killer cells and mild thyroid abnormalities in women with reproductive failure. Int. J. Immunopathol. Pharmacol. 2016, 29, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Practice Committee of American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: A committee opinion. Fertil. Steril. 2013, 99, 63. [Google Scholar] [CrossRef]
- McLeod, D.S.; Cooper, D.S. The incidence and prevalence of thyroid autoimmunity. Endocrine 2012, 42, 252–265. [Google Scholar] [CrossRef]
- Alijotas-Reig, J.; Esteve-Valverde, E.; Ferrer-Oliveras, R.; Sáez-Comet, L.; Lefkou, E.; Mekinian, A.; Belizna, C.; Ruffatti, A.; Hoxha, A.; Tincani, A.; et al. Comparative study of obstetric antiphospholipid syndrome (OAPS) and non-criteria obstetric APS (NC-OAPS): Report of 1640 cases from the EUROAPS registry. Rheumatology 2020, 59, 1306–1314. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.L.; Wolfe, F.; Huizinga, T.W. Rheumatoid arthritis. Lancet 2010, 376, 1094–1108. [Google Scholar] [CrossRef]
- Mosca, M.; Tani, C.; Talarico, R.; Bombardieri, S. Undifferentiated connective tissue diseases (UCTD): Simplified systemic autoimmune diseases. Autoimmun. Rev. 2011, 10, 256–258. [Google Scholar] [CrossRef]
- Assan, F.; Seror, R.; Mariette, X.; Nocturne, G. New 2019 SLE EULAR/ACR classification criteria are valuable for distinguishing patients with SLE from patients with pSS. Ann. Rheum. Dis. 2021, 80, e122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouvroye, M.D.; van Zijtveld, S.; Bonnet, P.; Spierings, E.; Bontkes, H.J. HLA-DQ Typing Kits in Diagnosis and Screening for Celiac Disease. Genet. Test Mol. Biomarkers 2019, 23, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Tye-Din, J.A.; Cameron, D.J.; Daveson, A.J.; Day, A.S.; Dellsperger, P.; Hogan, C.; Newnham, E.D.; Shepherd, S.J.; Steele, R.H.; Wienholt, L.; et al. Appropriate clinical use of human leukocyte antigen typing for coeliac disease: An Australasian perspective. Intern. Med. J. 2015, 45, 441–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choung, R.S.; Khaleghi, S.; Cartee, A.K.; Marietta, E.V.; Larson, J.J.; King, K.S.; Savolainen, O.; Ross, A.B.; Rajkumar, S.V.; Camilleri, M.J.; et al. Community-based Study of Celiac Disease Autoimmunity Progression in Adults. Gastroenterology 2020, 158, 151–159.e3. [Google Scholar] [CrossRef]
- Aldrich, C.; Verp, M.S.; Walker, M.A.; Ober, C. A null mutation in HLA-G is not associated with preeclampsia or intrauterine growth retardation. J. Reprod. Immunol. 2000, 47, 41–48. [Google Scholar] [CrossRef]
- Schacter, B.; Muir, A.; Gyves, M.; Tasin, M. HLA-A, B compatibility in parents of offspring with neural tube defects or couples experiencing involuntary fetal wastage. Lancet 1979, 1, 796–799. [Google Scholar] [CrossRef]
- D’Ippolito, S.; Gasbarrini, A.; Castellani, R.; Rocchetti, S.; Sisti, L.G.; Scambia, G.; Di Simone, N. Human leukocyte antigen (HLA) DQ2/DQ8 prevalence in recurrent pregnancy loss women. Autoimmun. Rev. 2016, 15, 638–643. [Google Scholar] [CrossRef]
- Ahmad, T.; Marshall, S.E.; Jewell, D. Genetics of inflammatory bowel disease: The role of the HLA complex. World J. Gastroenterol. 2006, 12, 3628–3635. [Google Scholar] [CrossRef]
- Lenti, M.V.; Miceli, E.; Padula, D.; Colleoni, R.; Beneventi, F.; Corazza, G.R.; Di Sabatino, A. Infertility and recurrent miscarriage in a patient with autoimmune atrophic gastritis. Intern. Emerg. Med. 2018, 13, 815–816. [Google Scholar] [CrossRef]
- Stazi, A.V.; Mantovani, A. A risk factor for female fertility and pregnancy: Celiac disease. Gynecol. Endocrinol. 2000, 14, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Bona, G.; Marinello, D.; Oderda, G. Mechanisms of abnormal puberty in coeliac disease. Horm. Res. 2002, 57, 63–65. [Google Scholar] [CrossRef]
- Tersigni, C.; Castellani, R.; de Waure, C.; Fattorossi, A.; De Spirito, M.; Gasbarrini, A.; Scambia, G.; Di Simone, N. Celiac disease and reproductive disorders: Meta-analysis of epidemiologic associations and potential pathogenic mechanisms. Hum. Reprod. Update 2014, 20, 582–593. [Google Scholar] [CrossRef]
- Tursi, A.; Giorgetti, G.; Brandimarte, G.; Elisei, W. Effect of gluten-free diet on pregnancy outcome in celiac disease patients with recurrent miscarriages. Dig. Dis. Sci. 2008, 53, 2925–2928. [Google Scholar] [CrossRef]
- Jukic, A.M.Z.; Baird, D.D.; Weinberg, C.R.; Wilcox, A.J.; McConnaughey, D.R.; Steiner, A.Z. Pre-conception 25-hydroxyvitamin D (25(OH)D) and fecundability. Hum. Reprod. 2019, 34, 2163–2172. [Google Scholar] [CrossRef] [PubMed]
- Machado, A.P.; Silva, L.R.; Zausner, B.; Oliveira, J.A.; Diniz, D.R.; de Oliveira, J. Undiagnosed celiac disease in women with infertility. J. Reprod. Med. 2013, 58, 61–66. [Google Scholar] [PubMed]
- Tersigni, C.; Redman, C.W.; Dragovic, R.; Tannetta, D.; Scambia, G.; Di Simone, N.; Sargent, I.; Vatish, M. HLA-DR is aberrantly expressed at feto-maternal interface in pre-eclampsia. J. Reprod. Immunol. 2018, 129, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Di Simone, N.; Silano, M.; Castellani, R.; Di Nicuolo, F.; D’Alessio, M.C.; Franceschi, F.; Tritarelli, A.; Leone, A.M.; Tersigni, C.; Gasbarrini, G.; et al. Anti-tissue transglutaminase antibodies from celiac patients are responsible for trophoblast damage via apoptosis in vitro. Am. J. Gastroenterol. 2010, 105, 2254–2261. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Trotta, L.; Alfano, C.; Balduzzi, D.; Staffieri, V.; Bianchi, P.I.; Marchese, A.; Vattiato, C.; Zilli, A.; Luinetti, O.; et al. Prevalence and natural history of potential celiac disease in adult patients. Scand. J. Gastroenterol. 2013, 48, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.; Lee, H.S.; Agardh, D. Risk of celiac disease according to HLA haplotype and country. N. Engl. J. Med. 2014, 371, 1074. [Google Scholar] [CrossRef] [Green Version]
- Auricchio, R.; Tosco, A.; Piccolo, E.; Galatola, M.; Izzo, V.; Maglio, M.; Paparo, F.; Troncone, R.; Greco, L. Potential celiac children: 9-year follow-up on a gluten-containing diet. Am. J. Gastroenterol. 2014, 109, 913–921. [Google Scholar] [CrossRef]
- Negro, R.; Mestman, J.H. Thyroid disease in pregnancy. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 927–943. [Google Scholar] [CrossRef]
- De Carolis, C.; Greco, E.; Guarino, M.D.; Perricone, C.; Dal Lago, A.; Giacomelli, R.; Fontana, L.; Perricone, R. Anti-thyroid antibodies and antiphospholipid syndrome: Evidence of reduced fecundity and of poor pregnancy outcome in recurrent spontaneous aborters. Am. J. Reprod. Immunol. 2004, 52, 263–266. [Google Scholar] [CrossRef]
- Dal Lago, A.; Vaquero, E.; Pasqualetti, P.; Lazzarin, N.; De Carolis, C.; Perricone, R.; Moretti, C. Prediction of early pregnancy maternal thyroid impairment in women affected with unexplained recurrent miscarriage. Hum. Reprod. 2011, 26, 1324–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twig, G.; Shina, A.; Amital, H.; Shoenfeld, Y. Pathogenesis of infertility and recurrent pregnancy loss in thyroid autoimmunity. J. Autoimmun. 2012, 38, J275–J281. [Google Scholar] [CrossRef] [PubMed]
- Pratt, D.E.; Kaberlein, G.; Dudkiewicz, A.; Karande, V.; Gleicher, N. The association of antithyroid antibodies in euthyroid nonpregnant women with recurrent first trimester abortions in the next pregnancy. Fertil. Steril. 1993, 60, 1001–1005. [Google Scholar] [CrossRef]
- Stagnaro-Green, A. Post-miscarriage thyroid dysfunction. Obstet. Gynecol. 1992, 80, 490–492. [Google Scholar]
- Barkia Beradhi, S.; Flesch, B.K.; Hansen, M.P.; Matheis, N.; Kahaly, G.J. HLA Class II Differentiates Between Thyroid and Polyglandular Autoimmunity. Horm. Metab. Res. 2016, 48, 232–237. [Google Scholar] [CrossRef]
- Stasiak, M.; Tymoniuk, B.; Stasiak, B.; Lewiński, A. The Risk of Recurrence of Subacute Thyroiditis Is HLA-Dependent. Int. J. Mol. Sci. 2019, 20, 1089. [Google Scholar] [CrossRef] [Green Version]
- Kosmopoulou, A.; Vlassi, M.; Stavrakoudis, A.; Sakarellos, C.; Sakarellos-Daitsiotis, M. T-cell epitopes of the La/SSB autoantigen: Prediction based on the homology modeling of HLA-DQ2/DQ7 with the insulin-B peptide/HLA-DQ8 complex. J. Comput. Chem. 2006, 27, 1033–1044. [Google Scholar] [CrossRef]
- Deroux, A.; Dumestre-Perard, C.; Dunand-Faure, C.; Bouillet, L.; Hoffmann, P. Female Infertility and Serum Auto-antibodies: A Systematic Review. Clin. Rev. Allergy Immunol. 2017, 53, 78–86. [Google Scholar] [CrossRef]
- D’Ippolito, S.; Ticconi, C.; Tersigni, C.; Garofalo, S.; Martino, C.; Lanzone, A.; Scambia, G.; Di Simone, N. The pathogenic role of autoantibodies in recurrent pregnancy loss. Am. J. Reprod. Immunol. 2020, 83, e13200. [Google Scholar] [CrossRef] [PubMed]
- Mosca, A.; De Cosmi, V.; Parazzini, F.; Raponi, M.; Alisi, A.; Agostoni, C.; Nobili, V. The Role of Genetic Predisposition, Programing During Fetal Life, Family Conditions, and Post-natal Diet in the Development of Pediatric Fatty Liver Disease. J. Pediatr. 2019, 211, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Andreoli, L.; Gerardi, M.C.; Fernandes, M.; Bortoluzzi, A.; Bellando-Randone, S.; Brucato, A.; Caporali, R.; Chighizola, C.B.; Chimenti, M.S.; Conigliaro, P.; et al. Disease activity assessment of rheumatic diseases during pregnancy: A comprehensive review of indices used in clinical studies. Autoimmun. Rev. 2018, 18, 164–176. [Google Scholar] [CrossRef]
- Levine, J.S.; Branch, D.W.; Rauch, J. The antiphospholipid syndrome. N. Engl. J. Med. 2002, 346, 752–763. [Google Scholar] [CrossRef] [Green Version]
- Stone, S.; Khamashta, M.A.; Poston, L. Placentation, antiphospholipid syndrome and pregnancy outcome. Lupus 2001, 10, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Kutteh, M.A.; Abiad, M.; Norman, G.L.; Kutteh, W.H. Comparison of celiac disease markers in women with early recurrent pregnancy loss and normal controls. Am. J. Reprod. Immunol. 2019, 82, e13127. [Google Scholar] [CrossRef] [PubMed]
- Al-Haddad, F.A.; Rajab, M.H.; Al-Qallaf, S.M.; Musaiger, A.O.; Hart, K.H. Assessment of vitamin D levels in newly diagnosed children with type 1 diabetes mellitus comparing two methods of measurement: A facility’s experience in the Middle Eastern country of Bahrain. Diabetes Metab. Syndr. Obes. 2016, 9, 11–16. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Primary Infertility (n = 78) | RSA (n = 109) | Controls (n = 350) | p Value | |
|---|---|---|---|---|
| Age (mean ± SD) | 37.3 ± 4.5 | 37 ± 4.3 | 37 ± 5 | Ns |
| N of SA (mean ± SD) | N.A. | 2.6 ± 0.6 | N.A. | N.A. |
| GW of SA (mean ± SD) | N.A. | 8 ± 2 | N.A. | N.A. |
| 25(OH)D (mean ± SD, ng/mL) § | 21.8 ± 10 * | 25.3 ± 11 | 26 ± 5.6 | 0.04 |
| VB12 (mean ± SD, pg/mL) § | 450 ± 181 | 400 ± 132 | 460 ± 120 | Ns |
| Folate (mean ± SD, ng/mL) § | 17.2 ± 16 | 18.9 ± 22 | 19 ± 9 | Ns |
| Ferritin (mean ± SD, ng/dl) § | 30 ± 21.6 | 29.3 ± 21.7 | 34 ± 22.8 | Ns |
| AIDs (N/%) | 38/48.7 ** | 36/33 | N.A. | 0.03 |
| Other AIDs (N/%) | 13/16.7 | 15/13.7 | N.A. | Ns |
| AITD (N/%) | 29/37.2 ** | 23/21.1 | N.A. | 0.01 |
| APS (N/%) | 5/6.4 | 10/9.2 | N.A. | Ns |
| RA (N/%) | 3/3.8 | 1/0.9 | N.A. | Ns |
| SjS (N/%) | 1/1.3 | 2/1.8 | N.A. | Ns |
| UCTD (N/%) | 2/2.6 | 2/1.8 | N.A. | Ns |
| G.I. diseases (N/%) | 4/5.13 | 3/2.7 | N.A. | Ns |
| DQA1*0201/B1*02 | DQA1*05/B1*02 | HLA-DQ8 | At Least One DQ2 | ||
|---|---|---|---|---|---|
| AIDs | RSA (n = 36) | 6/16.7 | 10/27.8 | 10/27.8 | 24/66.7 |
| Infertile (n = 38) | 6/15.8 | 12/31.6 ** | 7/18.4 | 33/86.8 * | |
| No AIDs | RSA (n = 73) | 9/12.3 | 16/21.9 | 16/21.9 | 51/69.9 |
| Infertile (n = 40) | 5/12.5 | 4/10 ** | 9/22.5 | 27/67.5 * | |
| AITD | RSA (n = 23) | 5/21.7 | 9/39.1 | 5/21.7 | 19/82.6 ** |
| Infertile (n = 29) | 6/20.7 | 11/37.9 * | 5/17.2 | 26/89.6 | |
| Other | RSA (n = 15) | 1/6.7 | 2/13.4 | 5/33.4 | 6/40 ** |
| Infertile (n = 13) | 1/7.7 | 1/7.7 * | 2/13.4 | 10/76.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triggianese, P.; Perricone, C.; De Martino, E.; D’Antonio, A.; Chimenti, M.S.; Conigliaro, P.; Ferrigno, S.; Giambini, I.; Greco, E.; De Carolis, C. Human Leukocyte Antigen (HLA) Typing Study Identifies Maternal DQ2 Susceptibility Alleles among Infertile Women: Potential Associations with Autoimmunity and Micronutrients. Nutrients 2021, 13, 3270. https://doi.org/10.3390/nu13093270
Triggianese P, Perricone C, De Martino E, D’Antonio A, Chimenti MS, Conigliaro P, Ferrigno S, Giambini I, Greco E, De Carolis C. Human Leukocyte Antigen (HLA) Typing Study Identifies Maternal DQ2 Susceptibility Alleles among Infertile Women: Potential Associations with Autoimmunity and Micronutrients. Nutrients. 2021; 13(9):3270. https://doi.org/10.3390/nu13093270
Chicago/Turabian StyleTriggianese, Paola, Carlo Perricone, Erica De Martino, Arianna D’Antonio, Maria Sole Chimenti, Paola Conigliaro, Sara Ferrigno, Ilio Giambini, Elisabetta Greco, and Caterina De Carolis. 2021. "Human Leukocyte Antigen (HLA) Typing Study Identifies Maternal DQ2 Susceptibility Alleles among Infertile Women: Potential Associations with Autoimmunity and Micronutrients" Nutrients 13, no. 9: 3270. https://doi.org/10.3390/nu13093270