
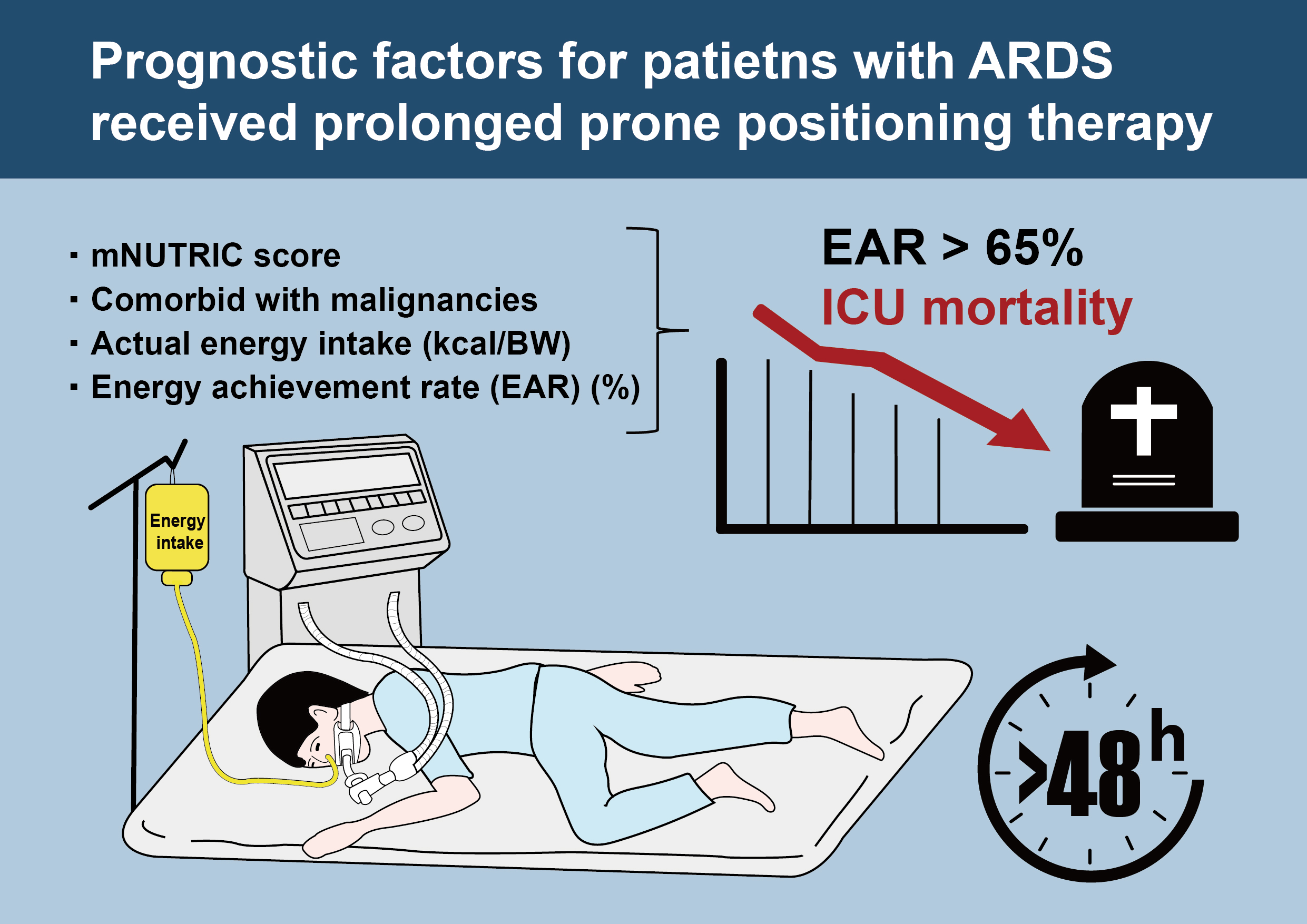
Energy Achievement Rate Is an Independent Factor Associated with Intensive Care Unit Mortality in High-Nutritional-Risk Patients with Acute Respiratory Distress Syndrome Requiring Prolonged Prone Positioning Therapy

 ,
,  , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Enrollment
2.2. Protocol of Prone Positioning Therapy
2.3. Protocol of Nutritional Risk Evaluation and Treatment
2.4. Data Collection, Assessment, and Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Patients’ Clinical and Demographic Characteristics
3.2. Differences between Survival and Non-Survival Groups
3.3. Factors Associated with ICU Mortality for Patients with ARDS Who Received PP Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Survival (n = 41) | Mortality (n = 38) | p Value | ||
|---|---|---|---|---|---|
| % | IQR | % | IQR | ||
| Energy achievement rate (%) | |||||
| day 1 | 18.3% | (7.3–46.8%) | 50.1% | (17.0–79.8%) | 0.010 * |
| day 2 | 46.8% | (19.1–71.3%) | 47.4% | (22.4–77.1%) | 0.603 |
| day 3 | 49.9% | (23.4–74.5%) | 46.6% | (28.4–76.0%) | 0.791 |
| day 4 | 69.9% | (40.7–86.1%) | 39.3% | (25.5–73.6%) | 0.052 |
| day 5 | 73.8% | (44.0–112.4%) | 47.0% | (30.7–83.0%) | 0.033 * |
| day 6 | 73.1% | (45.6–115.5%) | 65.2% | (24.6–98.5%) | 0.185 |
| day 7 | 72.3% | (52.1–105.3%) | 76.0% | (24.0–101.2%) | 0.388 |
References
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sioson, M.S.; Martindale, R.; Abayadeera, A.; Abouchaleh, N.; Aditianingsih, D.; Bhurayanontachai, R.; Chiou, W.C.; Higashibeppu, N.; Mat Nor, M.B.; Osland, E.; et al. Nutrition therapy for critically ill patients across the Asia-Pacific and Middle East regions: A consensus statement. Clin. Nutr. 2018, 24, 156–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, B.E.; McClave, S.A.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). Crit. Care Med. 2016, 44, 390–438. [Google Scholar] [CrossRef] [PubMed]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J. Parenter. Enteral. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef] [PubMed]
- Li, P.F.; Wang, Y.L.; Fang, Y.L.; Nan, L.; Zhou, J.; Zhang, D. Effect of early enteral nutrition on outcomes of trauma patients requiring intensive care. Chin. J. Traumatol. 2020, 23, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, A.; Henry, J.; Ong, V.; Leong, C.S.; Teh, A.L.; van Dam, R.M.; Kowitlawakul, Y. Association of modified NUTRIC score with 28-day mortality in critically ill patients. Clin. Nutr. 2017, 36, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; He, Z.; Yu, G.; Peng, D.; Feng, Y.; Ling, J.; Wang, Y.; Li, S.; Bian, Y. The modified NUTRIC score can be used for nutritional risk assessment as well as prognosis prediction in critically ill COVID-19 patients. Clin. Nutr. 2021, 40, 534–541. [Google Scholar] [CrossRef]
- Wang, W.N.; Wang, C.Y.; Hsu, C.Y.; Fu, P.K. Comparison of Feeding Efficiency and Hospital Mortality between Small Bowel and Nasogastric Tube Feeding in Critically Ill Patients at High Nutritional Risk. Nutrients 2020, 12, 2009. [Google Scholar] [CrossRef]
- Wang, C.Y.; Fu, P.K.; Chao, W.C.; Wang, W.N.; Chen, C.H.; Huang, Y.C. Full Versus Trophic Feeds in Critically Ill Adults with High and Low Nutritional Risk Scores: A Randomized Controlled Trial. Nutrients 2020, 12, 3518. [Google Scholar] [CrossRef]
- Wang, W.N.; Yang, M.F.; Wang, C.Y.; Hsu, C.Y.; Lee, B.J.; Fu, P.K. Optimal Time and Target for Evaluating Energy Delivery after Adjuvant Feeding with Small Bowel Enteral Nutrition in Critically Ill Patients at High Nutrition Risk. Nutrients 2019, 11, 645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.Y.; Fu, P.K.; Huang, C.T.; Chen, C.H.; Lee, B.J.; Huang, Y.C. Targeted Energy Intake Is the Important Determinant of Clinical Outcomes in Medical Critically Ill Patients with High Nutrition Risk. Nutrients 2018, 10, 1731. [Google Scholar] [CrossRef] [Green Version]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef]
- Hasan, S.S.; Capstick, T.; Ahmed, R.; Kow, C.S.; Mazhar, F.; Merchant, H.A.; Zaidi, S.T.R. Mortality in COVID-19 patients with acute respiratory distress syndrome and corticosteroids use: A systematic review and meta-analysis. Expert Rev. Respir Med. 2020, 14, 1149–1163. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.J.D.; McAuley, D.F.; Perkins, G.D.; Barrett, N.; Blackwood, B.; Boyle, A.; Chee, N.; Connolly, B.; Dark, P.; Finney, S.; et al. Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respir. Res. 2019, 6, e000420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Alhazzani, W.; Evans, L.; Alshamsi, F.; Moller, M.H.; Ostermann, M.; Prescott, H.C.; Arabi, Y.M.; Loeb, M.; Ng Gong, M.; Fan, E.; et al. Surviving Sepsis Campaign Guidelines on the Management of Adults With Coronavirus Disease 2019 (COVID-19) in the ICU: First Update. Crit. Care Med. 2021, 49, e219–e234. [Google Scholar] [CrossRef]
- Coppo, A.; Bellani, G.; Winterton, D.; Di Pierro, M.; Soria, A.; Faverio, P.; Cairo, M.; Mori, S.; Messinesi, G.; Contro, E.; et al. Feasibility and physiological effects of prone positioning in non-intubated patients with acute respiratory failure due to COVID-19 (PRON-COVID): A prospective cohort study. Lancet Respir. Med. 2020, 8, 765–774. [Google Scholar] [CrossRef]
- Behrens, S.; Kozeniecki, M.; Knapp, N.; Martindale, R.G. Nutrition Support During Prone Positioning: An Old Technique Reawakened by COVID-19. Nutr. Clin. Pract. 2021, 36, 105–109. [Google Scholar] [CrossRef]
- Ohbe, H.; Jo, T.; Matsui, H.; Fushimi, K.; Yasunaga, H. Early Enteral Nutrition in Patients Undergoing Sustained Neuromuscular Blockade: A Propensity-Matched Analysis Using a Nationwide Inpatient Database. Crit. Care Med. 2019, 47, 1072–1080. [Google Scholar] [CrossRef]
- Reignier, J.; Thenoz-Jost, N.; Fiancette, M.; Legendre, E.; Lebert, C.; Bontemps, F.; Clementi, E.; Martin-Lefevre, L. Early enteral nutrition in mechanically ventilated patients in the prone position. Crit. Care Med. 2004, 32, 94–99. [Google Scholar] [CrossRef]
- Bruni, A.; Garofalo, E.; Grande, L.; Auletta, G.; Cubello, D.; Greco, M.; Lombardo, N.; Garieri, P.; Papaleo, A.; Doldo, P.; et al. Nursing issues in enteral nutrition during prone position in critically ill patients: A systematic review of the literature. Intensive Crit. Care Nurs. 2020, 60, 102899. [Google Scholar] [CrossRef]
- Girard, R.; Baboi, L.; Ayzac, L.; Richard, J.C.; Guerin, C. The impact of patient positioning on pressure ulcers in patients with severe ARDS: Results from a multicentre randomised controlled trial on prone positioning. Intensive Care Med. 2014, 40, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Howell, M.D.; Davis, A.M. Management of ARDS in Adults. JAMA 2018, 319, 711–712. [Google Scholar] [CrossRef]
- Lee, P.H.; Kuo, C.T.; Hsu, C.Y.; Lin, S.P.; Fu, P.K. Prognostic Factors to Predict ICU Mortality in Patients with Severe ARDS Who Received Early and Prolonged Prone Positioning Therapy. J. Clin. Med. 2021, 10, 2323. [Google Scholar] [CrossRef] [PubMed]
- Hadaya, J.; Benharash, P. Prone Positioning for Acute Respiratory Distress Syndrome (ARDS). JAMA 2020, 324, 1361. [Google Scholar] [CrossRef]
- Fan, E.; Del Sorbo, L.; Goligher, E.C.; Hodgson, C.L.; Munshi, L.; Walkey, A.J.; Adhikari, N.K.J.; Amato, M.B.P.; Branson, R.; Brower, R.G.; et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1253–1263. [Google Scholar] [CrossRef]
- Chan, M.C.; Hsu, J.Y.; Liu, H.H.; Lee, Y.L.; Pong, S.C.; Chang, L.Y.; Kuo, B.I.; Wu, C.L. Effects of prone position on inflammatory markers in patients with ARDS due to community-acquired pneumonia. J. Formos. Med. Assoc. 2007, 106, 708–716. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.L.; Huang, C.T.; Chen, C.H.; Fu, P.K.; Wang, C.Y. Outcome of glycemic control in critically ill patients receiving enteral formulas. Asia Pac. J. Clin. Nutr. 2021, 30, 22–29. [Google Scholar] [CrossRef]
- Weijs, P.J.M.; Mogensen, K.M.; Rawn, J.D.; Christopher, K.B. Protein Intake, Nutritional Status and Outcomes in ICU Survivors: A Single Center Cohort Study. J. Clin. Med. 2019, 8, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp Lugli, A.; de Watteville, A.; Hollinger, A.; Goetz, N.; Heidegger, C. Medical Nutrition Therapy in Critically Ill Patients Treated on Intensive and Intermediate Care Units: A Literature Review. J. Clin. Med. 2019, 8, 1395. [Google Scholar] [CrossRef] [Green Version]
- Havens, J.M.; Columbus, A.B.; Seshadri, A.J.; Olufajo, O.A.; Mogensen, K.M.; Rawn, J.D.; Salim, A.; Christopher, K.B. Malnutrition at Intensive Care Unit Admission Predicts Mortality in Emergency General Surgery Patients. JPEN J. Parenter. Enteral. Nutr. 2018, 42, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Hasan, R.M.; Agarwala, R.; Martin, C.; Day, A.G.; Heyland, D.K. Identifying critically-ill patients who will benefit most from nutritional therapy: Further validation of the “modified NUTRIC” nutritional risk assessment tool. Clin. Nutr. 2016, 35, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.W.; Ju, S.; Lee, S.J.; Cho, Y.J.; Lee, J.D.; Kim, H.C. Geriatric nutritional risk index is associated with 30-day mortality in patients with acute respiratory distress syndrome. Medicine 2020, 99, e20671. [Google Scholar] [CrossRef]
- Yenibertiz, D.; Cirik, M.O. The comparison of GNRI and other nutritional indexes on short-term survival in geriatric patients treated for respiratory failure. Aging Clin. Exp. Res. 2021, 33, 611–617. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Modrykamien, A.M.; Daoud, Y. Factors among patients receiving prone positioning for the acute respiratory distress syndrome found useful for predicting mortality in the intensive care unit. Bayl. Univ. Med Cent. Proc. 2018, 31, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kao, K.C.; Chang, K.W.; Chan, M.C.; Liang, S.J.; Chien, Y.C.; Hu, H.C.; Chiu, L.C.; Chen, W.C.; Fang, W.F.; Chen, Y.M.; et al. Predictors of survival in patients with influenza pneumonia-related severe acute respiratory distress syndrome treated with prone positioning. Ann. Intensive Care 2018, 8, 94. [Google Scholar] [CrossRef] [PubMed]
- Savio, R.D.; Parasuraman, R.; Lovesly, D.; Shankar, B.; Ranganathan, L.; Ramakrishnan, N.; Venkataraman, R. Feasibility, tolerance and effectiveness of enteral feeding in critically ill patients in prone position. J. Intensive Care Soc. 2021, 22, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Machado, L.S.; Rizzi, P.; Silva, F.M. Administration of enteral nutrition in the prone position, gastric residual volume and other clinical outcomes in critically ill patients: A systematic review. Rev. Bras. Ter. Intensiva 2020, 32, 133–142. [Google Scholar] [CrossRef]
- Reignier, J.; Dimet, J.; Martin-Lefevre, L.; Bontemps, F.; Fiancette, M.; Clementi, E.; Lebert, C.; Renard, B. Before-after study of a standardized ICU protocol for early enteral feeding in patients turned in the prone position. Clin. Nutr. 2010, 29, 210–216. [Google Scholar] [CrossRef] [PubMed]




| Characteristics | Median (IQR) or n (%) (n = 79) |
|---|---|
| Demographic data | |
| Age (y/o) (n, %) | 61.5 (51.1–74) |
| Gender-Male (n, %) | 48 (60.8%) |
| mNUTRIC score | 7.0 (5–8) |
| APACHE II score | 31.0 (27–33) |
| SOFA | 10.0 (8–14) |
| Renal replacement therapy (n, %) | 35 (44.30%) |
| Comorbidity | |
| CAD (n, %) | 6 (7.59%) |
| COPD (n, %) | 10 (12.66%) |
| Solid cancer (n, %) | 11 (13.92%) |
| Hematologic malignancies (n, %) | 5 (6.33%) |
| DM (n, %) | 24 (30.38%) |
| CKD (n, %) | 27 (34.18%) |
| Autoimmune disease (n, %) | 12 (15.19%) |
| PaO2/FiO2 (PF ratio) | 92.5 (70.1–114.3) |
| Actual energy intake (kcal/BW) | |
| During prolonged PP (d 1–d 3) | 7.9 (4.6–13) |
| Post prolonged PP (d 4–d 7) | 12.0 (7.3–18.8) |
| Average in the first 7 d | 10.8 (6.6–15.2) |
| Energy achievement rate (%) | |
| During prolonged PP (d 1–d 3) | 42.0 (23.8–64.9) |
| Post prolonged PP (d 4–d 7) | 64.5 (36.4–91.8) |
| Average in the first 7 d | 55.5 (33.1–81.8) |
| ICU mortality (n, %) | 38 (48.10%) |
| Characteristics | Survival (n = 41) | Non-Survival (n = 38) | p Value |
|---|---|---|---|
| Demographic data | |||
| Age (y/o) (n, %) | 56.8 (46–68.3) | 63.8 (56.9–76.5) | 0.036 * |
| Gender-Male (n, %) | 27 (65.9%) | 21 (55.3%) | 0.464 |
| mNUTRIC score | 6.0 (4–7) | 7.0 (6–8) | 0.002 ** |
| APACHE II score | 31.0 (26.5–32.5) | 31.0 (26.8–34.3) | 0.470 |
| SOFA | 10.0 (8–14.5) | 10.5 (8–14.3) | 0.996 |
| Renal replacement therapy (n, %) | 13 (31.7%) | 22 (57.9%) | 0.034 * |
| Comorbidity | |||
| CAD (n, %) f | 3 (7.3%) | 3 (7.9%) | 1.000 |
| COPD (n, %) f | 6 (14.6%) | 4 (10.5%) | 0.739 |
| Solid cancer (n, %) | 1 (2.4%) | 10 (26.3%) | 0.006 ** |
| Hematologic malignancies (n, %) | 1 (2.4%) | 4 (10.5%) | 0.190 |
| DM (n, %) | 16 (39.0%) | 8 (21.1%) | 0.136 |
| CKD (n, %) | 12 (29.3%) | 15 (39.5%) | 0.473 |
| Autoimmune disease (n, %) | 5 (12.2%) | 7 (18.4%) | 0.648 |
| PaO2/FiO2 (PF ratio) | 96.5 (73.2–125.2) | 88.7 (65.5–104.3) | 0.133 |
| Actual energy intake (kcal/BW) | |||
| During prolonged PP (d 1–d 3) | 6.5 (4–11.6) | 9.2 (5.1–14.8) | 0.133 |
| Post prolonged PP (d 4–d 7) | 12.8 (9–21.2) | 10.2 (5.3–16.9) | 0.049 * |
| Average in the first 7 d | 10.5 (7.3–16.4) | 10.9 (5.6–15.5) | 0.638 |
| Energy achievement rate (%) | |||
| During prolonged PP (d 1–d 3) | 39.3% (19.8–59.4%) | 46.1% (29.2–76.0%) | 0.192 |
| Post prolonged PP (d 4–d 7) | 77.9% (47.2–102.7%) | 51.1% (26.6–87.4%) | 0.025 * |
| Average in the first 7 d | 57.4% (37.3–82.1%) | 55.1% (28.2–82.1%) | 0.498 |
| Characteristics | Univariate Analysis HR (95% CI) p Value | Multivariate Analysis HR (95% CI) p Value | ||
|---|---|---|---|---|
| Demographic data | ||||
| Age | 1.02 (1.00–1.04) | 0.062 | ||
| Sex (Female/Male) | 0.76 (0.40–1.44) | 0.401 | ||
| BMI (kg/m2) | 1.01 (0.94–1.08) | 0.848 | ||
| mNUTRIC score | 1.26 (1.01–1.58) | 0.038 * | 1.22 (0.95 0.56) | 0.116 |
| APACHE II score | 1.04 (0.98–1.09) | 0.182 | ||
| SOFA | 1.03 (0.95–1.12) | 0.510 | ||
| Renal replacement therapy (n, %) | 1.31 (0.68–2.50) | 0.422 | ||
| Comorbidity | ||||
| CAD (n, %) f | 1.32 (0.40–4.32) | 0.648 | ||
| COPD (n, %) f | 0.65 (0.23–1.86) | 0.426 | ||
| Solid cancer (n, %) | 2.68 (1.28–5.62) | 0.009 ** | 2.81 (1.25–6.33) | 0.013 * |
| Hematologic malignancies (n, %) | 2.90 (1.01–8.31) | 0.047 * | 2.74 (0.83–9.10) | 0.099 |
| DM (n, %) | 1.03 (0.46–2.28) | 0.945 | ||
| CKD (n, %) | 1.15 (0.60–2.22) | 0.668 | ||
| Autoimmune disease (n, %) | 1.09 (0.48–2.48) | 0.839 | ||
| PaO2/FiO2 (PF ratio) | 0.99 (0.98–1.00) | 0.084 | ||
| Actual energy intake (kcal/BW) | ||||
| During prolonged PP (d 1–d 3) | 1.00 (0.96–1.04) | 0.994 | ||
| Post prolonged PP (d 4–d 7) | 0.94 (0.90–0.98) | 0.007 ** | 0.93 (0.89–0.98) | 0.006 ** |
| Average in the first 7 d | 0.97 (0.92–1.01) | 0.144 | ||
| Energy achievement rate (%) | ||||
| During prolonged PP (d 1–d 3) | 1.00 (0.38–2.59) | 0.994 | ||
| Post prolonged PP (d 4–d 7) | 0.21 (0.07–0.64) | 0.006 ** | 0.19 (0.07–0.56) | 0.002 ** |
| Average in the first 7 d | 0.42 (0.14–1.27) | 0.124 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, P.-K.; Wang, C.-Y.; Wang, W.-N.; Hsu, C.-Y.; Lin, S.-P.; Kuo, C.-T. Energy Achievement Rate Is an Independent Factor Associated with Intensive Care Unit Mortality in High-Nutritional-Risk Patients with Acute Respiratory Distress Syndrome Requiring Prolonged Prone Positioning Therapy. Nutrients 2021, 13, 3176. https://doi.org/10.3390/nu13093176
Fu P-K, Wang C-Y, Wang W-N, Hsu C-Y, Lin S-P, Kuo C-T. Energy Achievement Rate Is an Independent Factor Associated with Intensive Care Unit Mortality in High-Nutritional-Risk Patients with Acute Respiratory Distress Syndrome Requiring Prolonged Prone Positioning Therapy. Nutrients. 2021; 13(9):3176. https://doi.org/10.3390/nu13093176
Chicago/Turabian StyleFu, Pin-Kuei, Chen-Yu Wang, Wei-Ning Wang, Chiann-Yi Hsu, Shih-Pin Lin, and Chen-Tsung Kuo. 2021. "Energy Achievement Rate Is an Independent Factor Associated with Intensive Care Unit Mortality in High-Nutritional-Risk Patients with Acute Respiratory Distress Syndrome Requiring Prolonged Prone Positioning Therapy" Nutrients 13, no. 9: 3176. https://doi.org/10.3390/nu13093176