Differing Nutrient Intake and Dietary Patterns According to the Presence of Hyper-Low-Density Lipoprotein Cholesterolemia or Hypertriglyceridemia


Abstract
:1. Introduction
2. Materials and Methods
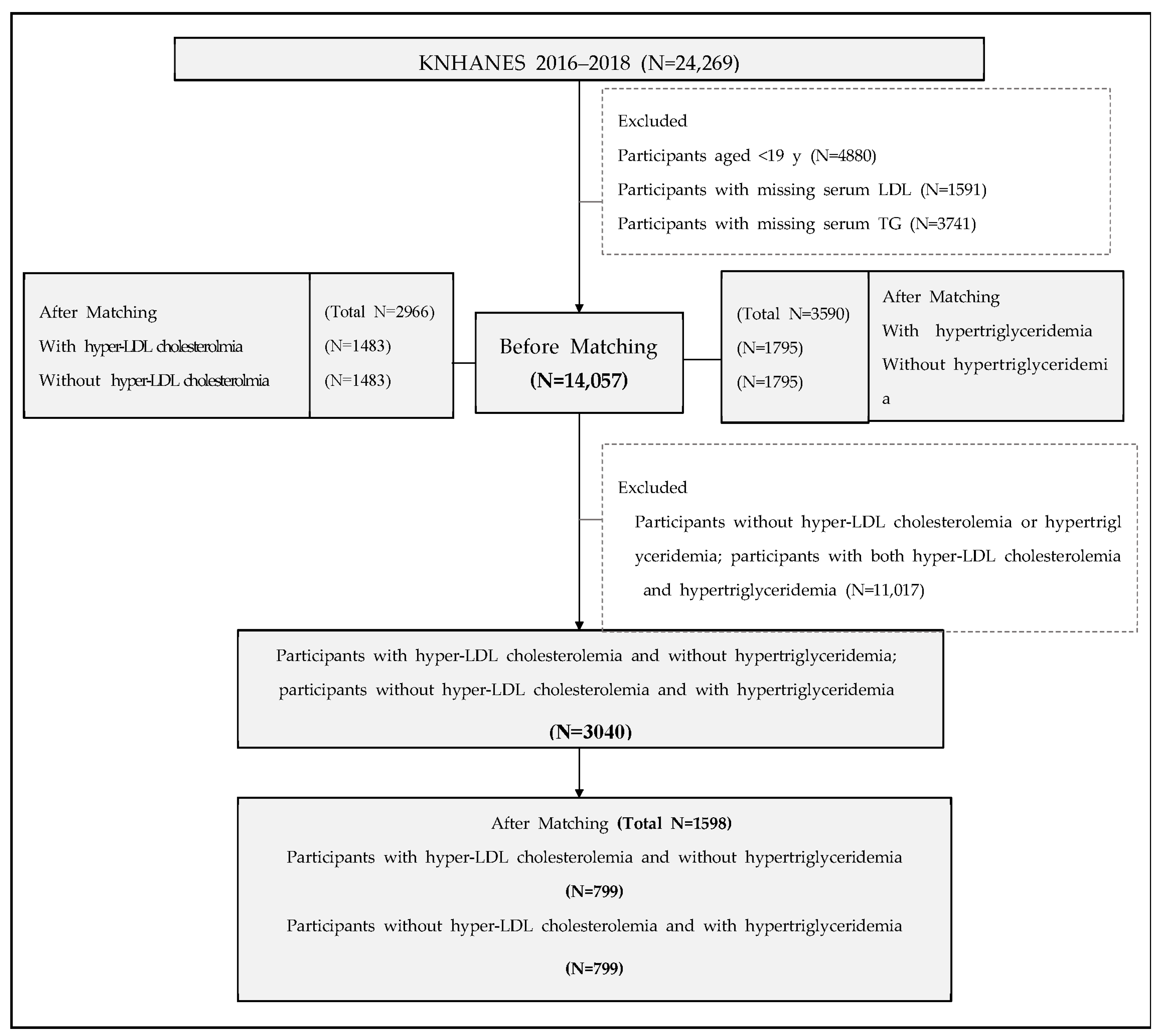
2.1. Study Population
2.2. Anthropometrics and Biochemical Variables
2.3. Definition of Dyslipidemia
2.4. Assessment of Nutrition Intake and Dietary Patterns
2.5. Statistical Analysis
3. Results
3.1. Clinical and Dietary Characteristics According to LDL-C Level
3.2. Clinical and Dietary Characteristics According to TG Level
3.3. Comparison of Nutrition Intake between hLDL-Only and hTG-Only Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Rhee, E.J. Prevalence and current management of cardiovascular risk factors in korean adults based on fact sheets. Endocrinol. Metab. 2020, 35, 85–94. [Google Scholar] [CrossRef]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 56. [Google Scholar] [CrossRef]
- Cho, S.M.J.; Lee, H.; Lee, H.H.; Baek, J.; Heo, J.E.; Joo, H.J.; Hong, S.J.; Kim, H.C. Dyslipidemia fact sheets in korea 2020: An analysis of nationwide population-based data. J. Lipid Atheroscler. 2021, 10, 202–209. [Google Scholar] [CrossRef]
- National Center for Health Statistics. National Center for Health Statistics; 2021. Available online: https://www.cdc.gov/nchs (accessed on 9 June 2021).
- Ministry of Health, Labour and Welfare. National Health and Nutrition Survey in Japan. Available online: http://www.mhlw.go.jp/toukei/itiran/gaiyo/k-eisei.html (accessed on 9 June 2021).
- Ko, M.; Kim, M.T.; Nam, J.J. Assessing risk factors of coronary heart disease and its risk prediction among Korean adults: The 2001 Korea national health and nutrition examination survey. Int. J. Cardiol. 2006, 110, 184–190. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 esc/eas guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 acc/aha guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 2019, 74, e177–e232. [Google Scholar] [CrossRef]
- Grundy, S.M. An international atherosclerosis society position paper: Global recommendations for the management of dyslipidemia. J. Clin. Lipidol. 2013, 7, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Georgia-Eirini, D.; Athina, S.; Wim, V.B.; Christos, K.; Theodoros, C. Natural products from mediterranean diet: From anti-hyperlipidemic agents to dietary epigenetic modulators. Curr. Pharm. Biotechnol. 2019, 20, 825–844. [Google Scholar] [CrossRef]
- Salehi-Abargouei, A.; Maghsoudi, Z.; Shirani, F.; Azadbakht, L. Effects of dietary approaches to stop hypertension (dash)-style diet on fatal or nonfatal cardiovascular diseases—Incidence: A systematic review and meta-analysis on observational prospective studies. Nutrition 2013, 29, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Mensink, R.P.; World Health Organization. Effects of Saturated Fatty Acids on Serum Lipids and Lipoproteins: A Systematic Review and Regression Analysis; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- The Scientific Advisory Committee on Nutrition (SACN). Report on Saturated Fats and Health 2019. Available online: https://www.gov.uk/government/publications/saturated-fats-and-health-sacn-report (accessed on 10 July 2021).
- Korea Centers for Disease Control and Prevention (KCDC). Korea National Health & Nutritional Examination Survey Sixth (2013–2015), Guidbook for Data User (Korean). Available online: https://knhanes.cdc.go.kr/knhanes/eng/index.do (accessed on 20 November 2017).
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the national cholesterol education program (ncep) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel iii). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the national cholesterol education program (ncep) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel iii) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Yun, S.H.; Shim, J.-S.; Kweon, S.; Oh, K. Development of a food frequency questionnaire for the korea national health and nutrition examination survey: Data from the fourth korea national health and nutrition examination survey (knhanes iv). Korean J. Nutr. 2013, 46, 186–196. [Google Scholar] [CrossRef] [Green Version]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The korea national health and nutrition examination survey (knhanes). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yook, S.-M.; Park, S.; Moon, H.-K.; Kim, K.; Shim, J.E.; Hwang, J.-Y. Development of korean healthy eating index for adults using the korea national health and nutrition examination survey data. J. Nutr. Health 2015, 48, 419–428. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Kim, K.; Lee, B.K.; Ahn, J. Association of the healthy eating index with estimated cardiovascular age in adults from the knhanes 2013–2017. Nutrients 2020, 12, 2912. [Google Scholar] [CrossRef]
- Musunuru, K. Atherogenic dyslipidemia: Cardiovascular risk and dietary intervention. Lipids 2010, 45, 907–914. [Google Scholar] [CrossRef] [Green Version]
- Ballantyne, C.M.; Olsson, A.G.; Cook, T.J.; Mercuri, M.F.; Pedersen, T.R.; Kjekshus, J. Influence of low high-density lipoprotein cholesterol and elevated triglyceride on coronary heart disease events and response to simvastatin therapy in 4s. Circulation 2001, 104, 3046–3051. [Google Scholar] [CrossRef] [Green Version]
- Toth, P.P. Triglyceride-rich lipoproteins as a causal factor for cardiovascular disease. Vasc. Health Risk Manag. 2016, 12, 171–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, A.H.; Tseng, C.H. The role of triglyceride in cardiovascular disease in asian patients with type 2 diabetes—A systematic review. Rev. Diabet. Stud. 2013, 10, 101–109. [Google Scholar] [CrossRef] [Green Version]
- Sone, H.; Tanaka, S.; Tanaka, S.; Iimuro, S.; Oida, K.; Yamasaki, Y.; Oikawa, S.; Ishibashi, S.; Katayama, S.; Ohashi, Y.; et al. Serum level of triglycerides is a potent risk factor comparable to ldl cholesterol for coronary heart disease in japanese patients with type 2 diabetes: Subanalysis of the japan diabetes complications study (jdcs). J. Clin. Endocrinol. Metab. 2011, 96, 3448–3456. [Google Scholar] [CrossRef]
- Song, S.; Song, W.O.; Song, Y. Dietary carbohydrate and fat intakes are differentially associated with lipid abnormalities in korean adults. J. Clin. Lipidol. 2017, 11, 338–347.e333. [Google Scholar] [CrossRef]
- Zock, P.L.; Blom, W.A.; Nettleton, J.A.; Hornstra, G. Progressing insights into the role of dietary fats in the prevention of cardiovascular disease. Curr. Cardiol. Rep. 2016, 18, 111. [Google Scholar] [CrossRef] [Green Version]
- Balk, E.M.; Lichtenstein, A.H.; Chung, M.; Kupelnick, B.; Chew, P.; Lau, J. Effects of omega-3 fatty acids on serum markers of cardiovascular disease risk: A systematic review. Atherosclerosis 2006, 189, 19–30. [Google Scholar] [CrossRef]
- López-Domínguez, J.A.; Ramsey, J.J.; Tran, D.; Imai, D.M.; Koehne, A.; Laing, S.T.; Griffey, S.M.; Kim, K.; Taylor, S.L.; Hagopian, K.; et al. The influence of dietary fat source on life span in calorie restricted mice. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1181–1188. [Google Scholar] [CrossRef] [Green Version]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; de Jesus, J.M.; Miller, N.H.; Hubbard, V.S.; Lee, I.M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 aha/acc guideline on lifestyle management to reduce cardiovascular risk: A report of the american college of cardiology/american heart association task force on practice guidelines. J. Am. Coll. Cardiol. 2014, 63, 2960–2984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobson, T.A.; Maki, K.C.; Orringer, C.E.; Jones, P.H.; Kris-Etherton, P.; Sikand, G.; La Forge, R.; Daniels, S.R.; Wilson, D.P.; Morris, P.B.; et al. National lipid association recommendations for patient-centered management of dyslipidemia: Part 2. J. Clin. Lipidol. 2015, 9, S1–S122.e1. [Google Scholar] [CrossRef] [Green Version]
- Siri-Tarino, P.W.; Sun, Q.; Hu, F.B.; Krauss, R.M. Saturated fat, carbohydrate, and cardiovascular disease. Am. J. Clin. Nutr. 2010, 91, 502–509. [Google Scholar] [CrossRef] [Green Version]
- Astrup, A.; Magkos, F.; Bier, D.M.; Brenna, J.T.; de Oliveira Otto, M.C.; Hill, J.O.; King, J.C.; Mente, A.; Ordovas, J.M.; Volek, J.S.; et al. Saturated fats and health: A reassessment and proposal for food-based recommendations: Jacc state-of-the-art review. J. Am. Coll. Cardiol. 2020, 76, 844–857. [Google Scholar] [CrossRef] [PubMed]
- Schap, T.; Kuczynski, K.; Hiza, H. Healthy eating index-beyond the score. J. Acad. Nutr. Diet. 2017, 117, 519–521. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Neelakantan, N.; Wu, Y.; Lote-Oke, R.; Pan, A.; van Dam, R.M. Palm oil consumption increases ldl cholesterol compared with vegetable oils low in saturated fat in a meta-analysis of clinical trials. J. Nutr. 2015, 145, 1549–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaidean, G.D.; Manczuk, M.; Vansal, S.S.; Griffith, J. The cholesterol-lowering effect of statins is potentiated by whole grains intake. The polish norwegian study (pons). Eur. J. Intern. Med. 2018, 50, 47–51. [Google Scholar] [CrossRef]
- Surampudi, P.; Enkhmaa, B.; Anuurad, E.; Berglund, L. Lipid lowering with soluble dietary fiber. Curr. Atheroscler. Rep. 2016, 18, 75. [Google Scholar] [CrossRef]
- Temple, N.J. Fat, sugar, whole grains and heart disease: 50 years of confusion. Nutrients 2018, 10, 39. [Google Scholar] [CrossRef] [Green Version]
- Committee for the Korean Guidelines for the Management of Dyslipidemia. 2015 Korean guidelines for the management of dyslipidemia: Executive summary (english translation). Korean Circ. J. 2016, 46, 275–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D.; Rosenberg, I.; Uauy, R. History of modern nutrition science-implications for current research, dietary guidelines, and food policy. BMJ 2018, 361, k2392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geleijnse, J.M.; Witteman, J.C.; Stijnen, T.; Kloos, M.W.; Hofman, A.; Grobbee, D.E. Sodium and potassium intake and risk of cardiovascular events and all-cause mortality: The rotterdam study. Eur. J. Epidemiol. 2007, 22, 763–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Salt Reduction and Iodine Fortification Strategies in Public Health: Report of a Joint Technical Meeting Convened by the World Health Organization and the George Institute for Global Health in Collaboration with the International Council for the Control of Iodine Deficiency Disorders Global Network, Sydney, Australia, March 2013; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Park, H.K.; Lee, Y.; Kang, B.W.; Kwon, K.I.; Kim, J.W.; Kwon, O.S.; Cobb, L.K.; Campbell, N.R.C.; Blakeman, D.E.; Kim, C.I. Progress on sodium reduction in South Korea. BMJ Glob. Health 2020, 5, e002028. [Google Scholar] [CrossRef]
- Sun, H.; Weaver, C.M. Rise in potassium deficiency in the us population linked to agriculture practices and dietary potassium deficits. J. Agric. Food Chem. 2020, 68, 11121–11127. [Google Scholar] [CrossRef]
- Mirmiran, P.; Bahadoran, Z.; Mirzaei, S.; Azizi, F. Dietary intake, changes in lipid parameters and the risk of hypertriglyceridemia: A prospective approach in the tehran lipid and glucose study. Int. J. Vitam. Nutr. Res. 2014, 84, 269–276. [Google Scholar] [CrossRef]
- Kim, S.H.; Song, Y.H.; Park, S.; Park, M.J. Impact of lifestyle factors on trends in lipid profiles among korean adolescents: The korea national health and nutrition examination surveys study, 1998 and 2010. Korean J. Pediatr. 2016, 59, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Deshmukh-Taskar, P.; Nicklas, T.A.; Radcliffe, J.D.; O’Neil, C.E.; Liu, Y. The relationship of breakfast skipping and type of breakfast consumed with overweight/obesity, abdominal obesity, other cardiometabolic risk factors and the metabolic syndrome in young adults. The national health and nutrition examination survey (nhanes): 1999–2006. Public Health Nutr. 2013, 16, 2073–2082. [Google Scholar] [PubMed] [Green Version]
- Soedamah-Muthu, S.S.; Ding, E.L.; Al-Delaimy, W.K.; Hu, F.B.; Engberink, M.F.; Willett, W.C.; Geleijnse, J.M. Milk and dairy consumption and incidence of cardiovascular diseases and all-cause mortality: Dose-response meta-analysis of prospective cohort studies. Am. J. Clin. Nutr. 2011, 93, 158–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.-J.; Park, J.; Song, H.J.; Lee, C.-H.; Lee, H.-J. Association between dairy product intake and hypertriglyceridemia in korean adults. Nutr. Res. Pract. 2020, 14, 152–159. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Before Propensity Score—Matching | After Propensity Score—Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| Total (N = 14,057) | Non-hLDL (N = 12,745) | hLDL (N = 1312) | p-Value | Total (N = 2966) | Non-hLDL (N = 1483) | hLDL (N = 1483) | p-Value | |
| Sex (male) | 5955 (42.4) | 5486 (43.0) | 469 (35.8) | <0.001 | 1126 (37.96) | 561 (37.83) | 565 (38.10) | 0.880 |
| Age (y) | 52.0 ± 16.6 | 51.7 ± 17.1 | 54.6 ± 14.3 | <0.001 | 54.1 ± 15.2 | 54.1 ± 16.3 | 54.0 ± 14.0 | 0.816 |
| BMI (kg/m2) | 23.9 ± 3.5 | 23.9 ± 3.5 | 24.6 ± 3.4 | <0.001 | 24.6 ± 3.5 | 24.6 ± 3.5 | 24.6 ± 3.5 | 0.720 |
| Waist circumstance (cm) | 82.4 ± 10.2 | 82.2 ± 10.3 | 84.0 ± 9.4 | <0.001 | 83.9 ± 9.7 | 83.7 ± 9.9 | 84.1 ± 9.5 | 0.258 |
| SBP (mm Hg) | 119.0 ± 16.9 | 118.7 ± 16.8 | 122.1 ± 17.5 | <0.001 | 120.5 ± 16.9 | 119.3 ± 16.3 | 121.8 ± 17.4 | <0.001 |
| DBP (mm Hg) | 75.3 ± 10.1 | 75.0 ± 10.1 | 77.7 ± 10.2 | <0.001 | 76.5 ± 10.0 | 75.1 ± 9.6 | 77.9 ± 10.3 | <0.001 |
| Glucose (mg/dL) | 100.8 ± 23.0 | 100.7 ± 22.9 | 101.4 ± 24.5 | 0.367 | 100.6 ± 22.2 | 99.4 ± 19.1 | 101.8 ± 24.8 | 0.004 |
| TC (mg/dL) | 192.6 ± 37.7 | 185.8 ± 32.0 | 257.9 ± 24.4 | <0.001 | 223.5 ± 45.0 | 188.6 ± 31.5 | 258.4 ± 24.9 | <0.001 |
| HDL-C (mg/dL) | 51.2 ± 12.6 | 51.1 ± 12.7 | 52.4 ± 11.9 | 0.002 | 51.3 ± 12.0 | 50.3 ± 12.1 | 52.3 ± 11.7 | <0.001 |
| TG (mg/dL) | 131.4 ± 92.7 | 131.1 ± 94.9 | 134.4 ± 68.1 | 0.115 | 133.5 ± 81.6 | 130.2 ± 90.2 | 136.8 ± 72.0 | 0.026 |
| LDL-C (mg/dL) | 115.1 ± 34.0 | 108.5 ± 28.0 | 178.7 ± 17.9 | <0.001 | 145.5 ± 40.4 | 112.2 ± 26.9 | 178.7 ± 18.1 | <0.001 |
| WBC count (×103/µL) | 6.2 ± 1.8 | 6.2 ± 1.8 | 6.2 ± 1.8 | 0.379 | 6.2 ± 1.8 | 6.2 ± 1.7 | 6.3 ± 1.8 | 0.142 |
| CRP | 1.22 ± 2.00 | 1.20 ± 2.00 | 1.39 ± 2.04 | 0.001 | 1.33 ± 2.03 | 1.29 ± 2.03 | 1.37 ± 2.03 | 0.284 |
| Uric acid | 5.05 ± 1.37 | 5.03 ± 1.37 | 5.17 ± 1.39 | 0.001 | 5.11 ± 1.37 | 5.03 ± 1.35 | 5.20 ± 1.39 | 0.001 |
| Current alcohol drinker | 7411 (53.1) | 6822 (53.9) | 589 (45.1) | <0.001 | 1366 (46.1) | 678 (45.7) | 688 (46.4) | 0.713 |
| Current smoker | 5089 (36.5) | 4669 (36.9) | 420 (32.2) | 0.001 | 996 (33.6) | 499 (33.7) | 497 (33.5) | 0.938 |
| Physically active | 5868 (43.3) | 5363 (43.7) | 505 (40.1) | 0.014 | 1187 (40.0) | 591 (39.9) | 596 (40.2) | 0.851 |
| Comorbidity | ||||||||
| HTN | 4608 (32.9) | 4226 (33.2) | 382 (29.2) | 0.003 | 884 (29.8) | 453 (30.6) | 431 (29.1) | 0.377 |
| DM | 1793 (12.8) | 1693 (13.3) | 100 (7.6) | <0.001 | 231 (7.8) | 109 (7.4) | 122 (8.2) | 0.373 |
| Before Propensity Score—Matching | After Propensity Score—Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| Total (N = 14,057) | Non-hLDL (N = 12,745) | hLDL (N = 1312) | p-Value | Total (N = 2966) | Non-hLDL (N = 1483) | hLDL (N = 1483) | p-Value | |
| Total calories (kcal) | 1809.5 ± 777.9 | 1813.6 ± 778.9 | 1770.0 ± 768.1 | 0.070 | 1869.9 ± 832.9 | 1883.4 ± 843.7 | 1856.0 ± 821.7 | 0.401 |
| Carbohydrates (%) | 66.0 ± 11.9 | 66.0 ± 11.9 | 66.1 ± 12.1 | 0.932 | 66.4 ± 11.7 | 66.9 ± 11.6 | 65.9 ± 11.8 | 0.021 |
| Carbohydrates (g) | 293.0 ± 123.6 | 293.6 ± 123.9 | 286.5 ± 120.6 | 0.062 | 294.2 ± 125.3 | 298.1 ± 128.2 | 290.1 ± 122.1 | 0.102 |
| Proteins (%) | 14.8 ± 4.5 | 14.8 ± 4.5 | 14.7 ± 4.5 | 0.449 | 14.7 ± 4.4 | 14.5 ± 4.3 | 14.8 ± 4.5 | 0.190 |
| Proteins (g) | 67.4 ± 37.8 | 67.7 ± 37.8 | 65.3 ± 37.1 | 0.045 | 66.6 ± 37.0 | 66.6 ± 36.5 | 66.6 ± 37.6 | 0.999 |
| Fats (%) | 19.2 ± 9.7 | 19.2 ± 9.7 | 19.3 ± 9.8 | 0.807 | 18.9 ± 9.5 | 18.5 ± 9.3 | 19.4 ± 9.6 | 0.025 |
| Fats (g) | 40.9 ± 32.9 | 40.9 ± 32.8 | 40.3 ± 33.4 | 0.534 | 39.9 ± 31.2 | 39.1 ± 30.1 | 40.7 ± 32.3 | 0.211 |
| SFA (%) | 6.1 ± 3.7 | 6.1 ± 3.7 | 6.2 ± 3.7 | 0.580 | 6.0 ± 3.6 | 5.9 ± 3.5 | 6.2 ± 3.6 | 0.013 |
| MUFA (%) | 6.0 ± 3.8 | 6.0 ± 3.8 | 6.0 ± 3.9 | 0.819 | 5.9 ± 3.7 | 5.8 ± 3.6 | 6.0 ± 3.8 | 0.163 |
| PUFA (%) | 5.2 ± 2.9 | 5.2 ± 2.9 | 5.2 ± 2.9 | 0.696 | 5.2 ± 2.8 | 5.1 ± 2.8 | 5.3 ± 2.9 | 0.111 |
| PUFA/SFA | 1.09 ± 0.71 | 1.09 ± 0.71 | 1.08 ± 0.72 | 0.563 | 1.10 ± 0.73 | 1.12 ± 0.74 | 1.08 ± 0.72 | 0.247 |
| (PUFA + MUFA)/ SFA | 2.12 ± 0.96 | 2.12 ± 0.96 | 2.08 ± 0.96 | 0.169 | 2.12 ± 0.97 | 2.15 ± 0.99 | 2.09 ± 0.96 | 0.106 |
| N-3 PUFA (%) | 0.90 ± 0.89 | 0.89 ± 0.88 | 0.96 ± 0.96 | 0.022 | 0.91 ± 0.86 | 0.89 ± 0.81 | 0.93 ± 0.90 | 0.191 |
| N-6 PUFA (%) | 4.30 ± 2.47 | 4.30 ± 2.47 | 4.27 ± 2.44 | 0.670 | 4.29 ± 2.45 | 4.22 ± 2.39 | 4.36 ± 2.50 | 0.145 |
| N-6 PUFA N-3 PUFA | 6.79 ± 4.87 | 6.81 ± 4.91 | 6.56 ± 4.45 | 0.062 | 6.75 ± 6.52 | 6.64 ± 4.95 | 6.86 ± 7.81 | 0.381 |
| Cholesterol (mg) | 218.7 ± 210.8 | 219.2 ± 210.0 | 213.4 ± 219.0 | 0.368 | 215.5 ± 212.7 | 214.2 ± 206.6 | 216.1 ± 218.8 | 0.751 |
| Fiber (g) | 25.3 ± 14.4 | 25.3 ± 14.0 | 25.30 ± 14.3 | 0.966 | 25.9 ± 14.9 | 26.1 ± 15.2 | 25.8 ± 14.5 | 0.646 |
| Na (g) | 3.3 ± 2.1 | 3.3 ± 2.1 | 3.1 ± 2.1 | 0.048 | 3.2 ± 2.1 | 3.2 ± 2.0 | 3.2 ± 2.1 | 0.735 |
| K (g) | 2.8 ± 1.4 | 2.8 ± 1.4 | 2.8 ± 1.4 | 0.694 | 2.8 ± 1.4 | 2.8 ± 1.4 | 2.9 ± 1.4 | 0.315 |
| Na/K | 1.25 ± 0.67 | 1.25 ± 0.67 | 1.19 ± 0.64 | 0.002 | 1.22 ± 0.65 | 1.2 ± 0.68 | 1.19 ± 0.62 | 0.050 |
| Before Propensity Score—Matching | After Propensity Score—Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| Total (N = 14,057) | Non-hTG (N = 12,015) | hTG (N = 2042) | p-Value | Total (N = 3590) | Non-hTG (N = 1795) | hTG (N = 1795) | p-Value | |
| Sex (male) | 5955 (42.4) | 4713 (39.2) | 1242 (60.8) | <0.001 | 2168 (60.4) | 1107 (61.7) | 1061 (59.1) | 0.117 |
| Age (y) | 52.0 ± 16.9 | 51.7 ± 17.2 | 53.5 ± 14.9 | <0.001 | 54.1 ± 15.7 | 54.4 ± 16.6 | 53.7 ± 14.7 | 0.138 |
| BMI (kg/m2) | 23.9 ± 3.5 | 23.7 ± 3.5 | 25.7 ± 3.4 | <0.001 | 25.3 ± 3.2 | 25.2 ± 3.3 | 25.3 ± 3.1 | 0.214 |
| Waist circumstance (cm) | 82.4 ± 10.2 | 81.3 ± 10.1 | 88.5 ± 8.7 | <0.001 | 87.1 ± 8.6 | 86.5 ± 9.1 | 87.7 ± 8.1 | <0.001 |
| SBP (mm Hg) | 119.0 ± 16.9 | 118.2 ± 16.8 | 124.1 ± 16.0 | <0.001 | 122.8 ± 16.4 | 121.8 ± 16.6 | 123.8 ± 16.1 | 0.002 |
| DBP (mm Hg) | 75.3 ± 10.1 | 74.6 ± 9.8 | 79.4 ± 10.8 | <0.001 | 77.7 ± 10.4 | 76.3 ± 10.1 | 79.2 ± 10.5 | <0.001 |
| Glucose (mg/dL) | 100.8 ± 23.0 | 99.3 ± 21.2 | 109.6 ± 30.4 | <0.001 | 106.6 ± 27.5 | 105.0 ± 25.5 | 108.2 ± 29.1 | 0.004 |
| TC (mg/dL) | 192.6 ± 37.7 | 189.6 ± 36.4 | 210.3 ± 40.3 | <0.001 | 199.5 ± 39.8 | 187.9 ± 36.1 | 211.2 ± 40.0 | <0.001 |
| HDL-C (mg/dL) | 51.2 ± 12.6 | 52.7 ± 12.4 | 42.2 ± 9.4 | <0.001 | 46.1 ± 11.2 | 50.0 ± 11.6 | 42.3 ± 9.3 | <0.001 |
| TG (mg/dL) | 131.4 ± 92.7 | 103.0 ± 41.7 | 298.5 ± 127.6 | <0.001 | 205.3 ± 132.6 | 112.0 ± 41.6 | 298.5 ± 126.6 | <0.001 |
| LDL-C (mg/dL) | 115.1 ± 34.0 | 116.2 ± 32.8 | 108.5 ± 39.8 | <0.001 | 112.3 ± 36.5 | 115.5 ± 32.8 | 109.2 ± 39.7 | <0.001 |
| WBC count (×103/µL) | 6.2 ± 1.8 | 6.1 ± 1.7 | 6.9 ± 1.8 | <0.001 | 6.6 ± 1.7 | 6.4 ± 1.7 | 6.8 ± 1.8 | <0.001 |
| CRP | 1.22 ± 2.0 | 1.19 ± 2.05 | 1.37 ± 1.74 | <0.001 | 1.33 ± 1.90 | 1.34 ± 2.09 | 1.33 ± 1.69 | 0.891 |
| Uric acid | 5.05 ± 1.37 | 4.92 ± 1.31 | 5.77 ± 1.45 | <0.001 | 5.52 ± 1.42 | 5.30 ± 1.35 | 5.74 ± 1.45 | <0.001 |
| Current alcohol drinker | 7411 (53.1) | 6189 (51.9) | 1222 (60.3) | <0.001 | 2142 (59.7) | 1080 (60.2) | 1062 (59.2) | 0.540 |
| Current smoker | 5089 (36.5) | 3973 (33.3) | 1116 (55.0) | <0.001 | 1921 (53.5) | 977 (54.4) | 944 (52.6) | 0.270 |
| Physically active | 5868 (43.3) | 5093 (44.0) | 775 (39.7) | 0.001 | 1444 (40.2) | 726 (40.5) | 718 (40.0) | 0.785 |
| Comorbidity | ||||||||
| HTN | 4608 (32.9) | 3693 (30.8) | 915(44.9) | <0.001 | 1508 (42.0) | 745 (41.5) | 763 (42.5) | 0.543 |
| DM | 1793 (12.8) | 1365 (11.4) | 428 (21.0) | <0.001 | 665 (18.5) | 329 (18.3) | 336 (18.7) | 0.764 |
| Before Propensity Score—Matching | After Propensity Score—Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| Total (N = 14,075) | Non-hTG (N = 12,015) | hTG (N = 2042) | p-Value | Total (N = 3590) | Non-hTG (N = 1795) | hTG (N = 1795) | p-Value | |
| Total calories (kcal) | 1809.5 ± 777.9 | 1799.0 ± 767.8 | 1873.6 ± 834.0 | 0.005 | 2025.6 ± 924.6 | 2010.2 ± 907.8 | 2041.5 ± 941.6 | 0.343 |
| Carbohydrates (%) | 66.0 ± 11.9 | 65.9 ± 11.9 | 66.7 ± 12.0 | 0.008 | 66.5 ± 11.9 | 66.4 ± 11.8 | 66.6 ± 12.0 | 0.640 |
| Carbohydrates (g) | 293.0 ± 123.6 | 290.9 ± 121.3 | 305.5 ± 136.5 | <0.001 | 307.0 ± 132.2 | 307.4 ± 128.6 | 306.7 ± 135.9 | 0.892 |
| Proteins (%) | 14.8 ± 4.5 | 14.8 ± 4.5 | 14.8 ± 4.5 | 0.583 | 14.8 ± 4.4 | 14.9 ± 4.3 | 14.8 ± 4.5 | 0.704 |
| Proteins (g) | 67.4 ± 37.8 | 67.0 ± 37.4 | 70.4 ± 40.1 | 0.007 | 71.0 ± 39.6 | 71.0 ± 39.2 | 70.9 ± 40.0 | 0.905 |
| Fats (%) | 19.2 ± 9.7 | 19.3 ± 9.7 | 18.4 ± 9.9 | 0.004 | 18.7 ± 9.8 | 18.7 ± 9.7 | 18.6 ± 9.8 | 0.689 |
| Fats (g) | 40.9 ± 32.9 | 40.8 ± 32.6 | 41.1 ± 34.2 | 0.780 | 41.7 ± 33.9 | 41.9 ± 33.9 | 41.5 ± 34.0 | 0.734 |
| SFA (%) | 6.15 ± 3.71 | 6.20 ± 3.71 | 5.85 ± 3.73 | 0.003 | 5.92 ± 3.67 | 5.95 ± 3.58 | 5.89 ± 3.75 | 0.663 |
| MUFA (%) | 6.00 ± 3.80 | 6.05 ± 3.78 | 5.71 ± 3.91 | 0.006 | 5.80 ± 3.86 | 5.83 ± 3.81 | 5.76 ± 3.90 | 0.670 |
| PUFA (%) | 5.20 ± 2.86 | 5.23 ± 2.87 | 5.05 ± 2.84 | 0.018 | 5.13 ± 2.83 | 5.16 ± 2.83 | 5.09 ± 2.84 | 0.487 |
| PUFA/SFA | 1.09 ± 0.71 | 1.08 ± 0.71 | 1.14 ± 0.77 | 0.007 | 1.12 ± 0.74 | 1.11 ± 0.71 | 1.14 ± 0.76 | 0.213 |
| (PUFA + MUFA)/SFA | 2.12 ± 0.96 | 2.11 ± 0.95 | 2.16 ± 1.02 | 0.052 | 2.15 ± 0.98 | 2.13 ± 0.96 | 2.17 ± 1.01 | 0.246 |
| N-3 PUFA (%) | 0.90 ± 0.89 | 0.89 ± 0.88 | 0.91 ± 0.90 | 0.532 | 0.89 ± 0.82 | 0.88 ± 0.76 | 0.91 ± 0.87 | 0.286 |
| N-6 PUFA (%) | 4.30 ± 2.47 | 4.33 ± 2.48 | 4.13 ± 2.40 | 0.002 | 4.23 ± 2.43 | 4.28 ± 2.44 | 4.18 ± 2.41 | 0.245 |
| N-6 PUFA N-3 PUFA | 6.79 ± 4.87 | 6.82 ± 4.96 | 6.62 ± 4.33 | 0.076 | 6.63 ± 4.27 | 6.64 ± 4.26 | 6.62 ± 4.27 | 0.883 |
| Cholesterol (mg) | 218.7 ± 210.8 | 218.7 ± 208.9 | 218.5 ± 222.1 | 0.972 | 220.1 ± 220.6 | 220.6 ± 219.3 | 219.5 ± 222.1 | 0.889 |
| Fiber (g) | 25.3 ± 14.4 | 25.2 ± 14.4 | 26.1 ± 14.4 | 0.021 | 26.4 ± 14.4 | 26.6 ± 14.6 | 26.2 ± 14.3 | 0.491 |
| Na (mg) | 3.3 ± 2.1 | 3.2 ± 2.1 | 3.6 ± 2.3 | <0.001 | 3.6 ± 2.3 | 3.5 ± 2.4 | 3.6 ± 2.3 | 0.316 |
| K (mg) | 2.8 ± 1.4 | 2.8 ± 1.4 | 2.9 ± 1.5 | 0.002 | 2.9 ± 1.5 | 3.0 ± 1.5 | 2.9 ± 1.4 | 0.338 |
| Na/K | 1.25 ± 0.67 | 1.23 ± 0.67 | 1.31 ± 0.67 | <0.001 | 1.28 ± 0.67 | 1.26 ± 0.68 | 1.30 ± 0.66 | 0.049 |
| Before Propensity Score—Matching | After Propensity Score—Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| Total (N = 3040) | hTG-Only (N = 1899) | hLDL-Only (N = 1141) | p-Value | Total (N = 1598) | hTG-Only (N = 799) | hLDL-Only (N = 799) | p-Value | |
| Total calories (kcal) | 1827.2 ± 805.0 | 1876.5 ± 833.9 | 1748.6 ± 750.3 | <0.001 | 1906.6 ± 878.7 | 1938.3 ± 900.6 | 1875.4 ± 856.0 | 0.177 |
| Carbohydrates (%) | 66.3 ± 11.9 | 66.6 ± 11.9 | 65.9 ± 11.8 | 0.145 | 66.6 ± 11.8 | 67.8 ± 11.6 | 65.3 ± 11.9 | <0.001 |
| Carbohydrates (g) | 296.9 ± 130.2 | 305.7 ± 136.9 | 282.8 ± 117.5 | <0.001 | 296.0 ± 131.6 | 303.0 ± 139.8 | 289.0 ± 122.7 | 0.046 |
| Proteins (%) | 14.8 ± 4.5 | 14.9 ± 4.5 | 14.7 ± 4.5 | 0.469 | 14.7 ± 4.4 | 14.4 ± 4.1 | 15.0 ± 4.6 | 0.006 |
| Proteins (g) | 68.4 ± 38.1 | 70.7 ± 39.4 | 64.7 ± 35.5 | <0.001 | 67.0 ± 36.8 | 66.3 ± 36.0 | 67.7 ± 37.5 | 0.487 |
| Fats (%) | 18.8 ± 9.7 | 18.5 ± 9.8 | 19.3 ± 9.6 | 0.034 | 18.7 ± 9.7 | 17.8 ± 9.6 | 19.6 ± 9.7 | 0.003 |
| Fats (g) | 40.7 ± 33.4 | 41.2 ± 33.9 | 39.8 ± 32.5 | 0.298 | 40.1 ± 33.5 | 38.3 ± 31.7 | 41.9 ± 35.1 | 0.041 |
| SFA (%) | 6.0 ± 3.7 | 5.9 ± 3.7 | 6.2 ± 3.6 | 0.021 | 6.0 ± 3.7 | 5.7 ± 3.7 | 6.3 ± 3.6 | 0.004 |
| MUFA (%) | 5.9 ± 3.9 | 5.8 ± 3.9 | 6.0 ± 3.9 | 0.083 | 5.9 ± 3.9 | 5.6 ± 3.8 | 6.2 ± 4.0 | 0.003 |
| PUFA (%) | 5.1 ± 2.8 | 5.1 ± 2.8 | 5.3 ± 2.9 | 0.085 | 5.1 ± 2.8 | 4.8 ± 2.7 | 5.4 ± 2.9 | <0.001 |
| PUFA/SFA | 1.11 ± 0.74 | 1.13 ± 0.76 | 1.07 ± 0.70 | 0.037 | 1.11 ± 0.75 | 1.13 ± 0.77 | 1.09 ± 0.73 | 0.267 |
| (PUFA + MUFA)/SFA | 2.13 ± 0.99 | 2.16 ± 1.01 | 2.07 ± 0.95 | 0.032 | 2.14 ± 1.01 | 2.18 ± 1.04 | 2.11 ± 0.97 | 0.200 |
| N-3 PUFA (%) | 0.92 ± 0.89 | 0.89 ± 0.87 | 0.95 ± 0.93 | 0.117 | 0.91 ± 0.90 | 0.85 ± 0.79 | 0.97 ± 0.98 | 0.011 |
| N-6 PUFA (%) | 4.21 ± 2.42 | 4.15 ± 2.41 | 4.30 ± 2.44 | 0.136 | 4.18 ± 2.39 | 3.97 ± 2.30 | 4.38 ± 2.46 | 0.001 |
| N-6 PUFA N-3 PUFA | 6.64 ± 4.45 | 6.69 ± 4.39 | 6.57 ± 4.55 | 0.527 | 6.63 ± 4.55 | 6.60 ± 4.30 | 6.67 ± 4.79 | 0.782 |
| Cholesterol (mg) | 217.9 ± 220.3 | 220.7 ± 221.8 | 213.5 ± 217.8 | 0.414 | 212.6 ± 208.8 | 205.3 ± 208.4 | 219.8 ± 209.1 | 0.195 |
| Fiber (g) | 25.7 ± 14.3 | 26.0 ± 14.3 | 25.2 ± 14.2 | 0.147 | 26.0 ± 14.3 | 26.5 ± 14.7 | 25.4 ± 13.9 | 0.151 |
| Na (mg) | 3.4 ± 2.2 | 3.6 ± 2.3 | 3.1 ± 2.0 | <0.001 | 3.3 ± 2.1 | 3.4 ± 2.1 | 3.2 ± 2.1 | 0.246 |
| K (mg) | 2.8 ± 1.4 | 2.9 ± 1.4 | 2.8 ± 1.3 | 0.082 | 2.8 ± 1.4 | 2.8 ± 1.4 | 2.8 ± 1.3 | 0.724 |
| Na/K | 1.26 ± 0.66 | 1.32 ± 0.67 | 1.18 ± 0.64 | <0.001 | 1.22 ± 0.61 | 1.26 ± 0.63 | 1.19 ± 0.59 | 0.038 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, Y.-J.; Lee, S.; Lee, H.S.; Lee, J.-W. Differing Nutrient Intake and Dietary Patterns According to the Presence of Hyper-Low-Density Lipoprotein Cholesterolemia or Hypertriglyceridemia. Nutrients 2021, 13, 3008. https://doi.org/10.3390/nu13093008
Kwon Y-J, Lee S, Lee HS, Lee J-W. Differing Nutrient Intake and Dietary Patterns According to the Presence of Hyper-Low-Density Lipoprotein Cholesterolemia or Hypertriglyceridemia. Nutrients. 2021; 13(9):3008. https://doi.org/10.3390/nu13093008
Chicago/Turabian StyleKwon, Yu-Jin, Sujee Lee, Hye Sun Lee, and Ji-Won Lee. 2021. "Differing Nutrient Intake and Dietary Patterns According to the Presence of Hyper-Low-Density Lipoprotein Cholesterolemia or Hypertriglyceridemia" Nutrients 13, no. 9: 3008. https://doi.org/10.3390/nu13093008