
Effect of Co-Administration of Curcumin with Amlodipine in Hypertension


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Animal
2.3. Plant Material and Extraction
2.4. Preparation of Rat Aortic Rings
2.5. Measurement of Vascular Tension
2.6. Measurement of Blood Pressure in SHRs
2.7. Curcumin Content of Different Solvent Extracts from C. longa by HPLC Analysis
2.8. Statistical Analysis
3. Results
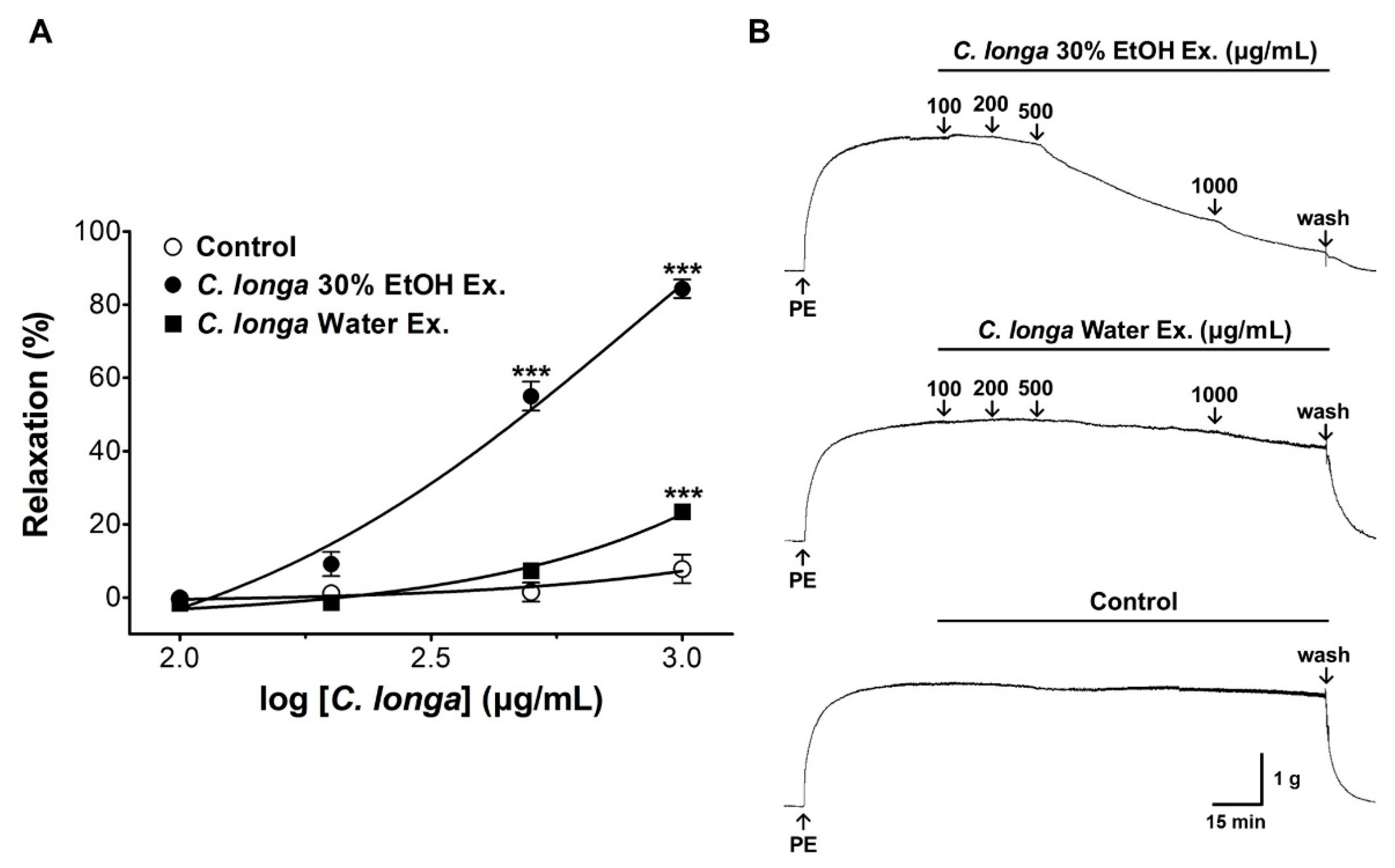
3.1. Vasorelaxant Effect of Different Extraction Solvents of C. longa
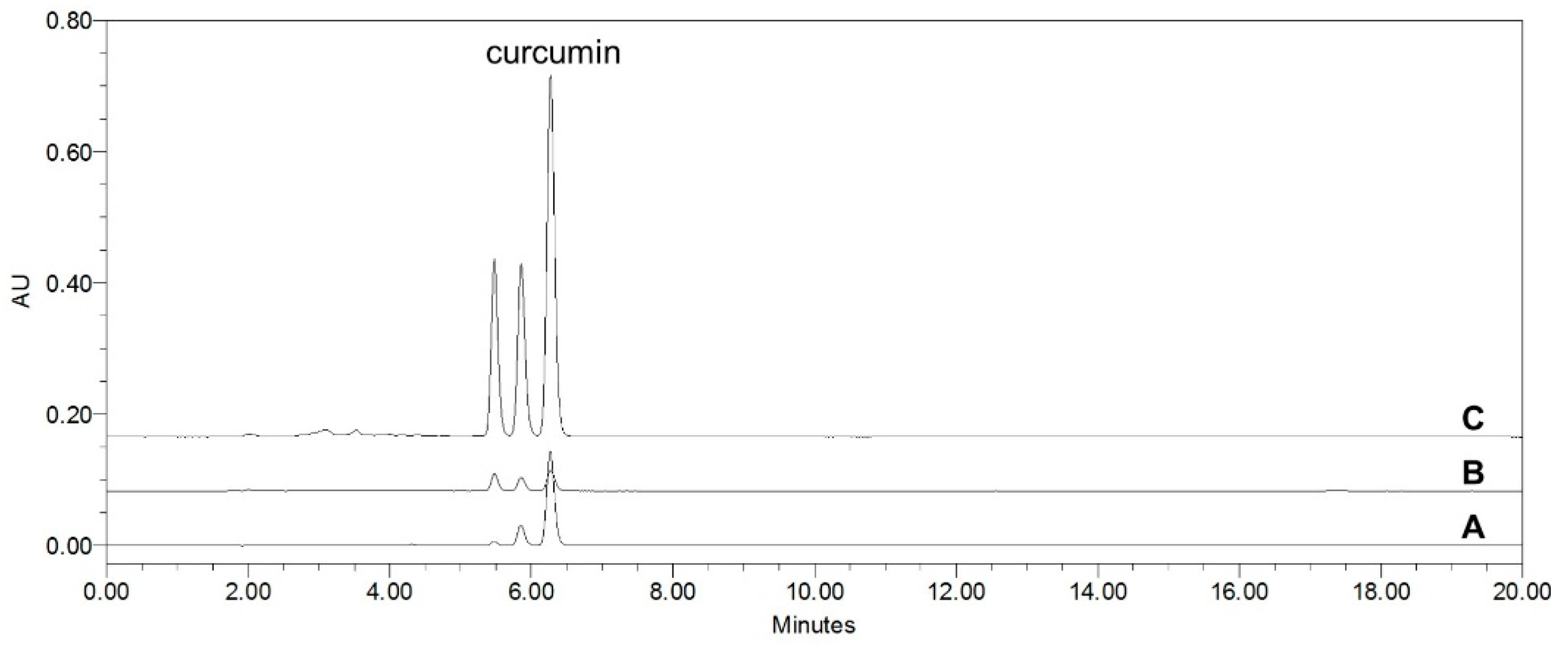
3.2. Curcumin Content of Different Solvent Extracts from C. longa by HPLC Analysis
3.3. Vasorelaxant Effect of Curcumin
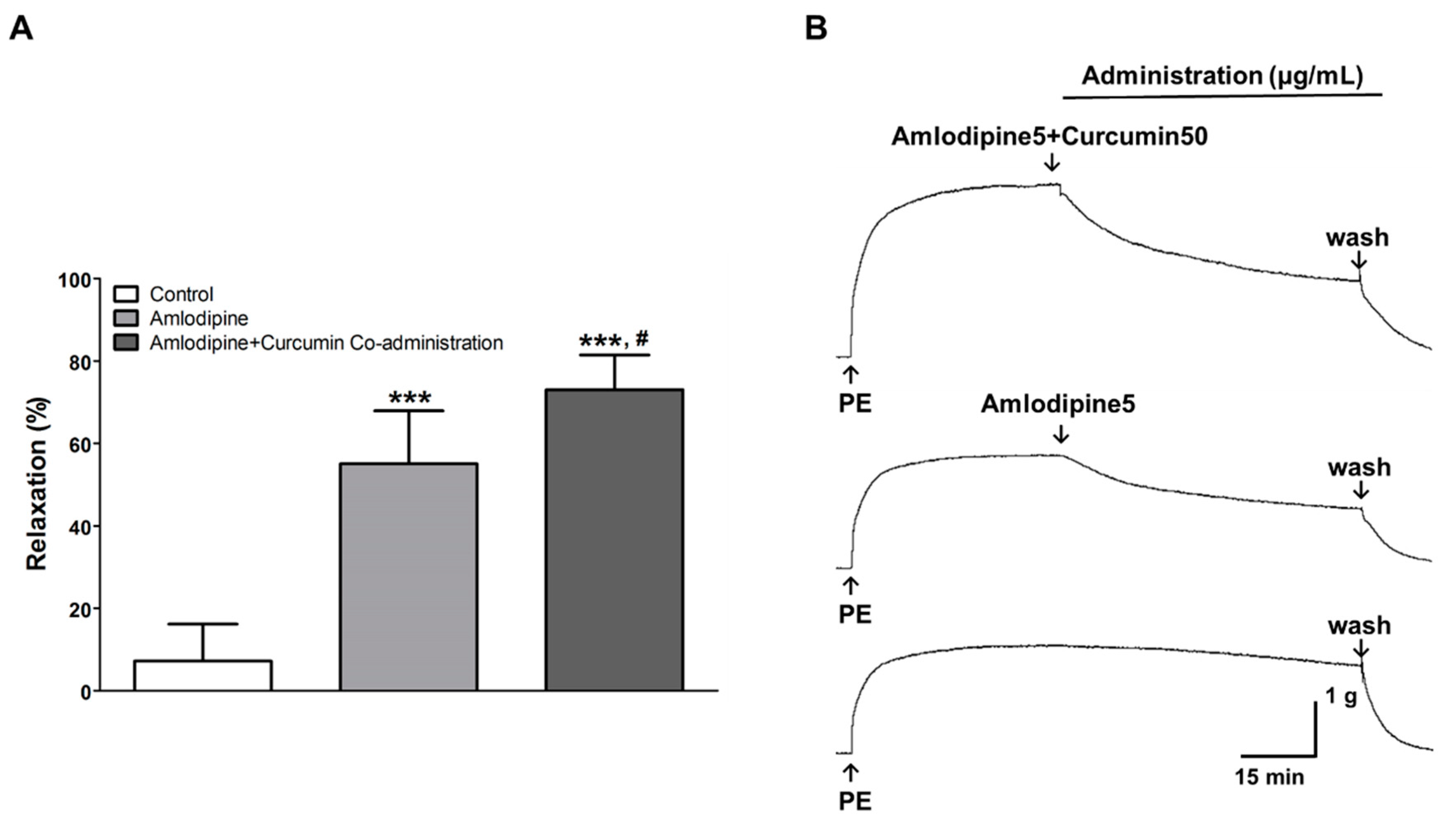
3.4. Vasorelaxant Effect of Co-Administration of Curcumin and Amlodipine
3.5. Hypotensive Effect of Co-Administration of Curcumin and Amlodipine
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Wunsche, S.; Yuan, L.; Seidel-Morgenstern, A.; Lorenz, H. A Contribution to the Solid State Forms of Bis(demethoxy)curcumin: Co-Crystal Screening and Characterization. Molecules 2021, 26, 720. [Google Scholar] [CrossRef] [PubMed]
- Damiano, S.; Longobardi, C.; Andretta, E.; Prisco, F.; Piegari, G.; Squillacioti, C.; Montagnaro, S.; Pagnini, F.; Badino, P.; Florio, S.; et al. Antioxidative Effects of Curcumin on the Hepatotoxicity Induced by Ochratoxin A in Rats. Antioxidants 2021, 10, 125. [Google Scholar] [CrossRef]
- ELBini-Dhouib, I.; Doghri, R.; Ellefi, A.; Degrach, I.; Srairi-Abid, N.; Gati, A. Curcumin Attenuated Neurotoxicity in Sporadic Animal Model of Alzheimer’s Disease. Molecules 2021, 26, 3011. [Google Scholar] [CrossRef]
- Wu, S.; Guo, T.; Qi, W.; Li, Y.; Gu, J.; Liu, C.; Sha, Y.; Yang, B.; Hu, S.; Zong, X. Curcumin ameliorates ischemic stroke injury in rats by protecting the integrity of the blood-brain barrier. Exp. Ther. Med. 2021, 22, 783. [Google Scholar] [CrossRef]
- Yao, Y.; Luo, R.; Xiong, S.; Zhang, C.; Zhang, Y. Protective effects of curcumin against rat intestinal inflammationrelated motility disorders. Mol. Med. Rep. 2021, 23, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Soetikno, V.; Sari, S.D.P.; Ul Maknun, L.; Sumbung, N.K.; Rahmi, D.N.I.; Pandhita, B.A.W.; Louisa, M.; Estuningtyas, A. Pre-Treatment with Curcumin Ameliorates Cisplatin-Induced Kidney Damage by Suppressing Kidney Inflammation and Apoptosis in Rats. Drug Res. 2018, 69, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bo, H.; Feng, X. Post-treatment curcumin reduced ischemia-reperfusion-induced pulmonary injury via the Notch2/Hes-1 pathway. J. Int. Med. Res. 2019, 48, 300060519892432. [Google Scholar]
- Huang, L.; Chen, C.; Zhang, X.; Li, X.; Chen, Z.; Yang, C.; Liang, X.; Zhu, G.; Xu, Z. Neuroprotective Effect of Curcumin Against Cerebral Ischemia-Reperfusion Via Mediating Autophagy and Inflammation. J. Mol. Neurosci. 2018, 64, 129–139. [Google Scholar] [CrossRef]
- Liu, W.; Huang, M.; Zou, Q.; Lin, W. Curcumin suppresses gastric cancer biological activity by regulation of miRNA-21: An in vitro study. Int. J. Clin. Exp. Pathol. 2018, 11, 5820–5829. [Google Scholar]
- Vaidya, F.U.; Sharma, R.; Shaikh, S.; Ray, D.; Aswal, V.K.; Pathak, C. Pluronic micelles encapsulated curcumin manifests apoptotic cell death and inhibits pro-inflammatory cytokines in human breast adenocarcinoma cells. Cancer Rep. 2019, 2, e1133. [Google Scholar] [CrossRef]
- Moradi-Marjaneh, R.; Hassanian, S.M.; Rahmani, F.; Aghaee-Bakhtiari, S.H.; Avan, A.; Khazaei, M. Phytosomal Curcumin Elicits Anti-tumor Properties Through Suppression of Angiogenesis, Cell Proliferation and Induction of Oxidative Stress in Colorectal Cancer. Curr. Pharm. Des. 2019, 24, 4626–4638. [Google Scholar] [CrossRef]
- El Nebrisi, E.; Javed, H.; Ojha, S.K.; Oz, M.; Shehab, S. Neuroprotective Effect of Curcumin on the Nigrostriatal Pathway in a 6-Hydroxydopmine-Induced Rat Model of Parkinson’s Disease is Mediated by alpha7-Nicotinic Receptors. Int. J. Mol. Sci. 2020, 21, 7329. [Google Scholar] [CrossRef]
- Amini, A.; Soleimani, H.; Rezaei, F.; Ghoreishi, S.K.; Chien, S.; Bayat, M. The Combined Effect of Photobiomodulation and Curcumin on Acute Skin Wound Healing in Rats. J. Lasers Med. Sci. 2021, 12, e9. [Google Scholar] [CrossRef] [PubMed]
- Abd-Elhakim, Y.M.; Moselhy, A.A.A.; Aldhahrani, A.; Beheiry, R.R.; Mohamed, W.A.M.; Soliman, M.M.; Saffaf, B.A.; M. El Deib, M. Protective Effect of Curcumin against Sodium Salicylate-Induced Oxidative Kidney Damage, Nuclear Factor-Kappa Dysregulation, and Apoptotic Consequences in Rats. Antioxidants 2021, 10, 826. [Google Scholar] [CrossRef]
- Ibrahim, K.G.; Wright, H.L.; Chivandi, E.; Madziva, M.T.; Erlwanger, K.H. The potential developmental programming effect of oral curcumin on the bone health and plasma total osteocalcin of male and female rats fed a high-fructose diet during suckling and post weaning. Gen. Physiol. Biophys. 2019, 38, 435–444. [Google Scholar] [CrossRef] [Green Version]
- Lan, C.; Chen, X.; Zhang, Y.; Wang, W.; Wang, W.E.; Liu, Y.; Cai, Y.; Ren, H.; Zheng, S.; Zhou, L.; et al. Curcumin prevents strokes in stroke-prone spontaneously hypertensive rats by improving vascular endothelial function. BMC Cardiovasc. Disord. 2018, 18, 43. [Google Scholar] [CrossRef] [Green Version]
- Boonla, O.; Kukongviriyapan, U.; Pakdeechote, P.; Kukongviriyapan, V.; Pannangpetch, P.; Prachaney, P.; Greenwald, S.E. Curcumin improves endothelial dysfunction and vascular remodeling in 2K-1C hypertensive rats by raising nitric oxide availability and reducing oxidative stress. Nitric Oxide 2014, 42, 44–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, Y.; Sun, H.J.; Tong, Y.; Chen, Y.Z.; Ye, C.; Qiu, Y.; Zhang, F.; Chen, A.D.; Qi, X.H.; Chen, Q.; et al. Curcumin attenuates migration of vascular smooth muscle cells via inhibiting NFkappaB-mediated NLRP3 expression in spontaneously hypertensive rats. J. Nutr. Biochem. 2019, 72, 108212. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, e177–e232. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.J.; Jeon, J.Y.; Yu, K.S.; Kim, M.G. Pharmacokinetic Interaction Among Telmisartan, Amlodipine, and Hydrochlorothiazide After a Single Oral Administration in Healthy Male Subjects. Clin. Ther. 2019, 41, 2273–2282. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar]
- Amlodipine-Drug Usage Statistics, United States, 2008–2018. Available online: https://clincalc.com/DrugStats/Drugs/Amlodipine (accessed on 19 February 2021).
- Setyaningsih, D.; Santoso, Y.A.; Hartini, Y.S.; Murti, Y.B.; Hinrichs, W.L.J.; Patramurti, C. Isocratic high-performance liquid chromatography (HPLC) for simultaneous quantification of curcumin and piperine in a microparticle formulation containing Curcuma longa and Piper nigrum. Heliyon 2021, 7, e06541. [Google Scholar] [CrossRef]
- Moghtaderi, H.; Sepehri, H.; Attari, F. Combination of arabinogalactan and curcumin induces apoptosis in breast cancer cells in vitro and inhibits tumor growth via overexpression of p53 level in vivo. Biomed. Pharmacother. 2017, 88, 582–594. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, A.; Rateri, D.; Hong, L.; Balakrishnan, A. Measuring blood pressure in mice using volume pressure recording, a tail-cuff method. JoVE 2009, 29, e14280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pourhabibi-Zarandi, F.; Shojaei-Zarghani, S.; Rafraf, M. Curcumin and rheumatoid arthritis: A systematic review of literature. Int. J. Clin. Pract. 2021, e14280. [Google Scholar] [CrossRef]
- Choi, Y.; Kim, W.; Lee, J.S.; Youn, S.J.; Lee, H.; Baik, M.Y. Enhanced Antioxidant Capacity of Puffed Turmeric (Curcuma longa L.) by High Hydrostatic Pressure Extraction (HHPE) of Bioactive Compounds. Foods 2020, 9, 1690. [Google Scholar] [CrossRef] [PubMed]
- Akter, J.; Islam, M.Z.; Hossain, M.A.; Kawabata, S.; Takara, K.; Nguyen, H.T.T.; Hou, D.X.; Miyamoto, A. Endothelium-independent and calcium channel-dependent relaxation of the porcine cerebral artery by different species and strains of turmeric. J. Tradit. Complement. Med. 2019, 9, 297–303. [Google Scholar] [CrossRef]
- Clark, M.; Finkel, R.; Rey, J.; Whalen, K. Antihypertensives. In Pharmacology, 5th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Balimore, MD, USA, 2012; pp. 227–242. [Google Scholar]
- Bulsara, K.G.; Cassagnolm, M. Amlodipine. Available online: https://www.ncbi.nlm.nih.gov/books/NBK519508/ (accessed on 23 June 2021).
- Athyros, V.G.; Katsiki, N.; Karagiannis, A. Cardiovascular risk reduction with combination of anti-atherosclerotic medications in younger and older patients. Curr. Med. Res. Opin. 2013, 29, 791–792. [Google Scholar] [CrossRef] [Green Version]
- Teo, K.K.; Pfeffer, M.; Mancia, G.; O’Donnell, M.; Dagenais, G.; Diaz, R.; Dans, A.; Liu, L.; Bosch, J.; Joseph, P.; et al. Aliskiren alone or with other antihypertensives in the elderly with borderline and stage 1 hypertension: The APOLLO trial. Eur. Heart J. 2014, 35, 1743–1751. [Google Scholar] [CrossRef] [Green Version]
- Brook, R.D.; Kaciroti, N.; Bakris, G.; Dahlof, B.; Pitt, B.; Velazquez, E.; Weber, M.; Zappe, D.H.; Hau, T.; Jamerson, K.A. Prior Medications and the Cardiovascular Benefits From Combination Angiotensin-Converting Enzyme Inhibition Plus Calcium Channel Blockade Among High-Risk Hypertensive Patients. J. Am. Heart Assoc. 2018, 7, e006940. [Google Scholar] [CrossRef] [Green Version]
- Ruilope, L.M. Fixed-Combination Olmesartan/Amlodipine Was Superior to Perindopril + Amlodipine in Reducing Central Systolic Blood Pressure in Hypertensive Patients With Diabetes. J. Clin. Hypertens. 2016, 18, 528–535. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.; Jo, C.; Choi, H.Y.; Lee, K. Vasorelaxant and Hypotensive Effects of Cheonwangbosimdan in SD and SHR Rats. Evid. Based Complement. Alternat. Med. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B. Bioavailability of curcumin: Problems and promises. Mol. Pharm. 2007, 4, 807–818. [Google Scholar] [CrossRef]
- Cheng, A.L.; Hsu, C.H.; Lin, J.K.; Hsu, M.M.; Ho, Y.F.; Shen, T.S.; Ko, J.Y.; Lin, J.T.; Lin, B.R.; Ming-Shiang, W.; et al. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res. 2001, 21, 2895–2900. [Google Scholar] [PubMed]
- National Toxicology Program. NTP Toxicology and Carcinogenesis Studies of Turmeric Oleoresin (CAS No. 8024-37-1) (Major Component 79%–85% Curcumin, CAS No. 458-37-7) in F344/N Rats and B6C3F1 Mice (Feed Studies). Natl. Toxicol. Program Tech. Rep. Ser. 1993, 427, 1–275. [Google Scholar]
- Sharma, R.A.; Steward, W.P.; Gescher, A.J. Pharmacokinetics and pharmacodynamics of curcumin. Adv. Exp. Med. Biol. 2007, 595, 453–470. [Google Scholar] [PubMed] [Green Version]
- Goel, A.; Kunnumakkara, A.B.; Aggarwal, B.B. Curcumin as “Curecumin”: From kitchen to clinic. Biochem. Pharmacol. 2008, 75, 787–809. [Google Scholar] [CrossRef] [Green Version]
- Kwon, Y. Estimation of curcumin intake in Korea based on the Korea National Health and Nutrition Examination Survey (2008–2012). Nutr. Res. Pract. 2014, 8, 589–594. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, M.L.; Chacko, K.M.; Kuruvilla, B.T. Systematic and comprehensive investigation of the toxicity of curcuminoidessential oil complex: A bioavailable turmeric formulation. Mol. Med. Rep. 2016, 13, 592–604. [Google Scholar] [CrossRef] [Green Version]
- Phipps, K.R.; Quesnot, N.; Privat, K.; Baldwin, N.J.; Ahlborn, E.; Fanca-Berthon, P. Toxicological safety evaluation of a novel highly bioavailable turmeric extract formulation. J. Appl. Toxicol. 2020, 40, 285–299. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Jo, C.; Choi, H.-Y.; Lee, K. Effect of Co-Administration of Curcumin with Amlodipine in Hypertension. Nutrients 2021, 13, 2797. https://doi.org/10.3390/nu13082797
Lee S, Jo C, Choi H-Y, Lee K. Effect of Co-Administration of Curcumin with Amlodipine in Hypertension. Nutrients. 2021; 13(8):2797. https://doi.org/10.3390/nu13082797
Chicago/Turabian StyleLee, Somin, Cheolmin Jo, Ho-Young Choi, and Kyungjin Lee. 2021. "Effect of Co-Administration of Curcumin with Amlodipine in Hypertension" Nutrients 13, no. 8: 2797. https://doi.org/10.3390/nu13082797