
Impact of Percutaneous Endoscopic Gastrostomy (PEG) on the Evolution of Disease in Patients with Amyotrophic Lateral Sclerosis (ALS)

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
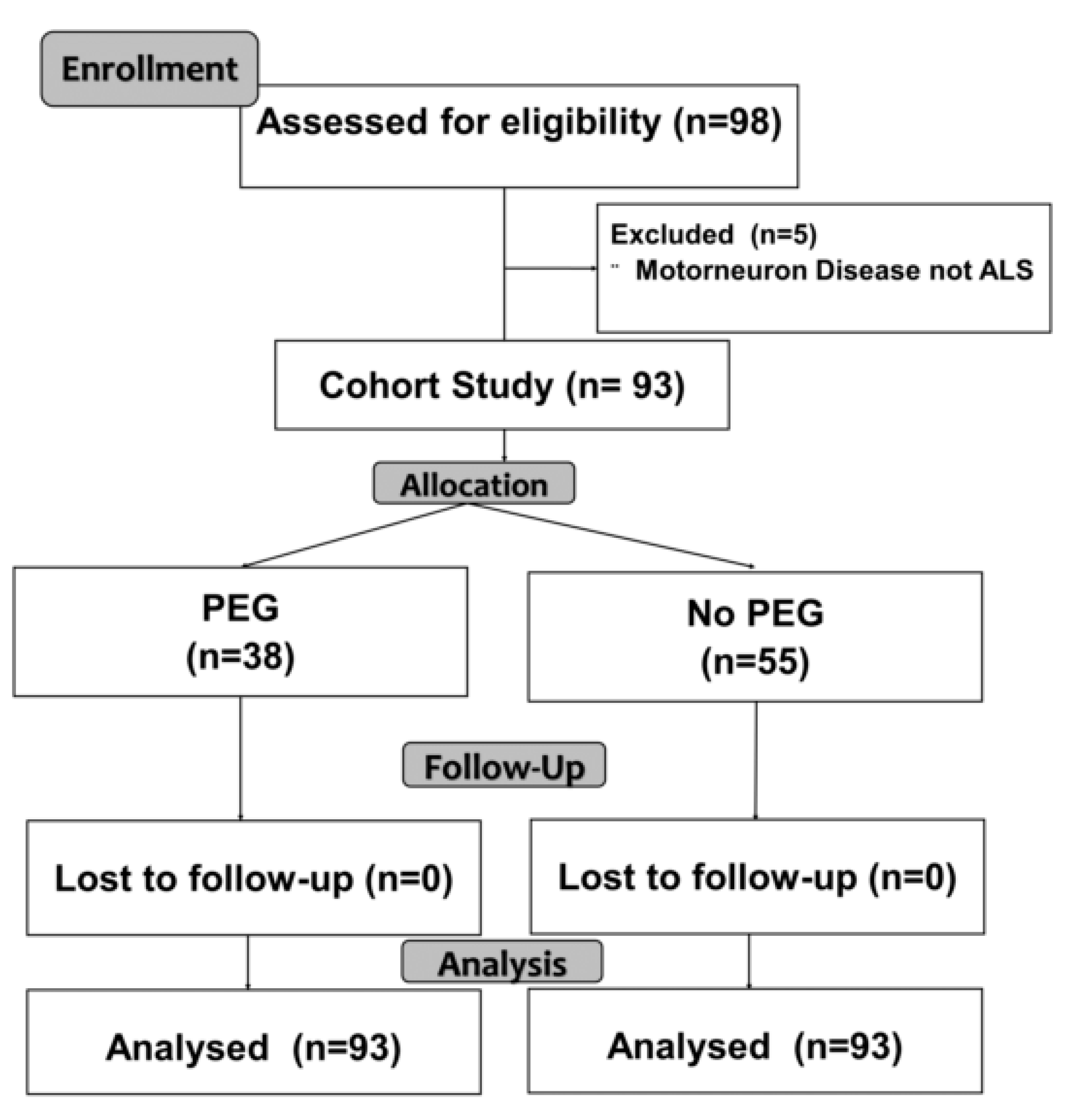
2.1. Design
2.2. Procedures
2.3. Variables
2.3.1. Characteristics of the Disease
2.3.2. Implantation of PEG
2.3.3. Anthropometry
2.3.4. Nutritional Assessment
2.4. Data Analysis
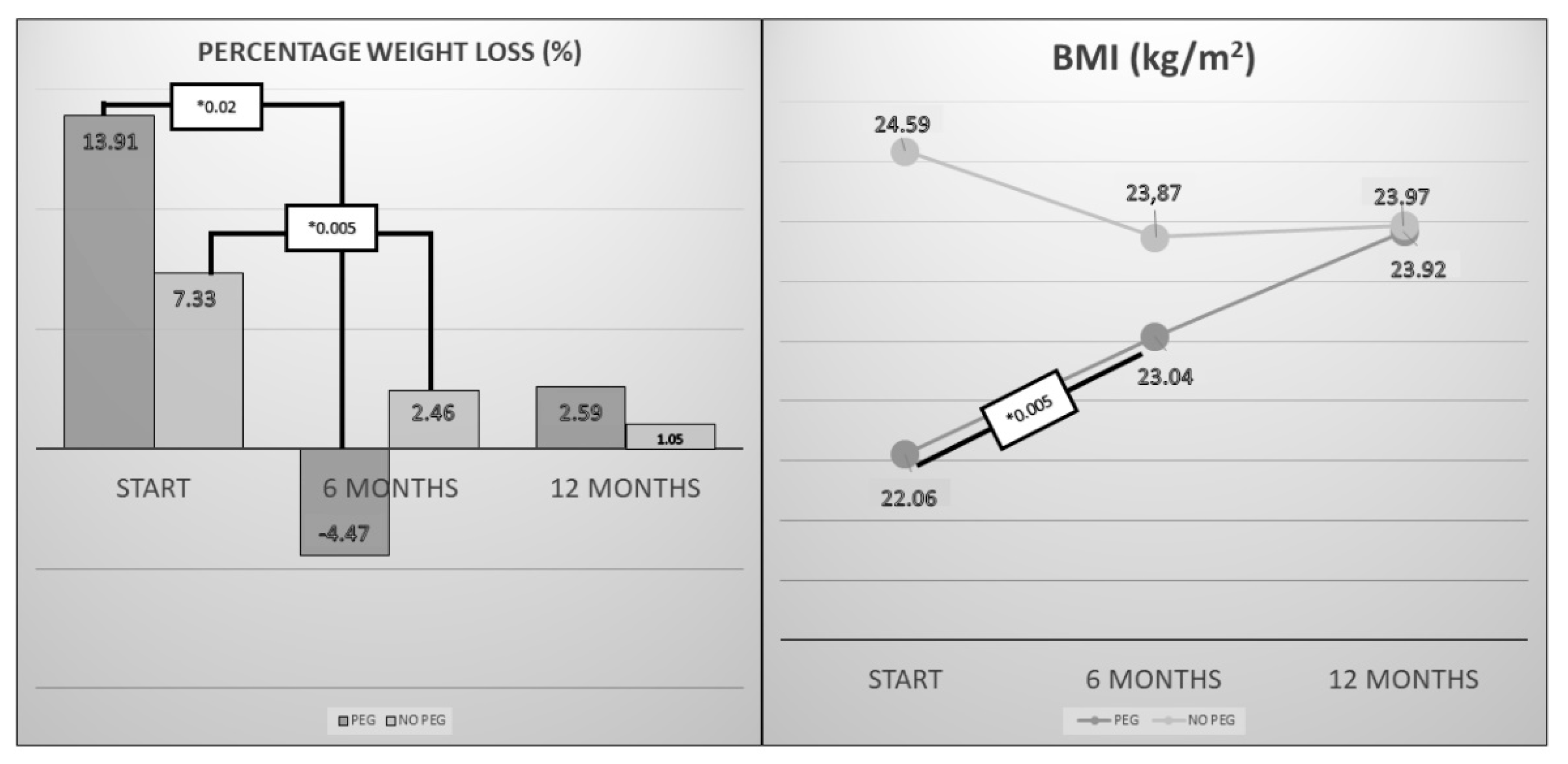
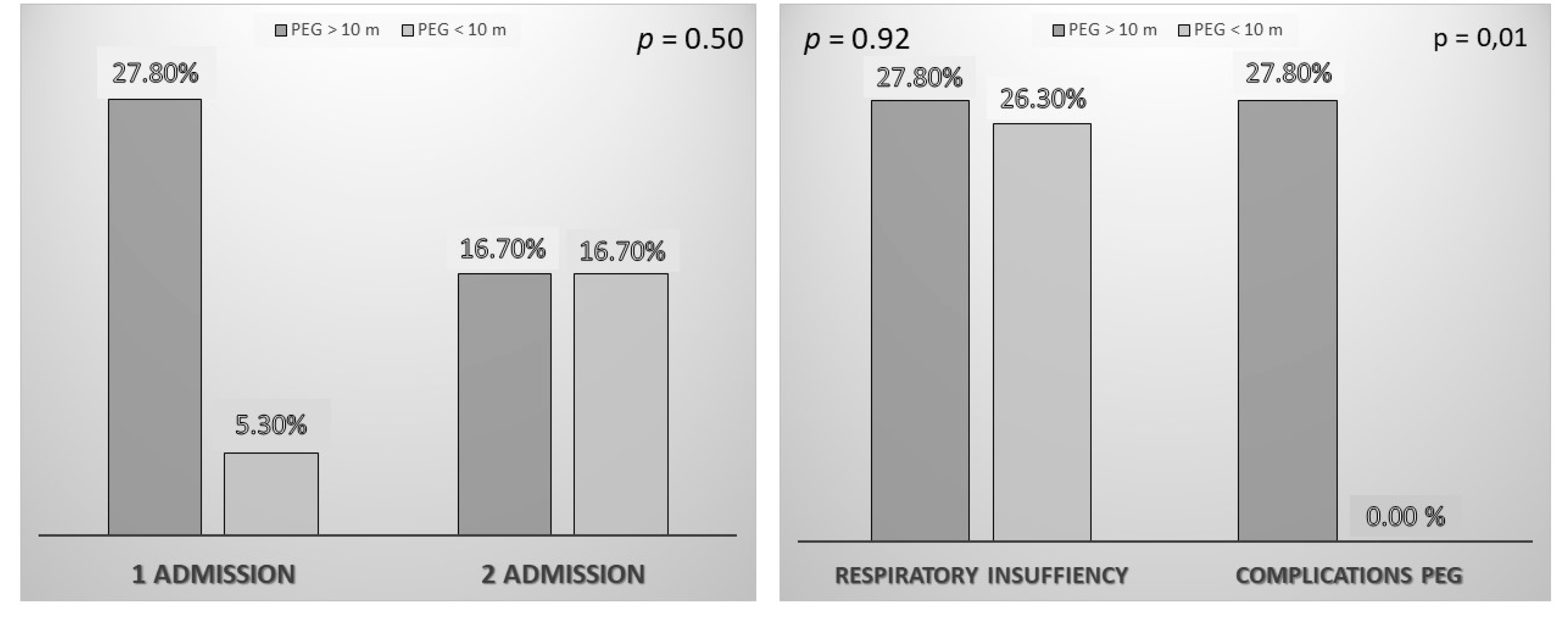
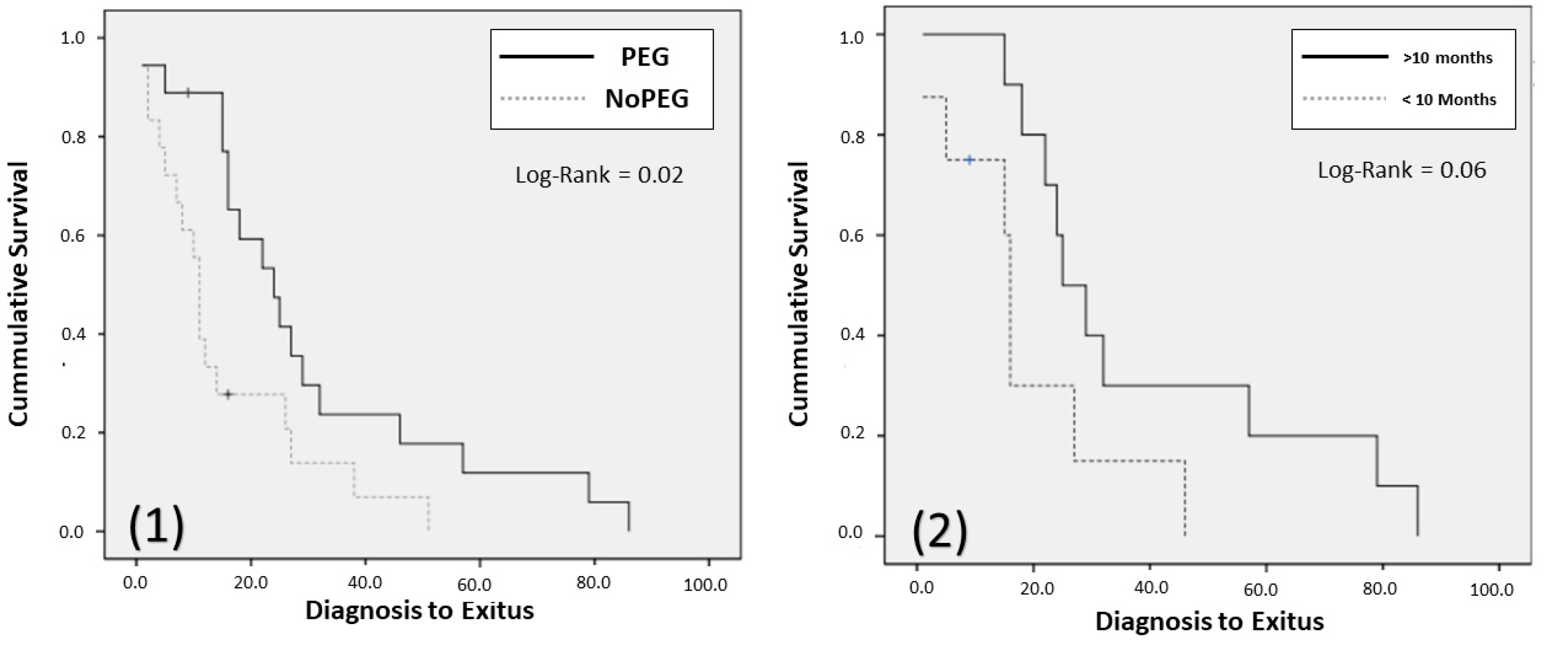
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Logroscino, G.; Traynor, B.J.; Hardiman, O.; Chio, A.; Mitchell, D.; Swingler, R.J.; Millul, A.; Benn, E.; Beghi, E.; Eurals, F. Incidence of amyotrophic lateral sclerosis in Europe. J. Neurol. Neurosurg. Psychiatry 2010, 81, 385–390. [Google Scholar] [CrossRef]
- Mehta, P.; Kaye, W.; Raymond, J.; Punjani, R.; Larson, T.; Cohen, J.; Muravov, O.; Horton, K. Prevalence of Amyotrophic Lateral Sclerosis—United States, 2015. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1285–1289. [Google Scholar] [CrossRef] [PubMed]
- Worms, P.M. The epidemiology of motor neuron diseases: A review of recent studies. J. Neurol. Sci. 2001, 191, 3–9. [Google Scholar] [CrossRef]
- Virgili Casas, M.N. La opinión del paciente cuenta: Experiencia en la atención nutricional en un equipo multidisciplinar. Nutr. Hosp. 2015, 31, 56–66. [Google Scholar] [CrossRef]
- Carbo Perseguer, J.; Madejon Seiz, A.; Romero Portales, M.; Martinez Hernandez, J.; Mora Pardina, J.S.; Garcia-Samaniego, J. Percutaneous endoscopic gastrostomy in patients with amyotrophic lateral sclerosis: Mortality and complications. Neurology 2018, 34, 582–588. [Google Scholar] [CrossRef]
- Salvioni CC dos, S.; Stanich, P.; Almeida, C.S.; Oliveira, A.S.B. Nutritional care in motor neurone disease/amyotrophic lateral sclerosis. Arq. Neuropsiquiatr. 2014, 72, 157–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prior-Sanchez, I.; Herrera-Martinez, A.D.; Jimenez, C.T.; Puerta, M.J.M.; Continente, A.J.C.; Garcia, G.M.; Moreno, G.G. Percutaneous endoscopic gastrostomy in a myotrophic lateral sclerosis. Experience in a district general hospital. Nutr. Hosp. 2014, 30, 1289–1294. [Google Scholar] [CrossRef]
- Burgos, R.; Bretón, I.; Cereda, E.; Desport, J.C.; Dziewas, R.; Genton, L.; Gomes, F.; Jésus, P.; Leischker, A.; Muscaritoli, M.; et al. ESPEN guideline clinical nutrition in neurology. Clin. Nutr. Edinb. Scotl. 2018, 37, 354–396. [Google Scholar] [CrossRef] [Green Version]
- The EFNS Task Force on Diagnosis and Management of Amyotrophic Lateral Sclerosis; Andersen, P.M.; Abrahams, S.; Borasio, G.D.; de Carvalho, M.; Chio, A.; Van Damme, P.; Hardiman, O.; Kollewe, K.; Morrison, K.; et al. EFNS guidelines on the clinical management of amyotrophic lateral sclerosis (MALS)—revised report of an EFNS task force. Eur. J. Neurol. 2012, 19, 360–375. [Google Scholar] [CrossRef] [PubMed]
- López-Gómez, J.J.; Ballesteros-Pomar, M.D.; Torres-Torres, B.; De la Maza, B.P.; Penacho-Lázaro, M.; Palacio-Mures, J.M.; Abreu-Padín, C.; López-Guzmán, A.; De Luis-Román, D.A. Malnutrition at diagnosis in amyotrophic lateral sclerosis (als) and its influence on survival: Using glim criteria. Clin. Nutr. Edinb. Scotl. 2020, 40, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Sacyl (Gerencia Regional de Salud. Dirección General de Asistencia Sanitaria). Plan Funcional para la atención a personas con Esclerosis Lateral Amiotrófica. 2015. Available online: https://www.saludcastillayleon.es/es/enfermedades-problemas-salud/ela.ficheros/1673692-PLAN-FUNCIONAL-PARA-LA-ATENCION-A-PERSONAS-CON-ELA.pdf (accessed on 13 July 2021).
- Brooks, B.R.; Miller, R.G.; Swash, M.; Munsat, T.L.; World Federation of Neurology Research Group on Motor Neuron Diseases. El Escorial revisited: Revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Mot. Neuron Disord. 2000, 1, 293–299. [Google Scholar] [CrossRef]
- Da Silva Fink, J.; Daniel de Mello, P.; Daniel de Mello, E. Subjective global assessment of nutritional status—A systematic review of the literature. Clin. Nutr. Edinb. Scotl. 2015, 34, 785–792. [Google Scholar] [CrossRef]
- Johnson, J.; Leigh, P.N.; Shaw, C.E.; Ellis, C.; Burman, R.; Al-Chalabi, A. Eating-derived pleasure in amyotrophic lateral sclerosis as a predictor of non-oral feeding. Amyotroph. Lateral Scler. Mot. Neuron Disord. 2012, 13, 555–559. [Google Scholar] [CrossRef]
- Morassutti, I.; Giometto, M.; Baruffi, C.; Marcon, M.L.; Michieletto, S.; Giometto, B.; Spinella, N.; Paccagnella, A. Nutritional intervention for amyotrophic lateral sclerosis. Minerva Gastroenterol. Dietol. 2012, 58, 253–260. [Google Scholar]
- López-Gómez, J.J.; Torres-Torres, B.; Gómez-Hoyos, E.; Fernández-Buey, N.; Ortolá-Buigues, A.; Castro-Lozano, A.; Arenillas-Lara, J.F.; De Luis-Román, D.A. Influence of a multidisciplinary protocol on nutritional status at diagnosis in amyotrophic lateral sclerosis. Nutrition 2018, 48, 67–72. [Google Scholar] [CrossRef]
- Körner, S.; Hendricks, M.; Kollewe, K.; Zapf, A.; Dengler, R.; Silani, V.; Petri, S. Weight loss, dysphagia and supplement intake in patients with amyotrophic lateral sclerosis (ALS): Impact on quality of life and therapeutic options. BMC Neurol. 2013, 13, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson-Tarlton, C.S.; Benstead, T.J.; Doucette, S. Correlating factors in the recommendation of feeding tubes in the nutritional management of amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Front. Degener. 2016, 17, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Nunes, G.; Santos, C.A.; Grunho, M.; Fonseca, J. Enteral feeding through endoscopic gastrostomy in amyotrophic lateral sclerosis patients. Nutr. Hosp. 2016, 33, 561. [Google Scholar] [CrossRef]
- Pena, M.J.; Ravasco, P.; Machado, M.; Pinto, A.; Pinto, S.; Rocha, L.; de Carvalho, M.; Pinto, H.C. What is the relevance of percutaneous endoscopic gastrostomy on the survival of patients with amyotrophic lateral sclerosis? Amyotroph. Lateral Scler. Mot. Neuron Disord. 2012, 13, 550–554. [Google Scholar] [CrossRef]
- Chiò, A.; Logroscino, G.; Hardiman, O.; Swingler, R.; Mitchell, D.; Beghi, E.; Traynor, B.G.; On Behalf of the Eurals Consortium. Prognostic factors in ALS: A critical review. Amyotroph. Lateral Scler. Mot. Neuron Disord. 2009, 10, 310–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czell, D.; Bauer, M.; Binek, J.; Schoch, O.D.; Weber, M. Outcomes of percutaneous endoscopic gastrostomy tube insertion in respiratory impaired amyotrophic lateral sclerosis patients under noninvasive ventilation. Respir. Care 2013, 58, 838–844. [Google Scholar] [CrossRef]
- Gastrostomy in patients with amyotrophic lateral sclerosis (ProGas): A prospective cohort study. Lancet Neurol. 2015, 14, 702–709. [CrossRef] [Green Version]
- Tsou, A.Y.; Karlawish, J.; McCluskey, L.; Xie, S.X.; Long, J.A. Predictors of emergent feeding tubes and tracheostomies in amyotrophic lateral sclerosis (ALS). Amyotroph. lateral Scler. Mot. Neuron Disord. 2012, 13, 318–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bokuda, K.; Shimizu, T.; Imamura, K.; Kawata, A.; Watabe, K.; Hayashi, M.; Nakayama, Y.; Isozaki, E.; Nakano, I. Predictive factors for prognosis following unsedated percutaneous endoscopic gastrostomy in ALS patients. Muscle Nerve 2016, 54, 277–283. [Google Scholar] [CrossRef]
- Nagashima, K.; Furuta, N.; Makioka, K.; Fujita, Y.; Ikeda, M.; Ikeda, Y. An analysis of prognostic factors after percutaneous endoscopic gastrostomy placement in Japanese patients with amyotrophic lateral sclerosis. J. Neurol. Sci. 2017, 376, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Dorst, J.; Dupuis, L.; Petri, S.; Kollewe, K.; Abdulla, S.; Wolf, J.; Weber, M.; Czell, D.; Burkhardt, C.; Hanisch, F.; et al. Percutaneous endoscopic gastrostomy in amyotrophic lateral sclerosis: A prospective observational study. J. Neurol. 2015, 262, 849–858. [Google Scholar] [CrossRef]
- Sarfaty, M.; Nefussy, B.; Gross, D.; Shapira, Y.; Vaisman, N.; Drory, V.E. Outcome of percutaneous endoscopic gastrostomy insertion in patients with amyotrophic lateral sclerosis in relation to respiratory dysfunction. Amyotroph. Lateral Scler. Front. Degener. 2013, 14, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Huang, R.; Chen, D.; Song, W.; Zeng, Y.; Zhao, B.; Zhou, N.; Shang, H.-F. Causes and places of death of patients with amyotrophic lateral sclerosis in south-west China. Amyotroph. lateral Scler. Mot. Neuron Disord. 2011, 12, 206–209. [Google Scholar] [CrossRef]
- Ramirez Puerta, R.; Yuste Ossorio, E.; Narbona Galdo, S.; Perez Izquierdo, N.; Penas Maldonado, L. Amyotrophyc lateral sclerosis; gastrointestinal complications in home enteral nutrition. Nutr. Hosp. 2013, 28, 2014–2020. [Google Scholar] [CrossRef]
- Zhang, M.; Hubbard, J.; Rudnicki, S.A.; Johansen, C.S.; Dalton, K.; Heiman-Patterson, T.; Forshew, D.A.; Wills, A.-M. Survey of current enteral nutrition practices in treatment of amyotrophic lateral sclerosis. E-SPEN J. 2013, 8, e25–e28. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PEG | No PEG | p-Value | |
|---|---|---|---|
| Gender (M/F) | 52.6%/47.4% | 61.7%/38.3% | 0.4 |
| Age (years) | 62.68 (13.33) | 65.23 (8.29) | 0.27 |
| ALS Onset (Bulbar/Spinal) | 57.1%/42.9% | 41.4%/58.6% | 0.14 |
| % Weight Loss | 10.31 (2.62–18.83) | 6.93 (2.44–16.33) | 0.24 |
| BMI (kg/m2) | 22.98 (21.06–25.44) | 24.88 (22.48–26.05) | 0.13 |
| SGA (A/B/C) | 22.9%/40%/37.1% | 32.8%/50%/17.2% | 0.09 |
| Mean Time of follow-up (months) | 15 (8–23) | 11 (6–19.25) | 0.22 |
| % patients with non-invasive ventilation | 31.4% | 12.1% | 0.02 |
| % patients with dysphagia | 88.6% | 72.4% | 0.09 |
| % type of dysphagia (L,S,M) | 54.3%/2.9%/42.9% | 51.7%/5.2%/13.8% | <0.01 |
| Time Diagnostic to dysphagia (months) | 0 (−5.5–8) | −1.5 (−5.75–0.25) | 0.28 |
| Time first symptoms to Nutrition Unit (months) | 14 (7–36) | 12.5 (8–24.5) | 0.41 |
| PEG < 10 Months | PEG > 10 Months | p-Value | |
|---|---|---|---|
| Gender (M/F) | 50%/50% | 50%/50% | 1.00 |
| Age (years) | 64.25 (13.23) | 61.06 (14.13) | 0.50 |
| ALS Onset (Bulbar/Spinal) | 87.5%/12.5% | 33.3%/66.7% | 0.01 |
| % Weight Loss | 10.31 (5.18–17.96) | 10.53 (4.40–22.51) | 0.80 |
| BMI (kg/m2) | 23.38 (20.33–25.57) | 23.09 (21.18–25.97) | 0.95 |
| SGA (A/B/C) | 18.8%/43.8%/37.5% | 22.2%/38.9%/38.9% | 0.95 |
| Time Diagnostic to dysphagia (months) | −3.5 (5.45) | 10.18 (20.44) | 0.02 |
| SURVIVAL > 12 Months | Odds Ratio | CI 95% | p-Value |
|---|---|---|---|
| PEG (Yes/No) | 6.81 | 2.05–22.68 | <0.01 |
| Age (years) | 1.01 | 0.966–1.06 | 0.65 |
| Type of ALS (Bulbar/Spinal) | 0.47 | 0.16–1.13 | 0.15 |
| Nutritional Status (Malnourished (SGA:B-C)/Well nourished (SGA:A) | 0.47 | 0.16–1.37 | 0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Gómez, J.J.; Ballesteros-Pomar, M.D.; Torres-Torres, B.; Pintor-De la Maza, B.; Penacho-Lázaro, M.A.; Palacio-Mures, J.M.; Abreu-Padín, C.; Sanz-Gallego, I.; De Luis-Román, D.A. Impact of Percutaneous Endoscopic Gastrostomy (PEG) on the Evolution of Disease in Patients with Amyotrophic Lateral Sclerosis (ALS). Nutrients 2021, 13, 2765. https://doi.org/10.3390/nu13082765
López-Gómez JJ, Ballesteros-Pomar MD, Torres-Torres B, Pintor-De la Maza B, Penacho-Lázaro MA, Palacio-Mures JM, Abreu-Padín C, Sanz-Gallego I, De Luis-Román DA. Impact of Percutaneous Endoscopic Gastrostomy (PEG) on the Evolution of Disease in Patients with Amyotrophic Lateral Sclerosis (ALS). Nutrients. 2021; 13(8):2765. https://doi.org/10.3390/nu13082765
Chicago/Turabian StyleLópez-Gómez, Juan J., María D. Ballesteros-Pomar, Beatriz Torres-Torres, Begoña Pintor-De la Maza, María A. Penacho-Lázaro, José M. Palacio-Mures, Cristina Abreu-Padín, Irene Sanz-Gallego, and Daniel A. De Luis-Román. 2021. "Impact of Percutaneous Endoscopic Gastrostomy (PEG) on the Evolution of Disease in Patients with Amyotrophic Lateral Sclerosis (ALS)" Nutrients 13, no. 8: 2765. https://doi.org/10.3390/nu13082765