
The Impact of Carbohydrate Quality on Dental Plaque pH: Does the Glycemic Index of Starchy Foods Matter for Dental Health?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Test Foods
2.3. Dental Sampling and pH Measurement
2.4. Blood Sampling and Plasma Glucose Measurement
2.5. Data Analysis
3. Results
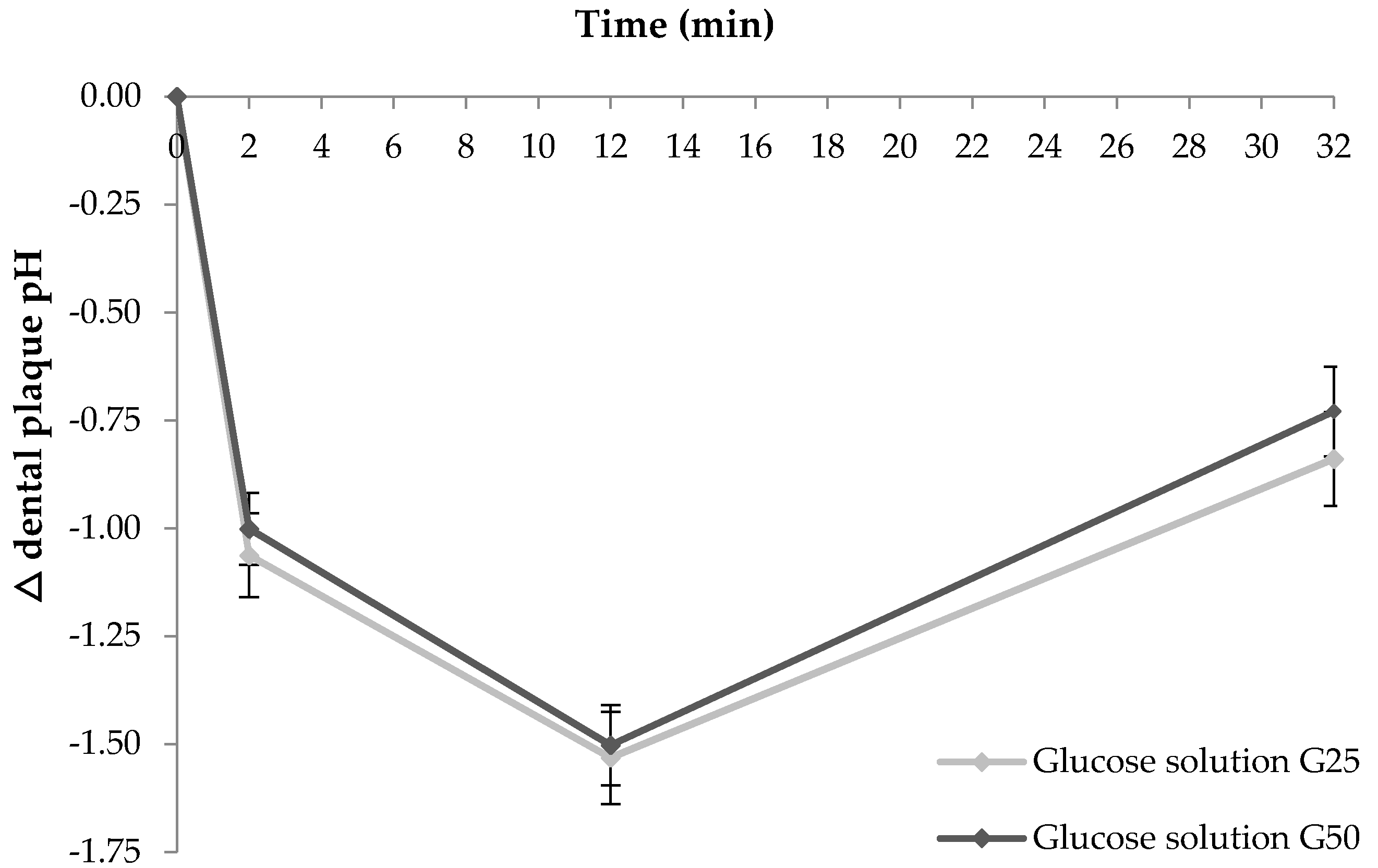
3.1. Study 1: Impact of Carbohydrate Dose on Acute Changes in Dental Plaque pH
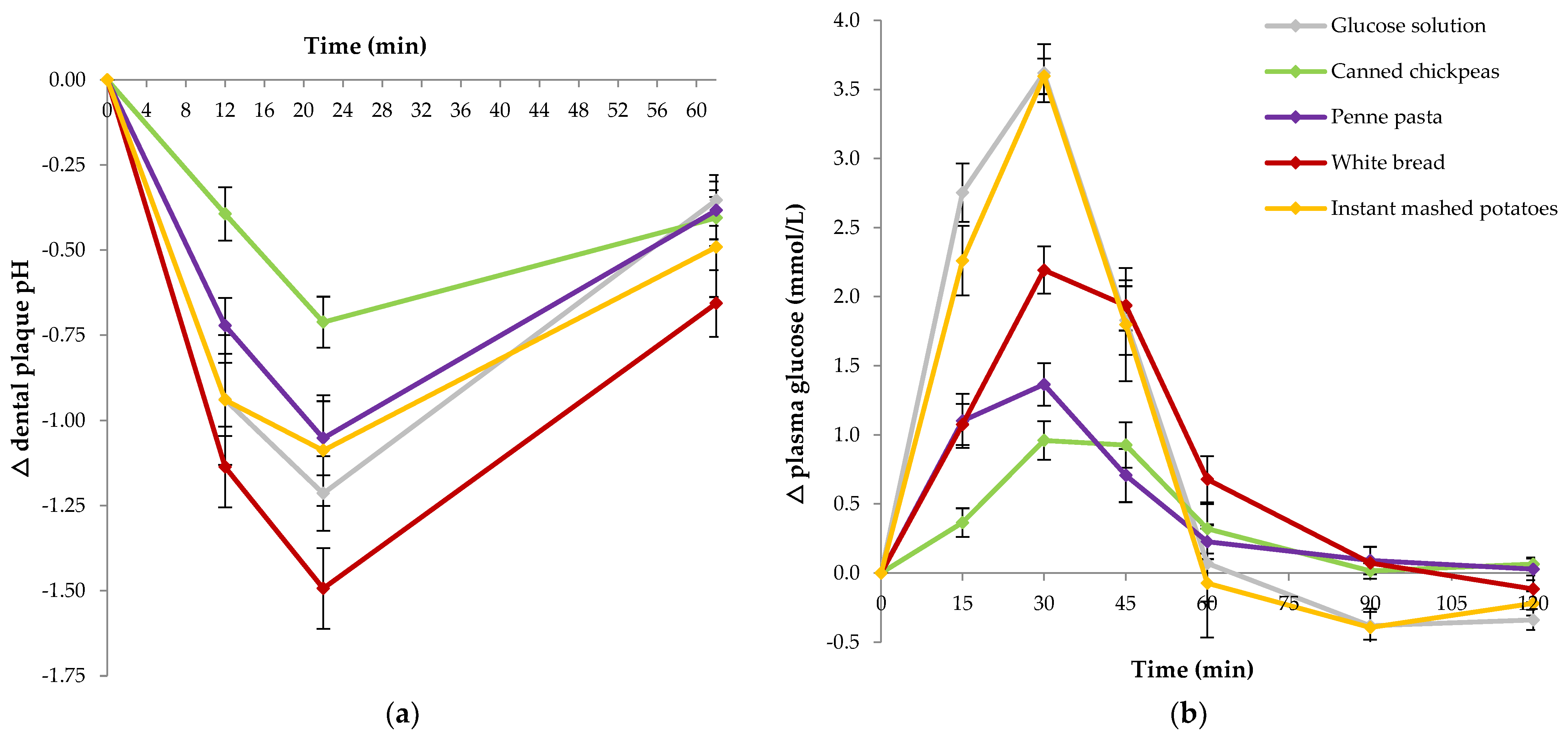
3.2. Study 2: Impact of Carbohydrate Quality (GI) on Acute Changes in Dental Plaque pH
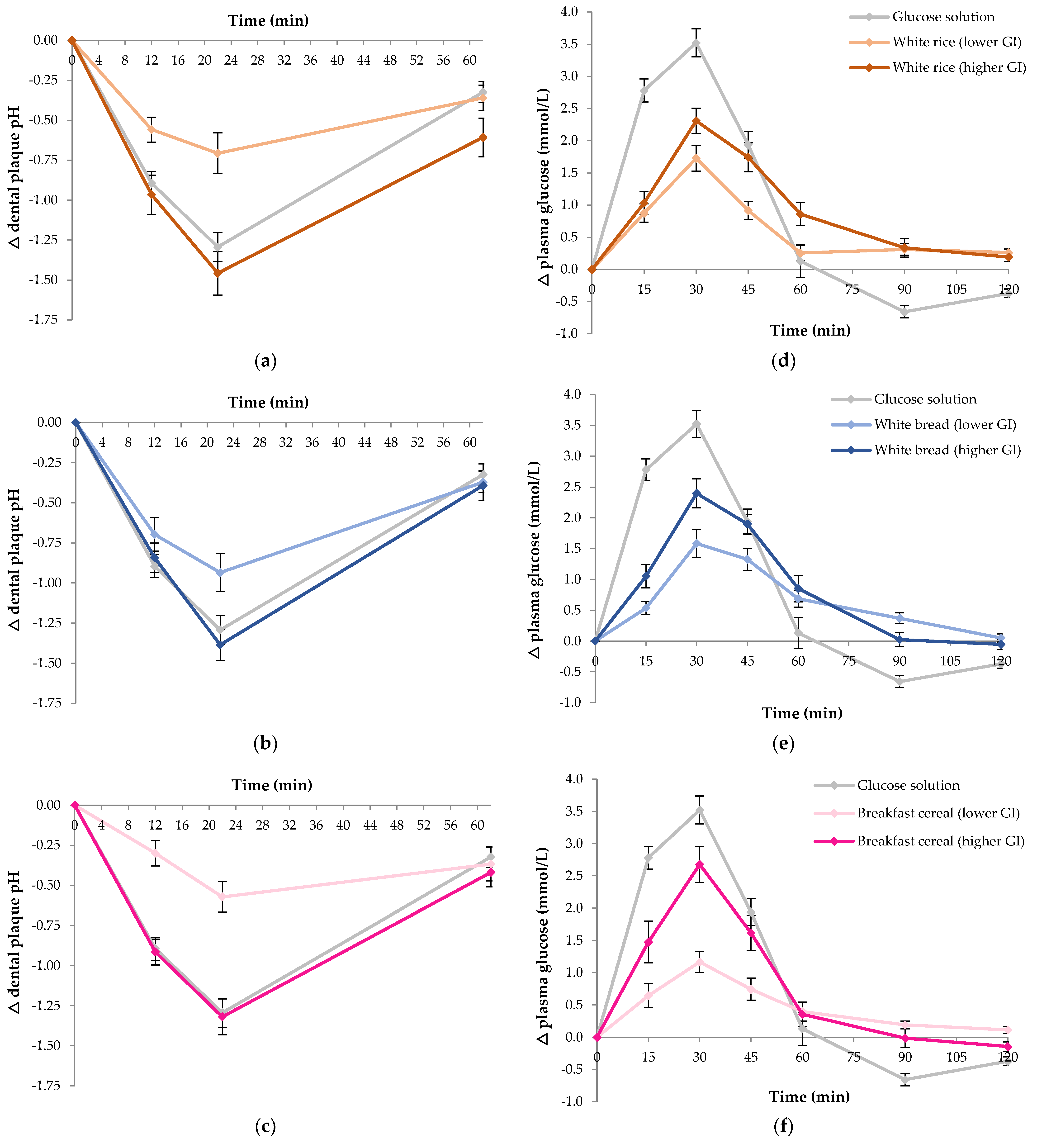
3.3. Study 3: Impact of GI in Paired Foods on Acute Changes in Dental Plaque pH
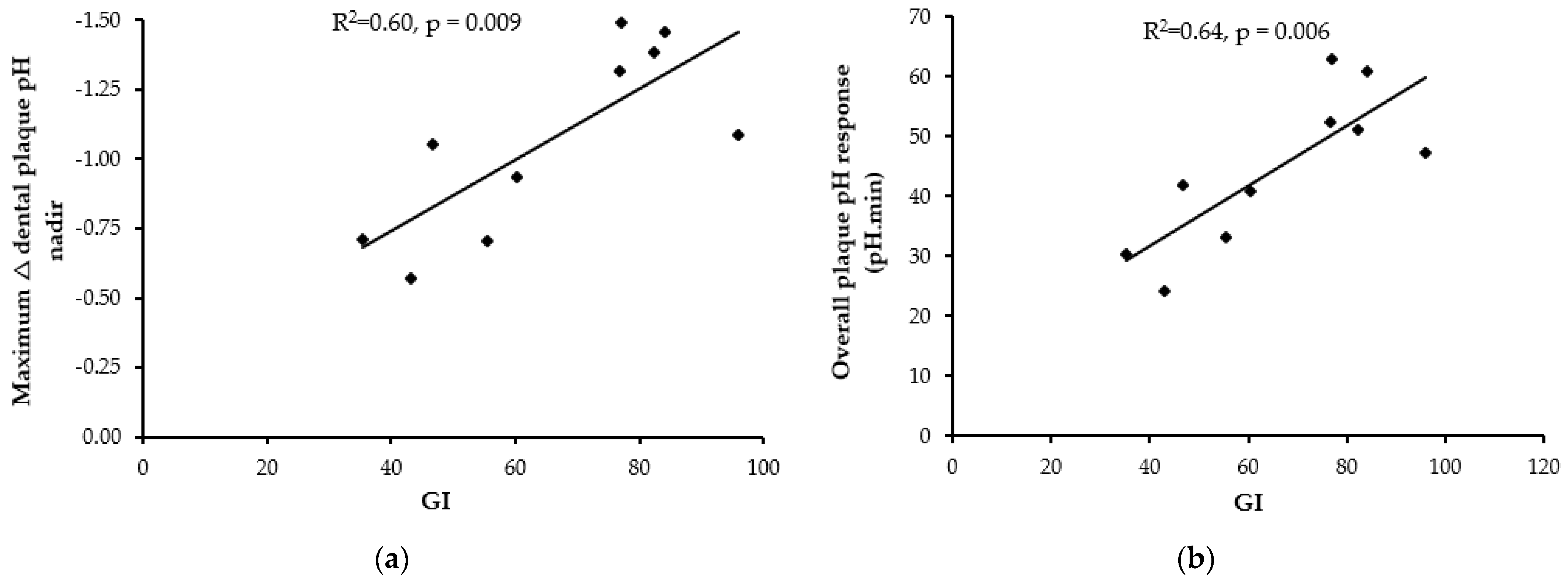
3.4. Association between GI and Change in Dental Plaque pH
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arantes, R.; Welch, J.R.; Tavares, F.G.; Ferreira, A.A.; Vettore, M.V.; Coimbra, C.E.A., Jr. Human ecological and social determinants of dental caries among the Xavante Indigenous people in Central Brazil. PLoS ONE 2018, 13, e0208312. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Sugar and Dental Caries. 2017. Contract No.: WHO/NMH/NHD/17.12; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Shokouhi, E.B.; Razani, M.; Gupta, A.; Tabatabaei, N. Comparative study on the detection of early dental caries using thermo-photonic lock-in imaging and optical coherence tomography. Biomed. Opt. Express 2018, 9, 3983–3997. [Google Scholar] [CrossRef]
- Tinanoff, N.; Baez, R.J.; Diaz Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Pitts, N.B.; Seow, W.K.; Sharkov, N.; et al. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int. J. Paediatr. Dent. 2019, 29, 238–248. [Google Scholar] [CrossRef]
- Larsen, M.J.; Jensen, A.F.; Madsen, D.M.; Pearce, E.I. Individual variations of pH, buffer capacity, and concentrations of calcium and phosphate in unstimulated whole saliva. Arch. Oral Biol. 1999, 44, 111–117. [Google Scholar] [CrossRef]
- Luoma, H.; Turtola, L.O.; Kuokka, I.M.; Kaartinen, A.J. Plaque pH during and after ingestion of solid sugar. J. Dent. Res. 1970, 49, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.H.; Donly, K.J. In vivo dental plaque pH variation with regular and diet soft drinks. Pediatr. Dent. 2002, 24, 350–353. [Google Scholar]
- Toumba, K.J.; Duggal, M.S. Effect on plaque pH of fruit drinks with reduced carbohydrate content. Br. Dent. J. 1999, 186, 626–629. [Google Scholar] [CrossRef]
- Johansson, A.K.; Lingstrom, P.; Birkhed, D. Effect of soft drinks on proximal plaque pH at normal and low salivary secretion rates. Acta Odontol. Scand. 2007, 65, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Birkhed, D. Sugar content, acidity and effect on plaque pH of fruit juices, fruit drinks, carbonated beverages and sport drinks. Caries Res. 1984, 18, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, N.; Kotwal, B.; Sachdev, V.; Rewal, N.; Gupta, R.; Goyal, S. Effect of commonly consumed sugar containing and sugar free fruit drinks on the hydrogen ion modulation of human dental plaque. J. Indian Soc. Pedod. Prev. Dent. 2014, 32, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Garg, D.; Karuna, Y.M.; Srikant, N.; Bhandary, M.; Nayak, A.P.; Rao, A.; Suprabha, B.S. Evaluation of Plaque pH Changes Following Consumption of Health Drinks by Children: A Pilot Study. J. Clin. Diagn. Res. 2017, 11, Zc05–Zc08. [Google Scholar] [CrossRef]
- Utreja, A.; Lingstrom, P.; Evans, C.A.; Salzmann, L.B.; Wu, C.D. The effect of raisin-containing cereals on the pH of dental plaque in young children. Pediatr. Dent. 2009, 31, 498–503. [Google Scholar] [PubMed]
- Thaweboon, S.; Suddhasthira, T.; Thaweboon, B.; Soo-Ampon, S.; Dechkunakorn, S. Plaque pH response to snack foods in children with different levels of mutans streptococci. SE Asian J. Trop. Med. 2007, 38, 598–603. [Google Scholar]
- Igarashi, K.; Lee, I.K.; Schachtele, C.F. Effect of chewing gum containing sodium bicarbonate on human interproximal plaque pH. J. Dent. Res. 1988, 67, 531–535. [Google Scholar] [CrossRef]
- Lingstrom, P.; Liljeberg, H.; Bjorck, I.; Birkhed, D. The relationship between plaque pH and glycemic index of various breads. Caries Res. 2000, 34, 75–81. [Google Scholar] [CrossRef]
- Lingstrom, P.; Imfeld, T.; Birkhed, D. Comparison of three different methods for measurement of plaque-pH in humans after consumption of soft bread and potato chips. J. Dent. Res. 1993, 72, 865–870. [Google Scholar] [CrossRef]
- Mortazavi, S.; Noin, S. Plaque pH Changes Following Consumption of Two Types of Plain and Bulky Bread. Dent. Res. J. 2011, 8, 80–84. [Google Scholar]
- Brudevold, F.; Goulet, D.; Tehrani, A.; Attarzadeh, F.; van Houte, J. Intraoral demineralization and maltose clearance from wheat starch. Caries Res. 1985, 19, 136–144. [Google Scholar] [CrossRef]
- Hoebler, C.; Karinthi, A.; Devaux, M.F.; Guillon, F.; Gallant, D.J.; Bouchet, B.; Melegari, C.; Barry, J.L. Physical and chemical transformations of cereal food during oral digestion in human subjects. Br. J. Nutr. 1999, 80, 429–436. [Google Scholar] [CrossRef]
- Wahlqvist, M.L.; Wilmshurst, E.G.; Murton, C.R.; Richardson, E.N. The effect of chain length on glucose absorption and the related metabolic response. Am. J. Clin. Nutr. 1978, 31, 1998–2001. [Google Scholar] [CrossRef]
- Halvorsrud, K.; Lewney, J.; Craig, D.; Moynihan, P.J. Effects of starch on oral health: Systematic review to inform WHO guideline. J. Dent. Res. 2019, 98, 46–53. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Wolever, T.M.; Taylor, R.H.; Barker, H.; Fielden, H.; Baldwin, J.M.; Bowling, A.C.; Newman, H.C.; Jenkins, A.L.; Goff, D.V. Glycemic index of foods: A physiological basis for carbohydrate exchange. Am. J. Clin. Nutr. 1981, 34, 362–366. [Google Scholar] [CrossRef] [Green Version]
- Brand, J.C.; Nicholson, P.L.; Thorburn, A.W.; Truswell, A.S. Food processing and the glycemic index. Am. J. Clin. Nutr. 1985, 42, 1192–1196. [Google Scholar] [CrossRef]
- International Standards Organisation. ISO/FDIS 26642:2010. Food Products—Determination of the Glycemic Index (GI) and Recommendation for Food Classification; International Standards Organisation: Geneva, Switzerland, 2010. [Google Scholar]
- Ericsson, Y. Clinical Investigations of the Salivary Buffering Action. Acta Odontol. Scand. 1959, 17, 131–165. [Google Scholar] [CrossRef]
- Gardiner, J.A.; Pollard, M.A.; Curzon, M.E. The effect of different concentrations of sugars in two foods (yoghurts and baked beans) on plaque pH. Int. Dent. J. 1997, 47, 115–120. [Google Scholar] [CrossRef]
- Hoebler, C.; Karinthi, A.; Chiron, H.; Champ, M.; Barry, J.L. Bioavailability of starch in bread rich in amylose: Metabolic responses in healthy subjects and starch structure. Eur. J. Clin. Nutr. 1999, 53, 360–366. [Google Scholar] [CrossRef] [Green Version]
- Granfeldt, Y.; Hagander, B.; Bjorck, I. Metabolic responses to starch in oat and wheat products. On the importance of food structure, incomplete gelatinization or presence of viscous dietary fibre. Eur. J. Clin. Nutr. 1995, 49, 189–199. [Google Scholar]
- O’Dea, K.; Nestel, P.J.; Antonoff, L. Physical factors influencing postprandial glucose and insulin responses to starch. Am. J. Clin. Nutr. 1980, 33, 760–765. [Google Scholar] [CrossRef] [Green Version]
- Fardet, A.; Hoebler, C.; Baldwin, P.M.; Bouchet, B.; Gallant, D.J.; Barry, J.L. Involvement of the Protein Network in the in vitro Degradation of Starch from Spaghetti and Lasagne: A Microscopic and Enzymic Study. J. Cereal Sci. 1998, 27, 133–145. [Google Scholar] [CrossRef]
- Lingstrom, P.; Holm, J.; Birkhed, D.; Bjorck, I. Effects of variously processed starch on pH of human dental plaque. Scand. J. Dent. Res. 1989, 97, 392–400. [Google Scholar] [CrossRef]
- Ross, S.W.; Brand, J.C.; Thorburn, A.W.; Truswell, A.S. Glycemic index of processed wheat products. Am. J. Clin. Nutr. 1987, 46, 631–635. [Google Scholar] [CrossRef]
- Loke, C.; Lee, J.; Sander, S.; Mei, L.; Farella, M. Factors affecting intra-oral pH—A review. J. Oral Rehabil. 2016, 43, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. Interntaional tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [Green Version]
- Hussein, I.; Pollard, M.A.; Curzon, M.E.J. A comparsion of the effects of some extrinsic and intrinsic sugars on dental plaque pH. Int. J. Paediatr. Dent. 1996, 6, 81–86. [Google Scholar] [CrossRef]
- Pettersson, S.; Ahnoff, M.; Edin, F.; Lingstrom, P.; Simark Mattsson, C.; Andersson-Hall, U. A hydrogel drink with high frutcose content generates higher exogenous carbohydrate oxidation and a reduced drop in dental biolfilm pH compared to two other, commercially available, carbohydrate sports drinks. Front. Nutr. 2020, 7, 88. [Google Scholar] [CrossRef] [PubMed]
- Islas-Granillo, H.; Borges-Yañez, S.A.; Medina-Solís, C.E.; Galan-Vidal, C.A.; Navarrete-Hernández, J.J.; Escoffié-Ramirez, M.; Maupomé, G. Salivary Parameters (Salivary Flow, pH and Buffering Capacity) in Stimulated Saliva of Mexican Elders 60 Years Old and Older. West. Indian Med. J. 2014, 63, 758–765. [Google Scholar] [PubMed] [Green Version]
- Hicks, J.; Garcia-Godoy, F.; Flaitz, C. Biological factors in dental caries: Role of saliva and dental plaque in the dynamic process of demineralization and remineralization (part 1). J. Clin. Pediatr. Dent. 2003, 28, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Kitasako, Y.; Ikeda, M.; Burrow, M.F.; Tagami, J. Oral health status in relation to stimulated saliva buffering capacity among Japanese adults above or below 35 years of age. J. Med. Dent. Sci. 2006, 53, 175–180. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Food | Weight (g) | Energy (kJ) | Protein (g) | Fat (g) | Available Carbohydrate (g) | Starch (g) | Sugar (g) | Fiber (g) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Glucose solution G25 | 25.7 | 436 | 0 | 0 | 25 | 0 | 25 | 0 |
| Glucose solution G50 | 51.4 | 873 | 0 | 0 | 50 | 0 | 50 | 0 | |
| 2 | Canned chickpeas | 131.5 | 751 | 9.4 | 2.7 | 25 | 24.4 | 0.6 | 7.8 |
| Penne pasta | 34.7 1 | 531 | 4.1 | 0.6 | 25 | 24.2 | 0.8 | 1.0 | |
| White bread | 58.5 | 585 | 4.3 | 1.8 | 25 | 23.0 | 2.0 | 4.1 | |
| Instant mashed potatoes | 37.1 1 | 602 | 3.3 | 2.7 | 25 | 23.3 | 1.7 | - | |
| 3 2 | White rice (lower GI) | 69.5 | 553 | 2.6 | 1.8 | 25 | 24.7 | 0.3 | 1.7 |
| White rice (higher GI) | 73.5 | 574 | 3.2 | 2.2 | 25 | 24.7 | 0.3 | 0.9 | |
| White bread (lower GI) | 60.5 | 604 | 4.9 | 1.3 | 25 | 23.4 | 1.6 | 5.6 | |
| White bread (higher GI) | 61.8 | 599 | 4.6 | 1.5 | 25 | 23.2 | 1.8 | 5.1 | |
| Breakfast cereal (lower GI) | 38.2 | 581 | 3.7 | 1.0 | 25 | 20.2 | 4.8 | 7.0 | |
| Breakfast cereal (higher GI) | 32.8 | 528 | 2.2 | 1.2 | 25 | 20.3 | 4.7 | 2.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atkinson, F.S.; Khan, J.H.; Brand-Miller, J.C.; Eberhard, J. The Impact of Carbohydrate Quality on Dental Plaque pH: Does the Glycemic Index of Starchy Foods Matter for Dental Health? Nutrients 2021, 13, 2711. https://doi.org/10.3390/nu13082711
Atkinson FS, Khan JH, Brand-Miller JC, Eberhard J. The Impact of Carbohydrate Quality on Dental Plaque pH: Does the Glycemic Index of Starchy Foods Matter for Dental Health? Nutrients. 2021; 13(8):2711. https://doi.org/10.3390/nu13082711
Chicago/Turabian StyleAtkinson, Fiona S., Jouhrah Hussain Khan, Jennie C. Brand-Miller, and Joerg Eberhard. 2021. "The Impact of Carbohydrate Quality on Dental Plaque pH: Does the Glycemic Index of Starchy Foods Matter for Dental Health?" Nutrients 13, no. 8: 2711. https://doi.org/10.3390/nu13082711