
Socioeconomic Status Impact on Diet Quality and Body Mass Index in Eight Latin American Countries: ELANS Study Results

 , , , ,
, , , ,  , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. ELANS Overview
2.2. Study Sample
2.3. Sociodemographic Characteristics
2.4. Dietary Assessment
2.5. Diet Quality
2.6. Dietary Diversity
2.7. Nutrient Adequacy
2.8. Weight Status
2.9. Data Analysis
3. Results
3.1. Distribution of Sociodemographic Variables among the Socioeconomic Levels
3.2. Consumption of Food Groups among the Socioeconomic Levels
3.3. Micronutrient Adequacy Ratio (NAR) among the Socioeconomic Statuses
3.4. Diet Quality Indicators among the Socioeconomic Levels
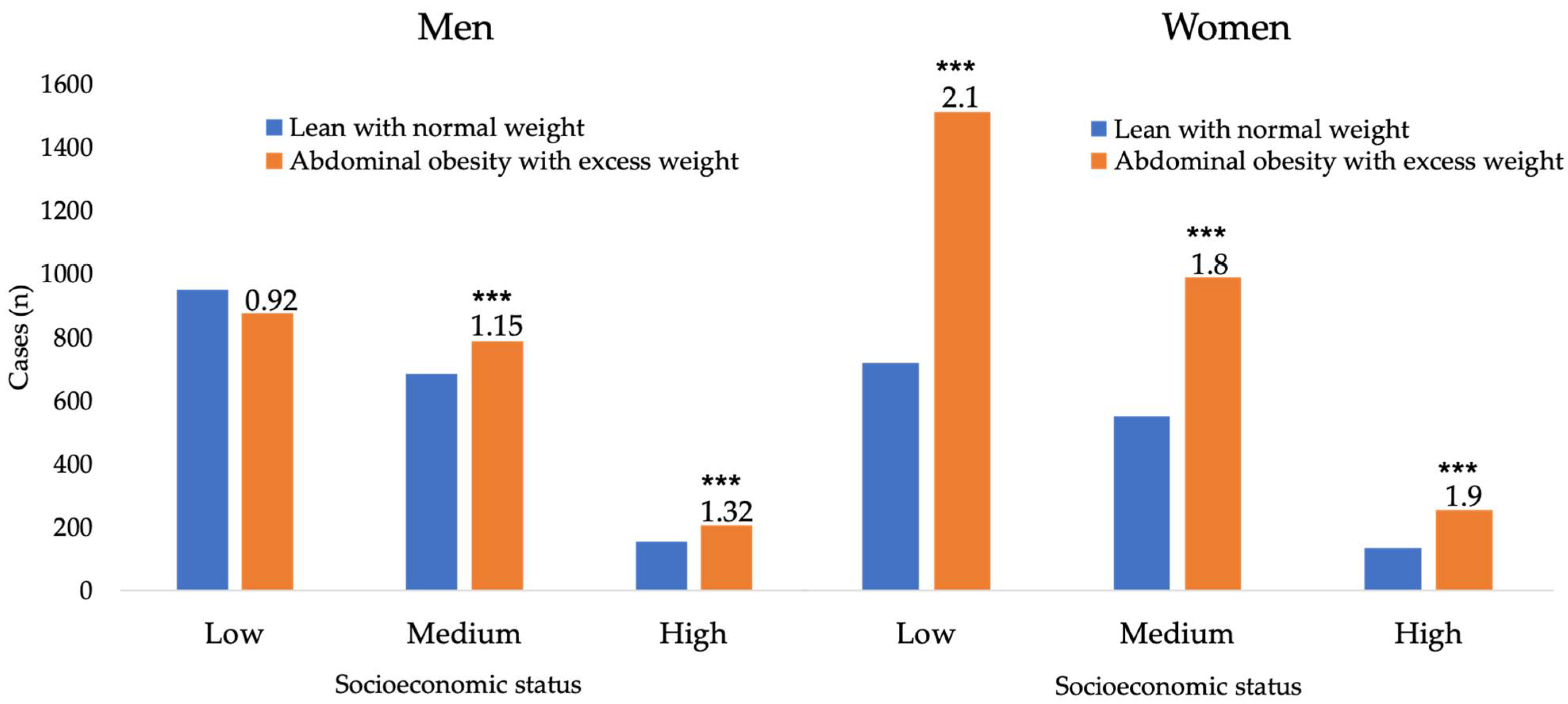
3.5. BMI among the Socioeconomic Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pérez-Ferrer, C.; Auchincloss, A.H.; de Menezes, M.C.; Kroker-Lobos, M.F.; Cardoso, L.D.O.; Barrientos-Gutierrez, T. The food environment in Latin America: A systematic review with a focus on environments relevant to obesity and related chronic diseases. Public Health Nutr. 2019, 22, 3447–3464. [Google Scholar] [CrossRef]
- Popkin, B.M.; Reardon, T. Obesity and the food system transformation in Latin America HHS Public Access. Obes Rev. 2018, 19, 1028–1064. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Kovalskys, I.; Fisberg, M.; Gómez, G.; Pareja, R.G.; García, M.C.; Sanabria, L.Y.; Herrera-Cuenca, M.; Rigotti, A.; Guajardo, V.; Zimberg, I.Z.; et al. Energy intake and food sources of eight Latin American countries: Results from the Latin American Study of Nutrition and Health (ELANS). Public Health Nutr. 2018, 21, 2535–2547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sisa, I.; Abeyá-Gilardon, E.; Fisberg, R.M.; Jackson, M.D.; Mangialavori, G.L.; Sichieri, R.; Cudhea, F.; Bannuru, R.R.; Ruthazer, R.; Mozaffarian, D.; et al. Impact of diet on CVD and diabetes mortality in Latin America and the Caribbean: A comparative risk assessment analysis. Public Health Nutr. 2021, 24, 2577–2591. [Google Scholar] [CrossRef]
- Leme, A.C.B.; Ferrari, G.; Fisberg, R.M.; Kovalskys, I.; Gómez, G.; Cortes, L.Y.; Yépez Gárcia, M.C.; Herrera-Cuenca, M.; Rigotti, A.; Liria-Domínguez, M.R.; et al. Co-Occurrence and Clustering of Sedentary Behaviors, Diet, Sugar-Sweetened Beverages, and Alcohol Intake among Adolescents and Adults: The Latin American Nutrition and Health Study (ELANS). Nutrients 2021, 13, 1809. [Google Scholar] [CrossRef]
- Kivimäki, M.; Batty, G.D.; Pentti, J.; Shipley, M.J.; Sipilä, P.N.; Nyberg, S.T.; Suominen, S.B.; Oksanen, T.; Stenholm, S.; Virtanen, M.; et al. Association between socioeconomic status and the development of mental and physical health conditions in adulthood: A multi-cohort study. Lancet Public Health 2020, 5, e140–e149. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Duan, M.J.; Riphagen, I.J.; Minovic, I.; Mierau, J.O.; Carrero, J.J.; Bakker, S.J.; Navis, G.J.; Dekker, L.H. Separate and combined effects of individual and neighbourhood socio-economic disadvantage on health-related lifestyle risk factors: A multilevel analysis. Int. J. Epidemiol. 2021, 1–11. [Google Scholar] [CrossRef]
- Cherta-Murillo, A.; Frost, G.S. The association of mycoprotein-based foods consumption with diet quality, energy intake and non-communicable diseases’ risk in the UK adult population using the National Diet and Nutrition Survey (NDNS) years 2008/09-2016/17: A cross-sectional study. Br. J. Nutr. 2021, 1–26. [Google Scholar] [CrossRef]
- Williams, J.; Townsend, N.; Rayner, M.; Jayawardena, R.; Katulanda, P.; Manoharan, S.; Wickramasinghe, K. Diet quality of adolescents in rural Sri Lanka based on the Diet Quality Index-International: Findings from the ‘Integrating Nutrition Promotion and Rural Development’ project. Public Health Nutr. 2019, 22, 1735–1744. [Google Scholar] [CrossRef]
- Leme, A.C.; Muszynski, D.; Mirotta, J.A.; Carrol, N.; Hogan, J.; Jewell, K.; Yu, J.; Fisberg, R.; Duncan, A.; Ma, D. Diet Quality of Canadian Preschool Children: Associations with Socio-demographic Characteristics. Can. J. Diet. Pract. Res. 2021, 1–5. [Google Scholar] [CrossRef]
- Gupta, S.; Rose, C.M.; Buszkiewicz, J.; Ko, L.K.; Mou, J.; Cook, A.; Aggarwal, A.; Drewnowski, A. Characterizing Percent Energy from Ultra-Processed Foods by Participant Demographics, Diet Quality, and Diet Cost Findings from the Seattle Obesity Study SOS III. Br. J. Nutr. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Brettschneider, A.K.; Barbosa, C.L.; Haftenberger, M.; Lehmann, F.; Mensink, G.B.M. Adherence to food-based dietary guidelines among adolescents in Germany according to socio-economic status and region: Results from Eating Study as a KiGGS Module (EsKiMo) II. Public Health Nutr. 2021, 24, 1216–1228. [Google Scholar] [CrossRef] [PubMed]
- Fisberg, M.; Kovalskys, I.; Gomez, G.; Rigotti, A.; Cortés, L.Y.; Herrera-Cuenca, M.; Yepez, M.C.; Pareja, R.G.; Guajardo, V.; Zimberg, I.Z.; et al. Latin American Study of Nutrition and Health (ELANS): Rationale and study design. BMC Public Health 2016, 16, 93. [Google Scholar] [CrossRef] [PubMed]
- Kovalskys, I.; Fisberg, M.; Gómez, G.; Rigotti, A.; Cortés, L.Y.; Yépez, M.C.; Pareja, R.G.; Herrera-Cuenca, M.; Zimberg, I.Z.; Tucker, K.L.; et al. Standardization of the food composition database used in the latin american nutrition and health study (Elans). Nutrients 2015, 7, 7914–7924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Adolescents Heatlh; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Comisión de Enlace Institucional AAM-SAIMO-CEIM. Nivel Socioeconómico. Antecedentes, Marco Conceptual, Enfoque Metodológico y Fortalezas; Comisión de Enlace Institucional AAM-SAIMO-CEIM: Buenos Aires, Argentina, 2006. [Google Scholar]
- Associação Brasileira de Empresas de Pesquisas. Critério Padrão de Classificação Econômica Brasil 2008. Available online: http://www.slideshare.net/rypax/novos-criterios-2008-classificacao-socieconomica/ (accessed on 20 March 2009).
- Departamento Administrativo Nacional de Estadisticas. Proyecciones Nacionales y Departamentales de Poblacion 2005–2020; UNFPA: Bogotá, Colombia, 2009. [Google Scholar]
- Asociación Investigadores de Mercadeo. Grupos Socioeconómicos Chile, 2012; Asociación Investigadores de Mercadeo: Santiago, Chile, 2012. [Google Scholar]
- Madrigal Pana, J. Estratificación de hogares y segmentos por niveles de ingreso en el censo 2000. Available online: http://www.kerwa.ucr.ac.cr/handle/10669/81093 (accessed on 12 July 2021).
- Instituto Nacional de Estadistica y Censos de Ecuador. Encuesta de Estratificación del Nivel Socioeconomico 2011; INEC: Loja, Ecuador, 2011; p. 37. [Google Scholar]
- Vera-Romero, O.E.; Vera-Romero, F.M. Evaluación del nivel socioeconómico: Presentación de una escala adaptada en una población de Lambayeque. Rev. Cuerpo Med. HNAAA 2015, 6, 41–45. [Google Scholar]
- Instituto Nacional de Estadística, República Bolivariana de Venezuela. Síntesis Estadística de Pobreza e Indicadores de Desigualdad, 2011; Instituto Nacional de Estadística, República Bolivariana de Venezuela: Caracas, Venezuela, 2011.
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Harttig, U.; Haubrock, J.; Knüppel, S.; Boeing, H. The MSM program: Web-based statistics package for estimating usual intake using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65, S87–S91. [Google Scholar] [CrossRef] [Green Version]
- Dalwood, P.; Marshall, S.; Burrows, T.L.; McIntosh, A.; Collins, C.E. Diet quality indices and their associations with health-related outcomes in children and adolescents: An. updated systematic review. Nutr. J. 2020, 19, 1–43. [Google Scholar] [CrossRef]
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D.; Global Burden of Diseases Nutrition and Chronic Diseases Expert Group. Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, e132–e142. [Google Scholar] [CrossRef] [Green Version]
- Gómez, G.; Fisberg, R.M.; Nogueira Previdelli, Á.; Hermes Sales, C.; Kovalskys, I.; Fisberg, M.; Herrera-Cuenca, M.; Cortés Sanabria, L.Y.; García, M.C.; Pareja Torres, R.G.; et al. Diet Quality and Diet Diversity in Eight Latin American Countries: Results from the Latin American Study of Nutrition and Health (ELANS). Nutrients 2019, 11, 1605. [Google Scholar] [CrossRef] [Green Version]
- FAO. Minimum Dietary Diversity for Women—A Guide to Measurement; FAO: Rome, Italy, 2016. [Google Scholar]
- Dwyer, J. Dietary Requirements of Adults. In Estimated Average Requirement; Elsevier Science B.V.: Amsterdam, The Netherlands, 2003. [Google Scholar]
- Committee to Review the Dietary Reference Inake for Sodium and Potassium. Dietary Reference Intakes for Sodium and Potassium; National Academies Press (US): Washington, DC, USA, 2019. [Google Scholar]
- Guthrie, H.; Scheer, J. Validity of dietary score for assesing nutrient adequacy. J. Am. Diet. Assoc. 1981, 78, 240–245. [Google Scholar] [PubMed]
- Gómez, G.; Nogueira Previdelli, Á.; Fisberg, R.M.; Kovalskys, I.; Fisberg, M.; Herrera-Cuenca, M.; Cortés Sanabria, L.Y.; Yépez García, M.C.; Rigotti, A.; Liria-Domínguez, M.R.; et al. Dietary diversity and micronutrients adequacy in women of childbearing age: Results from elans study. Nutrients 2020, 12, 1994. [Google Scholar] [CrossRef]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2017, 85, 660–667. [Google Scholar] [CrossRef]
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Fisberg, M.; Kovalskys, I.; Gómez, G.; Rigotti, A.; Sanabria, L.Y.; García, M.C.; Torres, R.G.; Herrera-Cuenca, M.; Zimberg, I.Z.; Koletzko, B.; et al. Total and added sugar intake: Assessment in eight Latin American countries. Nutrients 2018, 10, 389. [Google Scholar] [CrossRef] [Green Version]
- Drewnowski, A.; Darmon, N. The economics of obesity: Dietary energy density and energy cost. Am. J. Clin. Nutr. 2005, 82, 265S–273S. [Google Scholar] [CrossRef] [PubMed]
- de Mello, A.V.; Sarti, F.M.; Pereira, J.L.; Goldbaum, M.; Cesar, C.L.; Alves, M.C.; Fisberg, R.M. Determinants of inequalities in the quality of Brazilian diet: Trends in 12-year population-based study (2003–2015). Int. J. Equity Health 2018, 17, 1–11. [Google Scholar] [CrossRef]
- Lopez-Olmedo, N.; Popkin, B.M.; Taillie, L.S. Association between socioeconomic status and diet quality in Mexican men and women: A cross-sectional study. PLoS ONE 2019, 14, 1–16. [Google Scholar]
- Cembranel, F.; Jokavljevic, P.; González-Chica, D.; D’Orsi, E. Educational and income levels are associated with energy and micronutrient intake. Int. J. Vitam. Nutr. Res. 2019. [Google Scholar] [CrossRef]
- Viñas, B.R.; Barba, L.R.; Ngo, J.; Gurinovic, M.; Novakovic, R.; Cavelaars, A.; De Groot, L.C.; van’t Veer, P.; Matthys, C.; Majem, L.S. Projected prevalence of inadequate nutrient intakes in Europe. Ann. Nutr. Metab. 2011, 59, 84–95. [Google Scholar] [CrossRef]
- Cano-Ibáñez, N.; Gea, A.; Ruiz-Canela, M.; Corella, D.; Salas-Salvadó, J.; Schröder, H.; Navarrete-Muñoz, E.M.; Romaguera, D.; Martínez, J.A.; Barón-López, F.J.; et al. Diet quality and nutrient density in subjects with metabolic syndrome: Influence of socioeconomic status and lifestyle factors. A cross-sectional assessment in the PREDIMED-Plus study. Clin. Nutr. 2020, 39, 1161–1173. [Google Scholar] [CrossRef]
- Knez, M.; Nikolic, M.; Zekovic, M.; Stangoulis, J.C.; Gurinovic, M.; Glibetic, M. The influence of food consumption and socio-economic factors on the relationship between zinc and iron intake and status in a healthy population. Public Health Nutr. 2017, 20, 2486–2498. [Google Scholar] [CrossRef] [Green Version]
- Leme, A.C.B.; Fisberg, R.M.; Veroneze de Mello, A.; Sales, C.H.; Ferrari, G.; Haines, J.; Rigotti, A.; Gómez, G.; Kovalskys, I.; Cortés Sanabria, L.Y.; et al. Food sources of shortfall nutrients among latin americans: Results from the latin american study of health and nutrition (elans). Int. J. Environ. Res. Public Health 2021, 18, 4967. [Google Scholar] [CrossRef] [PubMed]
- Lortet-Tielent, J.; Georges, D.; Bray, F.; Vaccarella, S. Profiling global cancer incidence and mortality by socioeconomic develepment. Cancer Epidemiol. 2020, 147, 3029–3036. [Google Scholar]
- López-Casasnovas, G.; Soley-Bori, M. The socioeconomic determinants of health: Economic growth and health in the OECD countries during the last three decades. Int. J. Environ. Res. Public Health 2014, 11, 815–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.-Y.; Huang, C.-L.; Lei, W.-S.; Yang, S.-H. Alternative health eating index and the Dietary Guidelines from American Diabetes Association both may reduce the risk of cardiovascular disease in type 2 diabetes patients. J. Hum. Nutr. Diet. 2016, 29, 363–373. [Google Scholar] [CrossRef]
- GBD. Global, Regional, and National Age-Sex-Specific Mortality for 282 Causes of Death in 195 Countries and Territories, 1980–2017: A Systematic Analysis for the Global Burden of Disease Study 2017; Elsevier: Amsterdam, The Netherlands, 2018; Volume 392, pp. 1736–1788. [Google Scholar]
- Gil, Á.; de Victoria, E.M.; Olza, J. Indicadores de evaluación de la calidad de la dieta. Nutr. Hosp. 2015, 31, 128–144. [Google Scholar] [PubMed]
- Hiza, H.A.B.; Casavale, K.O.; Guenther, P.M.; Davis, C.A. Diet Quality of Americans Differs by Age, Sex, Race/Ethnicity, Income, and Education Level. J. Acad. Nutr. Diet. 2013, 113, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Kurotani, K.; Ishikawa-Takata, K.; Takimoto, H. Diet quality of Japanese adults with respect to age, sex, and income level in the National Health and Nutrition Survey, Japan. Public Health Nutr. 2020, 23, 821–832. [Google Scholar] [CrossRef] [Green Version]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Mello, A.V.; Pereira, J.L.; Leme, A.C.B.; Goldbaum, M.; Cesar, C.L.G.; Fisberg, R.M. Social determinants, lifestyle and diet quality: A population-based study from the 2015 Health Survey of São Paulo, Brazil. Public Health Nutr. 2020, 23, 1766–1777. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.; Yusuf, S.; Chow, C.K.; Dehghan, M.; Corsi, D.J.; Lock, K.; Popkin, B.; Rangarajan, S.; Khatib, R.; Lear, S.A.; et al. Availability, affordability, and consumption of fruits and vegetables in 18 countries across income levels: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet Glob. Health 2016, 4, e695–e703. [Google Scholar] [CrossRef] [Green Version]
- Morseth, M.S.; Grewal, N.K.; Kaasa, I.S.; Hatloy, A.; Barikmo, I.; Henjum, S. Dietary diversity is related to socioeconomic status among adult Saharawi refugees living in Algeria. BMC Public Health 2017, 17, 621. [Google Scholar] [CrossRef] [Green Version]
- Mayén, A.L.; Marques-Vidal, P.; Paccaud, F.; Bovet, P.; Stringhini, S. Socioeconomic determinants of dietary patterns in low- and middle-income countries: A systematic review. Am. J. Clin. Nutr. 2014, 100, 1520–1531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obayelu, O.A.; Osho, F.R. How diverse are the diets of low-income urban households in Nigeria? J. Agric. Food Res. 2020, 2, 100018. [Google Scholar] [CrossRef]
- Wolongevicz, D.M.; Zhu, L.; Pencina, M.J.; Kimokoti, R.W.; Newby, P.K.; D’Agostino, R.B.; Millen, B.E. Diet quality and obesity in women: The Framingham Nutrition Studies. Br. J. Nutr. 2010, 103, 1223–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Assumpção, D.; Senicato, C.; Fisberg, R.M.; Canesqui, A.M.; Barros, M.B.d. Are there differences in the quality of the diet of working and stay-at-home women? Rev. Saude Publica 2018, 52, 1–11. [Google Scholar]


{kind=link}
| Socioeconomic Levels | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 9218) | Low (n = 4796) | Middle (n = 3542) | High (n = 880) | ||||||
| n | % | n | % | n | % | n | % | p Value | |
| Country | <0.001 | ||||||||
| Brazil | 2000 | 21.7 | 916 | 19.1 | 915 | 25.8 | 169 | 25.8 | |
| Venezuela | 1132 | 12.3 | 880 | 18.3 | 190 | 5.4 | 62 | 5.4 | |
| Colombia | 1230 | 13.3 | 779 | 16.2 | 384 | 10.8 | 67 | 10.8 | |
| Argentina | 1266 | 13.7 | 616 | 12.8 | 585 | 16.5 | 65 | 16.5 | |
| Peru | 1113 | 12.1 | 533 | 11.1 | 355 | 10 | 225 | 10 | |
| Chile | 879 | 9.5 | 411 | 8.6 | 388 | 11 | 80 | 11 | |
| Ecuador | 800 | 8.7 | 399 | 8.3 | 297 | 8.4 | 104 | 8.4 | |
| Costa Rica | 798 | 8.7 | 262 | 5.5 | 428 | 12.1 | 108 | 12.1 | |
| Sex | 0.010 | ||||||||
| Male | 4409 | 47.8 | 2221 | 46.3 | 1752 | 49.5 | 436 | 49.5 | |
| Female | 4809 | 52.2 | 2575 | 53.7 | 1709 | 50.5 | 444 | 50.5 | |
| Age range (years) | 0.441 | ||||||||
| 15–19 | 1223 | 13.3 | 642 | 13.4 | 468 | 13.2 | 113 | 12.8 | |
| 20–34 | 3479 | 37.7 | 1803 | 37.6 | 1349 | 38.1 | 327 | 37.2 | |
| 35–49 | 2627 | 28.5 | 1332 | 27.8 | 1025 | 28.9 | 270 | 30.7 | |
| 50–65 | 1889 | 20.5 | 1019 | 21.2 | 700 | 19.8 | 170 | 19.3 | |
| Socioeconomic Status | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total (n = 9218) | Low (n = 4796) | Middle (n = 3542) | High (n = 880) | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | p Value | η2p | |
| Vegetables (g) | 105.6 | 54.1 | 100.3 | 51.4 | 109.4 | 56.2 | 119.8 | 56.2 | 0.0001 | 0.018 |
| Fruits (g) | 74.6 | 74.4 | 66.7 | 72.0 | 80.6 | 75.3 | 94.0 | 78.3 | 0.0001 | 0.013 |
| Whole grains (g) | 8.8 | 16.1 | 7.9 | 14.2 | 9.3 | 17.0 | 12.1 | 21.0 | 0.0001 | 0.007 |
| Fiber (g) | 15.8 | 5.8 | 15.6 | 5.8 | 15.6 | 5.9 | 16.9 | 5.7 | 0.0001 | 0.006 |
| Legumes (g) | 37.4 | 38.3 | 36.4 | 36.8 | 39.0 | 40.9 | 35.6 | 35.0 | 0.0001 | 0.004 |
| Dairy (g) | 94.2 | 94.6 | 89.3 | 90.2 | 100.0 | 99.7 | 97.6 | 95.6 | 0.0001 | 0.003 |
| Red meat (g) | 64.5 | 35.7 | 64.9 | 35.0 | 65.3 | 36.5 | 59.0 | 36.2 | 0.0001 | 0.003 |
| Fish and seafood (g) | 18.4 | 20.8 | 18.2 | 21.4 | 17.9 | 20.0 | 21.3 | 20.4 | 0.0001 | 0.002 |
| SSB (g) | 678.3 | 473.7 | 678.2 | 476.6 | 674.9 | 480.8 | 692.4 | 426.7 | 0.002 | 0.001 |
| Processed meat (g) | 19.5 | 16.4 | 19.1 | 16.3 | 20.3 | 16.5 | 17.7 | 16.0 | 0.005 | 0.001 |
| Nuts and seeds (g) | 2.1 | 9.0 | 1.9 | 9.8 | 2.1 | 8.6 | 2.5 | 5.7 | 0.049 | 0.001 |
| Energy (Kcal) | 1993.1 | 621.0 | 1987.7 | 631.6 | 1992.4 | 609.3 | 2025.3 | 608.6 | 0.255 | 0.000 |
| Socioeconomic Status | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total (n = 9218) | Low (n = 4796) | Middle (n = 3542) | High (n = 880) | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | p Value | η2p | |
| Vitamin C | 0.855 | 0.228 | 0.840 | 0.232 | 0.860 | 0.231 | 0.913 | 0.174 | 0.0001 | 0.010 |
| Vitamin A | 0.848 | 0.206 | 0.831 | 0.214 | 0.859 | 0.202 | 0.892 | 0.168 | 0.0001 | 0.009 |
| Vitamin D | 0.355 | 0.209 | 0.343 | 0.205 | 0.361 | 0.209 | 0.400 | 0.229 | 0.0001 | 0.007 |
| Calcium | 0.698 | 0.459 | 0.677 | 0.465 | 0.715 | 0.455 | 0.742 | 0.435 | 0.0001 | 0.003 |
| Magnesium | 0.764 | 0.184 | 0.759 | 0.185 | 0.765 | 0.183 | 0.792 | 0.176 | 0.0001 | 0.003 |
| Copper | 0.987 | 0.057 | 0.986 | 0.061 | 0.988 | 0.052 | 0.992 | 0.049 | 0.0001 | 0.001 |
| Pyridoxin | 0.972 | 0.087 | 0.970 | 0.087 | 0.972 | 0.087 | 0.980 | 0.073 | 0.0003 | 0.001 |
| Iron | 0.989 | 0.056 | 0.987 | 0.059 | 0.990 | 0.055 | 0.993 | 0.040 | 0.0005 | 0.001 |
| Riboflavin | 0.989 | 0.054 | 0.988 | 0.059 | 0.991 | 0.048 | 0.992 | 0.051 | 0.018 | 0.001 |
| Thiamin | 0.991 | 0.049 | 0.990 | 0.053 | 0.993 | 0.044 | 0.991 | 0.051 | 0.020 | 0.001 |
| Cobalamin | 0.985 | 0.076 | 0.983 | 0.081 | 0.987 | 0.071 | 0.988 | 0.067 | 0.041 | 0.001 |
| Vitamin E | 0.033 | 0.018 | 0.032 | 0.018 | 0.033 | 0.018 | 0.034 | 0.018 | 0.099 | 0.000 |
| Selenium | 0.999 | 0.021 | 0.999 | 0.024 | 1.000 | 0.010 | 0.999 | 0.034 | 0.214 | 0.000 |
| Phosphorous | 0.985 | 0.066 | 0.984 | 0.067 | 0.985 | 0.066 | 0.988 | 0.061 | 0.311 | 0.000 |
| Zinc | 0.965 | 0.091 | 0.964 | 0.091 | 0.966 | 0.091 | 0.968 | 0.089 | 0.437 | 0.000 |
| Folate | 0.656 | 0.183 | 0.654 | 0.184 | 0.657 | 0.181 | 0.658 | 0.182 | 0.677 | 0.000 |
| Niacin | 0.997 | 0.031 | 0.997 | 0.033 | 0.997 | 0.025 | 0.997 | 0.038 | 0.968 | 0.000 |
| Mean adequacy ratio | 0.828 | 0.063 | 0.823 | 0.065 | 0.831 | 0.062 | 0.842 | 0.057 | 0.001 | 0.010 |
| Socioeconomic Status | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | Low | Middle | High | |||||||
| (n = 9218) | (n = 4796) | (n = 3542) | (n = 880) | |||||||
| ELANS | Mean | SD | Mean | SD | Mean | SD | Mean | SD | p Value | η2p |
| Diet quality score | 63.01 | 9.29 | 62.64 | 9.11 | 63.34 | 9.42 | 63.65 | 9.68 | <0.001 | 0.002 |
| Dietary diversity score | 4.79 | 1.34 | 4.65 | 1.33 | 4.90 | 1.33 | 5.08 | 1.30 | <0.001 | 0.012 |
| Mean adequacy ratio | 0.83 | 0.06 | 0.82 | 0.06 | 0.83 | 0.06 | 0.84 | 0.06 | <0.001 | 0.007 |
| Argentina | (n = 1266) | (n = 616) | (n = 585) | (n = 65) | ||||||
| Diet quality score | 63.47 | 9.56 | 62.84 | 9.09 | 63.85 | 9.95 | 66.03 | 10.01 | <0.016 | 0.007 |
| Dietary diversity score | 4.48 | 1.30 | 4.33 | 1.28 | 4.62 | 1.33 | 4.72 | 1.19 | <0.001 | 0.013 |
| Mean adequacy ratio | 0.83 | 0.04 | 0.82 | 0.04 | 0.83 | 0.04 | 0.85 | 0.03 | <0.001 | 0.021 |
| Costa Rica | (n = 798) | (n = 262) | (n = 428) | (n = 108) | ||||||
| Diet quality score | 63.46 | 9.41 | 62.97 | 9.51 | 63.72 | 9.30 | 63.58 | 9.66 | >0.589 | 0.001 |
| Dietary diversity score | 4.97 | 1.35 | 4.70 | 1.27 | 5.08 | 1.37 | 5.20 | 1.35 | <0.001 | 0.020 |
| Mean adequacy ratio | 0.80 | 0.06 | 0.79 | 0.06 | 0.81 | 0.06 | 0.83 | 0.05 | <0.001 | 0.049 |
| Brazil | (n = 2000) | (n = 916) | (n = 915) | (n = 169) | ||||||
| Diet quality score | 63.51 | 9.16 | 63.29 | 8.91 | 63.65 | 9.27 | 63.91 | 9.94 | >0.596 | 0.001 |
| Dietary diversity score | 4.66 | 1.37 | 4.44 | 1.34 | 4.80 | 1.36 | 5.06 | 1.37 | <0.001 | 0.023 |
| Mean adequacy ratio | 0.79 | 0.07 | 0.78 | 0.07 | 0.80 | 0.07 | 0.82 | 0.06 | <0.001 | 0.026 |
| Chile | (n = 879) | (n = 411) | (n = 388) | (n = 80) | ||||||
| Diet quality score | 61.42 | 10.33 | 59.5 | 10.34 | 62.81 | 10.18 | 64.18 | 9.35 | <0.001 | 0.030 |
| Dietary diversity score | 4.78 | 1.20 | 4.75 | 1.26 | 4.78 | 1.16 | 4.95 | 0.99 | >0.406 | 0.002 |
| Mean adequacy ratio | 0.79 | 0.07 | 0.79 | 0.07 | 0.80 | 0.06 | 0.81 | 0.06 | <0.001 | 0.015 |
| Colombia | (n = 1230) | (n = 779) | (n = 384) | (n = 67) | ||||||
| Diet quality score | 63.47 | 9.04 | 63.18 | 8.87 | 63.67 | 9.29 | 65.62 | 9.30 | >0.093 | 0.004 |
| Dietary diversity score | 4.77 | 1.38 | 4.68 | 1.37 | 4.95 | 1.38 | 4.85 | 1.40 | <0.007 | 0.008 |
| Mean adequacy ratio | 0.87 | 0.05 | 0.86 | 0.05 | 0.87 | 0.03 | 0.87 | 0.08 | <0.008 | 0.008 |
| Peru | (n = 1113) | (n = 533) | (n = 355) | (n = 225) | ||||||
| Diet quality score | 63.50 | 9.23 | 64.30 | 8.95 | 63.01 | 9.30 | 62.3 | 9.62 | <0.015 | 0.007 |
| Dietary diversity score | 5.28 | 1.28 | 5.28 | 1.30 | 5.30 | 1.27 | 5.25 | 1.28 | >0.880 | 0.000 |
| MAR | 0.85 | 0.05 | 0.85 | 0.05 | 0.85 | 0.05 | 0.86 | 0.05 | <0.038 | 0.006 |
| Ecuador | (n = 800) | (n = 399) | (n = 297) | (n = 104) | ||||||
| Diet quality score | 63.45 | 8.70 | 63.31 | 8.52 | 63.47 | 8.64 | 63.91 | 9.59 | >0.820 | 0.000 |
| Dietary diversity score | 5.33 | 1.29 | 5.24 | 1.28 | 5.41 | 1.29 | 5.43 | 1.30 | >0.153 | 0.005 |
| Mean adequacy ratio | 0.88 | 0.04 | 0.87 | 0.04 | 0.88 | 0.03 | 0.88 | 0.04 | <0.009 | 0.012 |
| Venezuela | (n = 1132) | (n = 880) | (n = 190) | (n = 62) | ||||||
| Diet quality score | 61.23 | 8.67 | 61.37 | 8.69 | 60.35 | 8.31 | 62.01 | 9.38 | >0.259 | 0.002 |
| Dietary diversity score | 4.39 | 1.14 | 4.37 | 1.15 | 4.40 | 1.05 | 4.55 | 1.18 | >0.484 | 0.001 |
| Mean adequacy ratio | 0.84 | 0.05 | 0.83 | 0.05 | 0.84 | 0.05 | 0.85 | 0.03 | <0.009 | 0.008 |
| Total | Sex | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ELANS | Men | Women | |||||||||
| Socioeconomic Status | Mean | SD | N | Mean | SD | N | Mean | SD | N | % | p Value |
| Low | 26.92 | 5.71 | 879 | 26.01 | 5.11 | 2218 | 27.72 | 6.08 | 2572 | 6.17% | 0.001 |
| Middle | 26.91 | 5.48 | 3539 | 26.52 | 5.22 | 1749 | 27.30 | 5.70 | 1790 | 2.87% | 0.001 |
| High | 27.30 | 5.62 | 4790 | 27.10 | 5.62 | 436 | 27.49 | 5.62 | 443 | 1.40% | 0.311 |
| Total | 26.96 | 5.62 | 9208 | 26.32 | 5.22 | 4403 | 27.54 | 5.90 | 4805 | 1.09% | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez, G.; Kovalskys, I.; Leme, A.C.B.; Quesada, D.; Rigotti, A.; Cortés Sanabria, L.Y.; Yépez García, M.C.; Liria-Domínguez, M.R.; Herrera-Cuenca, M.; Fisberg, R.M.; et al. Socioeconomic Status Impact on Diet Quality and Body Mass Index in Eight Latin American Countries: ELANS Study Results. Nutrients 2021, 13, 2404. https://doi.org/10.3390/nu13072404
Gómez G, Kovalskys I, Leme ACB, Quesada D, Rigotti A, Cortés Sanabria LY, Yépez García MC, Liria-Domínguez MR, Herrera-Cuenca M, Fisberg RM, et al. Socioeconomic Status Impact on Diet Quality and Body Mass Index in Eight Latin American Countries: ELANS Study Results. Nutrients. 2021; 13(7):2404. https://doi.org/10.3390/nu13072404
Chicago/Turabian StyleGómez, Georgina, Irina Kovalskys, Ana Carolina B. Leme, Dayana Quesada, Attilio Rigotti, Lilia Yadira Cortés Sanabria, Martha Cecilia Yépez García, María Reyna Liria-Domínguez, Marianella Herrera-Cuenca, Regina Mara Fisberg, and et al. 2021. "Socioeconomic Status Impact on Diet Quality and Body Mass Index in Eight Latin American Countries: ELANS Study Results" Nutrients 13, no. 7: 2404. https://doi.org/10.3390/nu13072404