
The Role of Resilience and Basic Hope in the Adherence to Dietary Recommendations in the Polish Population during the COVID-19 Pandemic



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Data Collection
2.3. Instruments
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
3.1. Demographic Characteristics
3.2. Psychological Characteristics
3.3. Group Psychological Profile
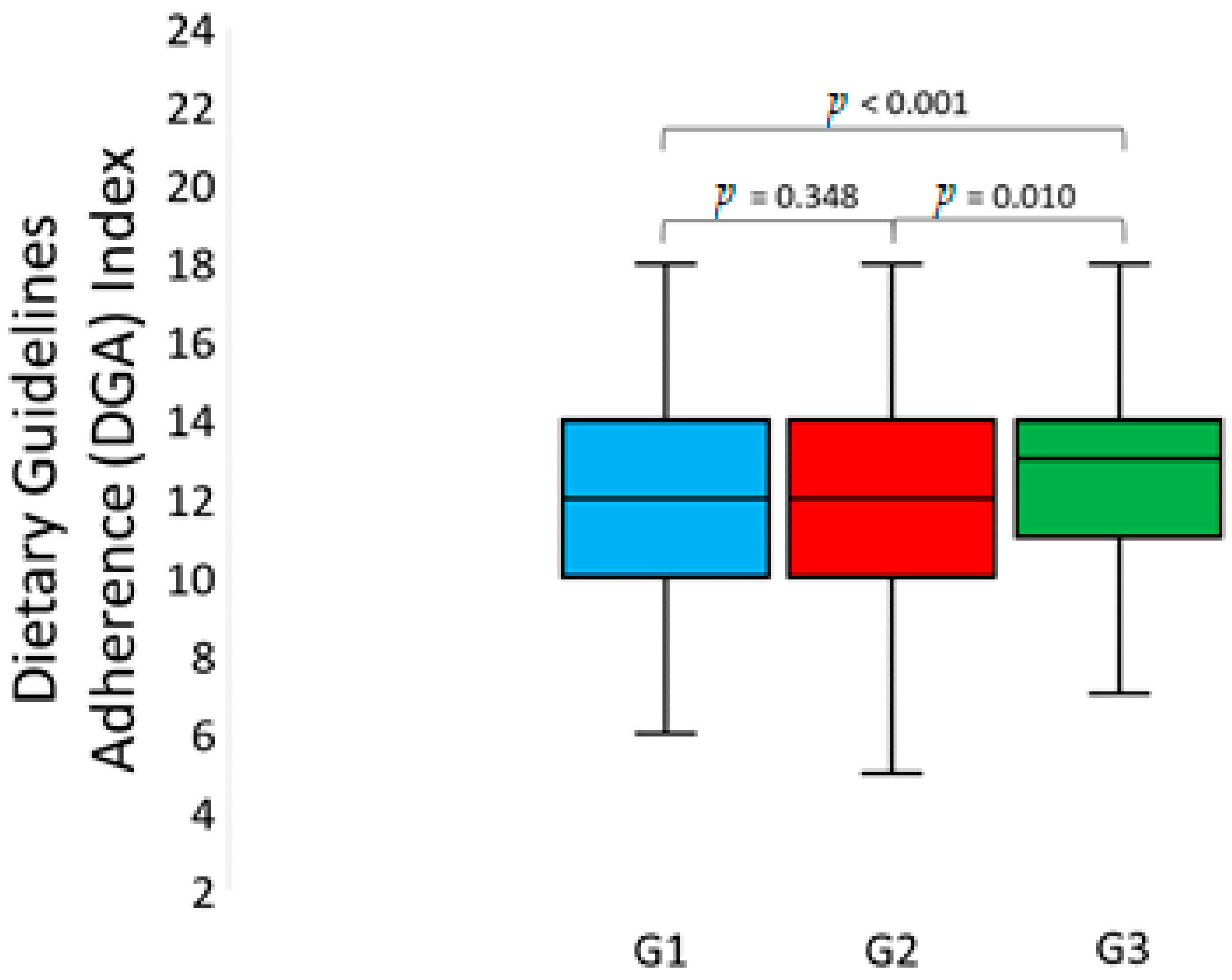
3.4. Intergroup Differences in Dietary Guidelines Adherence Index
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Szczepańska, A.; Pietrzyka, K. The COVID-19 epidemic in Poland and its influence on the quality of life of university students (young adults) in the context of restricted access to public spaces. Z Gesundh Wiss 2021, 7, 1–11. [Google Scholar]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Thu, T.P.B.; Ngoc, P.N.H.; Hai, N.M.; Tuan, L.A. Effect of the social distancing measures on the spread of COVID-19 in 10 highly infected countries. Sci. Total Environ. 2020, 742, 140430. [Google Scholar] [CrossRef] [PubMed]
- Belzunegui-Eraso, A.; Erro-Garcés, A. Teleworking in the Context of the Covid-19 Crisis. Sustainability 2020, 12, 3662. [Google Scholar] [CrossRef]
- Daniel, S.J. Education and the COVID-19 pandemic. Prospects 2020, 49, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Moeckel, R.; Moreno, A.T.; Shuai, B.; Gao, J. A work-life conflict perspective on telework. Transp. Res. Part A Policy Pract. 2020, 141, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Roso, M.B.; de Carvalho Padilha, P.; Mantilla-Escalante, D.C.; Ulloa, N.; Brun, P.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Aires, M.T.; de Oliveira Cardoso, L.; et al. Covid-19 Confinement and Changes of Adolescent’s Dietary Trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients 2020, 12, 1807. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef] [PubMed]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodríguez-Mañas, L. Impact of Social Isolation Due to COVID-19 on Health in Older People: Mental and Physical Effects and Recommendations. J. Nutr. Health Aging 2020, 24, 938–947. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Cinelli, G.; Bigioni, G.; Soldati, L.; Attinà, A.; Bianco, F.F.; Caparello, G.; Camodeca, V.; Carrano, E.; et al. Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients 2020, 12, 2152. [Google Scholar] [CrossRef] [PubMed]
- Piórowska, A.; Basińska, M.; Piórowski, K.; Janicka, M. The Brief Resilience Coping Scale-polska adaptacja Krótkiej Skali Prężności Zaradczej. Prz. Pedag. 2017, 1, 215–227. [Google Scholar]
- Ogińska-Bulik, N.; Juczyński, Z. Skala pomiaru prężności–SPP-25. Now. Psychol. 2008, 3, 39–56. [Google Scholar]
- Sęk, H.; Nadolska, K. Społeczny Kontekst Odkrywania Wiedzy o Zasobach Odpornościowych, Czyli Czym Jest Resilience i Jak ono Funkcjonuje; Wydawnictwo Naukowe Uam: Poznań, Poland, 2007. [Google Scholar]
- Fredrickson, B.L. The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. Am. Psychol. 2001, 56, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Tugade, M.M.; Fredrickson, B.L.; Feldman Barrett, L. Psychological resilience and positive emotional granularity: Examining the benefits of positive emotions on coping and health. J. Pers. 2004, 72, 1161–1190. [Google Scholar] [CrossRef] [PubMed]
- Ogińska-Bulik, N.; Juczyński, Z. Osobowość: Stres a Zdrowie, 2nd ed.; Difin: Warsaw, Poland, 2010; pp. 52–102. [Google Scholar]
- Juczyński, Z. Narzędzia Pomiaru w Promocji Psychologii Zdrowia [Measurement Tools in Promoting Health Psychology]; Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warsaw, Poland, 2009. [Google Scholar]
- Alessandri, G.; Vecchione, M.; Caprara, G.; Letzring, T.D. The ego resiliency scale revised. Eur. J. Psychol. Assess. 2011, 28, 139–146. [Google Scholar] [CrossRef]
- Erikson, E.H. Tożsamość a Cykl Życia; Wyd. Zysk i S-ka: Poznań, Poland, 2004; pp. 46–97. [Google Scholar]
- Geldsetzer, P. Use of Rapid Online Surveys to Assess People’s Perceptions during Infectious Disease Outbreaks: A Cross-sectional Survey on COVID-19. J. Med. Internet Res. 2020, 22, e18790. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Sinclair, V.G.; Wallston, K.A. The development and psychometric evaluation of the Brief Resilience Coping Scale. Assesment 2004, 11, 94–101. [Google Scholar] [CrossRef]
- Trzebiński, J.; Zięba, M. Kwestionariusz Nadziei Podstawowej-BHI-12: Podręcznik; Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warsaw, Poland, 2009. [Google Scholar]
- Talerz Zdrowego Żywienia. Available online: https://ncez.pzh.gov.pl/abc-zywienia/talerz-zdrowego-zywienia/ (accessed on 20 April 2021).
- Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [CrossRef]
- Błaszczyk-Bębenek, E.; Jagielski, P.; Bolesławska, I.; Jagielska, A.; Nitsch-Osuch, A.; Kawalec, P. Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown. Nutrients 2020, 12, 3084. [Google Scholar] [CrossRef] [PubMed]
- Faseeha, A.; Masood, S. How nutrition can help to fight against COVID-19 Pandemic. Pak. J. Med. Sci. 2020, 36, S121–S123. [Google Scholar]
- Connor, K.M. Assessment of resilience in aftermath of trauma. J. Clin. Psych. 2006, 67, 46–49. [Google Scholar]
- Chanduszko-Salska, J. Psychologiczne uwarunkowania nadmiernego zaabsorbowania jedzeniem. Psychiatria 2013, 10, 1–8. [Google Scholar]
- Cummings, J.R.; Ackerman, J.M.; Wolfson, J.A.; Gearhardt, A.N. COVID-19 stress and eating and drinking behaviors in the United States during the early stages of the pandemic. Appetite 2021, 162, 105163. [Google Scholar] [CrossRef] [PubMed]
- Huber, B.C.; Steffen, J.; Schlichtiger, J.; Brunner, S. Altered nutrition behavior during COVID-19 pandemic lockdown in young adults. Eur. J. Nutr. 2020, 1, 1–10. [Google Scholar]
- Yau, Y.H.C.; Potenza, M.N. Stress and eating behaviors. Minerva Endocrinol. 2013, 38, 255–267. [Google Scholar]
- Cecchetto, C.; Aiello, M.; Gentili, C.; Ionta, S.; Osimo, S.A. Increased emotional eating during COVID-19 associated with lockdown, psychological and social distress. Appetite 2021, 1, 105122. [Google Scholar] [CrossRef]
- Dąbrowski, A. Wpływ emocji na poznawanie. Przegląd Filoz. Nowa Ser. 2012, 3, 315–335. [Google Scholar]
- Resnicow, K.; McMaster, F.; Bocian, A.; Harris, D.; Zhou, Y.; Snetselaar, L.; Schwartz, R.; Myers, E.; Gotlieb, J.; Foster, J.; et al. Motivational interviewing and dietary counseling for obesity in primary care: An RCT. Pediatrics 2015, 135, 649–657. [Google Scholar] [CrossRef] [Green Version]
- Coelho-Ravagnani, C.D.F.; Corgosinho, F.C.; La, F.; Ziegler, F.; Marques, C.; Prado, M.; Laviano, A.; Mota, F. Dietary recommendations during the COVID-19 pandemic. Nutr. Rev. 2021, 79, 382–393. [Google Scholar] [CrossRef]
- World Health Organization. Fruit and Vegetables for Health: Report of the Joint FAO/WHO Workshop on Fruit and Vegetables for Health, 1–3 September 2004, Kobe, Japan; World Health Organization: Geneva, Switzerland, 2005; Available online: https://apps.who.int/iris/handle/10665/43143 (accessed on 20 April 2021).
- Jideani, A.I.O.; Silungwe, H.; Takalani, T.; Omolola, A.O.; Udeh, H.O.; Anyasi, T.A. Antioxidant-rich natural fruit and vegetable products and human health. Int. J. Food Prop. 2021, 24, 41–67. [Google Scholar] [CrossRef]
- Kaluza, J.; Harris, H.R.; Linden, A.; Wolk, A. Long-term consumption of fruits and vegetables and risk of chronic obstructive pulmonary disease: A prospective cohort study of women. Int. J. Epidemiol. 2018, 47, 1897–1909. [Google Scholar] [CrossRef] [PubMed]
- Holt, E.M.; Steffen, L.M.; Moran, A.; Basu, S.; Steinberger, J.; Ross, J.A.; Hong, C.P.; Sinaiko, A.R. Fruit and vegetable consumption and its relation to markers of inflammation and oxidative stress in adolescents. J. Am. Diet. Assoc. 2009, 109, 414–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohlouli, J. COVID-19 and Fast Foods Consumption: A Review. Int. J. Food Prop. 2021, 24, 203–209. [Google Scholar] [CrossRef]
- Liua, N.; Sunb, J.; Wang, X.; Zhang, T.; Zhao, M.; Li, H. Low vitamin D status is associated with coronavirus disease 2019, outcomes: A systematic review and meta-analysis. Int. J. Infect. Dis. 2021, 104, 58–64. [Google Scholar]
- Albert, C.M.; Hennekens, C.H.; O’Donnell, C.J.; Ajani, U.A.; Carey, V.J.; Willett, W.C.; Ruskin, J.N.; Manson, J.E. Fish consumption and risk of sudden cardiac death. JAMA 1998, 279, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Hathaway, D.; Pandav, K.; Patel, M.; Riva-Moscoso, A.; Singh, B.M.; Patel, A.; Min, Z.C.; Singh-Makkar, S.; Sana, M.K.; Sanchez-Dopazo, R.; et al. Omega 3 Fatty Acids and COVID-19: A Comprehensive Review. Infect. Chemother. 2020, 52, 478–495. [Google Scholar]
- Ruxton, C.H.; Reed, S.C.; Simpson, M.J.; Millington, K.J. The health benefits of omega-3 polyunsaturated fatty acids: A review of the evidence. J. Hum. Nutr. Diet. 2004, 17, 449–459. [Google Scholar] [CrossRef]
- Grupo Colaborativo de la Sociedad Española de Nutrición Comunitaria (SENC); Aranceta Bartrina, J.; Arija Val, V.; Maíz Aldalur, E.; Martínez de la Victoria Muñoz, E.; Ortega Anta, R.M.; Pérez Rodrigo, C.; Quiles Izquierdo, J.; Rodríguez Martín, A.; Román Viñas, B.; et al. Dietary guidelines for the Spanish population (SENC, December 2016); the new graphic icon of healthy nutrition. Nutr. Hosp. 2016, 33, 1–48. [Google Scholar]
- Granieland, I.P.; Salas-Salvadó, J. Nut Consumption in the Time of COVID-19 Health Benefits of Nuts and Dried Fruits. Available online: https://www.nutfruit.org/consumers/news/detail/nut-consumption-in-the-time-of-covid-19 (accessed on 18 April 2021).
- Jéquier, E.; Constant, F. Water as an essential nutrient: The physiological basis of hydration. Eur. J. Clin. Nutr. 2010, 64, 115–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, R. Boost Your Immune System by Drinking Water. Available online: https://www.tyentusa.com/blog/immune-systemdrinking-water/ (accessed on 15 April 2021).
- Apovian, C. Sugar-sweetened soft drinks, obesity, and type 2 diabetes. JAMA 2004, 292, 978–979. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.P.; Hu, F.B. Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation 2010, 12, 1356–1364. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Efects of soft drink consumption on nutrition and health: A systematic review and metaanalysis. Am. J. Public Health 2011, 97, 667–675. [Google Scholar] [CrossRef]
- Coulthard, H.; Sharps, M.; Cunliffe, L.; van den Tol, A. Eating in the lockdown during the Covid 19 pandemic; self-reported changes in eating behaviour, and associations with BMI, eating style, coping and health anxiety. Appetite 2021, 161, 105082. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group of Products | Recommended Frequency of Consumption |
|---|---|
| Groups of healthy products | |
| Vegetables | a few times a day |
| Fruits | once a day or more |
| Whole grains | once a day or more |
| Dairy products (no added sugar) | once a day or more |
| Legumes | a few times a week or more |
| Fish | once a week or more |
| Unsalted nuts, seeds | a few times a week or more |
| White meat | a few times a week or less |
| Oils/margarines | a few times a week or more |
| Water | once a day or more |
| Groups of unhealthy products | |
| Red and processed meat | once a week or less |
| Sweets | once a week or less |
| Salty snacks | once a week or less |
| Sweetened drinks | once a week or less |
| Refined grains | once a day or less |
| Fast food | once a week or less |
| Butter/lard | once a week or less |
| Processed cheese | once a week or less |
| Age (years) | The value of variable |
| M ± SD (95% CI) | 31.6 ± 11.98 (30.9–32.3) |
| Mdn ± IQR/2 | 27.0 ± 9.00 |
| Min-max | 18.0—82.0 |
| Gender, N (%) | The value of variable |
| Male | 148 (13.7) |
| Female | 934 (86.3) |
| Place of residence, N (%) | The value of variable |
| Village | 181 (16.7) |
| Small town | 193 (17.8) |
| Town | 178 (16.5) |
| Big city | 530 (49.0) |
| Education, N (%) | The value of variable |
| Primary/vocational | 13 (1.2) |
| Secondary | 355 (32.8) |
| Tertiary | 714 (66.0) |
| Psychological Characteristic | Level | N | % |
|---|---|---|---|
| Stress | |||
| low | 381 | 35.2 | |
| moderate | 348 | 32.2 | |
| high | 353 | 32.6 | |
| Resilience | |||
| low | 270 | 25.0 | |
| moderate | 483 | 44.6 | |
| high | 329 | 30.4 | |
| Basic hope | |||
| low | 301 | 27.8 | |
| moderate | 439 | 40.6 | |
| high | 342 | 31.6 |
| G1 (N = 352) | G2 (N = 334) | G3 (N = 396) | F(2, 1079) | p-Value * | ||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||
| Stress | 7.3 | 1.14 | 3.8 | 1.11 | 5.3 | 1.71 | 577.311 | <0.001 |
| Resilience | 4.5 | 1.73 | 4.7 | 1.61 | 7.0 | 1.29 | 302.021 | <0.001 |
| Basic hope | 4.3 | 1.59 | 5.0 | 1.58 | 7.2 | 1.37 | 373.917 | <0.001 |
| Product Group | G1 (N = 352) | G2 (N = 334) | G3 (N = 396) | χ2df = 2 | p-Value 1 | |||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Groups of healthy products | ||||||||
| Vegetables | 185 | 52.6 | 192 | 57.5 | 259 | 65.4 | 13.029 | 0.001 |
| Fruits | 212 | 60.2 | 201 | 60.2 | 272 | 68.7 | 7.778 | 0.020 |
| Whole grains | 135 | 38.4 | 130 | 38.9 | 188 | 47.5 | 8.093 | 0.017 |
| Dairy products (no added sugar) | 173 | 49.2 | 152 | 45.7 | 220 | 55.6 | 7.442 | 0.024 |
| Legumes | 109 | 31.1 | 105 | 31.4 | 131 | 33.1 | 0.403 | 0.818 |
| Fish | 111 | 31.5 | 115 | 34.4 | 180 | 45.6 | 17.650 | 0.000 |
| Unsalted nuts, seeds | 155 | 44.0 | 160 | 47.9 | 223 | 56.5 | 12.160 | 0.002 |
| White meat | 331 | 94.0 | 316 | 94.6 | 372 | 93.9 | 0.168 | 0.919 |
| Oils/margarines | 288 | 81.8 | 279 | 83.5 | 328 | 82.8 | 0.358 | 0.836 |
| Water | 329 | 93.5 | 304 | 91.0 | 381 | 96.2 | 8.355 | 0.015 |
| Groups of unhealthy products | ||||||||
| Red and processed meat | 294 | 83.5 | 272 | 81.4 | 309 | 78.0 | 3.735 | 0.155 |
| Sweets | 125 | 35.5 | 133 | 39.8 | 160 | 40.4 | 2.169 | 0.338 |
| Salty snacks | 290 | 82.4 | 289 | 86.5 | 342 | 86.6 | 3.275 | 0.195 |
| Sweetened drinks | 242 | 69.0 | 262 | 78.7 | 309 | 78.0 | 11.243 | 0.004 |
| Refined grains | 351 | 99.7 | 334 | 100.0 | 396 | 100.0 | 2.076 | 0.354 |
| Fast food | 329 | 93.5 | 321 | 96.1 | 379 | 96.0 | 3.397 | 0.183 |
| Butter/lard | 349 | 99.2 | 331 | 99.1 | 390 | 98.5 | 0.942 | 0.624 |
| Processed cheese | 158 | 44.9 | 146 | 43.8 | 168 | 42.4 | 0.466 | 0.792 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sińska, B.; Jaworski, M.; Panczyk, M.; Traczyk, I.; Kucharska, A. The Role of Resilience and Basic Hope in the Adherence to Dietary Recommendations in the Polish Population during the COVID-19 Pandemic. Nutrients 2021, 13, 2108. https://doi.org/10.3390/nu13062108
Sińska B, Jaworski M, Panczyk M, Traczyk I, Kucharska A. The Role of Resilience and Basic Hope in the Adherence to Dietary Recommendations in the Polish Population during the COVID-19 Pandemic. Nutrients. 2021; 13(6):2108. https://doi.org/10.3390/nu13062108
Chicago/Turabian StyleSińska, Beata, Mariusz Jaworski, Mariusz Panczyk, Iwona Traczyk, and Alicja Kucharska. 2021. "The Role of Resilience and Basic Hope in the Adherence to Dietary Recommendations in the Polish Population during the COVID-19 Pandemic" Nutrients 13, no. 6: 2108. https://doi.org/10.3390/nu13062108