
Dietary Patterns in Early Childhood and the Risk of Childhood Overweight: The GECKO Drenthe Birth Cohort

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Dietary Data
2.3. Growth Measures during Childhood
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Cross-Sectional and Prospective Associations between Dietary Patterns and Overweight at 3 and 10 Years
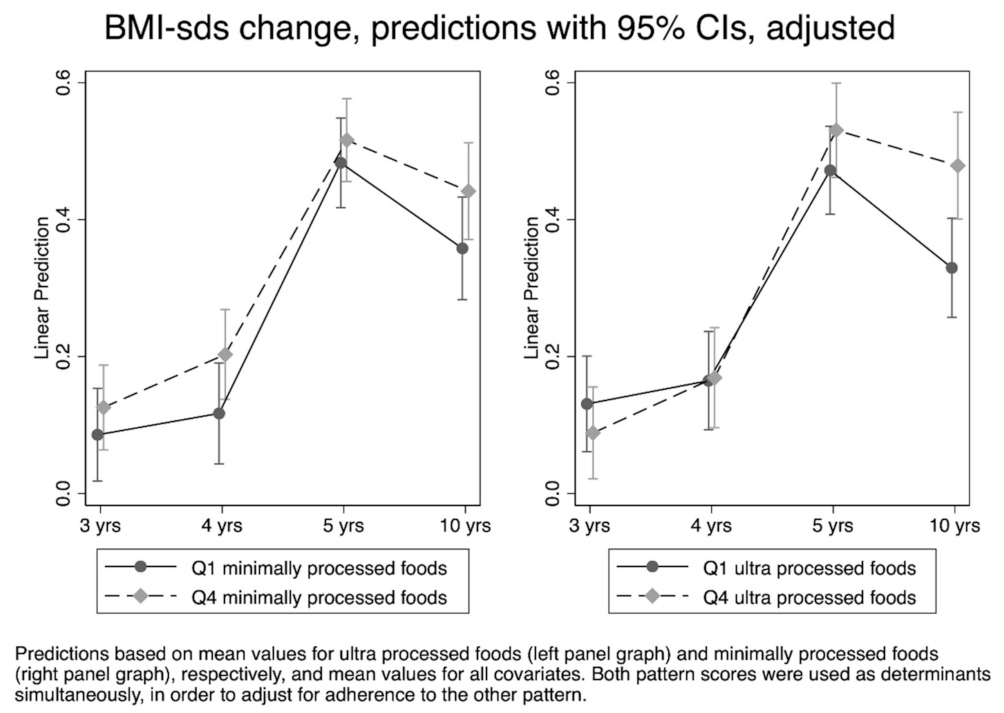
3.2. BMI-SDS Development
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, A.S.; Mulder, C.; Twisk, J.W.; van Mechelen, W.; Chinapaw, M.J. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef] [Green Version]
- Moreno, L.A.; Bel-Serrat, S.; Santaliestra-Pasías, A.M.; Rodríguez, G. Obesity prevention in children. World Rev. Nutr. Diet. 2013, 106, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Robinson, S.; Fall, C. Infant nutrition and later health: A review of current evidence. Nutrients 2012, 4, 859–874. [Google Scholar] [CrossRef] [Green Version]
- Liberali, R.; Kupek, E.; Assis, M.A.A. Dietary Patterns and Childhood Obesity Risk: A Systematic Review. Child. Obes. 2020, 16, 70–85. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Ambrosini, G.L. Childhood dietary patterns and later obesity: A review of the evidence. Proc. Nutr. Soc. 2014, 73, 137–146. [Google Scholar] [CrossRef]
- Flynn, A.C.; Thompson, J.M.D.; Dalrymple, K.V.; Wall, C.; Begum, S.; Pallippadan Johny, J.; Cutfield, W.S.; North, R.; McCowan, L.M.E.; Godfrey, K.M.; et al. Childhood dietary patterns and body composition at age 6 years: The Children of SCOPE study. Br. J. Nutr. 2020, 124, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Makrides, M.; Zhou, S.J. Dietary patterns and obesity in preschool children in Australia: A cross-sectional study. Asia Pac. J. Clin. Nutr. 2018, 27, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Dalrymple, K.V.; Flynn, A.C.; Seed, P.T.; Briley, A.L.; O’Keeffe, M.; Godfrey, K.M.; Poston, L. Associations between dietary patterns, eating behaviours, and body composition and adiposity in 3-year-old children of mothers with obesity. Pediatr. Obes. 2020, 15, e12608. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, L.; Shatila, H.; Itani, L.; Hwalla, N.; Jomaa, L.; Naja, F. A traditional dietary pattern is associated with lower odds of overweight and obesity among preschool children in Lebanon: A cross-sectional study. Eur. J. Nutr. 2019, 58, 91–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieira-Ribeiro, S.A.; Andreoli, C.S.; Fonseca, P.C.A.; Hermsdorff, H.H.M.; Pereira, P.F.; Ribeiro, A.Q.; Priore, S.E.; Franceschini, S.C.C. Dietary patterns and body adiposity in children in Brazil: A cross-sectional study. Public Health 2019, 166, 140–147. [Google Scholar] [CrossRef]
- Bell, L.K.; Golley, R.K.; Daniels, L.; Magarey, A.M. Dietary patterns of Australian children aged 14 and 24 months, and associations with socio-demographic factors and adiposity. Eur. J. Clin. Nutr. 2013, 67, 638–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shroff, M.R.; Perng, W.; Baylin, A.; Mora-Plazas, M.; Marin, C.; Villamor, E. Adherence to a snacking dietary pattern and soda intake are related to the development of adiposity: A prospective study in school-age children. Public Health Nutr. 2014, 17, 1507–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Alvira, J.M.; Bammann, K.; Eiben, G.; Hebestreit, A.; Kourides, Y.A.; Kovacs, E.; Michels, N.; Pala, V.; Reisch, L.; Russo, P.; et al. Prospective associations between dietary patterns and body composition changes in European children: The IDEFICS study. Public Health Nutr. 2017, 20, 3257–3265. [Google Scholar] [CrossRef] [Green Version]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. Energy-dense, low-fiber, high-fat dietary pattern is associated with increased fatness in childhood. Am. J. Clin. Nutr. 2008, 87, 846–854. [Google Scholar] [CrossRef] [Green Version]
- Durao, C.; Severo, M.; Oliveira, A.; Moreira, P.; Guerra, A.; Barros, H.; Lopes, C. Association between dietary patterns and adiposity from 4 to 7 years of age. Public Health Nutr. 2017, 20, 1973–1982. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Armstrong, J.; Dorosty, A.R.; Emmett, P.M.; Ness, A.; Rogers, I.; Steer, C.; Sherriff, A. Early life risk factors for obesity in childhood: Cohort study. BMJ 2005, 330, 1357. [Google Scholar] [CrossRef] [Green Version]
- Rashid, V.; Streppel, M.T.; Engberink, M.F.; Weijs, P.J.M.; Nicolaou, M.; Verhoeff, A.P. Weight development between age 5 and 10 years and its associations with dietary patterns at age 5 in the ABCD cohort. BMC Public Health 2020, 20, 427. [Google Scholar] [CrossRef]
- Luque, V.; Escribano, J.; Closa-Monasterolo, R.; Zaragoza-Jordana, M.; Ferré, N.; Grote, V.; Koletzko, B.; Totzauer, M.; Verduci, E.; ReDionigi, A.; et al. Unhealthy Dietary Patterns Established in Infancy Track to Mid-Childhood: The EU Childhood Obesity Project. J. Nutr. 2018, 148, 752–759. [Google Scholar] [CrossRef]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The cardiovascular risk in Young Finns Study. Br. J. Nutr. 2005, 93, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Betoko, A.; Forhan, A.; Charles, M.A.; Heude, B.; de Lauzon-Guillain, B. Dietary patterns track from infancy to preschool age: Cross-sectional and longitudinal perspectives. J. Nutr. 2015, 145, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, M.; Brantsæter, A.L.; Haugen, M.; Meltzer, H.M.; Nystad, W.; Andersen, L.F. Changes and tracking of fruit, vegetables and sugar-sweetened beverages intake from 18 months to 7 years in the Norwegian Mother and Child Cohort Study. BMC Public Health 2013, 13, 793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- L’Abée, C.; Sauer, P.J.; Damen, M.; Rake, J.P.; Cats, H.; Stolk, R.P. Cohort Profile: The GECKO Drenthe study, overweight programming during early childhood. Int. J. Epidemiol. 2008, 37, 486–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutman, A.E.; Stafleu, A.; Kruizinga, A.; Brants, H.A.; Westerterp, K.R.; Kistemaker, C.; Meuling, W.J.; Goldbohm, R.A. Validation of an FFQ and options for data processing using the doubly labelled water method in children. Public Health Nutr. 2011, 14, 410–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- RIVM/Voedingscentrum. NEVO-Tabel Nederlands Voedingsstoffenbestand; RIVM: Den Haag, The Netherlands, 2011. [Google Scholar]
- De Onis, M.; Garza, C.; Onyango, A.W.; Rolland-Cachera, M.F. WHO growth standards for infants and young children. Arch. Pediatr. 2009, 16, 47–53. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Fredriks, A.M.; van Buuren, S.; Burgmeijer, R.J.F.; Verloove-Vanhorick, S.P.; de Wit, J.M. Groeidiagrammen 2010. Handleiding bij het Meten en Wegen van Kinderen en het Invullen van Groeidiagrammen; TNO: Leiden, The Netherlands, 2010. [Google Scholar]
- Northstone, K.; Emmett, P. Multivariate analysis of diet in children at four and seven years of age and associations with socio-demographic characteristics. Eur. J. Clin. Nutr. 2005, 59, 751–760. [Google Scholar] [CrossRef] [Green Version]
- North, K.; Emmett, P. Multivariate analysis of diet among three-year-old children and associations with socio-demographic characteristics. The Avon Longitudinal Study of Pregnancy and Childhood (ALSPAC) Study Team. Eur. J. Clin. Nutr. 2000, 54, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Patrick, H.; Nicklas, T.A. A review of family and social determinants of children’s eating patterns and diet quality. J. Am. Coll. Nutr. 2005, 24, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Statistics Netherlands (CBS). Level of Education. Available online: http://www.cbs.nl/en-GB/menu/methoden/toelichtingen/alfabet/l/level+of+education+1.htm (accessed on 12 February 2021).
- Stronks, K.; Kulu-Glasgow, I.; Agyemang, C. The utility of ‘country of birth’ for the classification of ethnic groups in health research: The Dutch experience. Ethn. Health 2009, 14, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Cheikh Ismail, L.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Can. J. Diet. Pract. Res. 2007, 68, s1–s56. [Google Scholar]
- Powell, F.; Farrow, C.; Meyer, C.; Haycraft, E. The Stability and Continuity of Maternally Reported and Observed Child Eating Behaviours and Feeding Practices across Early Childhood. Int. J. Environ. Res. Public Health 2018, 15, 1017. [Google Scholar] [CrossRef] [Green Version]
- Cecil, J.E.; Palmer, C.N.; Wrieden, W.; Murrie, I.; Bolton-Smith, C.; Watt, P.; Wallis, D.J.; Hetherington, M.M. Energy intakes of children after preloads: Adjustment, not compensation. Am. J. Clin. Nutr. 2005, 82, 302–308. [Google Scholar] [CrossRef]
- Northstone, K.; Emmett, P.M. Are dietary patterns stable throughout early and mid-childhood? A birth cohort study. Br. J. Nutr. 2008, 100, 1069–1076. [Google Scholar] [CrossRef] [Green Version]
- Craig, L.C.; McNeill, G.; Macdiarmid, J.I.; Masson, L.F.; Holmes, B.A. Dietary patterns of school-age children in Scotland: Association with socio-economic indicators, physical activity and obesity. Br. J. Nutr. 2010, 103, 319–334. [Google Scholar] [CrossRef] [Green Version]
- Zhen, S.; Ma, Y.; Zhao, Z.; Yang, X.; Wen, D. Dietary pattern is associated with obesity in Chinese children and adolescents: Data from China Health and Nutrition Survey (CHNS). Nutr. J. 2018, 17, 68. [Google Scholar] [CrossRef] [Green Version]
- Brink, E.; van Rossum, C.; Postma-Smeets, A.; Stafleu, A.; Wolvers, D.; van Dooren, C.; Toxopeus, I.; Buurma-Rethans, E.; Geurts, M.; Ocké, M. Development of healthy and sustainable food-based dietary guidelines for the Netherlands. Public Health Nutr. 2019, 22, 2419–2435. [Google Scholar] [CrossRef] [Green Version]
- Rashid, V.; Engberink, M.F.; van Eijsden, M.; Nicolaou, M.; Dekker, L.H.; Verhoeff, A.P.; Weijs, P.J.M. Ethnicity and socioeconomic status are related to dietary patterns at age 5 in the Amsterdam born children and their development (ABCD) cohort. BMC Public Health 2018, 18, 115. [Google Scholar] [CrossRef] [Green Version]
- Gibney, M.J. Ultra-Processed Foods: Definitions and Policy Issues. Curr. Dev. Nutr. 2019, 3, nzy077. [Google Scholar] [CrossRef] [Green Version]
- Viskaal-van Dongen, M.; Kok, F.J.; de Graaf, C. Eating rate of commonly consumed foods promotes food and energy intake. Appetite 2011, 56, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Jebb, S.A. Dietary determinants of obesity. Obes. Rev. 2007, 8 (Suppl. S1), 93–97. [Google Scholar] [CrossRef]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.Y.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V.; et al. Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metab. 2019, 30, 67–77.e63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forde, C.G.; Mars, M.; de Graaf, K. Ultra-Processing or Oral Processing? A Role for Energy Density and Eating Rate in Moderating Energy Intake from Processed Foods. Curr. Dev. Nutr. 2020, 4, nzaa019. [Google Scholar] [CrossRef]
- Khandpur, N.; Neri, D.A.; Monteiro, C.; Mazur, A.; Frelut, M.L.; Boyland, E.; Weghuber, D.; Thivel, D. Ultra-Processed Food Consumption among the Paediatric Population: An Overview and Call to Action from the European Childhood Obesity Group. Ann. Nutr. Metab. 2020, 76, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Wiersma, R.; Hartman, E.; Boezen, H.M.; Corpeleijn, E. Adiposity and High Blood Pressure during Childhood: A Prospective Analysis of the Role of Physical Activity Intensity and Sedentary Time in the GECKO Drenthe Cohort. Int. J. Environ. Res. Public Health 2020, 17, 9526. [Google Scholar] [CrossRef] [PubMed]
- Olafsdottir, A.S.; Thorsdottir, I.; Gunnarsdottir, I.; Thorgeirsdottir, H.; Steingrimsdottir, L. Comparison of women’s diet assessed by FFQs and 24-hour recalls with and without underreporters: Associations with biomarkers. Ann. Nutr. Metab. 2006, 50, 450–460. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Maternal Characteristics | n (%) 1 |
|---|---|
| Age, mean (SD) | 31.2 (4.2) |
| Educational level | |
| Low | 28.6 (368) |
| Middle | 32.8 (422) |
| High | 38.7 (498) |
| Ethnicity | |
| Dutch | 97.5 (1259) |
| Other | 2.5 (32) |
| Pre-pregnancy BMI, mean (SD) | 24.8 (4.7) |
| Overweight % (n) | 38.5 (494) |
| Parity | |
| Multiparous | 39.6 (516) |
| Smoking during pregnancy | |
| Yes | 11.7 (152) |
| Child characteristics | |
| Sex | |
| Male | 50.5 (660) |
| Birth weight (g), mean (SD) | 3563.6 (557.0) |
| Age at diet measurement (years), mean (SD) | 3.1 (0.4) |
| Age at 3-year BMI measurement (years), mean (SD) | 3.1 (0.1) |
| Age at 10-year BMI measurement (years), mean (SD) | 10.6 (0.5) |
| BMI and overweight at 3 years (n = 938) | |
| BMI, mean (SD) | 16.0 (1.2) |
| Overweight (%, n); according to Cole and Lobstein [29] | 13.6 (128) |
| Overweight (%, n); according to WHO [27] | 3.5 (33) |
| BMI and overweight at 10 years (n = 938) | |
| BMI, mean (SD) | 17.8 (2.8) |
| Overweight (%, n); according to Cole and Lobstein [29] | 16.4 (154) |
| Overweight (%, n); according to WHO [28] | 22.3 (209) |
| Factor Loadings | ||
|---|---|---|
| Dietary Pattern 1 ‘Minimally Processed Foods’ | Dietary Pattern 2 ‘Ultra-Processed Foods’ | |
| Water | 0.20 | −0.04 |
| Vegetables | 0.61 | −0.17 |
| Fruit | 0.18 | −0.22 |
| Whole-grain bread | 0.28 | −0.65 |
| Fish | 0.30 | 0.01 |
| Sauces | 0.58 | 0.00 |
| Potatoes, plain | 0.41 | 0.14 |
| Eggs | 0.27 | 0.09 |
| Fried and baked potatoes | 0.40 | 0.18 |
| Savory dishes | 0.48 | −0.03 |
| Chicken | 0.32 | 0.03 |
| Meat | 0.43 | 0.29 |
| Milk and buttermilk | 0.12 | −0.21 |
| Dairy desserts | 0.23 | 0.07 |
| Crisps | 0.26 | 0.41 |
| Cheese | 0.28 | −0.18 |
| Cakes and confectionery | 0.22 | 0.26 |
| Butter and oil | 0.14 | 0.02 |
| White bread | −0.15 | 0.64 |
| Breakfast cereals | 0.16 | −0.12 |
| Added sugar | 0.16 | 0.17 |
| Sweet bread toppings | 0.05 | 0.05 |
| Sugar-sweetened beverages | 0.14 | 0.34 |
| Cookies | 0.24 | 0.27 |
| Rice and pasta | 0.53 | −0.26 |
| Vegetarian meat substitutes | 0.02 | −0.26 |
| Porridge | 0.11 | 0.02 |
| Soya milk products | 0.01 | −0.11 |
| Nuts and raisins | 0.25 | 0.00 |
| Crackers | 0.12 | 0.00 |
| Savory snacks | 0.31 | 0.41 |
| Dairy drinks with sugar | 0.04 | 0.34 |
| Light drinks | 0.02 | 0.07 |
| Nutrients | Pearson’s correlation coefficient | |
| Total energy, mean (kcal/d) | 0.7 ** | 0.4 ** |
| Protein (E%) | 0.3 ** | −0.2 ** |
| Fat (E%) | 0.2 ** | 0.1 * |
| Carbohydrates (E%) | −0.3 ** | 0.1 * |
| Mono- and disaccharides (E%) | −0.2 ** | 0.1 ** |
| Fiber (g/MJ) | 0.7 ** | −0.1 ** |
| Overweight at 3 Years * | ||||||
|---|---|---|---|---|---|---|
| Model 1, Crude | Model 2, Adjusted | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Dietary pattern | ||||||
| Pattern 1: ‘minimally processed foods foods’ | 1.07 | 0.89, 1.28 | 0.46 | 1.10 | 0.91, 1.33 | 0.31 |
| Pattern 2: ‘ultra-processed foods’ | 1.02 | 0.85, 1.23 | 0.67 | 0.94 | 0.77, 1.15 | 0.54 |
| Overweight at 10 Years * | ||||||
|---|---|---|---|---|---|---|
| Model 1, Crude | Model 2, Adjusted | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Dietary pattern | ||||||
| Pattern 1: ‘minimally processed foods’ | 0.99 | 0.84, 1.18 | 0.94 | 1.03 | 0.86, 1.24 | 0.74 |
| Pattern 2: ‘ultra-processed foods’ | 1.36 | 1.14, 1.61 | 0.001 | 1.30 | 1.08, 1.57 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sirkka, O.; Fleischmann, M.; Abrahamse-Berkeveld, M.; Halberstadt, J.; Olthof, M.R.; Seidell, J.C.; Corpeleijn, E. Dietary Patterns in Early Childhood and the Risk of Childhood Overweight: The GECKO Drenthe Birth Cohort. Nutrients 2021, 13, 2046. https://doi.org/10.3390/nu13062046
Sirkka O, Fleischmann M, Abrahamse-Berkeveld M, Halberstadt J, Olthof MR, Seidell JC, Corpeleijn E. Dietary Patterns in Early Childhood and the Risk of Childhood Overweight: The GECKO Drenthe Birth Cohort. Nutrients. 2021; 13(6):2046. https://doi.org/10.3390/nu13062046
Chicago/Turabian StyleSirkka, Outi, Maria Fleischmann, Marieke Abrahamse-Berkeveld, Jutka Halberstadt, Margreet R. Olthof, Jacob C. Seidell, and Eva Corpeleijn. 2021. "Dietary Patterns in Early Childhood and the Risk of Childhood Overweight: The GECKO Drenthe Birth Cohort" Nutrients 13, no. 6: 2046. https://doi.org/10.3390/nu13062046