
The Sleep and Recovery Practices of Athletes

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. EuroQoL (EQ-5D-5L)
2.3.2. Pittsburgh Sleep Quality Index (PSQI)
2.3.3. Epworth Sleepiness Scale (ESS)
2.3.4. The Recovery Stress Questionnaire for Athletes (RESTQ Sport)
2.3.5. Athlete Morningness/Eveningness Questionnaire (AMES)
2.3.6. Consensus Sleep Diary—Core (CSD-C)
2.4. Supplementation
2.5. Data Analysis
3. Results
3.1. Participant Characteristics
3.1.1. EuroQoL
3.1.2. Pittsburgh Sleep Quality Index
3.2. Epworth Sleepiness Scale
3.3. Recovery Stress Questionnaire
3.3.1. AMES
3.3.2. Consensus Sleep Diary—Core
3.3.3. Nutrition
4. Discussion
4.1. Sleep
4.2. Pittsburg Sleep Quality Index
4.3. Consensus Sleep Diary-Core
4.3.1. Daytime Sleepiness
4.3.2. Athlete Morningness/Eveningness
4.4. Recovery
4.4.1. EuroQoL
4.4.2. REST-Q Sport
4.5. Nutrition
4.6. Limitations
4.7. Future Research
4.8. Practical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Venter, R.E. Role of sleep in performance and recovery of athletes: A review article. S. Afr. J. Res. Sport Phys. Educ. Recreat. 2012, 34, 167–184. [Google Scholar]
- Hartwig, T.B.; Naughton, G.; Searl, J. Load, stress, and recovery in adolescent rugby union players during a competitive season. J. Sports Sci. 2009, 27, 1087–1094. [Google Scholar] [CrossRef] [PubMed]
- Knicker, A.J.; Renshaw, I.; Oldham, A.R.; Cairns, S.P. Interactive processes link the multiple symptoms of fatigue in sport competition. Sports Med. 2011, 41, 307–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noakes, T. Fatigue is a brain-derived emotion that regulates the exercise behaviour to ensure the protection of whole body homeostasis. Front. Physiol. 2012, 3, 1–13. [Google Scholar] [CrossRef] [Green Version]
- St Clair Gibson, A.; Noakes, T. Evidence for complex system integration and dynamic neural regulation of skeletal muscle recruitment during exercise in humans. Br. J. Sports Med. 2004, 38, 797–806. [Google Scholar] [CrossRef]
- Marcora, S.M. Do we really need a central governor to explain brain regulation of exercise performance? Eur. J. Appl. Physiol. 2008, 104, 929–931. [Google Scholar] [CrossRef]
- Marino, F.E. Anticipatory regulation and avoidance of catastrophe during exercise-induced hyperthermia. Comp. Biochem. Physiol. Part B Biochem. Mol. Biol. 2004, 139, 561–569. [Google Scholar] [CrossRef]
- Meerlo, P.; Sgoifo, A.; Suchecki, D. Restricted and disrupted sleep: Effects on autonomic function, neuroendocrine stress systems and stress responsivity. Sleep Med. Rev. 2008, 12, 197–210. [Google Scholar] [CrossRef]
- Morselli, L.; Leproult, R.; Balbo, M.; Spiegel, K. Role of sleep duration in the regulation of glucose metabolism and appetite. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 687–702. [Google Scholar] [CrossRef] [Green Version]
- Knutson, K.L.; Spiegel, K.; Penev, P.; Van Cauter, E. The metabolic consequences of sleep deprivation. Sleep Med. Rev. 2007, 11, 163–178. [Google Scholar] [CrossRef] [Green Version]
- Atrooz, F.; Salim, S. Sleep deprivation, oxidative stress and inflammation. In Advances in Protein Chemistry and Structural Biology; Donev, R., Ed.; Academic Press: Cambridge, MA, USA, 2020; pp. 309–336. [Google Scholar]
- Fullagar, H.H.; Bartlett, J.D. Time to wake up: Individualising the approach to sleep promotion interventions. Br. J. Sports Med. 2016, 50, 143–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Pauw, K.; Roelands, B.; Marušič, U.; Tellez, H.F.; Knaepen, K.; Meeusen, R. Brain mapping after prolonged cycling and during recovery in the heat. J. Appl. Physiol. 2013, 115, 1324–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borrensen, J.; Lambert, M.I. The quantification of training load, the training response and the effect on performance. Sports Med. 2009, 39, 779–795. [Google Scholar] [CrossRef] [PubMed]
- Spencer, M.; Bishop, D.; Dawson, B.; Goodman, C. Physiological and metabolic responses of repeated-sprint activities. Sports Med. 2005, 35, 1025–1044. [Google Scholar] [CrossRef] [PubMed]
- Rampinini, E.; Bosio, A.; Ferraresi, I.; Petruolo, A.; Morelli, A.; Sassi, A. Match-related fatigue in soccer players. Med. Sci. Sports Exerc. 2011, 43, 2161–2170. [Google Scholar] [CrossRef] [PubMed]
- Duffield, R.; Murphy, A.; Snape, A.; Minett, G.M.; Skein, M. Post-match changes in neuromuscular function and the relationship to match demands in amateur rugby league matches. J. Sci. Med. Sport 2012, 15, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, F.M.; Rampinini, E.; Coutts, A.J.; Sassi, A.; Marcora, S.M. Use of RPE-based training load in soccer. Med. Sci. Sports Exerc. 2004, 36, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.J.; Hoffman, M.D.; Stellingwerff, T. Considerations for ultra-endurance activities: Part 1- nutrition. Res. Sports Med. 2019, 27, 166–181. [Google Scholar] [CrossRef]
- Bishop, P.A.; Jones, E.; Woods, A.K. Recovery from training: A brief review: Brief review. J. Strength Cond. Res. 2008, 22, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A. Using recovery modalities between training sessions in elite athletes. Sports Med. 2006, 36, 781–796. [Google Scholar] [CrossRef]
- Minett, G.M.; Duffield, R. Is recovery driven by central or peripheral factors? A role for the brain in recovery following intermittent-sprint exercise. Front. Physiol. 2014, 5, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harty, P.S.; Cottet, M.L.; Malloy, J.K.; Kerksick, C.M. Nutritional and supplementation strategies to prevent and attenuate exercise-induced muscle damage: A brief review. Sports Med. Open 2019, 5, 1–17. [Google Scholar] [CrossRef]
- Owens, D.J.; Twist, C.; Cobley, J.N.; Howatson, G.; Close, G.L. Exercise-induced muscle damage: What is it, what causes it and what are the nutritional solutions? Eur. J. Sport Sci. 2019, 19, 71–85. [Google Scholar] [CrossRef] [PubMed]
- Erlacher, D.; Ehrlenspiel, F.; Adegbesan, O.A.; El-Din, H.G. Sleep habits in German athletes before important competitions or games. J. Sports Sci. 2011, 29, 859–866. [Google Scholar] [CrossRef]
- Tuomilehto, H.; Vuorinen, V.P.; Penttilä, E.; Kivimäki, M.; Vuorenmaa, M.; Venojärvi, M.; Airaksinen, O.; Pihlajamäki, J. Sleep of professional athletes: Underexploited potential to improve health and performance. J. Sports Sci. 2016, 35, 704–710. [Google Scholar] [CrossRef]
- Leeder, J.; Glaister, M.; Pizzoferro, K.; Dawson, J.; Pedlar, C. Sleep duration and quality in elite athletes measured using wristwatch actigraphy. J. Sports Sci. 2012, 30, 541–545. [Google Scholar] [CrossRef]
- Chennaoui, M.; Léger, D.; Gomez-Merino, D. Sleep and the GH/IGF-1 axis: Consequences and countermeasures of sleep loss/disorders. Sleep Med. Rev. 2020, 49, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Juliff, L.E.; Halson, S.L.; Peiffer, J.J. Understanding sleep disturbance in athletes prior to important competitions. J. Sci. Med. Sport 2015, 18, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Lastella, M.; Roach, G.D.; Halson, S.L.; Martin, D.T.; West, N.P.; Sargent, C. Sleep/wake behaviour of endurance cyclists before and during competition. J. Sports Sci. 2015, 33, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Frank, M.G. The mystery of sleep function: Current perspectives and future directions. Rev. Neurosci. 2006, 17, 375–392. [Google Scholar] [CrossRef]
- Halson, S.L. Sleep Monitoring in Athletes: Motivation, methods, miscalculations and why it matters. Sports Med. 2019, 49, 1487–1497. [Google Scholar] [CrossRef] [PubMed]
- Biggins, M.; Purtill, H.; Fowler, P.; Bender, A.; Sullivan, K.O.; Samuels, C.; Cahalan, R. Sleep in elite multi-sport athletes: Implications for athlete health and wellbeing. Phys. Ther. Sport 2019, 39, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Lastella, M.; Vincent, G.E.; Duffield, R.; Roach, G.D.; Halson, S.L.; Heales, L.J.; Sargent, C. Can sleep be used as an indicator of overreaching and overtraining in athletes? Front. Physiol. 2018, 9, 436–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnar, D.; Bartel, K.; Kakoschke, N.; Lang, C. Sleep interventions designed to improve athletic performance and recovery: A systematic review of current approaches. Sports Med. 2018, 48, 683–703. [Google Scholar] [CrossRef]
- Watson, A.M. Sleep and athletic performance. Curr. Sports Med. Rep. 2017, 16, 413–418. [Google Scholar] [CrossRef]
- Gupta, L.; Morgan, K.; Gilchrist, S. Does elite sport degrade sleep quality? A systematic review. Sports Med. 2017, 47, 1317–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuels, C.; James, L.; Lawson, D.; Meeuwisse, W. The Athlete Sleep Screening Questionnaire: A new tool for assessing and managing sleep in elite athletes. Br. J. Sports Med. 2016, 50, 418–422. [Google Scholar] [CrossRef] [Green Version]
- Irwin, M.R.; Olmstead, R.; Carroll, J.E. Sleep disturbance, sleep duration, and inflammation: A systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol. Psychiatry 2016, 80, 40–52. [Google Scholar] [CrossRef] [Green Version]
- Lastella, M.; Roach, G.D.; Halson, S.L.; Sargent, C. The Chronotype of Elite Athletes. J. Hum. Kinet. 2016, 54, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Von Rosen, P.; Frohm, A.; Kottorp, A.; Friden, C.; Heijne, A. Too little sleep and an unhealthy diet could increase the risk of sustaining a new injury in adolescent elite athletes. Scand. J. Med. Sci. Sports 2016, 27, 1364–1371. [Google Scholar] [CrossRef]
- Milewski, M.D.; Skaggs, D.L.; Bishop, G.A.; Pace, J.L.; Ibrahim, D.A.; Wren, T.A.; Barzdukas, A. Chronic lack of sleep is associated with increased sports injuries in adolescent athletes. J. Pediatr. Orthop. 2014, 34, 129–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venter, R.E. Perceptions of team athletes on the importance of recovery modalities. Eur. J. Sport Sci. 2014, 14, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Halson, S.L. Monitoring fatigue and recovery. Sports Med. 2014, 44, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peukhuri, K.; Sihvola, N.; Korpela, R. Diet promotes sleep duration and quality. Nutr. Res. 2012, 32, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Palaniappan, K.; Thenappan, A. Physiological Basis of Alternative Therapies to Alleviate Sleep Disturbances. J. Sleep Disord. Ther. 2015, 5, 221–227. [Google Scholar]
- Ohayon, M.; Wickwire, E.M.; Hirshkowitz, M.; Albert, S.M.; Avidan, A.; Daly, F.J.; Dauvilliers, Y.; Ferri, R.; Fung, C.; Gozal, D.; et al. National Sleep Foundation’s sleep quality recommendations: First report. Sleep Health 2017, 3, 6–19. [Google Scholar] [CrossRef] [Green Version]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef]
- Bird, S.P. Sleep, recovery, and athletic performance: A brief review and recommendations. J. Strength Cond. 2013, 35, 43–47. [Google Scholar] [CrossRef]
- Walsh, N.P.; Halson, S.L.; Sargent, C.; Roach, G.D.; Nédélec, M.; Gupta, L.; Leeder, J.; Fullagar, H.H.; Coutts, A.J.; Edwards, B.J.; et al. Sleep and the athlete: Narrative review and 2021 expert consensus recommendations. Br. J. Sports Med. 2021, 55, 358–368. [Google Scholar] [CrossRef]
- Roberts, S.S.H.; Teo, W.-P.; Warmington, S.A. Effcets of training and competition on the sleep of elite athletes: A systemativ review and meta-analysis. Br. J. Sports Med. 2019, 22, 23–36. [Google Scholar]
- Schaal, K.; Tafflet, M.; Nassif, H.; Thibault, V.; Pichard, C.; Alcotte, M.; Guillet, T.; El Helou, N.; Berthelot, G.; Simon, S.; et al. Psychological balance in high level athletes: Gender-based differences and sport-specific patterns. PLoS ONE 2011, 6, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swinbourne, R.; Gill, N.; Vaile, J.; Smart, D. Prevalence of poor sleep quality, sleepiness and obstructive sleep apnoea risk factors in athletes. Eur. J. Sport Sci. 2016, 16, 850–858. [Google Scholar] [CrossRef]
- Sargent, C.; Halson, S.; Roach, G.D. Sleep or swim? Early-morning training severely restricts the amount of sleep obtained by elite swimmers. Eur. J. Sport Sci. 2014, 14, 310–315. [Google Scholar] [CrossRef]
- Samuels, C. Sleep, recovery, and performance: The new frontier in high-performance athletics. Phys. Med. Rehabil. Clin. N. Am. 2008, 20, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Fischer, F.M.; Nagai, R.; Teixeira, L.R. Explaining Sleep Duration in Adolescents: The Impact of Socio-Demographic and Lifestyle Factors and Working Status. Chronobiol. Int. 2008, 25, 359–372. [Google Scholar] [CrossRef] [PubMed]
- Medic, G.; Wille, M.; Hemels, M.E. Short-and long-term health consequences of sleep disruption. Nat. Sci. Sleep 2017, 9, 15–161. [Google Scholar] [CrossRef] [Green Version]
- Yegneswaran, B.; Shapiro, C. Do sleep deprivation and alcohol have the same effects on psychomotor performance? J. Psychosom. Res. 2007, 63, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Fullagar, H.H.; Skorski, S.; Duffield, R.; Hammes, D.; Coutts, A.J.; Meyer, T. Sleep and athletic performance: The effects of sleep loss on exercise performance, and physiological and cognitive responses to exercise. Sports Med. 2015, 45, 161–186. [Google Scholar]
- Sateia, M.J. International classification of sleep disorders. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Adams, R.; Appleton, S.; Taylor, A.; McEvoy, D.; Antic, N. Report to the Sleep Health Foundation 2016 Sleep Health Survey of Australian Adults. Sleep Health Foundation. Available online: https://www.sleephealthfoundation.org.au/pdfs/surveys/SleepHealthFoundation-Survey.pdf (accessed on 4 August 2020).
- Thorpy, M. International classification of sleep disorders. In Sleep Disorders Medicine; Springer: New York, NY, USA, 2017; pp. 475–484. [Google Scholar]
- Marra, S.; Arnaldi, D.; Nobili, L. The pharmacotherapeutic management of obstructive sleep apnea. Expert Opin. Pharmacother. 2019, 20, 1981–1991. [Google Scholar] [CrossRef] [PubMed]
- Dunican, I.C.; Walsh, J.; Higgins, C.C.; Jones, M.J.; Maddison, K.; Caldwell, J.A.; David, H.; Eastwood, P.R. Prevalence of sleep disorders and sleep problems in an elite super rugby union team. J. Sports Sci. 2019, 37, 950–957. [Google Scholar] [CrossRef]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Dolenc Groselj, L.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef]
- Vaughn, B.V.; O’Neill, F.C. Cardinal manifestations of sleep disorders. In Principles and Practice of Sleep Medicine, 5th ed.; Kryger, M.H., Roth, R., Dement, W.C., Eds.; Elsevier: Philadelphia, PA, USA, 2011; pp. 594–601. [Google Scholar]
- Buysse, D.J. Sleep health: Can we define it? Does it matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Carney, C.E.; Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Krystal, A.D.; Lichstein, K.L.; Morin, C.M. The consensus sleep diary: Standardizing prospective sleep self-monitoring. Sleep 2012, 35, 287–302. [Google Scholar] [CrossRef] [Green Version]
- Irwin, M.R.; Opp, M.R. Sleep health: Reciprocal regulation of sleep and innate immunity. Neuropsychopharmacology 2017, 42, 129–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quante, M.; Kaplan, E.R.; Rueschman, M.; Cailler, M.; Buxton, O.M.; Redline, S. Practical considerations in using accelerometers to assess physical activity, sedentary behavior, and sleep. Sleep Health 2015, 1, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Kolla, B.P.; Mansukhani, S.; Mansukhani, M.P. Consumer sleep tracking devices: A review of mechanisms, validity and utility. Expert Rev. Med. Devices 2016, 13, 497–506. [Google Scholar] [CrossRef]
- Sedah, A. The role and validity of actigraphy in sleep medicine: An update. Sleep Med. Rev. 2011, 15, 259–267. [Google Scholar]
- Ancoli-Isreal, S.; Cole, R.; Alessi, C.; Chambers, M.; Moorcroft, W.; Pollock, C.P. The role of actigraphy in the study of sleep and circadian rhythmns. Sleep 2003, 26, 342–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Meur, Y.; Pichon, A.; Schaal, K.; Schmitt, L.; Louis, J.; Gueneron, J.; Vidal, P.P.; Hausswirth, C. Evidence of parasympathetic hyperactivity in functionally overreached athletes. Med. Sci. Sports Exerc. 2013, 45, 2061–2071. [Google Scholar] [CrossRef] [PubMed]
- Johnston, R.; Cahalan, R.; Bonnett, L.; Maguire, M.; Glasgow, P.; Madigan, S.; O’Sullivan, K.; Comyns, T. General health complaints and sleep associated with new injury within an endurance sporting population: A prospective study. J. Sci. Med. Sport 2020, 23, 252–257. [Google Scholar] [CrossRef]
- Bishop, D.J. The effects of travel on team performance in the Australian national netball competition. J. Sci. Med. Sport 2004, 7, 118–122. [Google Scholar] [CrossRef]
- Richmond, L.K.; Dawson, B.; Stewart, G.; Cormack, S.; Hillman, D.R.; Eastwood, P.R. The effect of interstate travel on the sleep patterns and performance of elite Australian Rules footballers. J. Sci. Med. Sport 2007, 10, 252–258. [Google Scholar] [CrossRef]
- Fowler, P.; Duffield, R.; Vaile, J. Effects of domestic air travel on technical and tactical performance and recovery in soccer. Int. J. Sports Physiol. Perform. 2014, 9, 378–386. [Google Scholar] [CrossRef]
- Froy, O. The relationship between nutrition and circadian rhythms in mammals. Front. Neuroendocrinol. 2007, 28, 61–71. [Google Scholar] [CrossRef]
- Saper, C.B.; Scammell, T.E.; Lu, J. Hypothalamic regulation of sleep and circadian rhythms. Nature 2005, 437, 1257–1263. [Google Scholar] [CrossRef]
- Jeukendrup, A.E. Periodized Nutrition for Athletes. Sports Med. 2017, 47, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heaton, L.E.; Davis, J.K.; Rawson, E.S.; Nuccio, R.P.; Witard, O.C.; Stein, K.W.; Baar, K.; Carter, J.M.; Baker, L.B. Selected In-Season Nutritional Strategies to Enhance Recovery for Team Sport Athletes: A Practical Overview. Sports Med. 2017, 47, 2201–2218. [Google Scholar] [CrossRef] [PubMed]
- Close, G.L.; Hamilton, D.L.; Philip, A.; Burke, L.M.; Morton, J.P. New strategies in sport nutrition to increase exercise performance. Free Radic. Biol. Med. 2016, 98, 144–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swann, C.; Moran, A.; Piggott, D. Defining elite athletes: Issues in the study of expert performance in sport psychology. Psychol. Sport Exerc. 2015, 16, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Davies, M.A.; Judge, A.D.; Delmestri, A.; Kemp, S.P.; Stokes, K.A.; Arden, N.K.; Newton, J.L. Health amongst former rugby union players: A cross-sectional study of morbidity and health-related quality of life. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Johns, M.W. Daytime sleepiness, snoring, and obstructive sleep apnoea: The Epworth Sleepiness Scale. Chest 1993, 103, 30–36. [Google Scholar] [CrossRef]
- Kryger, M.H.; Roth, T.; Dement, W.C. Principles and Practice of Sleep Medicine, 5th ed.; Elsevier Saunders: St. Louis, MO, USA, 2011. [Google Scholar]
- Kellmann, M.; Kallus, K.W. Recovery-Stress Questionnaire for Athletes: User Manual; Human Kinetics: Champaign, IL, USA, 2001. [Google Scholar]
- Horne, J.A.; Östberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1975, 4, 97–110. [Google Scholar]
- Bender, A.M.; Van Dongen, H.; Samuels, C.H. Sleep Quality and Chronotype Differences between Elite Athletes and Non-Athlete Controls. Clocks Sleep 2019, 1, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maich, K.H.; Lachowski, A.M.; Carney, C.E. Psychometric Properties of the Consensus Sleep Diary in Those with Insomnia Disorder. Behav. Sleep Med. 2016, 5, 1–18. [Google Scholar] [CrossRef]
- Thomas, J.R.; Silverman, S.; Nelson, J. Research Methods in Physical Activity, 7th ed.; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Knufinke, M.; Nieuwenhuys, A.; Geurts, S.A.; Møst, E.I.; Maase, K.; Moen, M.H.; Coenen, A.M.; Kompier, M.A. Train hard, sleep well? Perceived training load, sleep quantity and sleep stage distribution in elite level athletes. J. Sci. Med. Sport 2018, 21, 427–432. [Google Scholar] [CrossRef]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–Retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Spira, A.P.; Beaudreau, S.A.; Stone, K.L.; Kezirian, E.J.; Lui, L.Y.; Redline, S.; Ancoli-Israel, S.; Ensrud, K.; Stewart, A. Reliability and validity of the Pittsburgh Sleep Quality Index and the Epworth Sleepiness Scale in older men. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 67, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Glaesmer, H.; Brähler, E.; Löffler, M.; Engel, C.; Enzenbach, C.; Hegerl, U.; Sander, C. Sleep quality in the general population: Psychometric properties of the Pittsburgh Sleep Quality Index, derived from a German community sample of 9284 people. Sleep Med. 2017, 30, 57–63. [Google Scholar] [CrossRef]
- Mah, C.D.; Kezirian, E.J.; Marcello, B.M.; Dement, W.C. Poor sleep quality and insufficient sleep of a collegiate student-athlete population. Sleep Health 2018, 4, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Elbayoumy, A.; Elbayoumy, A. Relationship of sleep quality and competitive anxiety in a sample of swimming athletes. Swed. J. Sci. Res. 2015, 2, 38–43. [Google Scholar]
- Jarraya, S.; Jarraya, M.; Chtourou, H.; Souissi, N. Effect of time of day and partial sleep deprivation on the reaction time and the attentional capacities of the handball goalkeeper. Biol. Rhythm Res. 2014, 45, 183–191. [Google Scholar] [CrossRef]
- Reyner, L.A.; Horne, J.A. Sleep restriction and serving accuracy in performance tennis players, and effects of caffeine. Physiol. Behav. 2013, 120, 93–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, B.J.; Waterhouse, J. Effects of one night of partial sleep deprivation upon diurnal rhythms of accuracy and consistency in throwing darts. Chronobiol. Int. 2009, 26, 756–768. [Google Scholar] [CrossRef]
- Caia, J.; Thornton, H.R.; Kelly, V.G.; Scott, T.J.; Halson, S.L.; Cupples, B.; Driller, M.W. Does self-perceived sleep reflect sleep estimated via activity monitors in professional rugby league athletes? J. Sports Sci. 2018, 36, 1492–1496. [Google Scholar] [CrossRef]
- Dunican, I.C.; Martin, D.T.; Halson, S.L.; Reale, R.J.; Dawson, B.T.; Caldwell, J.A.; Jones, M.J.; Eastwood, P.R. The effects of the removal of electronic devices for 48 h on sleep in elite judo athletes. J. Strength Cond. Res. 2017, 31, 2832–2839. [Google Scholar] [CrossRef]
- Vlahoyiannis, A.; Aphamis, G.; Bogdanis, G.C.; Sakkas, G.K.; Andreou, E.; Giannaki, C.D. Deconstructing athletes’ sleep: A systematic review of the influence of age, sex, athletic expertise, sport type, and season on sleep characteristics. J. Sport Health Sci. 2020, in press. [Google Scholar] [CrossRef]
- Hagenauer, M.H.; Crodelle, J.A.; Piltz, S.H.; Toporikova, N.; Ferguson, P.; Booth, V. The modulation of pain by circadian and sleep-dependent processes: A review of the experimental evidence. Biology 2017, 17, 1–19. [Google Scholar]
- Hausswirth, C.; Louis, J.; Aubry, A.; Bonnet, G.; Duffield, R.; Le Meur, Y. Evidence of disturbed sleep and increased illness in overreached endurance athletes. Med. Sci. Sports Exerc. 2014, 46, 1036–1045. [Google Scholar] [CrossRef]
- Mah, C.D.; Mah, K.E.; Kezirian, E.J.; Dement, W.C. The effects of sleep extension on the athletic performance of collegiate basketball players. Sleep 2011, 34, 943–950. [Google Scholar] [CrossRef]
- Simpson, N.S.; Gibbs, E.L.; Matheson, G.O. Optimizing sleep to maximize performance: Implications and recommendations for elite athletes. Scand. J. Med. Sci. Sports 2017, 27, 266–274. [Google Scholar] [CrossRef]
- Merdad, R.A.; Merdad, L.A.; Nassif, R.A.; El-Derwi, D.; Wali, S.O. Sleep habits in adolescents of Saudi Arabia; distinct patterns and extreme sleep schedules. Sleep Med. 2014, 15, 1370–1378. [Google Scholar] [CrossRef]
- Pires, G.N.; Bezerra, A.G.; Tufik, S.; Andersen, M.L. Effects of acute sleep deprivation on state anxiety levels: A systematic review and meta-analysis. Sleep Med. 2016, 24, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Dinges, D.F.; Pack, F.; Williams, K.; Gillen, K.A.; Powell, J.W.; Ott, G.E.; Aptowicz, C.; Pack, A.I. Cumulative sleepiness, mood disturbance, and psychomotor vigilance performance decrements during a week of sleep restricted to 4–5 h per night. Sleep 1997, 20, 267–277. [Google Scholar]
- Shearer, D.A.; Jones, R.M.; Kilduff, L.P.; Cook, C.J. Effects of competition on the sleep patterns of elite rugby union players. Eur. J. Sport Sci. 2015, 15, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Ortuño, M.M.; Edinger, J.D.; Means, M.K.; Almirall, D. Home is where sleep is: An ecological approach to test the validity of actigraphy for the assessment of insomnia. J. Clin. Sleep Med. 2010, 6, 21–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antic, N.A.; Weeks, R.; McEvoy, D.; Sargent, C.; Jarema, L.; Okeefe, M.; Catcheside, P. Prevalence of sleep disorders and excessive daytime sleepiness in an elite Australian Rules football team. Am. J. Respir. Crit. Care Med. 2013, 187, 3455. [Google Scholar]
- George, C.F.; Kab, V.; Kab, P.; Villa, J.J.; Levy, A.M. Sleep and breathing in professional football players. Sleep Med. 2003, 4, 317–325. [Google Scholar] [CrossRef]
- Silva, A.; Queiroz, S.S.; Winckler, C.; Vital, R.; Sousa, R.A.; Fagundes, V.; Tufik, S.; de Mello, M.T. Sleep quality evaluation, chronotype, sleepiness and anxiety of Paralympic Brazilian athletes: Beijing 2008 Paralympic Games. Br. J. Sports Med. 2012, 46, 150–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caia, J.; Halson, S.L.; Scott, A.; Kelly, V.G. Obstructive sleep apnea in professional rugby league athletes: An exploratory study. J. Sci. Med. Sport 2020, 23, 1011–1015. [Google Scholar] [CrossRef]
- Rice, T.B.; Dunn, R.E.; Lincoln, A.E.; Tucker, A.M.; Vogel, R.A.; Heyer, R.A.; Yates, A.P.; Wilson, P.W.; Pellmen, E.J.; Allen, T.W.; et al. Sleep-disordered breathing in the National Football League. Sleep 2010, 33, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Vitale, J.A.; Bonato, M.; Galasso, L.; La Torre, A.; Merati, G.; Montaruli, A.; Roveda, E.; Carandente, F. Sleep quality and high intensity interval training at two different times of day: A crossover study on the influence of the chronotype in male collegiate soccer players. Chronobiol. Int. 2017, 34, 260–268. [Google Scholar] [CrossRef]
- Skein, M.; Duffield, R.; Minnett, G.M.; Snape, A.; Murphy, A. The effect of overnight sleep deprivation after competitive rugby league matches on postmatch physiological and perceptual recovery. Int. J. Sports Physiol. Perform. 2013, 8, 556–564. [Google Scholar] [CrossRef]
- Frank, R.; Nixdorf, I.; Beckmann, J. Stress, underrecovery, and health problems in athletes. In Sport, Recovery and Performance: Interdisciplinary Insights; Kellmann, M., Beckmann, J., Eds.; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Kellmann, M. Preventing overtraining in athletes in high intensity sports and stress/recovery monitoring. Scand. J. Med. Sci. Sport 2010, 20, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Vaske, J.J.; Beaman, J.; Sponarski, C.C. Rethinking internal consistency in Cronbach’s alpha. Leis. Sci. 2017, 39, 163–173. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L. Starting at the beginning: An introduction to coefficient alpha and internal consistency. J. Personal. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Timpka, T.; Jacobsson, J.; Bargoria, V.; Dahlström, Ö. Injury Pain in Track and Field Athletes: Cross-Sectional Study of Mediating Factors. Sports 2019, 7, 110. [Google Scholar] [CrossRef] [Green Version]
- Roehrs, T.; Timms, V.; Zwyghuizen-Doorenbos, A.; Roth, T. Sleep extension in sleepy and alert normals. Sleep 1989, 12, 449–457. [Google Scholar] [CrossRef]
- Pettersen, S.D.; Aslaksen, P.M.; Pettersen, S.A. Pain Processing in Elite and High-Level Athletes Compared to Non-athletes. Front. Psychol. 2020, 11, 1908–1916. [Google Scholar] [CrossRef] [PubMed]
- Laux, P.; Krumm, B.; Diers, M.; Flor, H. Recovery–Stress balance and injury risk in professional football players: A prospective study. J. Sports Sci. 2015, 33, 2140–2148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tibbert, S.; Morris, T.; Andersen, M. Validity of the recovery-stress questionnaire. J. Sci. Med. Sport 2009, 12 (Suppl. S), S32–S33. [Google Scholar] [CrossRef]
- Keaney, L.C.; Kilding, A.E.; Merien, F.; Dulson, D.K. Keeping Athletes Healthy at the 2020 Tokyo Summer Games: Considerations and Illness Prevention Strategies. Front. Physiol. 2019, 10, 426–434. [Google Scholar] [CrossRef]
- Schwellnus, M.; Soligard, T.; Alonso, J.M.; Bahr, R.; Clarsen, B.; Dijkstra, H.P.; Gabbett, T.J.; Gleeson, M.; Hägglund, M.; Hutchinson, M.R.; et al. How much is too much? (Part 2) International Olympic Committee consensus statement on load in sport and risk of illness. Br. J. Sports Med. 2016, 50, 1043–1052. [Google Scholar] [CrossRef] [Green Version]
- Soligard, T.; Schwellnus, M.; Alonso, J.M.; Bahr, R.; Clarsen, B.; Dijkstra, H.P.; Gabbett, T.; Gleeson, M.; Hägglund, M.; Hutchinson, M.R.; et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br. J. Sports Med. 2016, 50, 1030–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivarsson, A.; Johnson, U.; Andersen, M.B.; Tranaeus, U.; Stenling, A.; Lindwall, M. Psychosocial factors and sport injuries: Meta-analyses for prediction and prevention. Sports Med. 2017, 47, 353–365. [Google Scholar] [CrossRef]
- Meeusen, R.; Duclos, M.; Foster, C.; Fry, A.; Gleeson, M.; Nieman, D.; Raglin, J.; Rietjens, G.; Steinacker, J.; Urhausen, A. Prevention, diagnosis, and treatment of the overtraining syndrome: Joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med. Sci. Sports Exerc. 2013, 45, 186–205. [Google Scholar] [CrossRef] [Green Version]
- Wardenaar, F.C.; Ceelen, I.J.; Van Dijk, J.W.; Hangelbroek, R.W.; Van Roy, L.; Van der Pouw, B.; De Vries, J.H.; Mensink, M.; Witkamp, R.F. Nutritional supplement use by Dutch elite and sub-elite athletes: Does receiving dietary counseling make a difference? Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 32–42. [Google Scholar] [CrossRef]
- Knapik, J.J.; Steelman, R.A.; Hoedebecke, S.S.; Austin, K.G.; Farina, E.K.; Lieberman, H.R. Prevalence of dietary supplement use by athletes: Systematic review and meta-analysis. Sports Med. 2016, 46, 103–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snijders, T.; Trommelen, J.; Kouw, I.W.; Holwerda, A.M.; Verdijk, L.B.; Van Loon, L.J. The impact of pre-sleep protein ingestion on the skeletal muscle adaptive response to exercise in humans: An update. Front. Nutr. 2019, 6, 17. [Google Scholar] [CrossRef] [Green Version]
- Falkenberg, E.; Aisbett, B.; Lastella, M.; Roberts, S.; Condo, D. Nutrient intake, meal timing and sleep in elite male Australian football players. J. Sci. Med. Sport 2021, 24, 7–12. [Google Scholar] [CrossRef]
- Foster, R.G. Sleep, circadian rhythms and health. Interface Focus 2020, 10, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Del Coso, J.; Muñoz, G.; Muñoz-Guerra, J. Prevalence of caffeine use in elite athletes following its removal from the World Anti-Doping Agency list of banned substances. Appl. Physiol. Nutr. Metab. 2011, 36, 555–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Thuyne, W.; Roels, K.; Delbeke, F.T. Distribution of caffeine levels in urine in different sports in relation to doping control. Int. J. Sports Med. 2005, 26, 714–718. [Google Scholar] [CrossRef]
- Desbrow, B.; Leveritt, M. Awareness and use of caffeine by athletes competing at the 2005 Ironman Triathlon World Championships. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 545–558. [Google Scholar] [CrossRef]
- Beaumont, R.; Cordery, P.; Funnell, M.; Mears, S.; James, L.; Watson, P. Chronic ingestion of a low dose of caffeine induces tolerance to the performance benefits of caffeine. J. Sports Sci. 2017, 35, 1920–1927. [Google Scholar] [CrossRef]
- Pickering, C.; Kiely, J. What should we do about habitual caffeine use in athletes? Sports Med. 2019, 49, 833–842. [Google Scholar] [CrossRef] [Green Version]
- Miller, B.; O’Connor, H.; Orr, R.; Ruell, P.; Cheng, H.L.; Chow, C.M. Combined caffeine and carbohydrate ingestion: Effects on nocturnal sleep and exercise performance in athletes. Eur. J. Appl. Physiol. 2014, 114, 2529–2537. [Google Scholar] [CrossRef] [PubMed]
- Dunican, I.C.; Higgins, C.C.; Jones, M.J.; Clarke, M.W.; Murray, K.; Dawson, B.; Caldwell, J.A.; Halson, S.L.; Eastwood, P.R. Caffeine use in a super rugby game and its relationship to post-game sleep. Eur. J. Sport Sci. 2018, 18, 513–523. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, C.P.; Lyons, F. Alcohol and the athlete. Sports Med. 2000, 29, 295–300. [Google Scholar] [CrossRef]
- Barnes, M.J. Alcohol: Impact on sports performance and recovery in male athletes. Sports Med. 2014, 44, 909–919. [Google Scholar] [CrossRef] [PubMed]
- Roehrs, T.; Roth, T. Sleep, sleepiness, and alcohol use. Alcohol Res. Health 2001, 25, 101–109. [Google Scholar] [PubMed]
- Anderson, K.N. Insomnia and cognitive behavioural therapy-how to assess your patient and why it should be a standard part of care. J. Thorac. Dis. 2018, 10, 94–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchheit, M.; Racinais, S.; Bilsborough, J.C.; Bourdon, P.C.; Voss, S.C.; Hocking, J.; Cordy, J.; Mendez-Villanueva, A.; Coutts, A.J. Monitoring fitness, fatigue and running performance during a pre-season training camp in elite football players. J. Sci. Med. Sport 2013, 16, 550–555. [Google Scholar] [CrossRef]
- Saw, A.E.; Main, L.C.; Gastin, P.B. Monitoring athletes through self-report: Factors influencing implementation. J. Sports Sci. Med. 2015, 14, 137. [Google Scholar]
- Krystal, A.D.; Edinger, J.D. Measuring sleep quality. Sleep Med. 2008, 9, 10–17. [Google Scholar] [CrossRef]
- Heidari, J.; Kölling, S.; Pelka, M.; Kellmann, M. Monitoring the recovery-stress state in athletes. In Sport, Recovery and Performance: Interdisciplinary Insights; Kellmann, M., Beckmann, J., Eds.; Routledge: Abingdon, UK, 2018; pp. 3–18. [Google Scholar]
- McNair, P.M.; Lorr, M.; Droppleman, L.F. POMS Manual, 2nd ed.; Educational and Industrial Testing Service: San Diego, CA, USA, 1981. [Google Scholar]
- Shell, S.J.; Slattery, K.; Clark, B.; Broatch, J.R.; Halson, S.; Kellmann, M.; Coutts, A.J. Perceptions and use of recovery strategies: Do swimmers and coaches believe they are effective? J. Sports Sci. 2020, 38, 2092–2099. [Google Scholar] [CrossRef]


{kind=link}
| All (n = 338) | Elite (n = 115) | Sub-Elite (n = 223) | t/x2 Value | |
|---|---|---|---|---|
| Gender | Male n = 203; Female n = 135 | Male n = 74; Female n = 41 | Male n = 129; Female n = 94 | X 2 = 1.72 |
| Age * | 24.94 ± 5.93 | 23.44 ± 4.91 | 25.71 ± 6.27 | t = 3.384 |
| Body mass (kg) | 72.95 ± 13.26 | 73.95 ± 12.55 | 72.44 ± 13.61 | t = −0.995 |
| Height (cm) | 175.60 ± 9.70 | 176.6 ± 8.78 | 175.08 ± 10.12 | t = −1.361 |
| Training (mins·wk) * | 675.12 ± 306.59 | 801.35 ± 338.81 | 610.02 ± 266.90 | t = −5.682 |
| Sport | All | Elite n = 115 | Sub-Elite n = 223 |
|---|---|---|---|
| Athletics | 64 | 10 | 54 |
| Boxing | 12 | 11 | 1 |
| Gaelic games | 89 | 26 | 63 |
| Hockey | 10 | 9 | 1 |
| Rowing | 29 | 8 | 21 |
| Rugby | 20 | 8 | 12 |
| Sailing | 4 | 3 | 1 |
| Soccer | 31 | 10 | 21 |
| Swimming | 8 | 4 | 4 |
| Other | 71 | 26 | 45 |
| None | Slight | Moderate | Severe | Extreme | ||
|---|---|---|---|---|---|---|
| Mobility | Elite | 96 | 14 | 5 | ||
| Sub-elite | 177 | 42 | 2 | 1 | 1 | |
| Self-care | Elite | 113 | 1 | 1 | ||
| Sub-elite | 214 | 7 | 2 | |||
| Usual activities | Elite | 92 | 18 | 3 | 1 | 1 |
| Sub-elite | 182 | 33 | 8 | |||
| Pain | Elite | 62 | 47 | 6 | ||
| Sub-elite | 107 | 102 | 14 | |||
| Anxiety/Depression | Elite | 72 | 33 | 8 | 2 | |
| Sub-elite | 150 | 58 | 13 | 2 |
| Not during the Last Month | Less than Once per Week | Once or Twice per Week | Three or More Times per Week | ||
|---|---|---|---|---|---|
| Cannot get to sleep within 30 min | Elite Sub-elite | 40 99 | 24 56 | 27 82 | 34 48 |
| Wake up in the middle of the night or early morning | Elite Sub-elite | 30 37 | 24 56 | 27 82 | 34 48 |
| Have to get up to use the bathroom | Elite Sub-elite | 38 63 | 24 76 | 29 44 | 24 40 |
| Cannot breathe comfortably | Elite Sub-elite | 101 192 | 11 16 | 1 10 | 2 5 |
| Cough or snore loudly | Elite Sub-elite | 88 167 | 14 33 | 5 16 | 8 7 |
| Feel too cold | Elite Sub-elite | 79 160 | 27 41 | 7 19 | 2 3 |
| Feel too hot | Elite Sub-elite | 54 82 | 32 77 | 26 54 | 3 10 |
| Have bad dreams | Elite Sub-elite | 63 114 | 34 75 | 16 27 | 2 7 |
| Have pain | Elite Sub-elite | 81 152 | 22 48 | 11 19 | 1 4 |
| Other reasons | Elite Sub-elite | 101 180 | 9 27 | 3 9 | 2 7 |
| Problems staying awake | Elite Sub-elite | 66 125 | 29 66 | 13 27 | 7 5 |
| Lack of enthusiasm | Elite Sub-elite | 35 50 | 29 81 | 37 69 | 14 23 |
| Use of sleep medication | Elite Sub-elite | 104 189 | 5 18 | 3 7 | 3 9 |
| Classification (ESS Score) | Elite (n = 115) | Sub-Elite (n = 223) |
|---|---|---|
| Low Normal (0–5) | 53 | 114 |
| Higher Normal (6–10) | 45 | 70 |
| Mild Excessive (11–12) | 6 | 20 |
| Moderate Excessive (13–15) | 8 | 14 |
| Severe (16–24) | 3 | 5 |
| All (n = 338) | Elite (n = 115) | Sub-Elite (n = 223) | T= | p= | |
|---|---|---|---|---|---|
| General Stress | 1.7 ± 1.31 | 1.77 ± 1.39 | 1.67 ± 1.26 | −0.6602 | 0.51 |
| Emotional Stress | 1.95 ± 0.983 | 1.9 ± 0.98 | 1.97 ± 0.99 | 0.6858 | 0.493 |
| Social Stress | 1.85 ± 1.03 | 1.83 ± 1.04 | 1.86 ± 1.02 | 0.2199 | 0.826 |
| Conflicts/Pressure | 2.35 ± 1.24 | 2.24 ± 1.26 | 2.41 ± 1.24 | 1.1382 | 0.256 |
| Fatigue | 2.52 ± 1.32 | 2.46 ± 1.32 | 2.55 ± 1.32 | 0.6125 | 0.541 |
| Lack of Energy | 2 ± 1.06 | 1.95 ± 1.19 | 2.02 ± 1 | 0.5755 | 0.565 |
| Physical Complaints | 1.61 ± 1.22 | 1.59 ± 1.34 | 1.61 ± 1.16 | 0.1638 | 0.87 |
| Success | 2.85 ± 1 | 2.92 ± 1.01 | 2.81 ± 1 | −0.9189 | 0.359 |
| Social Relaxation | 3.3 ± 1.28 | 3.19 ± 1.26 | 3.36 ± 1.29 | 1.1573 | 0.248 |
| Physical Relaxation | 2.53 ± 1.06 | 2.59 ± 1.09 | 2.49 ± 1.04 | −0.8265 | 0.409 |
| General Well-Being | 3.35 ± 1.16 | 3.37 ± 1.22 | 3.35 ± 1.13 | −0.1497 | 0.881 |
| Sleep Quality | 2.81 ± 0.83 | 2.77 ± 0.78 | 2.83 ± 0.85 | 0.6552 | 0.513 |
| Disturbed Breaks | 1.68 ± 0.92 | 1.71 ± 0.91 | 1.67 ± 0.94 | −0.4119 | 0.681 |
| Burnout/Emotional Exhaustion | 1.83 ± 1.13 | 1.87 ± 1.22 | 1.81 ± 1.09 | −0.4695 | 0.639 |
| Fitness/Injury | 2.43 ± 1.12 | 2.32 ± 1.17 | 2.48 ± 1.09 | 1.2827 | 0.2 |
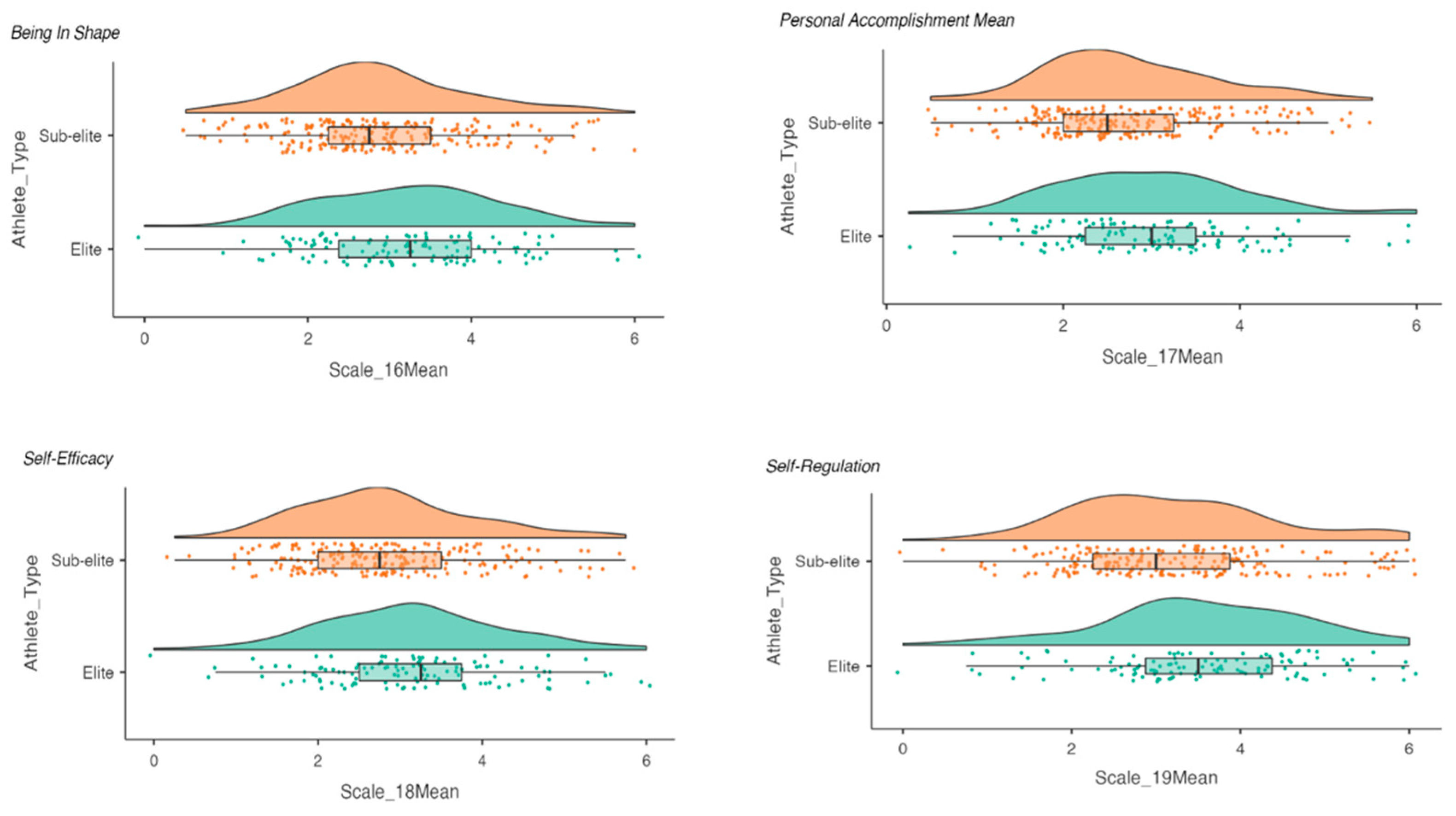
| Fitness/Being in Shape ** | 3.01 ± 1.06 | 3.22 ± 1.08 | 2.9 ± 1.04 | −2.6563 | 0.008 |
| Burnout/Personal Accomplishment * | 2.82 ± 1.01 | 2.97 ± 1.04 | 2.74 ± 0.98 | −1.9984 | 0.048 |
| Self-Efficacy ** | 2.94 ± 1.07 | 3.15 ± 1.12 | 2.83 ± 1.04 | −2.5747 | 0.01 |
| Self-Regulation ** | 3.31 ± 1.2 | 3.55 ± 1.19 | 3.18 ± 1.18 | −2.7121 | 0.007 |
| Chronotype Elite (n =) Sub-elite (n =) | Morning type | More morning type | More evening type | Evening type | |
| 24 45 | 40 84 | 36 65 | 15 29 | ||
| Preferred training time | 6 a.m.–9 a.m. | 9 a.m.–Noon | Noon–3 p.m. | 3 p.m.–6 p.m. | 6 p.m.–9 p.m. |
| Elite (n =) Sub-elite (n =) | 12 26 | 31 75 | 29 47 | 18 41 | 25 34 |
| Preferred competition time * Elite (n =) Sub-elite (n =) | 6 a.m.–9 a.m. 5 12 | 9 a.m.–Noon 21 78 | Noon–3 p.m. 47 62 | 3 p.m.–6 p.m. 21 47 | 6 p.m.–9 p.m. 21 24 |
| Time you usually get tired | 8 p.m.–9:30 p.m. | 9:31 p.m.–10:45 p.m. | 10:46 p.m.–12:30 a.m. | 12:30 a.m.–1:45 a.m. | 1:46 a.m.–3:00 a.m. |
| Elite (n =) Sub-elite (n =) | 27 50 | 51 94 | 26 66 | 3 9 | 8 4 |
| Sleep Measure | Training/Competition Day | Rest Day | |
|---|---|---|---|
| TIB (h) | Elite Sub-elite | 9.1 ± 1.18 9.2 ± 1.42 | 9.53 ± 1.49 9.6 ± 1.5 |
| TST (h) | Elite Sub-elite | 8.01 ± 1.30 * 8.2 ± 1.38 * | 8.58 ± 1.4 8.59 ± 1.44 |
| SL (Min) | Elite Sub-elite | 22.85 ± 20.74 22.65 ± 17.70 | 21.62 ± 18.7 23.72 ± 22.37 |
| NoA (#) | Elite Sub-elite | 1.38 ± 1.43 1.51 ± 1.73 | 1.03 ± 1.17 * 1.52 ± 2.44 * |
| WASO (Min) | Elite Sub-elite | 11.06 ± 17.06 10.14 ± 16.51 | 7.31 ± 9.99 9.56 ± 12.60 |
| SE (%) | Elite Sub-elite | 88.2 ± 10.18 89.77 ± 7.14 | 90.21 ± 6.6 89.1 ± 7.05 |
| Supplement | Frequency | Dose | Reason | Elite (n = 115) | Sub-Elite (n = 223) |
|---|---|---|---|---|---|
| Caffeine | Daily | 100 mg | Performance | 23 | 37 |
| Creatine | Daily | Varied | Performance | 13 | 20 |
| Fish Oil | Daily | 1 capsule | Health | 18 | 12 |
| Iron | Daily | Varied | Anaemia/Performance | 4 | 10 |
| Multivitamin | Daily | 1 capsule | Health | 24 | 32 |
| Nitrate | Daily | 1 shot | Performance | 11 | 1 |
| Probiotics | Daily | 1 capsule | Health | 13 | 25 |
| Vitamin D | Daily | 1000–4000 IU | Health/Performance | 21 | 5 |
| Whey | Daily | 25–40 g | Recovery | 22 | 48 |
| Other (e.g., BCAA, beta—alanine, HMB, casein, antioxidants) | Daily/weekly | Varied | Health/Performance | 30 | 19 |
| Sleep Quality | Disturbed Breaks | Emotional Exhaustion | Being in Shape | Self-Efficacy | |
|---|---|---|---|---|---|
| Supplement Use | −0.167 ** p = 0.002 | 0.119 * p = 0.029 | 0.137 * p = 0.012 | −0.114 * p = 0.036 | −0.108 * p = 0.048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doherty, R.; Madigan, S.M.; Nevill, A.; Warrington, G.; Ellis, J.G. The Sleep and Recovery Practices of Athletes. Nutrients 2021, 13, 1330. https://doi.org/10.3390/nu13041330
Doherty R, Madigan SM, Nevill A, Warrington G, Ellis JG. The Sleep and Recovery Practices of Athletes. Nutrients. 2021; 13(4):1330. https://doi.org/10.3390/nu13041330
Chicago/Turabian StyleDoherty, Rónán, Sharon M. Madigan, Alan Nevill, Giles Warrington, and Jason G. Ellis. 2021. "The Sleep and Recovery Practices of Athletes" Nutrients 13, no. 4: 1330. https://doi.org/10.3390/nu13041330