
Role of Dietary Habits in the Prevention of Diverticular Disease Complications: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Data Extraction
2.3. Quality Assessment
3. Results
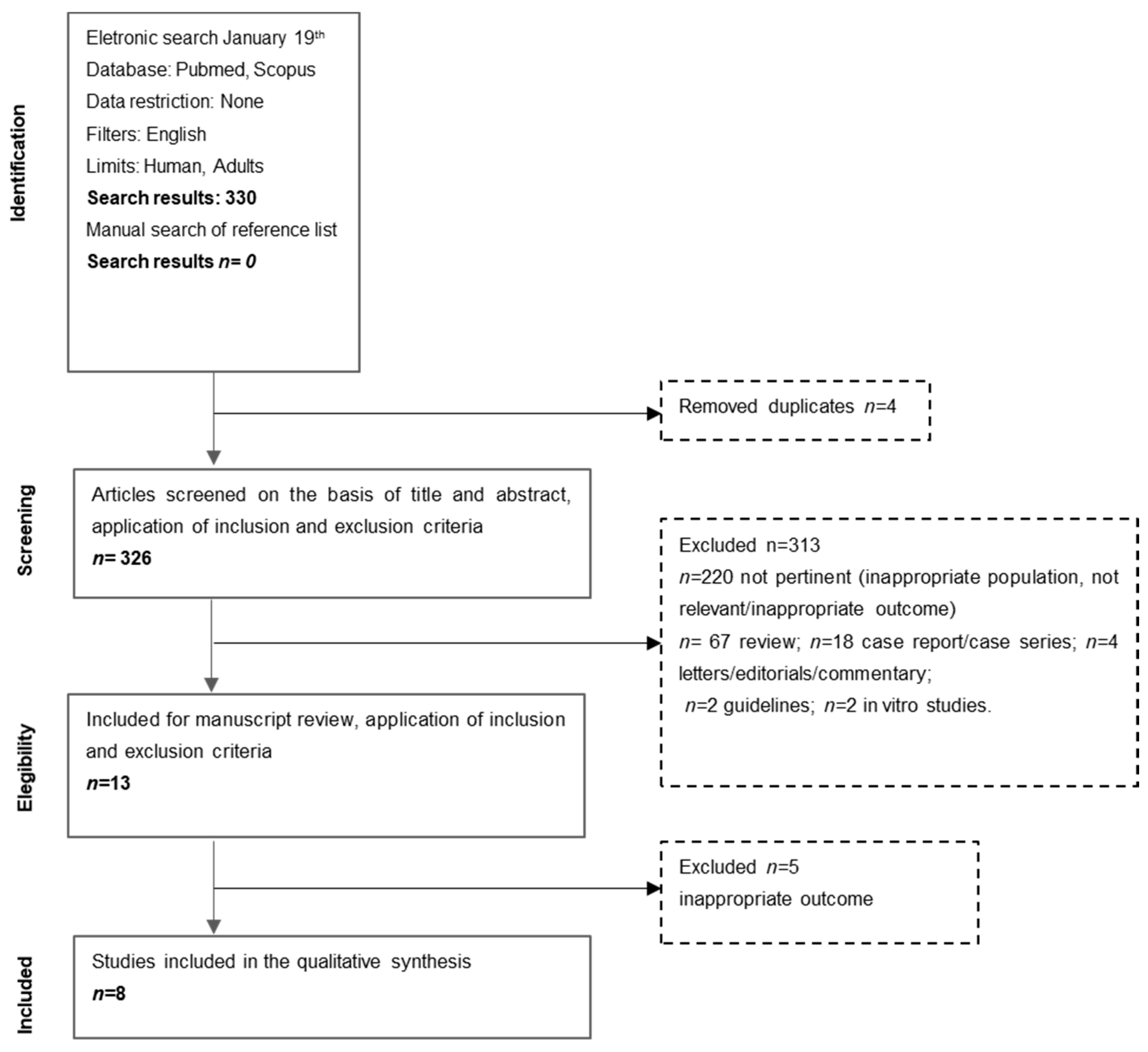
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Dietary Habits
3.3.1. Dietary Fiber and Meat Consumption
3.3.2. Alcohol and Coffee Consumption
3.4. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stollman, N.; Raskin, J.B. Diverticular disease of the colon. Lancet 2004, 363, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Cuomo, R.; Barbara, G.; Pace, F.; Annese, V.; Bassotti, G.; Binda, G.A.; Casetti, T.; Colecchia, A.; Festi, D.; Fiocca, R.; et al. Italian consensus conference for colonic diverticulosis and diverticular disease. United Eur. Gastroenterol. J. 2014, 2, 413–442. [Google Scholar] [CrossRef] [Green Version]
- Strate, L.L.; Modi, R.; Cohen, E.; Spiegel, B.M.R. Diverticular Disease as a Chronic Illness: Evolving Epidemiologic and Clinical Insights. Am. J. Gastroenterol. 2012, 107, 1486–1493. [Google Scholar] [CrossRef]
- Shahedi, K.; Fuller, G.; Bolus, R.; Cohen, E.; Vu, M.; Shah, R.; Agarwal, N.; Kaneshiro, M.; Atia, M.; Sheen, V.; et al. Long-term Risk of Acute Diverticulitis among Patients with Incidental Diverticulosis Found During Colonoscopy. Clin. Gastroenterol. Hepatol. 2013, 11, 1609–1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirocchi, R.; Grassi, V.; Cavaliere, D.; Renzi, C.; Tabola, R.; Poli, G.; Avenia, S.; Farinella, E.; Arezzo, A.; Vettoretto, N.; et al. New Trends in Acute Management of Colonic Diverticular Bleeding. Medicine 2015, 94, e1710. [Google Scholar] [CrossRef] [PubMed]
- Urabe, M.; Nishida, T.; Shimakoshi, H.; Shimoda, A.; Amano, T.; Sugimoto, A.; Takahashi, K.; Mukai, K.; Matsubara, T.; Yamamoto, M.; et al. Distinct Clinical Factors in Hospitalized Patients with Diverticular Bleeding and Diverticulitis. Digestion 2018, 99, 239–246. [Google Scholar] [CrossRef]
- Carabotti, M.; Labate, A.M.M.; Cremon, C.; Cuomo, R.; Pace, F.; Andreozzi, P.; Falangone, F.; Barbara, G.; Annibale, B. Distinguishing features between patients with acute diverticulitis and diverticular bleeding: Results from the REMAD registry. Dig. Liver Dis. 2021, 53, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Strate, L.L. Lifestyle Factors and the Course of Diverticular Disease. Dig. Dis. 2012, 30, 35–45. [Google Scholar] [CrossRef]
- The Definition of Dietary Fiber. Available online: http://www.aaccnet.org/initiatives/definitions/documents/dietaryfiber/dfdef.pdf (accessed on 5 March 2001).
- Slavin, J. Fiber and Prebiotics: Mechanisms and Health Benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef] [Green Version]
- Carabotti, M.; Annibale, B.; Severi, C.; Lahner, E. Role of Fiber in Symptomatic Uncomplicated Diverticular Disease: A Systematic Review. Nutrients 2017, 9, 161. [Google Scholar] [CrossRef] [Green Version]
- Ünlü, C.; Daniels, L.; Vrouenraets, B.C.; Boermeester, M.A. A systematic review of high-fibre dietary therapy in diverticular disease. Int. J. Color. Dis. 2012, 27, 419–427. [Google Scholar] [CrossRef] [Green Version]
- Dahl, C.; Crichton, M.; Jenkins, J.; Nucera, R.; Mahoney, S.; Marx, W.; Marshall, S. Evidence for Dietary Fibre Modification in the Recovery and Prevention of Reoccurrence of Acute, Uncomplicated Diverticulitis: A Systematic Literature Review. Nutrients 2018, 10, 137. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Sen, A.; Norat, T.; Riboli, E. Dietary fibre intake and the risk of diverticular disease: A systematic review and meta-analysis of prospective studies. Eur. J. Nutr. 2019, 59, 421–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aldoori, W.H.; Giovannucci, E.L.; Rimm, E.B.; Wing, A.L.; Trichopoulos, D.V.; Willett, W.C. A prospective study of alcohol, smoking, caffeine, and the risk of symptomatic diverticular disease in men. Ann. Epidemiol. 1995, 5, 221–228. [Google Scholar] [CrossRef]
- Tønnesen, H.; Engholm, G.; Møller, H. Association between alcoholism and diverticulitis. BJS 1999, 86, 1067–1068. [Google Scholar] [CrossRef] [PubMed]
- Crowe, F.L.; Appleby, P.N.; Allen, N.; Key, T.J. Diet and risk of diverticular disease in Oxford cohort of European Prospective Investigation into Cancer and Nutrition (EPIC): Prospective study of British vegetarians and non-vegetarians. BMJ 2011, 343, d4131. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa: Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 2 January 2021).
- Ma, W.; Nguyen, L.H.; Song, M.; Jovani, M.; Liu, P.-H.; Cao, Y.; Tam, I.; Wu, K.; Giovannucci, E.L.; Strate, L.L.; et al. Intake of Dietary Fiber, Fruits, and Vegetables and Risk of Diverticulitis. Am. J. Gastroenterol. 2019, 114, 1531–1538. [Google Scholar] [CrossRef]
- Cao, Y.; Strate, L.L.; Keeley, B.R.; Tam, I.; Wu, K.; Giovannucci, E.L.; Chan, A.T. Meat intake and risk of diverticulitis among men. Gut 2018, 67, 466–472. [Google Scholar] [CrossRef]
- Strate, L.L.; Keeley, B.R.; Cao, Y.; Wu, K.; Giovannucci, E.L.; Chan, A.T. Western Dietary Pattern Increases, and Prudent Dietary Pattern Decreases, Risk of Incident Diverticulitis in a Prospective Cohort Study. Gastroenterology 2017, 152, 1023–1030.e2. [Google Scholar] [CrossRef] [Green Version]
- Crowe, F.L.; Balkwill, A.; Cairns, B.J.; Appleby, P.N.; Green, J.; Reeves, G.K.; Key, T.J.; Beral, V. Source of dietary fibre and diverticular disease incidence: A prospective study of UK women. Gut 2014, 63, 1450–1456. [Google Scholar] [CrossRef] [Green Version]
- Strate, L.L. Nut, Corn, and Popcorn Consumption and the Incidence of Diverticular Disease. JAMA 2008, 300, 907–914. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-C.; Chung, J.-W.; Baek, J.-H.; Lee, W.-S.; Kim, O.; Park, Y.-H.; Yang, J.-Y.; Lee, W.-K. Risk Factors for Recurrence of Right Colonic Diverticulitis. Dig. Surg. 2019, 36, 509–513. [Google Scholar] [CrossRef]
- Nagata, N.; Niikura, R.; Aoki, T.; Shimbo, T.; Kishida, Y.; Sekine, K.; Tanaka, S.; Watanabe, K.; Sakurai, T.; Yokoi, C.; et al. Colonic diverticular hemorrhage associated with the use of nonsteroidal anti-inflammatory drugs, low-dose aspirin, antiplatelet drugs, and dual therapy. J. Gastroenterol. Hepatol. 2014, 29, 1786–1793. [Google Scholar] [CrossRef]
- Papagrigoriadis, S.; Macey, L.; Bourantas, N.; Rennie, J.A. Smoking may be associated with complications in diverticular disease. BJS 1999, 86, 923–926. [Google Scholar] [CrossRef]
- Mahmood, M.W.; Abraham-Nordling, M.; Håkansson, N.; Wolk, A.; Hjern, F. High intake of dietary fibre from fruit and vegetables reduces the risk of hospitalisation for diverticular disease. Eur. J. Nutr. 2019, 58, 2393–2400. [Google Scholar] [CrossRef] [Green Version]
- Aldoori, W.H.; Giovannucci, E.L.; Rockett, H.R.H.; Sampson, L.; Rimm, E.B.; Willett, A.W.C. A Prospective Study of Dietary Fiber Types and Symptomatic Diverticular Disease in Men. J. Nutr. 1998, 128, 714–719. [Google Scholar] [CrossRef] [Green Version]
- Aldoori, W.H. The Protective Role of Dietary Fiber in Diverticular Disease. Adv. Exp. Med. Biol. 1997, 427, 291–308. [Google Scholar] [CrossRef] [PubMed]
- Schultz, J.K.; Azhar, N.; Binda, G.A.; Barbara, G.; Biondo, S.; Boermeester, M.A.; Chabok, A.; Consten, E.C.J.; Van Dijk, S.T.; Johanssen, A.; et al. European Society of Coloproctology: Guidelines for the management of diverticular disease of the colon. Color. Dis. 2020, 22, 5–28. [Google Scholar] [CrossRef] [PubMed]
- Ley, S.H.; Sun, Q.; Willett, W.C.; Eliassen, A.H.; Wu, K.; Pan, A.; Grodstein, F.; Hu, F.B. Associations between red meat intake and biomarkers of inflammation and glucose metabolism in women. Am. J. Clin. Nutr. 2013, 99, 352–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micha, R.; Michas, G.; Mozaffarian, D. Unprocessed Red and Processed Meats and Risk of Coronary Artery Disease and Type 2 Diabetes—An Updated Review of the Evidence. Curr. Atheroscler. Rep. 2012, 14, 515–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Schulze, M.B.; Manson, J.; Willett, W.C.; Hu, F.B. Red meat consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1088–1096. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | Country | Type of Study | Follow-Up (Years) | Number of pts, Gender, Age | Dietary Assessment | Main Outcome | Intervention/Control | Main Results |
|---|---|---|---|---|---|---|---|---|
| Ma W, 2019 [20] | US | Prospective cohort study (Nurses’ Health Stydy) | 24 | 50,019 women, 43–70 years | FFQ (131 food items) | Dietary fibre consumption and risk of diverticulitis | Intake of fiber divided into quintile | Diverticulitis Compared with patients in the lowest quintile (Q1), patients in the highest quintile (Q5) had: Multivariable adjusted HR = 0.86 (95%CI: 0.78–0.95) for total fibre; HR = 0.89 (95%CI: 0.81–0.99) for cereal fibre; HR = 0.83 (95%CI: 0.75–0.92) for fruit fibre; HR = 0.91 (95%CI: 0.83–1.01) for vegetable fibre. |
| Cao Y, 2018 [21] | US | Prospective cohort study, (Health Professional Follow-up Study) | 26 | 46,461 men 40–75 years | FFQ | Meat consumption and risk of diverticulitis | Intake of meat divided into quintile | Diverticulitis Compared with men in the lowest quintile (Q1), men in the highest quintile (Q5) had: Multivariable RR of 1.58 (95% CI: 1.19–2.11) for total red meat; Multivariable RR of 1.51 (95% CI: 1.12–2.03) for unprocessed red meat; Multivariable RR of 1.03 (95% CI: 0.78–1.35) for processed red meat. Higher consumption of poultry or fish was not associated with risk of diverticulitis. |
| Strate LL, 2017 [22] | US | Prospective cohort study, (Health Professional Follow-up Study) | 26 | 46,295 men 40–75 years | FFQ (131–148 food items) | Dietary patterns and risk of diverticulitis | Western and Prudent dietary pattern, AHEI, into quintile | Diverticulitis Compared with men in the lowest quintile (Q1), men in the highest quintile (Q5) had: Multivariate HR= 1.55 (95% CI:1.20–1.99) for Western pattern; Multivariate HR = 0.74 (95%CI: 0.60–0.91) for Prudent pattern; Multivariate HR = 0.67 (0.55–0.82) for AHEI pattern. |
| Crowe FL, 2014 [23] | UK | Prospective cohort study (The Million Women Study) | 6 | 690,075 women 50–65 yrs | Questionnaire (40 food and beverage items) | Dietary fibre consumption and hospitalization for diverticular disease | Intake in quintile of fiber (g/day) | Complicated diverticular disease * The RR for complicated DD per 5 gr/day were: Total fiber: 0.70 (95%CI: 0.58–0.84); Cereal: 0.65 (95%CI: 0.49–0.85); Fruit:0.60 (95%CI: 0.42–0.85); Non-potato vegetable: 0.70 (95%CI: 0.37–1.30). |
| Strate LL, 2008 [24] | US | Prospective cohort study, (Health Professional Follow-up Study) | 18 | 47,228 men 40–75 years | FFQ (131 food items) | Nut, corn and popcorn consumption and risk of diverticulitis or diverticular bleeding | Frequency of food consumption, (from never /less than once a month, to more than 6 times a day) | Diverticulitis Compared to men with the highest intake, men with the lowest intake had: Multivariate HR: 0.80 (95%CI: 0.63–1.01) for nuts; Multivariate HR: 0.72 (95% CI: 0.56–0.92) for popcorn; Multivariate HR: 1.13 (95% CI: 0.83–1.54) for corn. Diverticular bleeding Multivariate HR: 1.08 (95%CI: 0.77–1.49) for nuts; Multivariate HR: 0.82 (95% CI: 0.59–1.15) for popcorn; Multivariate HR: 1.07 (95% CI: 0.67–1.71) for corn. |
| Author, Year | Country | Type of Study | Follow-Up (Months) | Number of pts, Gender, Age | Alcohol Consumption Assessment | Main Outcome | Intervention/Control | Main Results |
|---|---|---|---|---|---|---|---|---|
| Kim YC, 2019 [25] | South Korea | Retrospective cohort study | 32.9 | 296 pts; women 58.1%; mean age 42.8 ± 13.7 years | Qualitative assessment | Risk factors for recurrent right colonic diverticulitis | Alcohol consumer vs non-alcohol consumer | Recurrent diverticulitis Recurrence rate was higher in alcohol consumer than non-alcohol consumer (p = 0.017). The association was not confirmed at multivariate analysis. |
| Nagata N, 2014 [26] | Japan | Cross-sectional study | NA | 911 pts; women 34%; mean age 66 ± 12 years | Questionnaire | Risk factors for diverticular bleeding | Quantitative assessment: nondrinker/ light drinker, moderate to heavy drinker | Diverticular bleeding Multivariable adjusted HR: OR 3.4 (95%CI:1.4–8.1) for light drinker Multivariable adjusted HR: OR 3.3 (95%CI 1.3–8.5) for moderate to heavy drinker. |
| Papagrigoriadis S, 1999 [27] | UK | Cross-sectional study | NA | 80 pts; women 62.5%; Mean age 69.1 years | Clinical assessment | Risk factors for diverticular complications | Alcohol consumer (≥21 units/week) vs non-alcohol consumer | Complicated diverticular disease (diverticulitis and bleeding) Alcohol consuption was not significantly more common in group 1 (complicated diverticular disease) than in group 2 (not complicated diverticular disease) (OR 2.7, 95%CI: 0.9–7.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carabotti, M.; Falangone, F.; Cuomo, R.; Annibale, B. Role of Dietary Habits in the Prevention of Diverticular Disease Complications: A Systematic Review. Nutrients 2021, 13, 1288. https://doi.org/10.3390/nu13041288
Carabotti M, Falangone F, Cuomo R, Annibale B. Role of Dietary Habits in the Prevention of Diverticular Disease Complications: A Systematic Review. Nutrients. 2021; 13(4):1288. https://doi.org/10.3390/nu13041288
Chicago/Turabian StyleCarabotti, Marilia, Francesca Falangone, Rosario Cuomo, and Bruno Annibale. 2021. "Role of Dietary Habits in the Prevention of Diverticular Disease Complications: A Systematic Review" Nutrients 13, no. 4: 1288. https://doi.org/10.3390/nu13041288