
The Prevalence of Anti-Zein Antibodies: A Comparative Study between Celiac Disease and Irritable Bowel Syndrome

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Populations
2.2. Ethics Statement
2.3. In-House Enzyme-Linked Immunosorbent Assay (ELISA) for IgA/IgG AZA
2.4. Statistical Analysis
3. Results
3.1. Higher Levels of IgA AZA Antibodies in Celiac Disease than Irritable Bowel Syndrome
3.2. Higher Prevalence of Anti-Zein IgA (IgA AZA) Antibodies in Celiac Disease Patients than in Irritable Bowel Syndrome Patients and Healthy Controls
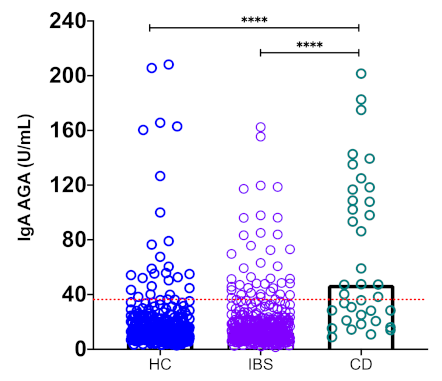
3.3. Higher Prevalence of Anti-Gliadin IgA (IgA AGA) Antibodies in Celiac Disease Patients than Irritable Bowel Syndrome Patients and Healthy Controls
3.4. High Serum Levels of Celiac Disease-Related Antibodies in the IgA AZA-Positive Patients
3.5. Correlation Analysis of IgA AZA, IgA DGP, and IgA AGA Serum Levels in Celiac Disease and Irritable Bowel Syndrome
4. Discussion
5. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Green, P.H.R.; Cellier, C. Celiac Disease. N. Engl. J. Med. 2007, 357, 1731–1743. [Google Scholar] [CrossRef]
- Trovato, C.M.; Raucci, U.; Valitutti, F.; Montuori, M.; Villa, M.P.; Cucchiara, S.; Parisi, P. Neuropsychiatric Manifestations in Celiac Disease. Epilepsy Behav. 2019, 99, 106393. [Google Scholar] [CrossRef]
- Jericho, H.; Guandalini, S. Extra-Intestinal Manifestation of Celiac Disease in Children. Nutrients 2018, 10, 755. [Google Scholar] [CrossRef] [Green Version]
- Trovato, C.M.; Albanese, C.V.; Leoni, S.; Celletti, I.; Valitutti, F.; Cavallini, C.; Montuori, M.; Barbato, M.; Catalano, C.; Cucchiara, S. Lack of Clinical Predictors for Low Mineral Density in Children With Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 799–802. [Google Scholar] [CrossRef]
- Janatuinen, E.K. No Harm from Five Year Ingestion of Oats in Coeliac Disease. Gut 2002, 50, 332–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffenberg, E.J.; Haas, J.; Drescher, A.; Barnhurst, R.; Osberg, I.; Bao, F.; Eisenbarth, G. A Trial of Oats in Children with Newly Diagnosed Celiac Disease. J. Pediatr. 2000, 137, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Spaenij-Dekking, L.; Kooy-Winkelaar, Y.; Koning, F. The Ethiopian Cereal Tef in Celiac Disease. N. Engl. J. Med. 2005, 353, 1748–1749. [Google Scholar] [CrossRef] [PubMed]
- Kristjansson, G. Gut Mucosal Granulocyte Activation Precedes Nitric Oxide Production: Studies in Coeliac Patients Challenged with Gluten and Corn. Gut 2005, 54, 769–774. [Google Scholar] [CrossRef] [Green Version]
- Remes-Troche, J.M.; Nuñez-Alvares, C.; Uscanga-Dominguez, L.F. Celiac Disease in Mexican Population: An Update. Am. J. Gastroenterol. 2013, 108, 283–284. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Ludvigsson, J.F.; Brantner, T.L.; Murray, J.A.; Everhart, J.E. The Prevalence of Celiac Disease in the United States. Am. J. Gastroenterol. 2012, 107, 1538–1544. [Google Scholar] [CrossRef]
- Ford, A.C.; Chey, W.D.; Talley, N.J.; Malhotra, A.; Spiegel, B.M.R.; Moayyedi, P. Yield of Diagnostic Tests for Celiac Disease in Individuals With Symptoms Suggestive of Irritable Bowel Syndrome: Systematic Review and Meta-Analysis. Arch. Intern. Med. 2009, 169, 651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional Bowel Disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef]
- Ragnarsson, G.; Bodemar, G. Pain Is Temporally Related to Eating but Not to Defaecation in the Irritable Bowel Syndrome (IBS). Patients’ Description of Diarrhoea, Constipation and Symptom Variation during a Prospective 6-Week Study. Eur. J. Gastroenterol. Hepatol. 1998, 10, 415–422. [Google Scholar] [CrossRef]
- Fernández-Bañares, F.; Esteve-Pardo, M.; de Leon, R.; Humbert, P.; Cabré, E.; Llovet, J.M.; Gassull, M.A. Sugar Malabsorption in Functional Bowel Disease: Clinical Implications. Am. J. Gastroenterol. 1993, 88, 2044–2050. [Google Scholar] [PubMed]
- Atkinson, W. Food Elimination Based on IgG Antibodies in Irritable Bowel Syndrome: A Randomised Controlled Trial. Gut 2004, 53, 1459–1464. [Google Scholar] [CrossRef] [PubMed]
- Zar, S.; Kumar, D.; Benson, M.J. Food Hypersensitivity and Irritable Bowel Syndrome. Review: Food Hypersensitivity and IBS. Aliment. Pharmacol. Ther. 2001, 15, 439–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zar, S.; Benson, M.J.; Kumar, D. Food-Specific Serum IgG4 and IgE Titers to Common Food Antigens in Irritable Bowel Syndrome. Am. J. Gastroenterol. 2005, 100, 1550–1557. [Google Scholar] [CrossRef]
- Böhn, L.; Störsrud, S.; Törnblom, H.; Bengtsson, U.; Simrén, M. Self-Reported Food-Related Gastrointestinal Symptoms in IBS Are Common and Associated With More Severe Symptoms and Reduced Quality of Life. Am. J. Gastroenterol. 2013, 108, 634–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eswaran, S.; Tack, J.; Chey, W.D. Food: The Forgotten Factor in the Irritable Bowel Syndrome. Gastroenterol. Clin. N. Am. 2011, 40, 141–162. [Google Scholar] [CrossRef]
- Domżał-Magrowska, D.; Kowalski, M.K.; Szcześniak, P.; Bulska, M.; Orszulak-Michalak, D.; Małecka-Panas, E. The Prevalence of Celiac Disease in Patients with Irritable Bowel Syndrome and Its Subtypes. Prz. Gastroenterol. 2016, 11, 276–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo Definitions for Coeliac Disease and Related Terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Dierks-Ventling, C.; Ventling, D. Tissue-Specific Immunofluorescent Localization of Zein and Globulin in Zea Mays (L) Seeds. FEBS Lett. 1982, 144, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Cabrera-Chávez, F.; Iametti, S.; Miriani, M.; de la Barca, A.M.C.; Mamone, G.; Bonomi, F. Maize Prolamins Resistant to Peptic-Tryptic Digestion Maintain Immune-Recognition by IgA from Some Celiac Disease Patients. Plant Foods Hum. Nutr. 2012, 67, 24–30. [Google Scholar] [CrossRef]
- Baydoun, A.; Maakaron, J.E.; Halawi, H.; Abou Rahal, J.; Taher, A.T. Hematological Manifestations of Celiac Disease. Scand. J. Gastroenterol. 2012, 47, 1401–1411. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, K.; Halmos, E.P.; Knowles, S.; Mullan, B.; Tye-Din, J.A. Maintenance of a Gluten Free Diet in Coeliac Disease: The Roles of Self-Regulation, Habit, Psychological Resources, Motivation, Support, and Goal Priority. Appetite 2018, 125, 356–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valitutti, F.; De Santis, B.; Trovato, C.M.; Montuori, M.; Gatti, S.; Oliva, S.; Brera, C.; Catassi, C. Assessment of Mycotoxin Exposure in Breastfeeding Mothers with Celiac Disease. Nutrients 2018, 10, 336. [Google Scholar] [CrossRef] [Green Version]
- Rai, S.; Kaur, A.; Chopra, C.S. Gluten-Free Products for Celiac Susceptible People. Front. Nutr. 2018, 5, 116. [Google Scholar] [CrossRef]
- Ortiz Sánchez, J.P.; Mata Haro, V.; Cabrera Chávez, F.; Calderón de la Barca, A.M. Prolamins of Maize and Wheat Differentially Affect Intestinal Cells Both in Biopsies of Celiac Patients and CACO-2 Cell Line. Food Agric. Immunol. 2016, 27, 259–272. [Google Scholar] [CrossRef] [Green Version]
- Ortiz-Sánchez, J.; Cabrera-Chávez, F.; de la Barca, A. Maize Prolamins Could Induce a Gluten-Like Cellular Immune Response in Some Celiac Disease Patients. Nutrients 2013, 5, 4174–4183. [Google Scholar] [CrossRef]
- Accomando, S.; Albino, C.; Montaperto, D.; Amato, G.M.; Corsello, G. Multiple Food Intolerance or Refractory Celiac Sprue? Dig. Liver Dis. 2006, 38, 784–785. [Google Scholar] [CrossRef]
- Cabrera-Chávez, F.; Rouzaud-Sández, O.; Sotelo-Cruz, N.; Calderón de la Barca, A.M. Transglutaminase Treatment of Wheat and Maize Prolamins of Bread Increases the Serum IgA Reactivity of Celiac Disease Patients. J. Agric. Food Chem. 2008, 56, 1387–1391. [Google Scholar] [CrossRef]
- Skerritt, J.H.; Devery, J.M.; Penttila, I.A.; LaBrooy, J.T. Cellular and Humoral Responses in Coeliac Disease. 2. Protein Extracts from Different Cereals. Clin. Chim. Acta 1991, 204, 109–122. [Google Scholar] [CrossRef]
- Bizzaro, N.; Tonutti, E. Anti-Gliadin Antibodies. In Autoantibodies; Elsevier: Amsterdam, The Netherlands, 2007; pp. 451–456. ISBN 978-0-444-52763-9. [Google Scholar]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac Disease: A Comprehensive Current Review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [Green Version]
- Kumar, V.; Jarzabek-Chorzelska, M.; Sulej, J.; Karnewska, K.; Farrell, T.; Jablonska, S. Celiac Disease and Immunoglobulin A Deficiency: How Effective Are the Serological Methods of Diagnosis? CVI 2002, 9, 1295–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbato, M.; Maiella, G.; Di Camillo, C.; Guida, S.; Valitutti, F.; Lastrucci, G.; Mainiero, F.; Cucchiara, S. The Anti-Deamidated Gliadin Peptide Antibodies Unmask Celiac Disease in Small Children with Chronic Diarrhoea. Dig. Liver Dis. 2011, 43, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Hollén, E.; Högberg, L.; Stenhammar, L.; Fälth-Magnusson, K.; Magnusson, K.E. Antibodies to Oat Prolamines (Avenins) in Children with Coeliac Disease. Scand. J. Gastroenterol. 2003, 38, 742–746. [Google Scholar] [CrossRef]
- Volta, U.; Granito, A.; Fiorini, E.; Parisi, C.; Piscaglia, M.; Pappas, G.; Muratori, P.; Bianchi, F.B. Usefulness of Antibodies to Deamidated Gliadin Peptides in Celiac Disease Diagnosis and Follow-Up. Dig. Dis. Sci. 2008, 53, 1582–1588. [Google Scholar] [CrossRef]
- Penny, H.A.; Raju, S.A.; Lau, M.S.; Marks, L.J.; Baggus, E.M.; Bai, J.C.; Bassotti, G.; Bontkes, H.J.; Carroccio, A.; Danciu, M.; et al. Accuracy of a No-Biopsy Approach for the Diagnosis of Coeliac Disease across Different Adult Cohorts. Gut 2020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Diagnosis | n | Sex (F/M) | Age (years) Median (range) |
|---|---|---|---|
| Celiac disease | 37 | 28/9 | 45 (18–85) |
| IBS with constipation | 121 | 107/14 | 43 (18–80) |
| IBS with mixed pattern | 210 | 173/37 | 41.5 (12–77) |
| IBS with diarrhea | 44 | 40/4 | 45 (18–69) |
| Total IBS | 375 | 320/55 | 43 (12–80) |
| Healthy controls | 302 | 167/135 | 21 (17–51) |
| Diagnosis | n | IgA AZA+ n (F/M) | Prevalence (%) | p-Value | IgA AGA+ n (F/M) | Prevalence (%) | p-Value |
|---|---|---|---|---|---|---|---|
| CD | 37 | 13 (8/5) | 35.1 | <0.0001 | 24 (16/8) | 64.9 | <0.0001 |
| IBS-C | 121 | 4 (4/0) | 3.3 | 0.5185 | 15 (12/3) | 12.4 | 1.0000 |
| IBS-M | 210 | 12 (12/0) | 5.7 | 0.0571 | 32 (29/3) | 15.2 | 0.3582 |
| IBS-D | 44 | 0 (0/0) | 0 | 1.0000 | 8 (8/0) | 18.2 | 0.3342 |
| Total IBS | 375 | 16 (16/0) | 4.36 | 0.0726 | 55 (49/6) | 17.7 | 0.3697 |
| HC | 302 | 7 (3/4) | 2.3 | – | 37 (11/26) | 12.3 | --- |
| Serological Marker | IgA AZA Negative (n = 24) | IgA AZA Positive (n = 13) | p-Value | |
|---|---|---|---|---|
| IgA tTG | n (%) | 15 (62.5) | 7 (53.9) | 0.7304 |
| U/mL | 36.1 (2.9–133) | 30.9 (6.9–99.8) | 0.8839 | |
| IgA DGP | n (%) | 12 (50.0) | 9 (69.2) | 0.3149 |
| U/mL | 29.88 (4.05–66.3) | 51.5 (7.6–104.1) | 0.0337 | |
| IgA AGA | n (%) | 14 (58.3) | 10 (76.9) | 0.3052 |
| U/mL | 56.37 (8.87–135.14) | 97.99 (18.3–201.5) | 0.0359 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Vargas, L.A.; Hernández-Flores, K.G.; Cabrera-Jorge, F.J.; Remes-Troche, J.M.; Reyes-Huerta, J.; Vivanco-Cid, H. The Prevalence of Anti-Zein Antibodies: A Comparative Study between Celiac Disease and Irritable Bowel Syndrome. Nutrients 2021, 13, 649. https://doi.org/10.3390/nu13020649
Sánchez-Vargas LA, Hernández-Flores KG, Cabrera-Jorge FJ, Remes-Troche JM, Reyes-Huerta J, Vivanco-Cid H. The Prevalence of Anti-Zein Antibodies: A Comparative Study between Celiac Disease and Irritable Bowel Syndrome. Nutrients. 2021; 13(2):649. https://doi.org/10.3390/nu13020649
Chicago/Turabian StyleSánchez-Vargas, Luis Alberto, Karina Guadalupe Hernández-Flores, Francisco Javier Cabrera-Jorge, José María Remes-Troche, Job Reyes-Huerta, and Héctor Vivanco-Cid. 2021. "The Prevalence of Anti-Zein Antibodies: A Comparative Study between Celiac Disease and Irritable Bowel Syndrome" Nutrients 13, no. 2: 649. https://doi.org/10.3390/nu13020649