
Systematic Review of Behaviour Change Theories Implementation in Dietary Interventions for People Who Have Survived Cancer

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Searching
2.2. Study Inclusion Criteria
2.3. Outcomes
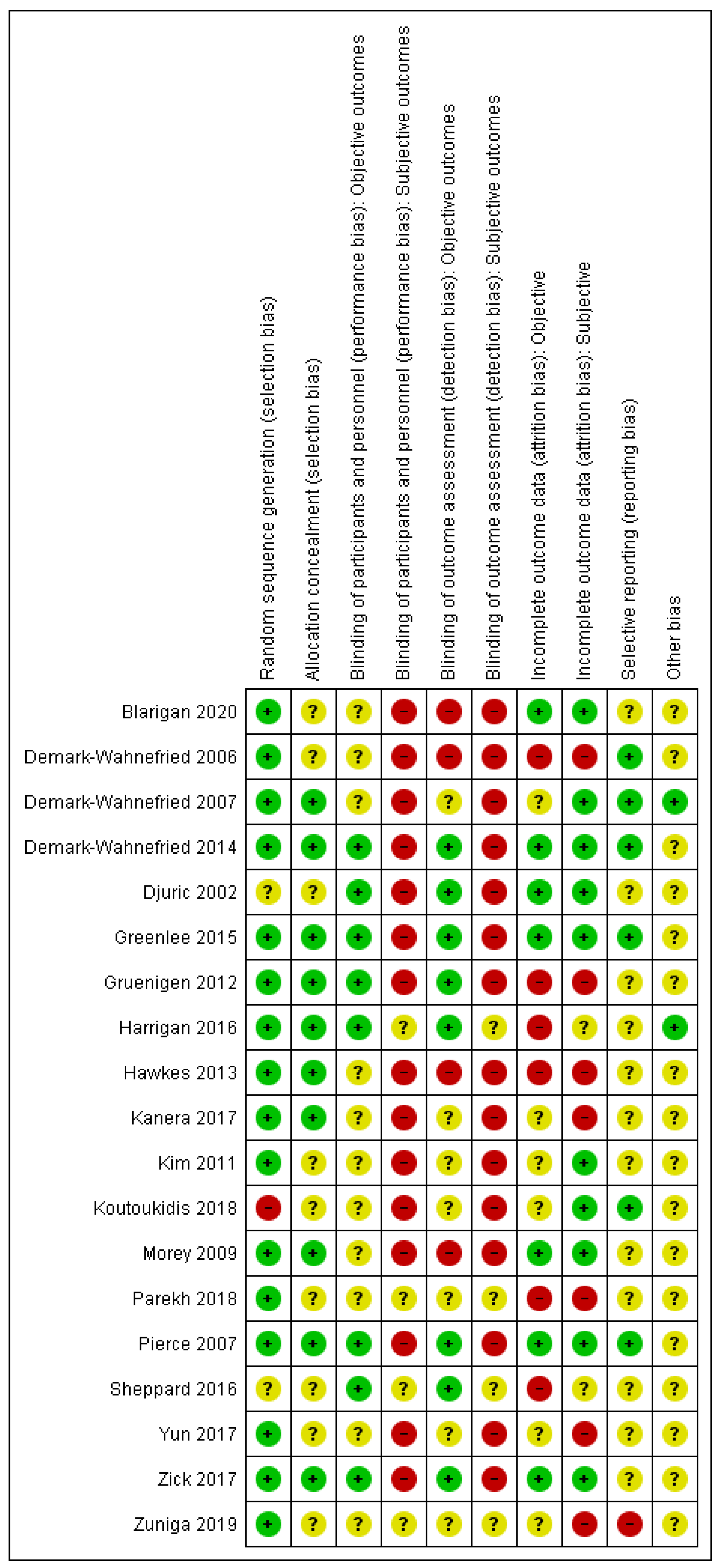
2.4. Data Extraction and Risk of Bias Assessment
2.5. Statistical Methods
3. Results
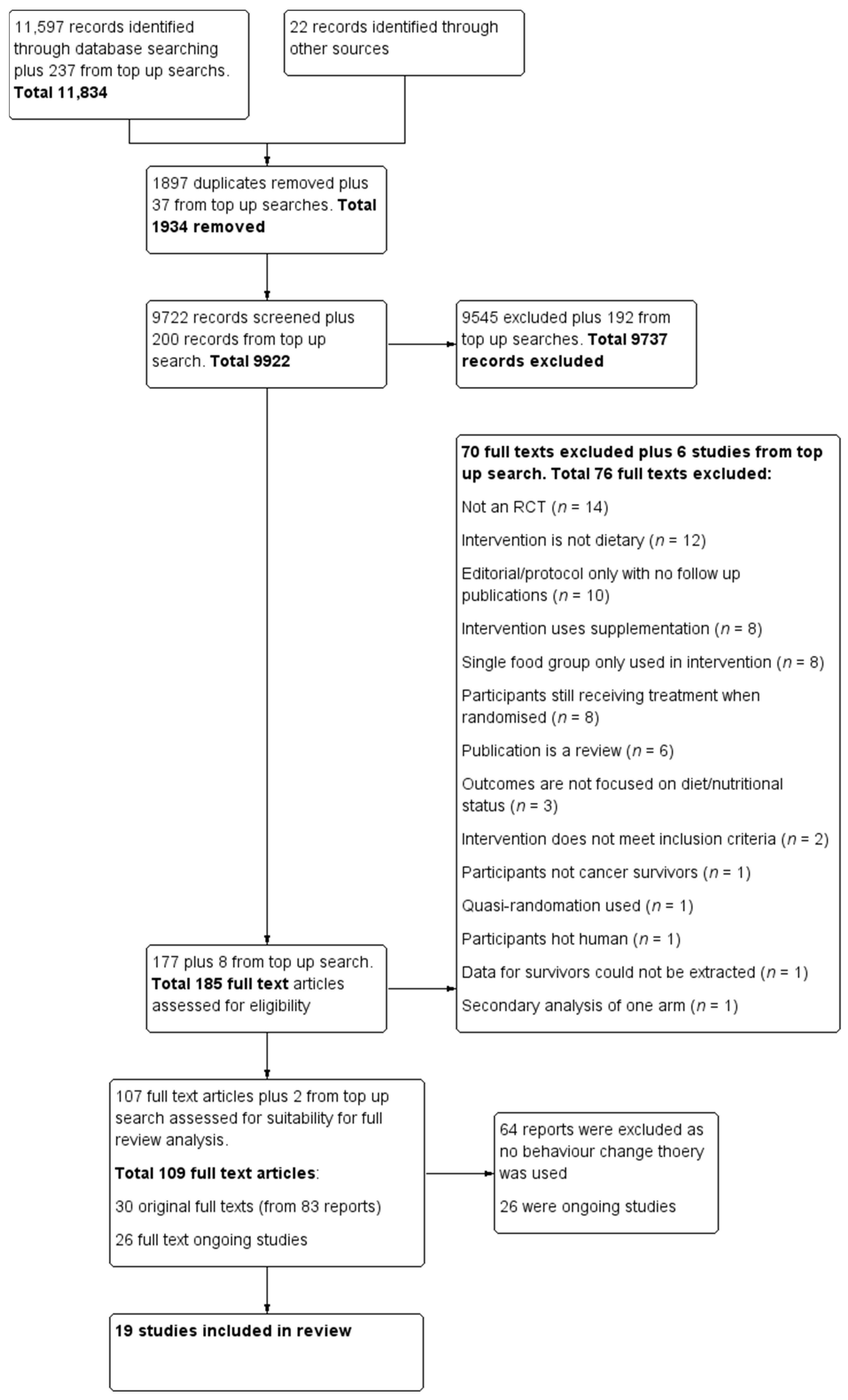
3.1. Search Results
3.2. Studies Characteristics
3.3. Theoretical Framework
3.3.1. Implementation of Behaviour Change Theory in the Interventions
3.3.2. Use and Reporting of Behaviour Change Techniques in the Interventions
3.4. Dietary Behaviour Outcomes
3.5. Mediators of Behaviour
4. Discussion
4.1. Intervention Design
4.2. Description of the Intervention
4.3. Outcomes Reporting
4.4. Assessment of the Behaviour Change Theory in Interventions
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- National Cancer Research Institute. Definitions. 2021. Available online: https://cancercontrol.cancer.gov/ocs/statistics#definition-survivorship (accessed on 16 January 2021).
- Vergnaud, A.C.; Romaguera, D.; Peeters, P.H.; Van Gils, C.H.; Chan, D.S.M.; Romieu, I.; Freisling, H.; Ferrari, P.; Clavel-Chapelon, F.; Fagherazzi, G.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research guidelines and risk of death in Europe: Results from the European Prospective Investigation into Nutrition and Cancer cohort study. Am. J. Clin. Nutr. 2013, 97, 1107–1120. [Google Scholar] [CrossRef] [Green Version]
- Schwedhelm, C.; Boeing, H.; Hoffmann, G.; Aleksandrova, K.; Schwingshackl, L. Effect of diet on mortality and cancer recurrence among cancer survivors: A systematic review and meta-analysis of cohort studies. Nutr. Rev. 2016, 74, 737–748. [Google Scholar] [CrossRef] [Green Version]
- Demark-Wahnefried, W.; Aziz, N.M.; Rowland, J.H.; Pinto, B.M. Riding the Crest of the Teachable Moment: Promoting Long-Term Health After the Diagnosis of Cancer. J. Clin. Oncol. 2005, 23, 5814–5830. [Google Scholar] [CrossRef] [Green Version]
- Bluethmann, S.M.; Basen-Engquist, K.; Vernon, S.W.; Cox, M.G.; Gabriel, K.P.; Stansberry, S.A.; Carmack, C.L.; Blalock, J.A.; Demark-Wahnefried, W. Grasping the ‘teachable moment’: Time since diagnosis, symptom burden and health behaviors in breast, colorectal and prostate cancer survivors. Psycho-Oncology 2015, 24, 1250–1257. [Google Scholar] [CrossRef] [PubMed]
- Pinto, B.M.; Maruyama, N.C.; Clark, M.M.; Cruess, D.G.; Park, E.; Roberts, M. Motivation to Modify Lifestyle Risk Behaviors in Women Treated for Breast Cancer. Mayo Clin. Proc. 2002, 77, 122–129. [Google Scholar] [CrossRef]
- Smith, L.; Croker, H.; Fisher, A.; Williams, K.; Wardle, J.; Beeken, R.J. Cancer survivors’ attitudes towards and knowledge of physical activity, sources of information, and barriers and facilitators of engagement: A qualitative study. Eur. J. Cancer Care 2017, 26, e12641. [Google Scholar] [CrossRef] [Green Version]
- Sremanakova, J.; Jones, D.; Cooke, R.; Burden, S. Exploring Views of Healthcare Professionals, Researchers, and People Living with and beyond Colorectal Cancer on a Healthy-Eating and Active Lifestyle Resource. Nutrients 2019, 11, 2482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, S.J.; Gibson, D.; Eden, M.; Lal, S.; Todd, C.; Ness, A.; Burden, S. What are colorectal cancer survivors’ preferences for dietary advice? A best-worst discrete choice experiment. J. Cancer Surviv. 2017, 11, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Avery, L.; Flynn, D.; Van Wersch, A.; Sniehotta, F.F.; Trenell, M.I. Changing Physical Activity Behavior in Type 2 Diabetes: A systematic review and meta-analysis of behavioral interventions. Diabetes Care 2012, 35, 2681–2689. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, Y.K.; Sheeran, P.; Hawley, M.S. Effective behaviour change techniques in smoking cessation interventions for people with chronic obstructive pulmonary disease: A meta-analysis. Br. J. Health Psychol. 2013, 19, 181–203. [Google Scholar] [CrossRef] [Green Version]
- Lara, J.; Evans, E.H.; O’Brien, N.; Moynihan, P.J.; Meyer, T.D.; Adamson, A.J.; Errington, L.; Sniehotta, F.F.; White, M.; Mathers, J.C. Association of behaviour change techniques with effectiveness of dietary interventions among adults of retirement age: A systematic review and meta-analysis of randomised controlled trials. BMC Med. 2014, 12, 177. [Google Scholar] [CrossRef] [Green Version]
- McEachan, R.R.C.; Conner, M.; Taylor, N.J.; Lawton, R.J. Prospective prediction of health-related behaviours with the Theory of Planned Behaviour: A meta-analysis. Health Psychol. Rev. 2011, 5, 97–144. [Google Scholar] [CrossRef]
- Will, J.C.; Farris, R.P.; Sanders, C.G.; Stockmyer, C.K.; Finkelstein, E.A. Health Promotion Interventions for Disadvantaged Women: Overview of the WISEWOMAN Projects. J. Womens Health 2004, 13, 484–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanz, K.; Bishop, D.B. The Role of Behavioral Science Theory in Development and Implementation of Public Health Interventions. Annu. Rev. Public Health 2010, 31, 399–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noar, S.M.; Benac, C.N.; Harris, M.S. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol. Bull. 2007, 133, 673–693. [Google Scholar] [CrossRef] [Green Version]
- Sheeran, P.; Klein, W.M.; Rothman, A.J. Health Behavior Change: Moving from Observation to Intervention. Annu. Rev. Psychol. 2017, 68, 573–600. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion from the perspective of social cognitive theory. Psychol. Health 1998, 13, 623–649. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C.; Norcross, J.C. In search of how people change: Applications to addictive behaviors. Am. Psychol. 1992, 47, 1102–1114. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Why people use health services. Milbank Mem. Fund Q. 1966, 44, 94–127. [Google Scholar] [CrossRef] [Green Version]
- Glanz, K. Theory at a Glance: A Guide for Health Promotion Practice; US Department of Health and Human Services, Public Health Service, National Institute of Health: USA, 1997; Volume 97. [Google Scholar]
- Grimmett, C.; Corbett, T.; Brunet, J.; Shepherd, J.; Pinto, B.M.; May, C.R.; Foster, C. Systematic review and meta-analysis of maintenance of physical activity behaviour change in cancer survivors. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 37. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Carey, R.N.; Johnston, M.; Rothman, A.J.; De Bruin, M.; Kelly, M.P.; Connell, L.E. From Theory-Inspired to Theory-Based Interventions: A Protocol for Developing and Testing a Methodology for Linking Behaviour Change Techniques to Theoretical Mechanisms of Action. Ann. Behav. Med. 2018, 52, 501–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Johnston, M. Theories and Techniques of Behaviour Change: Developing a Cumulative Science of Behaviour Change. Health Psychol. Rev. 2012, 6, 1–6. [Google Scholar] [CrossRef]
- Michie, S.; West, R.; Sheals, K.; A Godinho, C. Evaluating the effectiveness of behavior change techniques in health-related behavior: A scoping review of methods used. Transl. Behav. Med. 2018, 8, 212–224. [Google Scholar] [CrossRef] [Green Version]
- Noar, S.M.; Zimmerman, R.S. Health Behavior Theory and cumulative knowledge regarding health behaviors: Are we moving in the right direction? Health Educ. Res. 2005, 20, 275–290. [Google Scholar] [CrossRef] [Green Version]
- Stacey, F.G.; James, E.L.; Chapman, K.; Courneya, K.S.; Lubans, D.R. A systematic review and meta-analysis of social cognitive theory-based physical activity and/or nutrition behavior change interventions for cancer survivors. J. Cancer Surviv. 2015, 9, 305–338. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Graves, K.D. Social cognitive theory and cancer patients’ quality of life: A meta-analysis of psychosocial intervention components. Health Psychol. 2003, 22, 210–219. [Google Scholar] [CrossRef]
- Burden, S.; Jones, D.J.; Sremanakova, J.; Sowerbutts, A.M.; Lal, S.; Pilling, M.; Todd, C. Dietary interventions for adult cancer survivors. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Altman, D.; Sterne, J.; Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1; (updated March 2011); Cochrane: London, UK, 2011; Available online: training.cochrane.org/handbook (accessed on 16 January 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Demark-Wahnefried, W.; Clipp, E.C.; Lipkus, I.M.; Lobach, D.; Snyder, D.C.; Sloane, R.; Peterson, B.; Macri, J.M.; Rock, C.L.; McBride, C.M.; et al. Main Outcomes of the FRESH START Trial: A Sequentially Tailored, Diet and Exercise Mailed Print Intervention Among Breast and Prostate Cancer Survivors. J. Clin. Oncol. 2007, 25, 2709–2718. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Clipp, E.C.; Morey, M.C.; Pieper, C.F.; Sloane, R.; Snyder, D.C.; Cohen, H.J. Lifestyle Intervention Development Study to Improve Physical Function in Older Adults With Cancer: Outcomes From Project LEAD. J. Clin. Oncol. 2006, 24, 3465–3473. [Google Scholar] [CrossRef] [Green Version]
- Demark-Wahnefried, W.; Jones, L.W.; Snyder, D.C.; Sloane, R.J.; Kimmick, G.G.; Hughes, D.C.; Badr, H.J.; Miller, P.E.; Burke, L.E.; Lipkus, I.M. Daughters and Mothers Against Breast Cancer (DAMES): Main outcomes of a randomized controlled trial of weight loss in overweight mothers with breast cancer and their overweight daughters. Cancer 2014, 120, 2522–2534. [Google Scholar] [CrossRef] [PubMed]
- Djuric, Z.; DiLaura, N.M.; Jenkins, I.; Darga, L.; Jen, C.K.-L.; Mood, D.; Bradley, E.; Hryniuk, W.M. Combining Weight-Loss Counseling with the Weight Watchers Plan for Obese Breast Cancer Survivors. Obes. Res. 2002, 10, 657–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenlee, H.; Gaffney, A.O.; Aycinena, A.C.; Koch, P.; Contento, I.; Karmally, W.; Richardson, J.M.; Lim, E.; Tsai, W.-Y.; Crew, K.; et al. ¡Cocinar Para Su Salud!: Randomized Controlled Trial of a Culturally Based Dietary Intervention among Hispanic Breast Cancer Survivors. J. Acad. Nutr. Diet. 2015, 115, 709–723.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrigan, M.; Cartmel, B.; Loftfield, E.; Sanft, T.; Chagpar, A.B.; Zhou, Y.; Playdon, M.; Li, F.; Irwin, M.L. Randomized Trial Comparing Telephone Versus In-Person Weight Loss Counseling on Body Composition and Circulating Biomarkers in Women Treated for Breast Cancer: The Lifestyle, Exercise, and Nutrition (LEAN) Study. J. Clin. Oncol. 2016, 34, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, A.L.; Chambers, S.K.; Pakenham, K.I.; Patrao, T.A.; Baade, P.D.; Lynch, B.M.; Aitken, J.F.; Meng, X.; Courneya, K.S. Effects of a Telephone-Delivered Multiple Health Behavior Change Intervention (CanChange) on Health and Behavioral Outcomes in Survivors of Colorectal Cancer: A Randomized Controlled Trial. J. Clin. Oncol. 2013, 31, 2313–2321. [Google Scholar] [CrossRef]
- Koutoukidis, D.A.; Beeken, R.J.; Manchanda, R.; Burnell, M.; Ziauddeen, N.; Michalopoulou, M.; Knobf, M.T.; Lanceley, A. Diet, physical activity, and health-related outcomes of endometrial cancer survivors in a behavioral lifestyle program: The Diet and Exercise in Uterine Cancer Survivors (DEUS) parallel randomized controlled pilot trial. Int. J. Gynecol. Cancer 2019, 29, 531–540. [Google Scholar] [CrossRef]
- Morey, M.C.; Snyder, D.C.; Sloane, R.; Cohen, H.J.; Peterson, B.; Hartman, T.J.; Miller, P.; Mitchell, D.C.; Demark-Wahnefried, W. Effects of Home-Based Diet and Exercise on Functional Outcomes Among Older, Overweight Long-term Cancer Survivors. JAMA 2009, 301, 1883–1891. [Google Scholar] [CrossRef] [Green Version]
- Pierce, J.P.; Natarajan, L.; Caan, B.J.; Parker, B.A.; Greenberg, E.R.; Flatt, S.W.; Rock, C.L.; Kealey, S.; Al-Delaimy, W.K.; Bardwell, W.A.; et al. Influence of a Diet Very High in Vegetables, Fruit, and Fiber and Low in Fat on Prognosis Following Treatment for Breast Cancer. JAMA 2007, 298, 289–298. [Google Scholar] [CrossRef]
- Von Gruenigen, V.; Frasure, H.; Kavanagh, M.B.; Janata, J.; Waggoner, S.; Rose, P.; Lerner, E.; Courneya, K.S. Survivors of uterine cancer empowered by exercise and healthy diet (SUCCEED): A randomized controlled trial. Gynecol. Oncol. 2012, 125, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- RevMan R, version 5.4.1; The Nordic Cochrane Centre, The Cochrane Collaboration: Oxford, UK, 2014.
- Van Blarigan, E.L.; Kenfield, S.A.; Chan, J.M.; Van Loon, K.; Paciorek, A.; Zhang, L.; Chan, H.; Savoie, M.B.; Bocobo, A.G.; Liu, V.N.; et al. Feasibility and acceptability of a web-based dietary intervention with text messages for colorectal cancer: A randomized pilot trial. Cancer Epidemiol. Biomark. Prev. 2020, 29, 752–760. [Google Scholar] [CrossRef]
- Kanera, I.M.; Willems, R.A.; Bolman, C.A.W.; Mesters, I.; Verboon, P.; Lechner, L. Long-term effects of a web-based cancer aftercare intervention on moderate physical activity and vegetable consumption among early cancer survivors: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Shin, M.S.; Lee, H.S.; Lee, E.S.; Ro, J.S.; Kang, H.S.; Kim, S.W.; Lee, W.H.; Kim, H.S.; Kim, C.J.; et al. Randomized Pilot Test of a Simultaneous Stage-Matched Exercise and Diet Intervention for Breast Cancer Survivors. Oncol. Nurs. Forum 2011, 38, E97–E106. [Google Scholar] [CrossRef] [Green Version]
- Parekh, N.; Jiang, J.; Buchan, M.; Meyers, M.; Gibbs, H.; Krebs, P. Nutrition Literacy among Cancer Survivors: Feasibility Results from the Healthy Eating and Living Against Breast Cancer (HEAL-BCa) Study: A Pilot Randomized Controlled Trial. J. Cancer Educ. 2018, 33, 1239–1249. [Google Scholar] [CrossRef]
- Sheppard, V.B.; Hicks, J.; Makambi, K.H.; Hurtado-De-Mendoza, A.; Demark-Wahnefried, W.; Adamscampbell, L.L. The feasibility and acceptability of a diet and exercise trial in overweight and obese black breast cancer survivors: The Stepping STONE study. Contemp. Clin. Trials 2016, 46, 106–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yun, Y.H.; Kim, Y.A.; Lee, M.K.; Sim, J.A.; Nam, B.-H.; Kim, S.; Lee, E.S.; Noh, D.-Y.; Lim, J.-Y.; Kim, S.; et al. A randomized controlled trial of physical activity, dietary habit, and distress management with the Leadership and Coaching for Health (LEACH) program for disease-free cancer survivors. BMC Cancer 2017, 17, 298. [Google Scholar] [CrossRef]
- Zick, S.M.; Colacino, J.; Cornellier, M.; Khabir, T.; Surnow, K.; Djuric, Z. Fatigue reduction diet in breast cancer survivors: A pilot randomized clinical trial. Breast Cancer Res. Treat. 2017, 161, 299–310. [Google Scholar] [CrossRef]
- Zuniga, K.E.; Parma, D.L.; Muñoz, E.; Spaniol, M.; Wargovich, M.; Ramirez, A.G. Dietary intervention among breast cancer survivors increased adherence to a Mediterranean-style, anti-inflammatory dietary pattern: The Rx for Better Breast Health Randomized Controlled Trial. Breast Cancer Res. Treat. 2018, 173, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Dombrowski, S.U.; Sniehotta, F.F.; Avenell, A.; Coyne, J.C. Current issues and future directions inPsychology and Health: Towards a cumulative science of behaviour change: Do current conduct and reporting of behavioural interventions fall short of best practice? Psychol. Health 2007, 22, 869–874. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; MacIntyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kok, G.; Schaalma, H.; Ruiter, R.A.C.; Van Empelen, P.; Brug, J. Intervention Mapping: Protocol for Applying Health Psychology Theory to Prevention Programmes. J. Health Psychol. 2004, 9, 85–98. [Google Scholar] [CrossRef] [Green Version]
- Lorencatto, F.; West, R.; Stavri, Z.; Michie, S. How Well Is Intervention Content Described in Published Reports of Smoking Cessation Interventions? Nicotine Tob. Res. 2012, 15, 1273–1282. [Google Scholar] [CrossRef]
- Balhareth, A.; Aldossary, M.Y.; McNamara, D. Impact of physical activity and diet on colorectal cancer survivors’ quality of life: A systematic review. World J. Surg. Oncol. 2019, 17, 153. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, P.; Grant, S.; Mayo-Wilson, E.; Macdonald, G.; Michie, S.; Hopewell, S.; Moher, D. Reporting randomised trials of social and psychological interventions: The CONSORT-SPI 2018 Extension. Trials 2018, 19, 407. [Google Scholar] [CrossRef]
- Chiarotto, A.; Ostelo, R.W.; Turk, D.C.; Buchbinder, R.; Boers, M. Core outcome sets for research and clinical practice. Braz. J. Phys. Ther. 2017, 21, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Rejeski, W.; Brawley, L.R.; McAuley, E.; Rapp, S. An examination of theory and behavior change in randomized clinical trials. Control. Clin. Trials 2000, 21, S164–S170. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors | n | Mean Age (SD) (Years) | Gender (F:M ratio) | Ethnicity (%) | Higher education (%) | Cancer Site |
|---|---|---|---|---|---|---|
| Blarigan 2020 [47] | 50 | 5.5 (3.5) | 33/17 | White 70%, Other 30% | College graduate 96% | Colorectal |
| Demark- Wahnefried 2006 [34] | 182 | 71.5 (4.4) vs. 71.9 (5.6) | 104/78 | White 82.0% vs. 82.8% African American 14.6% vs. 15.0%, Other 3.4% vs. 2.2% | Not reported | Breast, prostate |
| Demark- Wahnefried 2007 [33] | 543 | 57 (10.8) | 304/239 | White 83%, Black 13%, Other 4% | College graduate/ post graduate 58% | Breast, prostate |
| Demark- Wahnefried 2014 [35] | 43 | 61.3 (7.4) ** | 43/0 | Non-Hispanic White 74% Hispanic white 7%, African American 18%, Asian 1% | College graduate 34.3% | Breast |
| Djuric 2002 [36] | 48 | 36–70 * | 48/0 | White 73%, African American 25% | College graduate 63% | Breast |
| Greenlee 2015 [37] | 70 | 55.1 (9.1) vs. 58.0 (10.1) | 70/0 | White 41.2% vs. 38.9%, Black 20.6% vs. 30.6%, Mixed 14.7% vs. 16.7%, Native American 5.9% vs. 0.0% | College degree or higher 14.7% vs. 5.6% | Breast |
| Gruenigen 2012 [43] | 75 | 57 (8.6) vs. 58.9 (10.9) | 75/0 | Caucasian 87.8% vs. 94.1%, African American 9.8% vs. 2.9%, Other 2.4% vs. 2.9% | College graduate or higher 39.0% vs. 41.2% | Gynaeco-logical |
| Harrigan 2016 [38] | 100 | 59 (7.5) | 100/0 | Non-Hispanic White 91% | College degree 29%, graduate degree 37% | Breast |
| Hawkes 2013 | 410 | 64.9 (10.8) vs. 67.8 (9.2) | 189/221 | Not reported | Not reported | Colon |
| Kanera 2017 [48] | 462 | 55.6 (11.5) vs. 56.2 (11.3) | 369/93 | Not reported | High education 34.2% vs. 27.7% | Mix |
| Kim 2011 [49] | 45 | 44.6 (9.9) vs. 47.1 (7.3) | 45/0 | Not reported | Completed university 35.5% | Breast |
| Koutoukidis 2019 [40] | 62 | 62.1 (8.3) | 62/0 | White 67% Asian 18% Black 8% Other 6% | Degree 47% | Gynaeco-logical |
| Morey 2009 [41] | 641 | 73 (5.0) vs. 73.1 (5.1) | 349/292 | White 89.0% vs. 88.5% | Not reported | Mix ° |
| Parekh 2018 [50] | 59 | 58.5 (9.8) vs. 57 (10.8) | 59/0 | Asian 3.6% vs. 6.5%, Black or African American 28.6% vs. 16.1%, White 67.9% vs. 67.7, American Indian/Alaska Native 0.0% vs. 6.5%, Other race 0 vs. 3.2% | BA 25% vs. 35.5%, MA 39.3% vs. 35.5%, PhD 3.6% | Breast |
| Pierce 2007 [42] | 3088 | 53.3 (9.8) vs. 53.0 (9.0) | 3088/0 | White 85% vs. 85.6%, African American 4% vs. 3.7%, Hispanic 5.7% vs. 5%, Asian American 3% vs. 3.2%, Mixed/other 2.3% vs. 2.5% | Not reported | Breast |
| Sheppard 2016 [51] | 22 | 54.7 (9.8) | 22/0 | African American 100% | Not reported | Breast |
| Yun 2017 [52] | 206 | 50.68 (9.4) | 164/42 | Korean 100% | College 48.53% | Mix ° |
| Zick 2017 [53] | 30 | 64.4 (10.0) vs. 10.4 (9.35) | 30/0 | White 93% | Not reported | Breast |
| Zuniga 2019 [50] | 125 | 55.3 (10.3) vs. 58.4 (8.2) | 125/0 | Anglo 41.7% vs. 43.1% Latino 51.7% vs. 50.8% Other 6.7% vs. 6.2% | Some college/degree 40.0% vs. 26.2% college or higher 45.0% vs. 63.1% | Breast |
| Authors | Theory | Intervention Design and Resources | Behavioural Mediators Measured | Dietary Behaviour Beasures | Dietary Assessment Method | Physical Activity | Time Point (Months) |
|---|---|---|---|---|---|---|---|
| Blarigan 2020 [47] | SCT, TPB | Web based—text messages, printed materials, and personalised reports | Not reported | Vegetables, grains, fish, meat, sugary drinks, alcohol | 24 h recall for 4 days | No | 3, 6 follow up |
| Demark- Wahnefried 2006 [34] | TTM, SCT | Paper based—mailed information, telephone counselling, tailored workbook—information on current stage of diet/exercise, comparison to national guide and tips for change | Readiness to healthy diet, self-efficacy to healthy diet | Fruit and vegetables, BMI, DQI | 3-day recall | Yes | 6, 12 follow up |
| Demark- Wahnefried 2007 [33] | TTM, SCT | Paper based—mailed information, customized messages based on IT system programme reflecting TTM, SCT in tailored workbook, record logs, newsletter, advice for overcoming barriers, fun facts, graphic depiction of progress, update cards, pedometers | Self-efficacy of eating fruits and vegetables, stage of readiness to increase fruits and vegetables, behaviours practised at goal level | Fruit and vegetables, BMI, Fat (kcal), DQI | Diet history questionnaire | Yes | 10 |
| Demark- Wahnefried 2014 [35] | SCT, TTM | Mailed intervention—SCT tailored newsletters, messages on progress, reinforcement, encouragement, feedback, barriers, shoe chip, food records, activities logs, logbook, reference manual, website | Self-efficacy of adhering to healthy weight loss diet | EI, BMI, weight, WC, DQI | 24 h recall | Yes | 12 |
| Djuric 2002 [36] | SCT | One to one/telephone counselling, group meetings, written resources but details not reported | Not reported | EI | 3-day food diary | Yes | 3, 12 |
| Greenlee 2015 [37] | TTM, SCT | Group sessions on education, cooking and healthy shopping, resources—no details | Not reported | EI, fruit and vegetables, weight, BMI, WC, HC, WHP | 24 h recall | No | 3, 6 follow up |
| Gruenigen 2012 [43] | SCT | Group sessions, follow up newsletter, telephone, and emails to reinforce goals, resources—no detials | Not reported | fruit and vegetables, EI, weight, WC | 24 h recall | Yes | 6, 12 follow up |
| Harrigan 2016 [38] | SCT | One to one counselling, pedometer, scale, LEAN book—no details | Not reported | fruit and vegetables, weight, WC, % fat | FFQ | Yes | 6, 12 follow up |
| Hawkes 2013 [39] | ACM, MIT | Telephone delivered health coaching sessions; postcard prompts; pedometer, book with educational information on lifestyle behaviours | Not reported | Fibre, fruit and vegetables, alcohol, BMI | FFQ | Yes | 6, 12 follow up |
| Kanera 2017 [48] | SCT, TPB, SRT, IMC | Web-based programme with personalised feedback, online-evaluation session at the end | Not reported | Vegetable intake | Dutch standard questionnaire | Yes | 12 follow up |
| Kim 2011 [49] | TTM | Telephone counselling, workbook on diet and exercise, heart rate monitor | Readiness to change | DQI | 3-day recall | Yes | 3 |
| Koutoukidis 2018 [40] | SCT, CT | Group based intervention on eating pattern, balanced diet, portion size, food triggers, food labels and physical activity, study manual | Not reported | Healthy Eating Index | 24 h recall | Yes | 1.8, 5.5 follow up |
| Morey 2009 [41] | TTM, SCT | Paper based tailored workbook, newsletters, SCT telephone counselling, automated prompts, pedometer, exercise bands, table guide, record logs, workbook on diet and exercise | Not reported | Fruit and vegetables, weight, BMI | 24 h recall | Yes | 12 |
| Parekh 2018 [50] | SCT | Group education sessions on diet, exercise and cooking classes, information brochures—no details | Not reported | Fruit and vegetables | Validated tool for fruit and vegetables | Yes | 3 |
| Pierce 2007 [42] | SCT | Telephone counselling sessions, cooking classes, newsletters—no details | Not reported | EI, fruit and vegetables, fibre, weight, adherence | 24 h recall | No | 72 |
| Sheppard 2016 [51] | SCT, TPB, MIT | Group session—SCT, TBP, MIT telephone sessions, pedometers, notebook, resources—no details | Not reported | EI, fibre, weight, BMI, WC, HC, WHR | 4-day food diary | Yes | 3, 12 |
| Yun 2017 [52] | TTM | Educational workshop, individual telephone coaching, partnership with cancer survivors, resources—no details | Not reported | Vegetable intake | Validated questionnaire | Yes | 12 |
| Zick 2017 [53] | SCT | Individualised telephone counselling, self-monitoring check list | Not reported | EI, vegetable intake, BMI | 24 h recall | No | 3 |
| Zuniga 2019 [54] | TTM, MIT | Workshops with cooking demonstration, MIT telephone calls, newsletter, copies of lectures, TTM based sheet with goals | Not reported | EI, fibre, fruit and vegetables | Mediterranean diet questionnaire | No | 6 |
| BCT no. | BCTs/Authors | Blarigan 2020 [47] | Demark- Wahnefried 2006 [34] | Demark- Wahnefried 2007 [33] | Demark- Wahnefried 2014 [35] | Djuric 2002 [36] | Greenlee 2015 [37] | Gruenigen 2012 [43] | Harrigan 2016 [31] | Hawkes 2013 [39] | Kanera 2017 [48] | Kim 2011 [49] | Koutoukidis 2019 [40] | Morey 2009 [41] | Parekh 2018 [50] | Pierce 2007 [42] | Sheppard 2016 [51] | Yun 2017 [52] | Zick 2017 [53] | Zuniga 2019 [54] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1.1 | Goal setting (behaviour) | 1 | 1 | 1 | 1 | - | - | - | - | - | - | - | 1 | - | - | - | - | - | - | 1 |
| 1.2 | Problem solving | - | - | 1 | 1 | 1 | 1 | - | - | 1 | 1 | 1 | - | 1 | - | 1 | 1 | - | - | - |
| 1.3 | Goal setting (outcomes) | - | 1 | - | - | 1 | - | 1 | 1 | 1 | 1 | 1 | - | 1 | - | 1 | 1 | 1 | 1 | - |
| 1.4 | Action planning | 1 | - | - | - | - | 1 | - | - | 1 | 1 | - | 1 | - | - | - | - | - | - | - |
| 1.5 | Review behaviour goal(s) | - | 1 | - | - | 1 | - | - | - | 1 | 1 | - | 1 | - | - | - | - | - | - | - |
| 1.6 | Discrepancy between current behaviour and goal | - | 1 | 1 | - | - | 1 | - | - | - | 1 | - | - | - | - | - | - | - | - | - |
| 1.7 | Review outcome goal(s) | - | 1 | - | - | - | - | - | - | - | - | - | - | - | - | 1 | - | - | - | - |
| 1.8 | Commitment | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| 2.2 | Feedback on behaviour | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | 1 | - | 1 | - | - | - | - | - | - | |
| 2.3 | Self-monitoring of behaviour | - | - | 1 | 1 | 1 | - | - | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - |
| 2.7 | Feedback on outcome(s) of behaviour | - | 1 | - | - | - | - | - | - | - | - | - | - | 1 | - | 1 | - | - | - | - |
| 3.1 | Social support (unspecified) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 3.2 | Social support (practical) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 1 | - | 1 | - | - |
| 4.1 | Instruction on how to perform the behaviour | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 |
| 5.1 | Information on health consequences | - | - | - | - | - | 1 | - | - | 1 | 1 | 1 | 1 | - | 1 | - | - | - | - | 1 |
| 5.4 | Monitoring of emotional consequences | - | - | - | - | - | - | - | - | 1 | - | - | - | - | - | - | - | - | - | - |
| 5.6 | Information on emotional consequences | - | - | - | - | - | - | - | - | - | - | - | 1 | - | - | - | - | - | - | - |
| 6.1 | Demonstration of the behaviour | - | - | - | - | - | 1 | - | - | - | - | - | 1 | - | 1 | - | 1 | - | - | 1 |
| 6.2 | Social comparison | - | - | - | - | - | 1 | - | - | - | - | - | - | - | - | - | - | - | - | - |
| 7.1 | Prompts/cues | 1 | - | - | - | - | - | - | - | 1 | - | - | - | - | - | - | - | - | - | - |
| 7.3 | Reduce prompts/cues | - | - | - | - | 1 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| 8.1 | Behavioural practice/rehearsal | - | - | - | - | - | - | - | - | - | - | - | 1 | - | 1 | 1 | - | - | - | - |
| 8.7 | Graded task | - | - | - | - | - | - | - | - | - | 1 | 1 | 1 | - | - | - | - | - | - | - |
| 9.1 | Credible source | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 9.2 | Pros and cons | - | - | - | - | - | 1 | - | - | - | 1 | 1 | 1 | - | - | - | - | - | - | - |
| 10.7 | Self-incentive | - | - | - | - | - | - | - | - | - | - | 1 | 1 | - | - | - | - | - | - | - |
| 10.9 | Self-reward | - | - | - | - | - | - | - | - | - | - | 1 | 1 | - | - | - | - | - | - | - |
| 11.2 | Reduce negative emotions | - | - | - | - | - | - | - | - | 1 | - | - | - | - | - | - | - | - | - | - |
| 12.3 | Avoidance/reducing exposure to cues for the behaviour | - | - | - | - | 1 | - | - | - | - | - | 1 | 1 | - | - | - | - | - | - | - |
| 13.2 | Framing/reframing | - | - | - | - | - | - | - | - | - | - | - | 1 | - | - | - | - | - | - | - |
| Total number | 7 | 10 | 8 | 7 | 10 | 10 | 5 | 5 | 13 | 13 | 13 | 17 | 8 | 6 | 10 | 6 | 5 | 4 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sremanakova, J.; Sowerbutts, A.M.; Todd, C.; Cooke, R.; Burden, S. Systematic Review of Behaviour Change Theories Implementation in Dietary Interventions for People Who Have Survived Cancer. Nutrients 2021, 13, 612. https://doi.org/10.3390/nu13020612
Sremanakova J, Sowerbutts AM, Todd C, Cooke R, Burden S. Systematic Review of Behaviour Change Theories Implementation in Dietary Interventions for People Who Have Survived Cancer. Nutrients. 2021; 13(2):612. https://doi.org/10.3390/nu13020612
Chicago/Turabian StyleSremanakova, Jana, Anne Marie Sowerbutts, Chris Todd, Richard Cooke, and Sorrel Burden. 2021. "Systematic Review of Behaviour Change Theories Implementation in Dietary Interventions for People Who Have Survived Cancer" Nutrients 13, no. 2: 612. https://doi.org/10.3390/nu13020612