
The Association between Trajectories of Anthropometric Variables and Risk of Diabetes among Prediabetic Chinese

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Ethical Approval
2.3. Data Collection
2.4. Statistical Analysis
3. Results
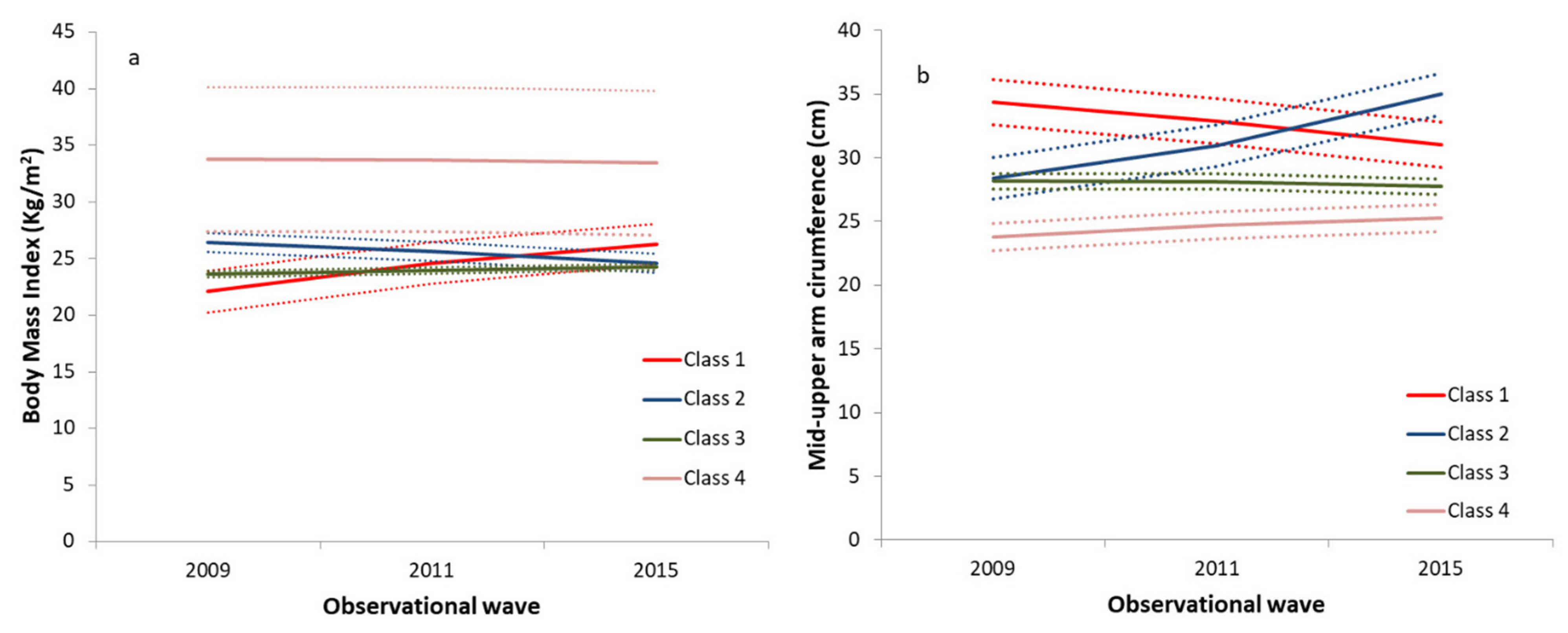
3.1. GMM for BMI and Upper Arm Circumference
3.2. Characteristics across Trajectory Groups
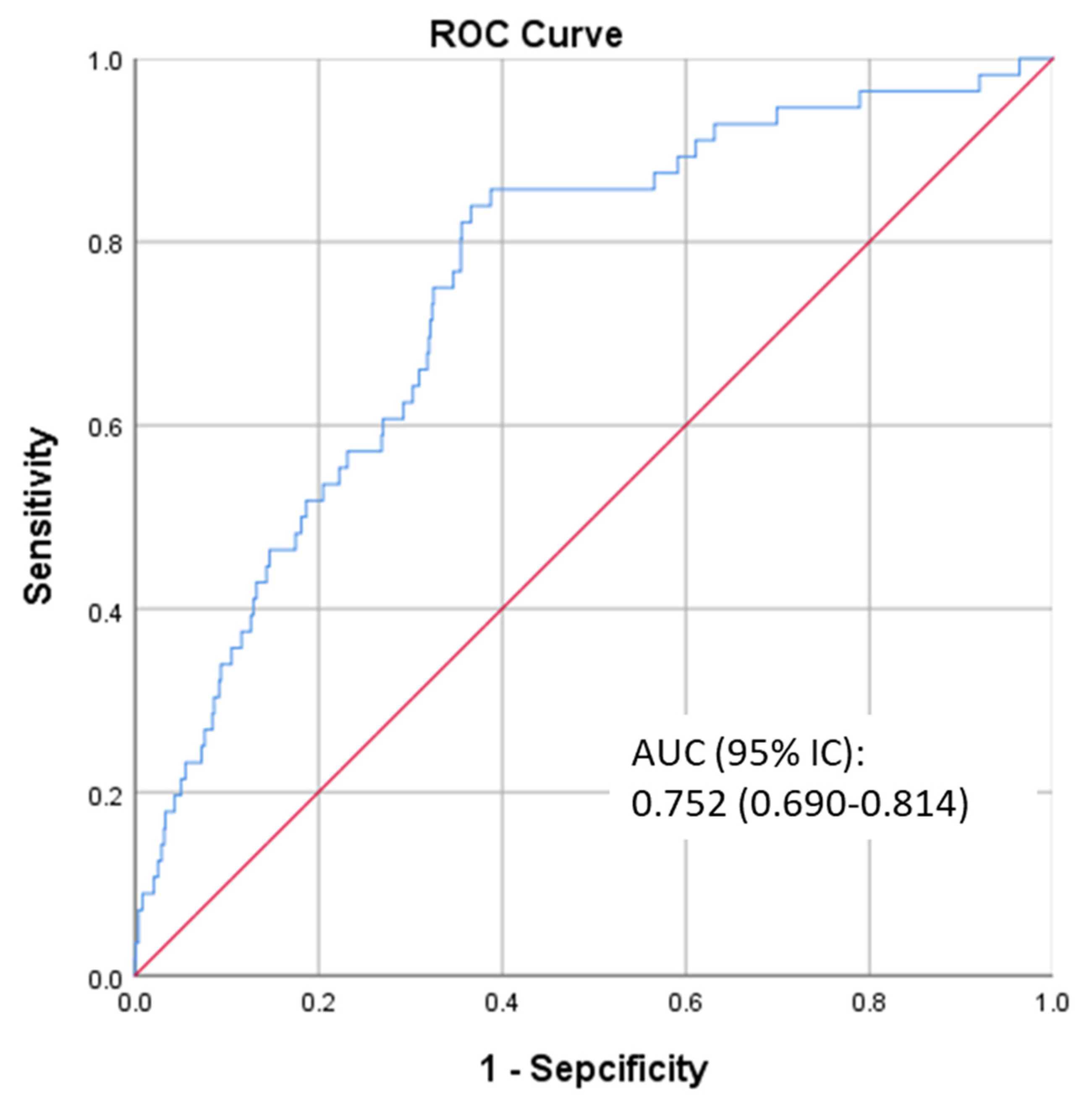
3.3. Logistic Regression and Receiver Operating Characteristic Curve for Diabetes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef]
- Rett, K.; Gottwald-Hostalek, U. Understanding prediabetes: Definition, prevalence, burden and treatment options for an emerging disease. Curr. Med. Res. Opin. 2019, 35, 1529–1534. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Teng, D.; Shi, X.; Qin, G.; Qin, Y.; Quan, H.; Shi, B.; Sun, H.; Ba, J.; Chen, B.; et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: National cross-sectional study. BMJ 2020, 369, m997. [Google Scholar] [CrossRef]
- Wang, L.; Gao, P.; Zhang, M.; Huang, Z.; Zhang, D.; Deng, Q.; Li, Y.; Zhao, Z.; Qin, X.; Jin, D.; et al. Prevalence and Ethnic Pattern of Diabetes and Prediabetes in China in 2013. JAMA 2017, 317, 2515–2523. [Google Scholar] [CrossRef]
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Zhang, P.; Wang, J.; Gregg, E.W.; Yang, W.; Gong, Q.; Li, H.; Li, H.; Jiang, Y.; An, Y.; et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: A 20-year follow-up study. Lancet 2008, 371, 1783–1789. [Google Scholar] [CrossRef]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Cheung, C.M.; Larsen, M.; Sharma, S.; Simó, R. Diabetic retinopathy. Nat. Rev. Dis. Primers 2016, 2, 16012. [Google Scholar] [CrossRef]
- Papatheodorou, K.; Banach, M.; Bekiari, E.; Rizzo, M.; Edmonds, M. Complications of Diabetes 2017. J. Diabetes Res. 2018, 2018, 3086167. [Google Scholar] [CrossRef]
- Brannick, B.; Dagogo-Jack, S. Prediabetes and Cardiovascular Disease: Pathophysiology and Interventions for Prevention and Risk Reduction. Endocrinol. Metab. Clin. N. Am. 2018, 47, 33–50. [Google Scholar] [CrossRef]
- Brannick, B.; Wynn, A.; Dagogo-Jack, S. Prediabetes as a toxic environment for the initiation of microvascular and macrovascular complications. Exp. Biol. Med. 2016, 241, 1323–1331. [Google Scholar] [CrossRef] [Green Version]
- Mutie, P.M.; Pomares-Millan, H.; Atabaki-Pasdar, N.; Jordan, N.; Adams, R.; Daly, N.L.; Tajes, J.F.; Giordano, G.N.; Franks, P.W. An investigation of causal relationships between prediabetes and vascular complications. Nat. Commun. 2020, 11, 4592. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Sheard, N.F.; Pi-Sunyer, X.; Daly, A.; Wylie-Rosett, J.; Kulkarni, K.; Clark, N.G. Weight management through lifestyle modification for the prevention and management of type 2 diabetes: Rationale and strategies. A statement of the American Diabetes Association, the North American Association for the Study of Obesity, and the American Society for Clinical Nutrition. Am. J. Clin. Nutr. 2004, 80, 257–263. [Google Scholar] [PubMed] [Green Version]
- Hsu, W.C.; Araneta, M.R.; Kanaya, A.M.; Chiang, J.L.; Fujimoto, W. BMI cut points to identify at-risk Asian Americans for type 2 diabetes screening. Diabetes Care 2015, 38, 150–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mi, B.; Wu, C.; Gao, X.; Wu, W.; Du, J.; Zhao, Y.; Wang, D.; Dang, S.; Yan, H. Long-term BMI change trajectories in Chinese adults and its association with the hazard of type 2 diabetes: Evidence from a 20-year China Health and Nutrition Survey. BMJ Open Diabetes Res. Care 2020, 8, e000879. [Google Scholar] [CrossRef] [PubMed]
- Peter, R.S.; Keller, F.; Klenk, J.; Concin, H.; Nagel, G. Body mass trajectories, diabetes mellitus, and mortality in a large cohort of Austrian adults. Medicine 2016, 95, e5608. [Google Scholar] [CrossRef]
- Lv, J.; Fan, B.; Wei, M.; Zhou, G.; Dayimu, A.; Wu, Z.; Su, C.; Zhang, T. Trajectories of early to mid-life adulthood BMI and incident diabetes: The China Health and Nutrition Survey. BMJ Open Diabetes Res. Care 2020, 8, e000972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, H.; Kawasaki, Y.; Kuwahara, K.; Nakagawa, T.; Honda, T.; Yamamoto, S.; Eguchi, M.; Kochi, T.; Nishihara, A.; Imai, T.; et al. Trajectories of body mass index and waist circumference before the onset of diabetes among people with prediabetes. Clin. Nutr. 2020, 39, 2881–2888. [Google Scholar] [CrossRef] [Green Version]
- Eaton-Evans, J. Nutritional Assessment: Anthropometry. In Encyclopedia of Human Nutrition, 3rd ed.; Caballero, B., Ed.; Academic Press: Waltham, MA, USA, 2013; pp. 227–232. [Google Scholar]
- Zhu, Y.; Lin, Q.; Zhang, Y.; Deng, H.; Hu, X.; Yang, X.; Yao, B. Mid-upper arm circumference as a simple tool for identifying central obesity and insulin resistance in type 2 diabetes. PLoS ONE 2020, 15, e231308. [Google Scholar] [CrossRef]
- Shi, J.; Yang, Z.; Niu, Y.; Zhang, W.; Li, X.; Zhang, H.; Lin, N.; Gu, H.; Wen, J.; Ning, G.; et al. Large mid-upper arm circumference is associated with metabolic syndrome in middle-aged and elderly individuals: A community-based study. BMC Endocr. Disord. 2020, 20, 78. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Zhai, F.Y.; Du, S.F.; Popkin, B.M. The China Health and Nutrition Survey, 1989–2011. Obes. Rev. 2014, 15 (Suppl. S1), 2–7. [Google Scholar] [CrossRef] [Green Version]
- China Health and Nutrition Survey. Available online: https://www.cpc.unc.edu/projects/china (accessed on 11 December 2020).
- China-Japan Friendship Hospital, the Ministry of Health. Available online: https://www.cpc.unc.edu/projects/china/data/datasets/Blood%20Collection%20Protocol_English.pdf (accessed on 11 December 2020).
- China Health And Nutrition Survey. Biomarkers Methods. Available online: https://www.cpc.unc.edu/projects/china/data/datasets/Biomarker_Methods.pdf (accessed on 11 December 2020).
- Yan, S.; Li, J.; Li, S.; Zhang, B.; Du, S.; Gordon-Larsen, P.; Adair, L.; Popkin, B. The expanding burden of cardiometabolic risk in China: The China Health and Nutrition Survey. Obes. Rev. 2012, 13, 810–821. [Google Scholar] [CrossRef] [Green Version]
- Working Group on Obesity in China. Guidelines on prevention and Control of Overweight and Obesity in Chinese Adults (Excerpts). Acta Nutr. Sin. 2004, 26, 1–4. [Google Scholar]
- Zhao, J.; Su, C.; Wang, H.; Wang, Z.; Wang, Y.; Zhang, B. Secular Trends in Energy and Macronutrient Intakes and Distribution among Adult Females (1991–2015): Results from the China Health and Nutrition Survey. Nutrients 2018, 10, 115. [Google Scholar] [CrossRef] [Green Version]
- China Health and Nutrition Survey. Available online: https://www.cpc.unc.edu/projects/china/about/design/datacoll (accessed on 11 December 2020).
- China Health and Nutrition Survey. Available online: https://www.cpc.unc.edu/projects/china/data/questionnaires/C09adult_Fin20090715.pdf (accessed on 11 December 2020).
- Li, F.; Lin, Q.; Li, M.; Chen, L.; Li, Y. The Association between Blood Pressure Trajectories and Risk of Cardiovascular Diseases among Non-Hypertensive Chinese Population: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 2909. [Google Scholar] [CrossRef] [PubMed]
- Andruff, H.; Carraro, N.; Thompson, A.; Gaudreau, P.; Louvet, B. Latent Class Growth Modelling: A Tutorial. Tutor. Quant. Methods Psychol. 2009, 5, 11–24. [Google Scholar] [CrossRef]
- Mattsson, M.; Maher, G.M.; Boland, F.; Fitzgerald, A.P.; Murray, D.M.; Biesma, R. Group-based trajectory modelling for BMI trajectories in childhood: A systematic review. Obes. Rev. 2019, 20, 998–1015. [Google Scholar] [CrossRef] [PubMed]
- Ames, M.E.; Wintre, M.G. Growth Mixture Modeling of Adolescent Body Mass Index Development: Longitudinal Patterns of Internalizing Symptoms and Physical Activity. J. Res. Adolesc. 2016, 26, 889–901. [Google Scholar] [CrossRef]
- Xian, H.; Scherrer, J.F.; Madden, P.A.; Lyons, M.J.; Tsuang, M.; True, W.R.; Eisen, S.A. Latent class typology of nicotine withdrawal: Genetic contributions and association with failed smoking cessation and psychiatric disorders. Psychol. Med. 2005, 35, 409–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubke, G.; Muthén, B.O. Performance of Factor Mixture Models as a Function of Model Size, Covariate Effects, and Class-Specific Parameters. Struct. Equ. Modeling A Multidiscip. J. 2007, 14, 26–47. [Google Scholar] [CrossRef]
- Lo, Y.; Mendell, N.R.; Rubin, D.B. Testing the number of components in a normal mixture. Biometrika 2001, 88, 767–778. [Google Scholar] [CrossRef]
- Petras, H.; Masyn, K. General Growth Mixture Analysis with Antecedents and Consequences of Change. In Handbook of Quantitative Criminology; Piquero, A.R., Weisburd, D., Eds.; Springer: New York, NY, USA, 2010; pp. 69–100. [Google Scholar]
- Lee, K.J.; Carlin, J.B. Multiple imputation for missing data: Fully conditional specification versus multivariate normal imputation. Am. J. Epidemiol. 2010, 171, 624–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spratt, M.; Carpenter, J.; Sterne, J.A.; Carlin, J.B.; Heron, J.; Henderson, J.; Tilling, K. Strategies for multiple imputation in longitudinal studies. Am. J. Epidemiol. 2010, 172, 478–487. [Google Scholar] [CrossRef]
- Dempster, A.P.; Laird, N.M.; Rubin, D.B. Maximum Likelihood from Incomplete Data via the EM Algorithm. J. R. Stat. Soc. Ser. B Methodol. 1977, 39, 1–38. [Google Scholar]
- Wong, M.S.; Gu, K.; Heng, D.; Chew, S.K.; Chew, L.S.; Tai, E.S. The Singapore impaired glucose tolerance follow-up study: Does the ticking clock go backward as well as forward? Diabetes Care. 2003, 26, 3024–3030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, J. Body composition and susceptibility to type 2 diabetes: An evolutionary perspective. Eur. J. Clin. Nutr. 2017, 71, 881–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malone, J.I.; Hansen, B.C. Does obesity cause type 2 diabetes mellitus (T2DM)? Or is it the opposite? Pediatr. Diabetes 2019, 20, 5–9. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Prevention or Delay of Type 2 Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S34–S39. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [Green Version]
- Chinese Diabetes Society. Guidelines for the prevention and control of type 2 diabetes in China (2017 Edition). Chin. J. Pract. Intern. Med. 2018, 38, 292–344. [Google Scholar]
- Lixandrão, M.E.; Ugrinowitsch, C.; Berton, R.; Vechin, F.C.; Conceição, M.S.; Damas, F.; Libardi, C.A.; Roschel, H. Magnitude of Muscle Strength and Mass Adaptations Between High-Load Resistance Training Versus Low-Load Resistance Training Associated with Blood-Flow Restriction: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 361–378. [Google Scholar] [CrossRef]
- Dai, X.; Zhai, L.; Chen, Q.; Miller, J.D.; Lu, L.; Hsue, C.; Liu, L.; Yuan, X.; Wei, W.; Ma, X.; et al. Two-year-supervised resistance training prevented diabetes incidence in people with prediabetes: A randomised control trial. Diabetes Metab. Res. Rev. 2019, 35, e3143. [Google Scholar] [CrossRef] [PubMed]
- Hull, H.R.; Thornton, J.; Wang, J.; Pierson, R.J.; Kaleem, Z.; Pi-Sunyer, X.; Heymsfield, S.; Albu, J.; Fernandez, J.R.; Vanitallie, T.B.; et al. Fat-free mass index: Changes and race/ethnic differences in adulthood. Int. J. Obes. Lond. 2011, 35, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menke, A.; Casagrande, S.; Geiss, L.; Cowie, C.C. Prevalence of and Trends in Diabetes among Adults in the United States, 1988–2012. JAMA 2015, 314, 1021–1029. [Google Scholar] [CrossRef] [Green Version]
- Heymsfield, S.B.; McManus, C.; Smith, J.; Stevens, V.; Nixon, D.W. Anthropometric measurement of muscle mass: Revised equations for calculating bone-free arm muscle area. Am. J. Clin. Nutr. 1982, 36, 680–690. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Models | Variable | OR (95% CI) | p |
|---|---|---|---|
| Model 1 | Class 3 BMI | Ref | - |
| Class 2 BMI | 4.219 (2.145–8.298) | 0.000 | |
| Class 1 BMI | - | - | |
| Class 4 BMI | 9.915 (2.630–37.379) | 0.001 | |
| Model 2 | Class 3 BMI | Ref | - |
| Class 2 BMI | 3.924 (1.959–7.861) | 0.000 | |
| Class 1 BMI | - | - | |
| Class 4 BMI | 10.050 (2.582–39.119) | 0.001 | |
| Model 3 | Class 3 BMI | Ref | - |
| Class 2 BMI | 3.634 (1.795–7.356) | 0.000 | |
| Class 1 BMI | - | 0.999 | |
| Class 4 BMI | 10.060 (2.510–40.316) | 0.001 | |
| Model 4 | Class 3 BMI | Ref | - |
| Class 2 BMI | 3.309 (1.626–6.735) | 0.001 | |
| Class 1 BMI | - | - | |
| Class 4 BMI | 7.103 (1.673–30.147) | 0.008 | |
| Model 5 | Class 3 BMI | Ref | - |
| Class 2 BMI | 3.139 (1.538–6.408) | 0.002 | |
| Class 1 BMI | - | - | |
| Class 4 BMI | 4.639 (0.967–22.259) | 0.055 | |
| Class 3 MUAC | Ref | - | |
| Class 2 MUAC | - | - | |
| Class 1 MUAC | 2.181 (0.733–6.491) | 0.161 | |
| Class 4 MUAC | 0.579 (0.198–1.689) | 0.317 |
| Models | Variable | OR (95% CI) | p |
|---|---|---|---|
| Model 1 | Class 3 MUAC | Ref | - |
| Class 2 MUAC | - | - | |
| Class 1 MUAC | 3.955 (1.597–9.799) | 0.003 | |
| Class 4 MUAC | 0.500 (0.178–1.403) | 0.188 | |
| Model 2 | Class 3 MUAC | Ref | - |
| Class 2 MUAC | - | - | |
| Class 1 MUAC | 4.336 (1.718–10.944) | 0.002 | |
| Class 4 MUAC | 0.466 (0.164–1.326) | 0.152 | |
| Model 3 | Class 3 MUAC | Ref | - |
| Class 2 MUAC | - | - | |
| Class 1 MUAC | 4.127 (1.614–10.557) | 0.003 | |
| Class 4 MUAC | 0.467 (0.164–1.333) | 0.155 | |
| Model 4 | Class 3 MUAC | Ref | - |
| Class 2 MUAC | - | - | |
| Class 1 MUAC | 3.085 (1.139–8.356) | 0.027 | |
| Class 4 MUAC | 0.554 (0.191–1.608) | 0.278 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, F.; Chen, L. The Association between Trajectories of Anthropometric Variables and Risk of Diabetes among Prediabetic Chinese. Nutrients 2021, 13, 4356. https://doi.org/10.3390/nu13124356
Li F, Chen L. The Association between Trajectories of Anthropometric Variables and Risk of Diabetes among Prediabetic Chinese. Nutrients. 2021; 13(12):4356. https://doi.org/10.3390/nu13124356
Chicago/Turabian StyleLi, Fang, and Lizhang Chen. 2021. "The Association between Trajectories of Anthropometric Variables and Risk of Diabetes among Prediabetic Chinese" Nutrients 13, no. 12: 4356. https://doi.org/10.3390/nu13124356