
Association of Obesity with the Risk of Hyperhomocysteinemia among the Chinese Community Residents: A Prospective Cohort Study in Shanghai, China

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Anthropometric and Other Measurements
2.3. Blood Sampling and Measurements
2.4. Statistical Analysis
2.5. Ethical Approval
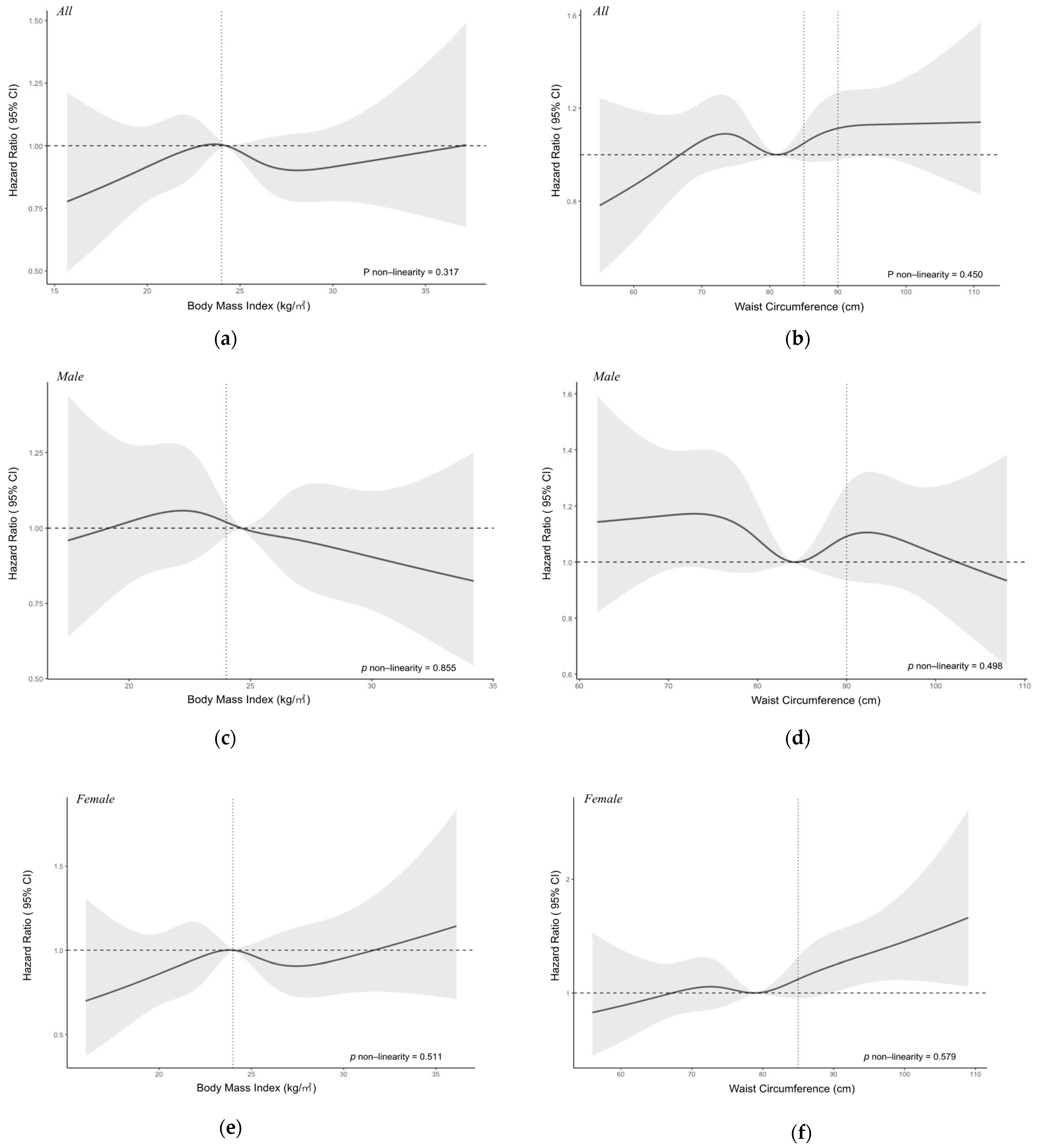
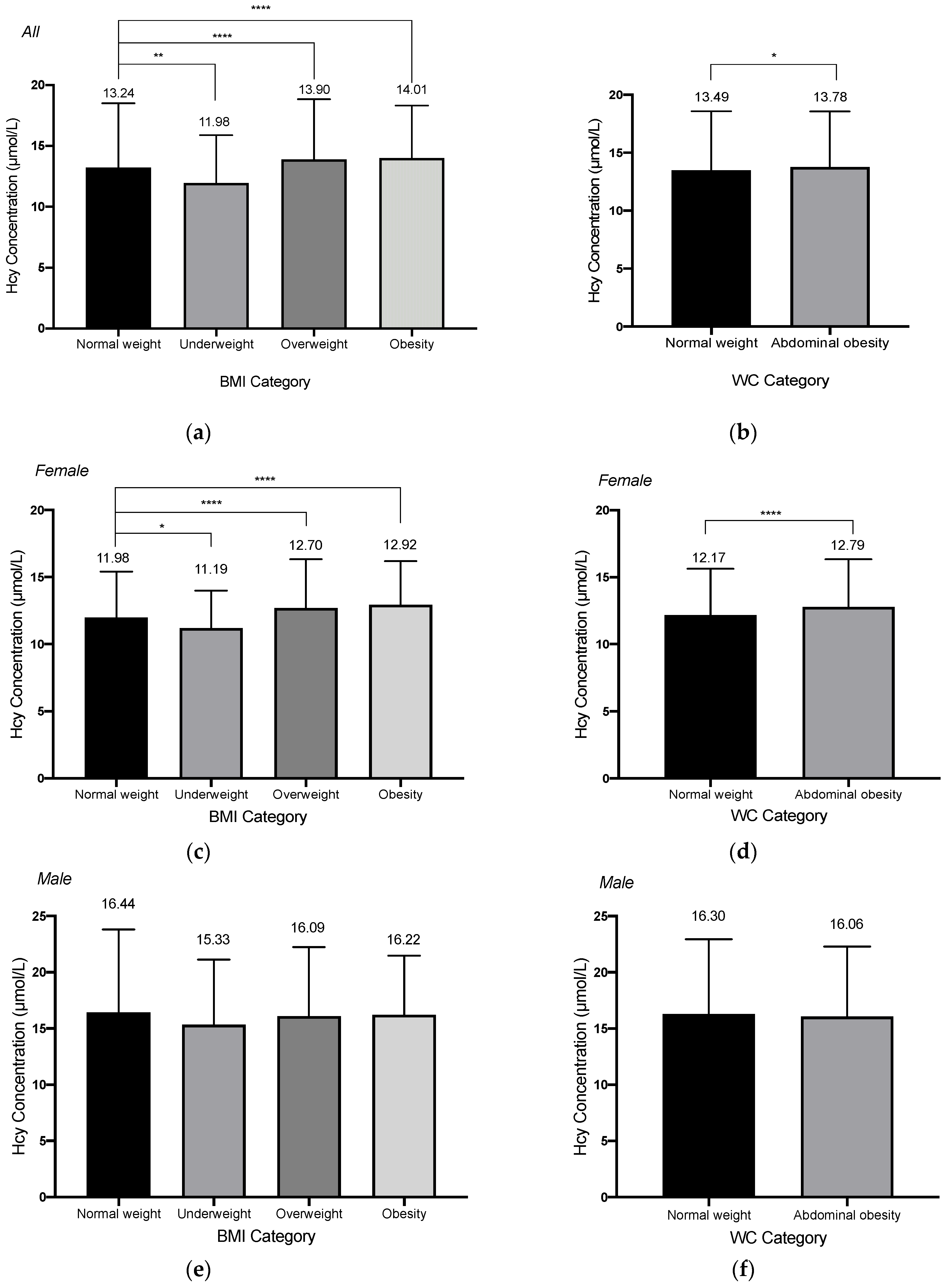
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CVD | cardiovascular disease |
| Hcy | homocysteine |
| HHcy | hyperhomocysteinemia |
| BMI | body mass index |
| WC | waist circumference |
| IR | insulin resistance |
References
- Faeh, D.; Chiolero, A.; Paccaud, F. Homocysteine as a risk factor for cardiovascular disease: Should we (still) worry about? Swiss. Med. Wkly. 2006, 136, 745–756. [Google Scholar]
- Liu, S.; Li, Y.; Zeng, X.; Wang, H.; Yin, P.; Wang, L.; Liu, Y.; Liu, J.; Qi, J.; Ran, S.; et al. Burden of Cardiovascular Diseases in China, 1990–2016: Findings From the 2016 Global Burden of Disease Study. JAMA Cardiol. 2019, 4, 342–352. [Google Scholar] [CrossRef]
- Kim, J.; Kim, H.; Roh, H.; Kwon, Y. Causes of hyperhomocysteinemia and its pathological significance. Arch. Pharm. Res. 2018, 41, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, F.; Van Gool, W.A. Hyperhomocysteinemia and Alzheimer’s disease: A systematic review. Arch. Gerontol. Geriatr. 2009, 48, 425–430. [Google Scholar] [CrossRef]
- Baszczuk, A.; Kopczyński, Z. Hyperhomocysteinemia in patients with cardiovascular disease. Postepy Hig. Med. Dosw. (Online) 2014, 68, 579–589. [Google Scholar] [CrossRef]
- Mandviwala, T.; Khalid, U.; Deswal, A. Obesity and Cardiovascular Disease: A Risk Factor or a Risk Marker? Curr. Atheroscler. Rep. 2016, 18, 21. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xue, H.; Sun, M.; Zhu, X.; Zhao, L.; Yang, Y. Prevention and control of obesity in China. Lancet Glob. Health 2019, 7, e1166–e1167. [Google Scholar] [CrossRef]
- Lavie, C.J.; Milani, R.V.; Ventura, H.O. Obesity and cardiovascular disease: Risk factor, paradox, and impact of weight loss. J. Am. Coll. Cardiol. 2009, 53, 1925–1932. [Google Scholar] [CrossRef] [Green Version]
- Din-Dzietham, R.; Liu, Y.; Bielo, M.V.; Shamsa, F. High blood pressure trends in children and adolescents in national surveys, 1963 to 2002. Circulation 2007, 116, 1488–1496. [Google Scholar] [CrossRef] [Green Version]
- Nakazato, M.; Maeda, T.; Takamura, N.; Wada, M.; Yamasaki, H.; Johnston, K.E.; Tamura, T. Relation of body mass index to blood folate and total homocysteine concentrations in Japanese adults. Eur. J. Nutr. 2011, 50, 581–585. [Google Scholar] [CrossRef] [Green Version]
- Jacques, P.F.; Bostom, A.G.; Wilson, P.W.; Rich, S.; Rosenberg, I.H.; Selhub, J. Determinants of plasma total homocysteine concentration in the Framingham Offspring cohort. Am. J. Clin. Nutr. 2001, 73, 613–621. [Google Scholar] [CrossRef] [Green Version]
- Elshorbagy, A.K.; Nurk, E.; Gjesdal, C.G.; Tell, G.S.; Ueland, P.M.; Nygård, O.; Tverdal, A.; Vollset, S.E.; Refsum, H. Homocysteine, cysteine, and body composition in the Hordaland Homocysteine Study: Does cysteine link amino acid and lipid metabolism? Am. J. Clin. Nutr. 2008, 88, 738–746. [Google Scholar] [CrossRef] [Green Version]
- Al-Bayyari, N.; Hamadneh, J.; Hailat, R.; Hamadneh, S. Total homocysteine is positively correlated with body mass index, waist-to-hip ratio, and fat mass among overweight reproductive women: A cross-sectional study. Nutr. Res. 2017, 48, 9–15. [Google Scholar] [CrossRef]
- Wang, Y.; Jiang, Y.; Wang, N.; Zhu, M.; Liu, X.; Wang, R.; Jiang, F.; Chen, Y.; Zhao, Q.; Zhao, G. Central But Not General Obesity Is Positively Associated with the Risk of Hyperhomocysteinemia in Middle-Aged Women. Nutrients 2019, 11, 1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Q.; Chen, B.; Wang, R.; Zhu, M.; Shao, Y.; Wang, N.; Liu, X.; Zhang, T.; Jiang, F.; Wang, W.; et al. Cohort profile: Protocol and baseline survey for the Shanghai Suburban Adult Cohort and Biobank (SSACB) study. BMJ Open 2020, 10, e035430. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Mi, J.; Shan, X.Y.; Wang, Q.J.; Ge, K.Y. Is China facing an obesity epidemic and the consequences? The trends in obesity and chronic disease in China. Int. J. Obes. 2007, 31, 177–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Standard of the People’s Republic of China. No. WS/T 428-2013: Criteria of Weight for Adults; Health Standard of the People’s Republic of China: Beijing, China, 2013. [Google Scholar]
- Jin, M.; Wang, F.; Uthup, M.; Szydlowska, M. Analytical performance of an enzymatic cycling method for total homocysteine measurement. Clin. Chim. Acta 2009, 399, 119–120. [Google Scholar] [CrossRef]
- Papandreou, D.; Rousso, I.; Makedou, A.; Arvanitidou, M.; Mavromichalis, I. Association of blood pressure, obesity and serum homocysteine levels in healthy children. Acta Paediatr. 2007, 96, 1819–1823. [Google Scholar] [CrossRef]
- Huemer, M.; Vonblon, K.; Födinger, M.; Krumpholz, R.; Hubmann, M.; Ulmer, H.; Simma, B. Total homocysteine, folate, and cobalamin, and their relation to genetic polymorphisms, lifestyle and body mass index in healthy children and adolescents. Pediatr. Res. 2006, 60, 764–769. [Google Scholar] [CrossRef] [Green Version]
- Vayá, A.; Rivera, L.; Hernández-Mijares, A.; de la Fuente, M.; Solá, E.; Romagnoli, M.; Alis, R.; Laiz, B. Homocysteine levels in morbidly obese patients: Its association with waist circumference and insulin resistance. Clin. Hemorheol. Microcirc. 2012, 52, 49–56. [Google Scholar] [CrossRef]
- Mojtabai, R. Body mass index and serum folate in childbearing age women. Eur. J. Epidemiol. 2004, 19, 1029–1036. [Google Scholar] [CrossRef]
- Papandreou, D.; Mavromichalis, I.; Makedou, A.; Rousso, I.; Arvanitidou, M. Reference range of total serum homocysteine level and dietary indexes in healthy Greek schoolchildren aged 6-15 years. Br. J. Nutr. 2006, 96, 719–724. [Google Scholar]
- Rhee, E.J.; Hwang, S.T.; Lee, W.Y.; Yoon, J.H.; Kim, B.J.; Kim, B.S.; Kang, J.H.; Lee, M.H.; Park, J.R.; Sung, K.C. Relationship between metabolic syndrome categorized by newly recommended by International Diabetes Federation criteria with plasma homocysteine concentration. Endocr. J. 2007, 54, 995–1002. [Google Scholar] [CrossRef] [Green Version]
- Mahabir, S.; Ettinger, S.; Johnson, L.; Baer, D.J.; Clevidence, B.A.; Hartman, T.J.; Taylor, P.R. Measures of adiposity and body fat distribution in relation to serum folate levels in postmenopausal women in a feeding study. Eur. J. Clin. Nutr. 2008, 62, 644–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.B.; Georgiades, A. Changes in body composition predict homocysteine changes and hyperhomocysteinemia in Korea. J. Korean Med. Sci. 2013, 28, 1015–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laha, A.; Majumder, A.; Singh, M.; Tyagi, S.C. Connecting homocysteine and obesity through pyroptosis, gut microbiome, epigenetics, peroxisome proliferator-activated receptor γ, and zinc finger protein 407. Can. J. Physiol. Pharmacol. 2018, 96, 971–976. [Google Scholar] [CrossRef] [PubMed]
- Komorniak, N.; Szczuko, M.; Kowalewski, B.; Stachowska, E. Nutritional Deficiencies, Bariatric Surgery, and Serum Homocysteine Level: Review of Current Literature. Obes. Surg. 2019, 29, 3735–3742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roust, L.R.; DiBaise, J.K. Nutrient deficiencies prior to bariatric surgery. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 138–144. [Google Scholar] [CrossRef]
- Welch, G.N.; Loscalzo, J. Homocysteine and atherothrombosis. N. Engl. J. Med. 1998, 338, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Després, J.P. Abdominal obesity as important component of insulin-resistance syndrome. Nutrition 1993, 9, 452–459. [Google Scholar]
- Misra, A.; Alappan, N.K.; Vikram, N.K.; Goel, K.; Gupta, N.; Mittal, K.; Bhatt, S.; Luthra, K. Effect of supervised progressive resistance-exercise training protocol on insulin sensitivity, glycemia, lipids, and body composition in Asian Indians with type 2 diabetes. Diabetes Care 2008, 31, 1282–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keshel, T.E.; Coker, R.H. Exercise Training and Insulin Resistance: A Current Review. J. Obes. Weight Loss Ther. 2015, S5, 003. [Google Scholar] [CrossRef]
- DeFronzo, R.A. Insulin resistance, lipotoxicity, type 2 diabetes and atherosclerosis: The missing links. The Claude Bernard Lecture 2009. Diabetologia 2010, 53, 1270–1287. [Google Scholar] [CrossRef] [Green Version]
- Björck, J.; Hellgren, M.; Råstam, L.; Lindblad, U. Associations between serum insulin and homocysteine in a Swedish population-a potential link between the metabolic syndrome and hyperhomocysteinemia: The Skaraborg project. Metabolism 2006, 55, 1007–1013. [Google Scholar] [CrossRef]
- Carbone, S.; Canada, J.M.; Billingsley, H.E.; Siddiqui, M.S.; Elagizi, A.; Lavie, C.J. Obesity paradox in cardiovascular disease: Where do we stand? Vasc Health Risk Manag. 2019, 15, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Elagizi, A.; Kachur, S.; Lavie, C.J.; Carbone, S.; Pandey, A.; Ortega, F.B.; Milani, R.V. An Overview and Update on Obesity and the Obesity Paradox in Cardiovascular Diseases. Prog. Cardiovasc. Dis. 2018, 61, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Tiwari, M.; Tiwari, R.K. Hyperhomocysteinemia: Impact on Neurodegenerative Diseases. Basic Clin. Pharmacol. Toxicol. 2015, 117, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Meng, H.; Li, Y.; Zhang, W.; Zhao, Y.; Niu, X.; Guo, J. The relationship between cognitive impairment and homocysteine in a B12 and folate deficient population in China: A cross-sectional study. Medicine 2019, 98, e17970. [Google Scholar] [CrossRef]
- Wu, H.; Wang, B.; Ban, Q.; Chen, L.; Yan, D.; Yu, Y.; Song, Y.; Liu, C.; Cao, J.; Zhang, J.; et al. Association of total homocysteine with blood pressure in a general population of Chinese adults: A cross-sectional study in Jiangsu province, China. BMJ Open 2018, 8, e021103. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Wang, Q.; An, P.; Du, Y.; Zhao, J.; Song, A.; Huang, G. Relationship between folate, vitamin B(12), homocysteine, transaminase and mild cognitive impairment in China: A case-control study. Int. J. Food Sci. Nutr. 2020, 71, 315–324. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Hhcy | Non-Hhcy | Total | p Value | |
|---|---|---|---|---|
| n = 2104 | n = 6848 | n = 8952 | ||
| Age (years) | <0.001 | |||
| 20–39 | 41 (1.95) | 521 (7.61) | 562 (6.28) | |
| 40–49 | 95 (4.52) | 867 (12.66) | 962 (10.75) | |
| 50–59 | 524 (24.90) | 2556 (37.32) | 3080 (34.41) | |
| 60–69 | 1145 (54.42) | 2497 (36.46) | 3642 (40.68) | |
| ≥70 | 299 (14.21) | 407 (5.94) | 706 (7.89) | |
| Body mass index (kg/m2) | <0.001 | |||
| Normal Weight | 829 (39.51) | 3168 (46.34) | 3997 (44.74) | |
| Underweight | 22 (1.05) | 182 (2.66) | 204 (2.28) | |
| Overweight | 902 (42.99) | 2597 (37.99) | 3499 (39.16) | |
| Obese | 345 (16.44) | 889 (13.00) | 1234 (13.81) | |
| Waist circumference (cm) | 0.017 | |||
| Normal | 1464 (69.58) | 4951 (72.30) | 6415 (71.66) | |
| Abdominal obesity | 640 (30.42) | 1897 (27.70) | 2537 (28.34) | |
| Gender | <0.001 | |||
| Male | 1268 (60.27) | 1552 (22.66) | 2820 (31.50) | |
| Female | 836 (39.73) | 5296 (77.34) | 6132 (68.50) | |
| Education Degree | <0.001 | |||
| Middle School or Below | 1264 (60.54) | 3456 (51.30) | 4720 (53.48) | |
| High School or Above | 824 (39.46) | 3281 (48.70) | 4105 (46.52) | |
| Cardiovascular comorbidities | <0.001 | |||
| Ye | 1024 (48.67) | 2489 (36.35) | 3513 (39.24) | |
| No | 1080 (51.33) | 4359 (63.65) | 5439 (60.76) | |
| Alcohol Drinking | <0.001 | |||
| Yes | 448 (21.29) | 629 (9.19) | 1077 (12.03) | |
| No | 1656 (78.71) | 6219 (90.81) | 7875 (87.97) | |
| Smoking | <0.001 | |||
| Yes | 727 (34.55) | 903 (13.19) | 1630 (18.21) | |
| No | 1377 (65.45) | 5945 (86.81) | 7322 (81.79) | |
| Tea Drinking | <0.001 | |||
| Yes | 846 (40.21) | 1531 (22.36) | 2377 (26.55) | |
| No | 1258 (59.79) | 5317 (77.64) | 6575 (73.45) | |
| Retirement | <0.001 | |||
| Yes | 1613 (76.66) | 4308 (62.91) | 5921 (66.14) | |
| No | 491 (23.34) | 2540 (37.09) | 3031 (33.86) | |
| Exercise | <0.001 | |||
| Yes | 816 (38.78) | 2302 (33.62) | 3118 (34.83) | |
| No | 1288 (61.22) | 4546 (66.38) | 5834 (65.17) |
| Normal Weight 18.5 ≤ BMI ≤ 23.9 | Underweight BMI < 18.5 | Overweight 24.0 ≤ BMI ≤ 27.9 | Obesity BMI ≥ 28 | Total | |||||
|---|---|---|---|---|---|---|---|---|---|
| Cases/n | HR (ref) | Cases/n | HR (95% CI) | Cases/n | HR (95% CI) | Cases/n | HR (95% CI) | ||
| Allsubjects a | 829/3997 | 22/204 | 902/3499 | 829/3997 | 8934 | ||||
| Model 1 | 1.0 | 0.57 (0.37 to 0.87) ** | 1.07 (0.98 to 1.18) | 1.10 (0.97 to 1.24) | |||||
| Model 2 | 1.0 | 0.64 (0.42 to 0.98) * | 1.02 (0.93 to 1.12) | 1.06 (0.93 to 1.20) | |||||
| Model 3 | 1.0 | 0.63 (0.40 to 0.96) * | 0.99 (0.89 to 1.10) | 1.04 (1.91 to 1.19) | |||||
| Model 4 | 1.0 | 0.64 (0.42 to 0.99) * | 0.95 (0.85 to 1.07) | 0.97 (0.82 to 1.15) | |||||
| Gender b | |||||||||
| Male | 503/1131 | 1.0 | 13/49 | 0.82 (0.46 to 1.45) | 560/1237 | 0.92 (0.80 to 1.07) | 190/407 | 0.88 (0.70 to 1.11) | 2814 |
| Female | 326/2866 | 1.0 | 9/165 | 0.49 (0.29 to 0.95) * | 342/2262 | 1.01 (0.84 to 1.20) | 155/827 | 1.08 (0.82 to 1.40) | 6120 |
| Age(years)c | |||||||||
| 20–39 | 21/331 | 1.0 | 1/44 | 0.66 (0.33 to 4.93) | 13/126 | 0.69 (0.33 to 1.43) | 6/60 | 1.40 (0.55 to 3.50) | 561 |
| 40–49 | 37/533 | 1.0 | 1/21 | 2.47 (0.32 to 19.05) | 37/302 | 1.10 (0.61 to 1.97) | 20/106 | 0.94 (0.37 to 2.39) | 962 |
| 50–59 | 184/1355 | 1.0 | 5/69 | 0.78 (0.32 to 1.93) | 229/1205 | 0.95 (0.75 to 1.19) | 103/440 | 1.01 (0.72 to 1.41) | 3069 |
| 60–69 | 464/1476 | 1.0 | 9/52 | 0.69 (0.35 to 1.35) | 500/1583 | 0.89 (0.77 to 1.04) | 169/525 | 0.81 (0.64 to 1.02) | 3636 |
| ≥70 | 123/302 | 1.0 | 12/18 | 0.52 (0.21 to 1.28) | 123/283 | 1.03 (0.75 to 1.41) | 47/103 | 1.13 (0.71 to 1.82) | 706 |
| CVD comorbiditiesb | |||||||||
| Yes | 325/1159 | 1.0 | 3/29 | 0.32 (0.10 to 1.02) | 456/1566 | 0.84 (0.71 to 0.98) * | 238/754 | 0.86 (0.69 to 1.08) | 3508 |
| No | 504/2838 | 1.0 | 19/175 | 0.80 (0.50 to 1.29) | 446/1933 | 1.04 (0.90 to 1.23) | 107/480 | 1.10 (0.83 to 1.46) | 5426 |
| Normal Weight | Abdominal Obesity | Total | |||
|---|---|---|---|---|---|
| WC < 85.00 cm for Females | WC ≥ 85.00 cm for Females | ||||
| WC < 90.00 cm for Males | WC ≥ 90.00 cm for Males | ||||
| Cases/n | HR (95%CI) | Cases/n | HR (95%CI) | ||
| All Subjects a | 1464/6415 | 640/2537 | 8952 | ||
| Model 1 | 1.0 | 1.05 (0.96 to 1.15) | |||
| Model 2 | 1.0 | 1.11 (1.01 to 1.21) * | |||
| Model 3 | 1.0 | 1.10 (0.99 to 1.21) | |||
| Model 4 | 1.0 | 1.11 (0.99 to 1.24) | |||
| Gender b | |||||
| Male | 925/2051 | 1.0 | 343/769 | 1.09 (0.93 to 1.27) | 2820 |
| Female | 539/4364 | 1.0 | 297/1768 | 1.09 (0.91 to 1.30) | 6132 |
| Age (years) c | |||||
| 20–39 | 35/489 | 1.0 | 6/73 | 0.93 (0.38 to 2.25) | 562 |
| 40–49 | 69/783 | 1.0 | 26/179 | 1.20 (0.60 to 2.42) | 962 |
| 50–59 | 372/2274 | 1.0 | 152/806 | 1.19 (0.59 to 2.43) | 3080 |
| 60–69 | 793/2422 | 1.0 | 352/1220 | 1.15 (0.98 to 1.34) | 3642 |
| ≥70 | 195/447 | 1.0 | 104/259 | 0.93 (0.67 to 1.28) | 706 |
| CVD comorbiditiesb | |||||
| Yes | 623/2098 | 1.0 | 401/1415 | 1.08 (0.93 to 1.27) | 3513 |
| No | 841/4317 | 1.0 | 239/1122 | 1.26 (1.05 to 1.51) * | 5439 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiang, Y.; Zhao, Q.; Wang, N.; Yu, Y.; Wang, R.; Zhang, Y.; Cui, S.; Wu, Y.; Liu, X.; Jiang, Y.; et al. Association of Obesity with the Risk of Hyperhomocysteinemia among the Chinese Community Residents: A Prospective Cohort Study in Shanghai, China. Nutrients 2021, 13, 3648. https://doi.org/10.3390/nu13103648
Xiang Y, Zhao Q, Wang N, Yu Y, Wang R, Zhang Y, Cui S, Wu Y, Liu X, Jiang Y, et al. Association of Obesity with the Risk of Hyperhomocysteinemia among the Chinese Community Residents: A Prospective Cohort Study in Shanghai, China. Nutrients. 2021; 13(10):3648. https://doi.org/10.3390/nu13103648
Chicago/Turabian StyleXiang, Yu, Qi Zhao, Na Wang, Yuting Yu, Ruiping Wang, Yue Zhang, Shuheng Cui, Yiling Wu, Xing Liu, Yonggen Jiang, and et al. 2021. "Association of Obesity with the Risk of Hyperhomocysteinemia among the Chinese Community Residents: A Prospective Cohort Study in Shanghai, China" Nutrients 13, no. 10: 3648. https://doi.org/10.3390/nu13103648