
Effects of Water Restriction and Supplementation on Cognitive Performances and Mood among Young Adults in Baoding, China: A Randomized Controlled Trial (RCT)


Abstract
:1. Introduction
2. Materials and Methods
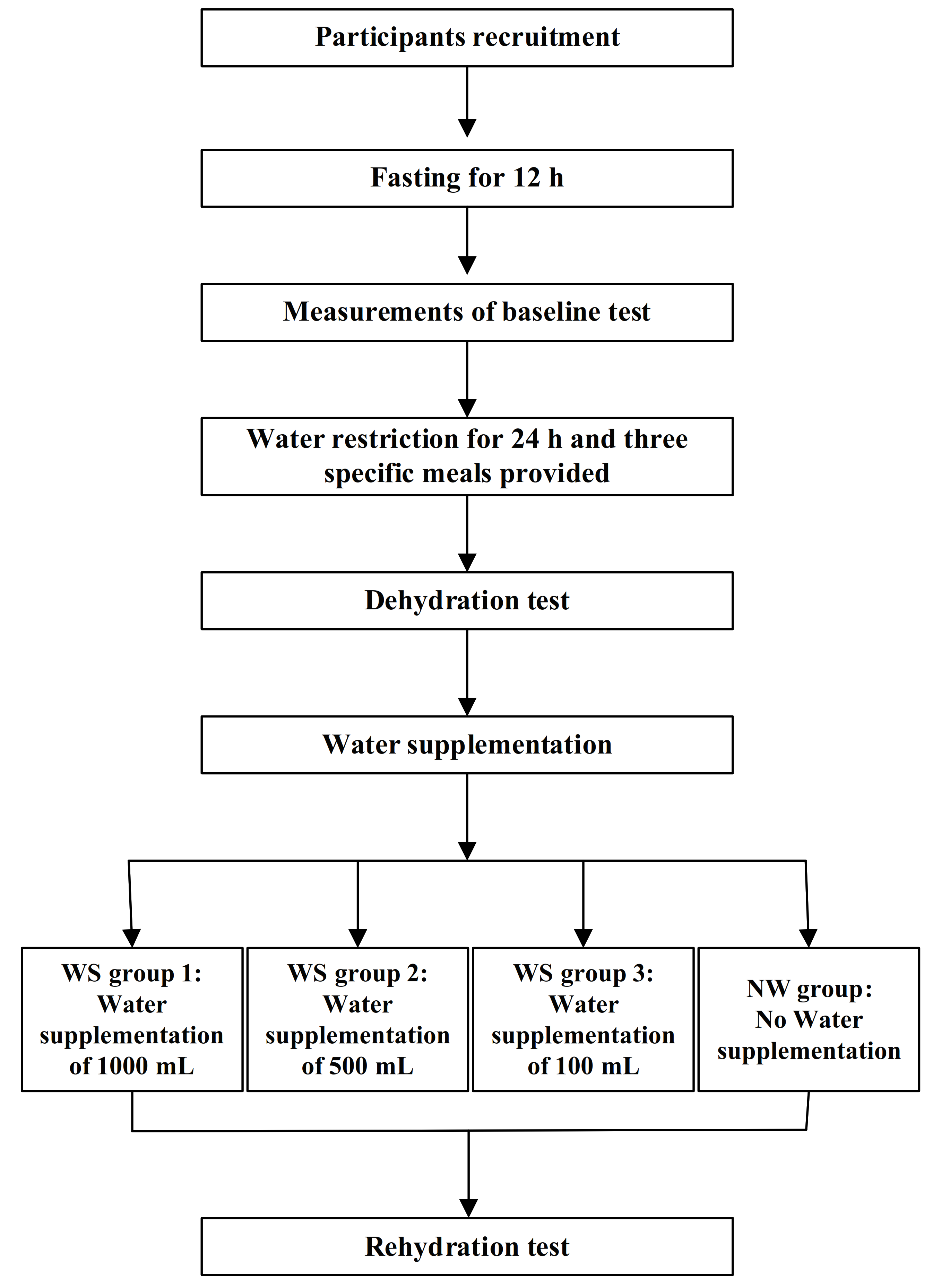
2.1. Study Design
2.2. Participants
2.3. Interventions
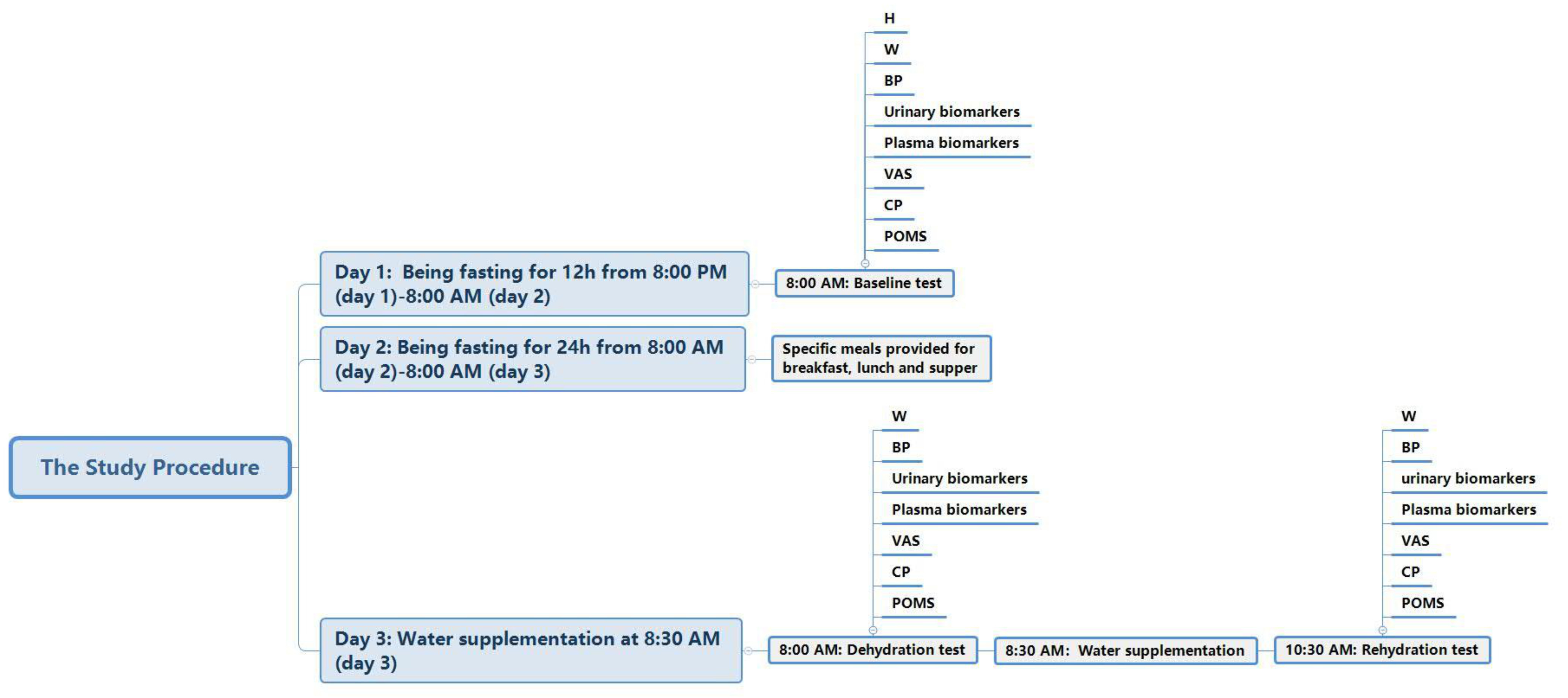
2.4. Study Procedure
2.5. Outcomes
2.6. Randomization and Blinding
2.7. Sample Size Calculation
2.8. Ethical Standards
2.9. Anthropometric Measurements
2.10. Temperature and Humidity of the Environment
2.11. Assessment of Total Water Intake (TWI)
2.12. Urinary and Plasma Biomarkers
2.13. Hydration Status
2.14. Visual Analogue Scales (VAS) for Subjective Sensation
2.15. Profile of Mood States (POMS)
2.16. Cognitive Performance (CP)
2.17. Vocabulary Test
2.18. Similarities Test
2.19. Symbol Search Test
2.20. Operation Span Test
2.21. Portrait Memory Test
2.22. Statistical Analyses
3. Results
3.1. Characteristics of the Participants
3.2. Temperature and Humidity
3.3. Amounts of TWI
3.4. Thirst, Urinary, and Plasma Biomarkers
3.5. Effects of Dehydration and Rehydration on POMS
3.6. Effects of Dehydration and Rehydration on Cognitive Performance (CP)

{kind=link}
{kind=link}
| Baseline Test | Dehydration Test | t | p | Rehydration Test | Interaction | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | F | p | |||
| Thirst | 5.2 ± 2.1 | 4.7 ± 2.5 | 4.3 ± 2.6 | 4.5 ± 2.7 | 4.6 ± 2.3 | 6.4 ± 2.1 | 6.4 ± 2.1 | 6.2 ± 2.8 | 6.0 ± 2.4 | 6.3 ± 2.3 | −6.758 | <0.001 | 1.7 ± 1.7 #† | 3.5 ± 2.1 † | 4.7 ± 2.4 † | 6.4 ± 2.1 | 19.847 | <0.001 |
| Urinary Biomarkers | ||||||||||||||||||
| Osmolality (mOsm/kg) * | 840 ± 261 | 829 ± 170 | 786 ± 205 | 830 ± 234 | 822 ± 217 | 1111 ± 130 | 1079 ± 114 | 1093 ± 71 | 1092 ± 78 | 1094 ± 101 | −11.221 | <0.001 | 453 ± 273 #† | 888 ± 352 † | 921 ± 265 † | 1131 ± 72 | 23.697 | <0.001 |
| Na (mmol/L) * | 167 ± 64 | 167 ± 69 | 170 ± 60 | 160 ± 61 | 166 ± 62 | 228 ± 44 | 225 ± 37 | 254 ± 31 | 241 ± 37 | 236 ± 39 | −8.784 | <0.001 | 72 ± 55 # | 151 ± 65 | 195 ± 87 | 199 ± 59 | 9.875 | <0.001 |
| K (mmol/L) | 43.3 ± 21.7 | 42.6 ± 20.2 | 40.3 ± 22.0 | 50.5 ± 22.6 | 44.1 ± 21.5 | 46.3 ± 23.7 | 44.4 ± 17.0 | 40.5 ± 19.3 | 42.5 ± 16.6 | 43.5 ± 19.1 | 0.219 | 0.828 | 34.1 ± 23.0 # | 67.8 ± 35.0 | 58.3 ± 21.6 | 83.5 ± 21.1 | 11.986 | <0.001 |
| Cl (mmol/L) * | 148 ± 52 | 156 ± 55 | 153 ± 58 | 154 ± 58 | 153 ± 55 | 196 ± 46 | 196 ± 45 | 210 ± 43 | 202 ± 38 | 201 ± 43 | −6.029 | <0.001 | 91 ± 67 # | 187 ± 80 | 218 ± 87 | 253 ± 71 | 11.354 | <0.001 |
| Ca (mmol/L) * | 2.61 ± 1.25 | 2.96 ± 1.84 | 2.38 ± 1.44 | 2.74 ± 1.86 | 2.68 ± 1.60 | 7.20 ± 3.48 | 6.84 ± 3.19 | 7.02 ± 2.57 | 6.76 ± 2.65 | 6.96 ± 2.96 | −13.321 | <0.001 | 1.54 ± 1.58 # | 2.81 ± 1.59 | 2.94 ± 1.69 | 3.71 ± 1.05 | 2.617 | 0.057 |
| Phosphorus (mmol/L) | 39.94 ± 19.50 | 32.85 ± 10.93 | 36.90 ± 16.10 | 37.08 ± 15.58 | 36.67 ± 15.72 | 43.01 ± 17.41 | 40.08 ± 11.62 | 36.63 ± 10.78 | 37.17 ± 11.98 | 39.35 ± 13.28 | −1.398 | 0.166 | 9.64 ± 6.93 # | 23.30 ± 12.75 | 18.34 ± 7.46 | 27.79 ± 10.87 | 7.916 | <0.001 |
| Mg (mmol/L) * | 3.49 ± 1.49 | 3.00 ± 1.41 | 3.10 ± 1.15 | 3.77 ± 2.60 | 3.33 ± 1.73 | 7.07 ± 3.20 | 6.03 ± 3.36 | 7.58 ± 3.53 | 6.44 ± 3.56 | 6.77 ± 3.39 | −8.457 | <0.001 | 1.41 ± 0.90 # | 2.62 ± 1.55 | 3.05 ± 1.37 | 3.83 ± 1.58 | 3.063 | 0.033 |
| pH | 6.38 ± 0.36 | 6.35 ± 0.37 | 6.39 ± 0.37 | 6.36 ± 0.33 | 6.37 ± 0.35 | 6.40 ± 0.42 | 6.30 ± 0.34 | 6.39 ± 0.21 | 6.44 ± 0.29 | 6.38 ± 0.33 | −0.293 | 0.770 | 6.1 ± 0.3 | 6.2 ± 0.4 | 6.1 ± 0.2 | 6.1 ± 0.2 | 1.041 | 0.380 |
| USG | 1.025 ± 0.006 | 1.025 ± 0.004 | 1.024 ± 0.006 | 1.026 ± 0.005 | 1.025 ± 0.005 | 1.028 ± 0.004 | 1.029 ± 0.003 | 1.029 ± 0.004 | 1.029 ± 0.002 | 1.029 ± 0.003 | −5.019 | <0.001 | 1.014 ± 0.009 †# | 1.025 ± 0.008 | 1.026 ± 0.007 | 1.029 ± 0.004 | 13.475 | <0.001 |
| Hydration statuses (%) * | ||||||||||||||||||
| Dehydration | 13 (65.0) | 12 (60.0) | 9 (50.0) | 10 (55.6) | 20 (100.0) | 20 (100.0) | 18 (100.0) | 18 (100.0) | 3 (15.0) #† | 15 (75.0) † | 14 (77.8) | 18 (100.0) | 35.714 | <0.001 | ||||
| Middle hydration | 5 (25.0) | 8 (40.0) | 8 (44.4) | 5 (27.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 46.973 | <0.001 | 4 (20.0) | 0 (0.0) | 2 (11.1) | 0 (0.0) | ||||
| Optimal hydration | 2 (10.0) | 0 (0.0) | 1 (5.6) | 3 (16.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 13 (65.0) | 5 (25.0) | 2 (11.1) | 0 (0.0) | ||||||
| Baseline Test | Dehydration Test | t | p | Rehydration Test | Interaction | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS GROUP 3 (n = 18) | NW group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | F | p | |||
| Osmolality (mOsm/kg) * | 293 ± 5 | 293 ± 7 | 294 ± 5 | 293 ± 4 | 293 ± 5 | 297 ± 6 | 298 ± 4 | 296 ± 5 | 296 ± 4 | 297 ± 5 | −6.157 | <0.001 | 292 ± 4 † | 294 ± 4 | 293 ± 5 | 295 ± 6 | 2.035 | 0.117 |
| Na (mmol/L) | 140 ± 2 | 140 ± 1 | 140 ± 1 | 140 ± 2 | 140 ± 1 | 140 ± 1 | 140 ± 2 | 141 ± 1 | 138 ± 11 | 140 ± 6 | 0.716 | 0.476 | 138 ± 2 | 139 ± 2 | 139 ± 2 | 140 ± 2 | 2.128 | 0.104 |
| K (mmol/L) | 4.4 ± 0.6 | 4.5 ± 0.6 | 4.6 ± 1.0 | 4.6 ± 0.6 | 4.51 ± 0.70 | 4.4 ± 0.4 | 4.5 ± 0.4 | 4.4 ± 0.4 | 4.5 ± 0.5 | 4.43 ± 0.40 | 0.842 | 0.403 | 4.2 ± 0.3 | 4.3 ± 0.3 | 4.3 ± 0.3 | 4.5 ± 0.4 | 0.796 | 0.500 |
| Cl (mmol/L) | 105 ± 2 | 104 ± 2 | 105 ± 1 | 104 ± 2 | 104 ± 2 | 104 ± 2 | 105 ± 1 | 105 ± 2 | 103 ± 8 | 104 ± 4 | 0.844 | 0.402 | 102 ± 2# | 103 ± 1 | 104 ± 2 | 104 ± 3 | 2.816 | 0.045 |
| Ca (mmol/L) | 2.41 ± 0.08 | 2.40 ± 0.08 | 2.42 ± 0.08 | 2.42 ± 0.07 | 2.41 ± 0.08 | 2.45 ± 0.08 | 2.42 ± 0.08 | 2.46 ± 0.09 | 2.44 ± 0.09 | 2.44 ± 0.08 | −3.477 | 0.001 | 2.47 ± 0.08 | 2.46 ± 0.06 | 2.48 ± 0.09 | 2.47 ± 0.08 | 0.647 | 0.588 |
| Phosphorus (mmol/L) | 1.30 ± 0.17 | 1.30 ± 0.21 | 1.28 ± 0.14 | 1.32 ± 0.15 | 1.30 ± 0.17 | 1.37 ± 0.16 | 1.30 ± 0.20 | 1.26 ± 0.12 | 1.32 ± 0.15 | 1.31 ± 0.16 | −0.657 | 0.513 | 1.25 ± 0.07 | 1.21 ± 0.13 | 1.16 ± 0.14 | 1.24 ± 0.09 | 0.366 | 0.778 |
| Mg (mmol/L) | 0.88 ± 0.06 | 0.88 ± 0.05 | 0.90 ± 0.07 | 0.89 ± 0.05 | 0.89 ± 0.06 | 0.86 ± 0.05 | 0.87 ± 0.06 | 0.89 ± 0.06 | 0.89 ± 0.04 | 0.88 ± 0.05 | 1.691 | 0.095 | 0.83 ± 0.06# | 0.86 ± 0.06 | 0.87 ± 0.04 | 0.89 ± 0.05 | 3.071 | 0.033 |
| Creatine (mmol/L) * | 62 ± 13 | 61 ± 11 | 66 ± 15 | 66 ± 10 | 63 ± 12 | 62 ± 12 | 61 ± 12 | 65 ± 15 | 63 ± 12 | 62 ± 13 | 2.803 | 0.006 | 58 ± 13 | 59 ± 13 | 62 ± 17 | 60 ± 10 | 0.822 | 0.486 |
| Nitrogen (mmol/L)* | 4.41 ± 1.09 | 4.53 ± 1.31 | 4.54 ± 0.99 | 4.09 ± 1.19 | 4.40 ± 1.14 | 6.63 ± 1.39 | 6.58 ± 1.45 | 6.34 ± 0.98 | 5.91 ± 1.06 | 6.38 ± 1.25 | −20.576 | <0.001 | 5.76 ± 1.34 | 6.03 ± 1.43 | 5.85 ± 1.03 | 5.76 ± 1.08 | 8.878 | <0.001 |
| Baseline Test | Dehydration Test | t | p | Rehydration Test | Interaction | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | F | p | |||
| Tension | 3.8 ± 2.5 | 3.4 ± 2.4 | 4.1 ± 3.5 | 3.7 ± 2.3 | 3.8 ± 2.7 | 3.7 ± 3.3 | 3.1 ± 3.0 | 4.3 ± 5.0 | 4.2 ± 3.7 | 3.8 ± 3.8 | −0.146 | 0.885 | 1.8 ± 2.2 † | 2.0 ± 2.9 † | 2.4 ± 3.4 | 3.8 ± 4.4 | 1.043 | 0.379 |
| Anger | 1.8 ± 2.9 | 2.5 ± 3.6 | 2.5 ± 3.0 | 1.9 ± 1.9 | 2.2 ± 2.9 | 2.1 ± 3.6 | 2.1 ± 3.0 | 2.7 ± 3.7 | 2.7 ± 3.8 | 2.4 ± 3.5 | −0.579 | 0.564 | 0.9 ± 2.2 † | 2.0 ± 3.4 | 1.9 ± 3.6 | 2.4 ± 3.7 | 0.663 | 0.578 |
| Fatigue * | 3.2 ± 2.9 | 4.3 ± 4.1 | 4.3 ± 2.6 | 2.8 ± 2.2 | 3.6 ± 3.1 | 4.8 ± 3.9 | 4.9 ± 4.8 | 4.7 ± 3.5 | 4.8 ± 4.7 | 4.8 ± 4.2 | −2.976 | 0.004 | 3.1 ± 2.4 † | 3.5 ± 3.1 † | 4.1 ± 3.2 | 6.9 ± 4.3 † | 6.302 | 0.001 |
| Depression | 1.8 ± 2.3 | 2.4 ± 2.6 | 2.4 ± 3.4 | 2.7 ± 2.8 | 2.3 ± 2.7 | 2.5 ± 3.5 | 2.5 ± 3.4 | 3.1 ± 3.7 | 3.1 ± 4.1 | 2.8 ± 3.6 | −1.325 | 0.189 | 1.3 ± 2.3 † | 2.5 ± 3.6 | 1.8 ± 3.7 † | 2.8 ± 3.5 | 1.673 | 0.180 |
| Confusion | 3.2 ± 2.0 | 3.6 ± 2.3 | 4.1 ± 3.2 | 3.3 ± 2.1 | 3.5 ± 2.4 | 3.3 ± 2.8 | 3.6 ± 3.3 | 3.9 ± 3.4 | 3.9 ± 2.8 | 3.7 ± 3.0 | −0.547 | 0.586 | 2.5 ± 2.4 | 2.8 ± 3.3 | 2.4 ± 3.4 † | 3.5 ± 2.7 | 0.638 | 0.593 |
| Vigor * | 12.9 ± 4.9 | 10.4 ± 4.7 | 11.7 ± 4.0 | 12.2 ± 3.2 | 11.8 ± 4.3 | 11.0 ± 5.5 | 8.9 ± 4.4 | 7.6 ± 6.0 | 9.4 ± 4.4 | 9.2 ± 5.2 | 6.479 | <0.001 | 11.3 ± 5.3 | 9.2 ± 4.1 | 9.6 ± 4.6 † | 7.7 ± 3.8 | 3.188 | 0.029 |
| Esteem-related affect * | 8.2 ± 3.2 | 7.4 ± 3.1 | 7.9 ± 2.9 | 7.9 ± 2.0 | 7.8 ± 2.8 | 7.1 ± 3.8 | 6.6 ± 3.0 | 5.8 ± 3.2 | 5.9 ± 3.3 | 6.4 ± 3.3 | 5.828 | <0.001 | 6.8 ± 3.6 | 6.7 ± 3.2 | 5.9 ± 3.3 | 5.7 ± 3.4 | 0.237 | 0.871 |
| TMD * | 92.6 ± 13.8 | 98.3 ± 15.6 | 97.8 ± 14.8 | 94.2 ± 11.2 | 95.7 ± 13.9 | 98.5 ± 19.0 | 100.9 ± 17.1 | 105.4 ± 22.0 | 103.4 ± 21.0 | 101.8 ± 19.6 | −3.699 | <0.001 | 91.9 ± 12.7 † | 96.9 ± 17.3 † | 97.2 ± 19.1 | 106.7 ± 20.1 | 2.849 | 0.043 |
| Baseline Test | Dehydration Test | t | p | Rehydration Test | Interaction | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | F | p | |||
| Vocabulary test | 55 ± 4 | 56 ± 7 | 58 ± 7 | 57 ± 3 | 57 ± 6 | 55 ± 4 | 56 ± 7 | 58 ± 7 | 57 ± 3 | 57 ± 6 | - | - | 55 ± 4 | 56 ± 7 | 58 ± 7 | 57 ± 3 | - | - |
| Similarities test | 50 ± 8 | 49 ± 7 | 48 ± 8 | 51 ± 7 | 50 ± 7 | 50 ± 8 | 49 ± 7 | 48 ± 8 | 51 ± 7 | 50 ± 7 | - | - | 50 ± 8 | 49 ± 7 | 48 ± 8 | 51 ± 7 | - | - |
| Symbol search test * | 37 ± 6 | 39 ± 5 | 39 ± 7 | 36 ± 5 | 38 ± 6 | 43 ± 6 | 44 ± 3 | 45 ± 8 | 42 ± 8 | 43 ± 6 | −8.956 | <0.001 | 45 ± 6 † | 47 ± 5 † | 47 ± 9 | 41 ± 7 | 2.859 | 0.043 |
| Operation span test * | 9 ± 3 | 9 ± 2 | 7 ± 4 | 8 ± 3 | 8 ± 3 | 10 ± 2 | 10 ± 3 | 8 ± 4 | 9 ± 3 | 9 ± 3 | −3.909 | <0.001 | 11 ± 2 † | 11 ± 3 † | 10 ± 3 | 9 ± 3 | 3.463 | 0.021 |
| Portrait memory test * | 33 ± 9 | 37 ± 7 | 32 ± 7 | 34 ± 8 | 34 ± 8 | 25 ± 8 | 27 ± 9 | 25 ± 11 | 29 ± 10 | 27 ± 10 | 6.782 | <0.001 | 29 ± 7 † | 28 ± 10 | 27 ± 10 | 28 ± 7 | 1.496 | 0.223 |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jequier, E.; Constant, F. Water as an essential nutrient: The physiological basis of hydration. Eur. J. Clin. Nutr. 2010, 64, 115–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popkin, B.M.; D’Anci, K.E.; Rosenberg, I.H. Water, hydration, and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- El-Sharkawy, A.M.; Sahota, O.; Lobo, D.N. Acute and chronic effects of hydration status on health. Nutr. Rev. 2015, 732, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Watso, J.C.; Farquhar, W.B. Hydration Status and Cardiovascular Function. Nutrients 2019, 11, 1866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goulet, E.D.B.; Mélançon, M.O.; Lafrenière, D.; Paquin, J.; Maltais, M.; Morais, J.A. Impact of Mild Hypohydration on Muscle Endurance, Power and Strength in Healthy, Active Older Men. J. Strength. Cond. Res. 2018, 32, 3405–3415. [Google Scholar] [CrossRef]
- Manz, F.; Wentz, A. The importance of good hydration for the prevention of chronic diseases. Nutr. Rev. 2005, 63, S2–S5. [Google Scholar] [CrossRef]
- Ganio, M.S.; Armstrong, L.E.; Casa, D.J.; McDermott, B.P.; Lee, E.C.; Yamamoto, L.M.; Marzano, S.; Lopez, R.M.; Jimenez, L.; Le Bellego, L. Mild dehydration impairs cognitive performance and mood of men. Br. J. Nutr. 2011, 106, 1535–1543. [Google Scholar] [CrossRef] [Green Version]
- Stachenfeld, N.S.; Leone, C.A.; Mitchell, E.S.; Freese, E.; Harkness, L. Water intake reverses dehydration associated impaired executive function in healthy young women. Physiol. Behav. 2018, 185, 103–111. [Google Scholar] [CrossRef]
- Baker, L.B.; Conroy, D.E.; Kenney, W.L. Dehydration impairs vigilance-related attention in male basketball players. Med. Sci. Sport. Exerc. 2007, 39, 976–983. [Google Scholar] [CrossRef] [Green Version]
- Goodman, S.P.J.; Moreland, A.T.; Marino, F.E. The effect of active hypohydration on cognitive function: A systematic review and meta-analysis. Physiol. Behav. 2019, 204, 297–308. [Google Scholar] [CrossRef]
- Adam, G.E.; Arter, R.R.; Cheuvront, S.N.; Merullo, D.J.; Castellani, J.W.; Lieberman, H.R.; Sawka, M.N. Hydration effects on cognitive performance during military tasks in temperate and cold environments. Physiol. Behav. 2008, 93, 748–756. [Google Scholar] [CrossRef]
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The effects of acute exercise on cognitive performance: A meta-analysis. Brain. Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef] [Green Version]
- Caldwell, H.G.; Coombs, G.B.; Howe, C.A.; Hoiland, R.L.; Patrician, A.; Lucas, S.J.E.; Ainslie, P.N. Evidence for temperature-mediated regional increases in cerebral blood flow during exercise. J. Physiol. 2020, 598, 1459–1473. [Google Scholar] [CrossRef]
- Hogervorst, E.; Riedel, W.; Jeukendrup, A.; Jolles, J. Cognitive performance after strenuous physical exercise. Percept. Mot. Skill. 1996, 83, 479–488. [Google Scholar] [CrossRef]
- Mazlomi, A.; Golbabaei, F.; Farhang, D.S.; Abbasinia, M.; Mahmoud, K.S.; Ansari, M.; Hosseini, M. The influence of occupational heat exposure on cognitive performance and blood level of stress hormones: A field study report. Int. J. Occup. Saf. Ergon. 2017, 23, 431–439. [Google Scholar] [CrossRef]
- Szinnai, G.; Schachinger, H.; Arnaud, M.J.; Linder, L.; Keller, U. Effect of water deprivation on cognitive-motor performance in healthy men and women. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005, 289, R275–R280. [Google Scholar] [CrossRef] [Green Version]
- Petri, N.M.; Dropulic, N.; Kardum, G. Effects of voluntary fluid intake deprivation on mental and psychomotor performance. Croat. Med. J. 2006, 47, 855–861. [Google Scholar]
- Zhang, N.; Du, S.; Zhang, J.; Ma, G. Effects of Dehydration and Rehydration on Cognitive Performance and Mood among Male College Students in Cangzhou, China: A Self-Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 1891. [Google Scholar] [CrossRef] [Green Version]
- Edmonds, C.J.; Crosbie, L.; Fatima, F.; Hussain, M.; Jacob, N.; Gardner, M. Dose-response effects of water supplementation on cognitive performance and mood in children and adults. Appetite 2017, 108, 464–470. [Google Scholar] [CrossRef]
- Edmonds, C.J.; Jeffes, B. Does having a drink help you think? 6–7-Year-old children show improvements in cognitive performance from baseline to test after having a drink of water. Appetite 2009, 53, 469–472. [Google Scholar] [CrossRef]
- Robinson, K.; Staples, V.; Appleton, K.; Sheffield, D. Illness perceptions and obesity. Obesity related illness representations vary according to BMI category. Appetite 2014, 83, 355. [Google Scholar] [CrossRef]
- Perry, C.S.; Rapinett, G.; Glaser, N.S.; Ghetti, S. Hydration status moderates the effects of drinking water on children’s cognitive performance. Appetite 2015, 95, 520–527. [Google Scholar] [CrossRef]
- Edmonds, C.J.; Crombie, R.; Ballieux, H.; Gardner, M.R.; Dawkins, L. Water consumption, not expectancies about water consumption, affects cognitive performance in adults. Appetite 2013, 60, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhang, N.; Wang, Y.; Liang, S.; Liu, S.; Du, S.; Xu, Y.; He, H.; Cai, H.; Ma, G. Drinking patterns and hydration biomarkers among young adults with different levels of habitual total drinking fluids intake in Baoding, Hebei Province, China: A cross sectional study. BMC Public Health 2020, 20, 468. [Google Scholar] [CrossRef]
- Standardization Administration of China. National Food Safety Standard GB 5009.3–2016: Determination of Moisture in Foods; China Standard Press: Beijing, China, 2016. [Google Scholar]
- Bar-David, Y.; Urkin, J.; Kozminsky, E. The effect of voluntary dehydration on cognitive functions of elementary school children. Acta Paediatr. 2005, 94, 1667–1673. [Google Scholar] [CrossRef]
- Perrier, E.T.; Buendia-Jimenez, I.; Vecchio, M.; Armstrong, L.E.; Tack, I.; Klein, A. Twenty-four-hour urine osmolality as a physiological index of adequate water intake. Dis. Markers 2015, 2015, 231063. [Google Scholar] [CrossRef] [Green Version]
- Stookey, J.D.; Brass, B.; Holliday, A.; Arieff, A. What is the cell hydration status of healthy children in the USA? Preliminary data on urine osmolality and water intake. Public Health Nutr. 2012, 15, 2148–2156. [Google Scholar] [CrossRef] [Green Version]
- Hill, A.J.; Blundell, J.E. Nutrients and behaviour: Research strategies for the investigation of taste characteristics, food preferences, hunger sensations and eating patterns in man. J. Psychiatr. Res. 1982, 17, 203–212. [Google Scholar] [CrossRef]
- Short, M.; Lack, L.; Wright, H. Does subjective sleepiness predict objective sleep propensity? Sleep 2010, 33, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhang, N.; Du, S.; He, H.; Xu, Y.; Cai, H.; Guo, X.; Ma, G. The Effects of Hydration Status on Cognitive Performances among Young Adults in Hebei, China: A Randomized Controlled Trial (RCT). Int. J. Environ. Res. Public Health 2018, 15, 1477. [Google Scholar] [CrossRef] [Green Version]
- Grove, J.R.; Prapavessis, H. Preliminary evidence for the reliability and validity of an abbreviated profile of mood states. Int. J. Sport Psychol. 1992, 23, 93–109. [Google Scholar]
- Xu, S.; Wu, Z. The Construction of “The Clinical Memory Test”. Acta Psychol. Sin. 1986, 18, 102–110. [Google Scholar]
- Lichtenberger, E.O.; Kaufman, A.S. Essentials of WAIS-IV Assessment; John Wiley: Hoboken, NJ, USA, 2012. [Google Scholar]
- Conway, A.R.A.; Kane, M.J.; Bunting, M.F.; Hambrick, D.Z.; Wilhelm, O.; Engle, R.W. Working memory span tasks: A methodological review and user’s guide. Psychon. Bull. Rev. 2005, 12, 769–786. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, H.R. The effects of ginseng, ephedrine, and caffeine on cognitive performance, mood and energy. Nutr. Rev. 2001, 59, 91–102. [Google Scholar] [CrossRef]
- Nehlig, A. Is caffeine a cognitive enhancer? J. Alzheimers Dis. 2010, 20, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Pross, N.; Demazieres, A.; Girard, N.; Barnouin, R.; Santoro, F.; Chevillotte, E.; Klein, A.; Le Bellego, L. Influence of progressive fluid restriction on mood and physiological markers of dehydration in women. Br. J. Nutr. 2013, 109, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Ely, B.R.; Sollanek, K.J.; Cheuvront, S.N.; Liberman, H.R.; Kenefick, R.W. Hypohydration and acute thermal stress affect mood state but not cognition or dynamic postural balance. Eur. J. Appl. Physiol. 2013, 113, 1027–1034. [Google Scholar] [CrossRef]
- Irwin, C.; Campagnolo, N.; Iudakhina, E.R.; Cox, G.; Desbrow, B. Effects of acute exercise, dehydration and rehydration on cognitive function in well-trained athletes. J. Sports Sci. 2017, 3, 1. [Google Scholar]
- Patsalos, O.C.; Thoma, V. Water supplementation after dehydration improves judgment and decision-making performance. Psychol. Res. 2020, 84, 1223–1234. [Google Scholar] [CrossRef] [Green Version]
- Edmonds, C.J.; Crombie, R.; Gardner, M.R. Subjective thirst moderates changes in speed of responding associated with water consumption. Front. Hum. Neurosci. 2020, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chard, A.N.; Trinies, V.; Edmonds, C.J.; Sogore, A.; Freeman, M.C. The impact of water consumption on hydration and cognition among schoolchildren: Methods and results from a crossover trial in rural Mali. PLoS ONE 2019, 14, e210568. [Google Scholar] [CrossRef] [Green Version]
- Young, H.A.; Benton, D. The use of moderated mediated analysis to study the influence of hypo-hydration on working memory. Nutr. Hosp. 2016, 33, 71–75. [Google Scholar] [CrossRef] [Green Version]
- Cian, C.; Barraud, P.A.; Melin, B.; Raphel, C. Effects of fluid ingestion on cognitive function after heat stress or exercise-induced dehydration. Int. J. Psychophysiol. 2010, 42, 243–251. [Google Scholar] [CrossRef]
- Wittbrodt, M.T.; Melinda, M.S. Dehydration Impairs Cognitive Performance: A Meta-analysis. Med. Sci. Sports Exerc. 2018, 1, 2360–2368. [Google Scholar] [CrossRef]
- Heuvel, A.M.J.; Haberley, B.J.; Hoyle, D.J.R.; Taylor, N.A.S.; Croft, R.J. The independent influences of heat strain and dehydration upon cognition. Eur. J. Appl. Physiol. 2017, 117, 1025–1037. [Google Scholar] [CrossRef]
- Drozdowska, A.; Falkenstein, M.; Jendrusch, G.; Platen, P.; Luecke, T.; Kersting, M.; Jansen, K. Water Consumption during a School Day and Children’s Short-Term Cognitive Performance: The CogniDROP Randomized Intervention Trial. Nutrients 2020, 12, 1297. [Google Scholar] [CrossRef]
- Backes, T.; Fitzgerald, K. Fluid consumption, exercise, and cognitive performance. Biol. Sport 2016, 33, 291–296. [Google Scholar] [CrossRef] [Green Version]
- McCartney, D.; Desbrow, B.; Irwin, C. The Effect of Fluid Intake Following Dehydration on Subsequent Athletic and Cognitive Performance: A Systematic Review and Meta-analysis. Sports Med. Open 2017, 3, 13. [Google Scholar] [CrossRef] [Green Version]


| Baseline Test | Dehydration Test | t | p | Rehydration Test | Interaction | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total | WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | F | p | |||
| Age (year) | 21 ± 1 | 21 ± 1 | 21 ± 1 | 21 ± 1 | 21 ± 1 | 21 ± 1 | 21 ± 1 | 21 ± 1 | 21 ± 1 | 21 ± 1 | - | - | 21 ± 1 | 21 ± 1 | 21 ± 1 | 21 ± 1 | - | - |
| Height (cm) | 168.3 ± 8.1 | 167.1 ± 7.8 | 163.5 ± 7.9 | 165.9 ± 9.0 | 166.3 ± 8.2 | 168.3 ± 8.1 | 167.1 ± 7.8 | 163.5 ± 7.9 | 165.9 ± 9.0 | 166.3 ± 8.2 | - | - | 168.3 ± 8.1 | 167.1 ± 7.8 | 163.5 ± 7.9 | 165.9 ± 9.0 | - | - |
| Weight (kg) * | 63.7 ± 9.0 | 64.4 ± 13.8 | 58.9 ± 11.9 | 60.8 ± 10.2 | 62.1 ± 11.4 | 63.4 ± 9.2 | 63.9 ± 13.8 | 58.5 ± 11.8 | 60.4 ± 10.2 | 61.6 ± 11.4 | 6.985 | <0.001 | 63.9 ± 9.2 | 64.0 ± 13.8 | 58.5 ± 11.7 | 60.2 ± 10.1 | 1.102 | 0.354 |
| BMI (kg/m2) * | 22.6 ± 3.6 | 22.9 ± 3.8 | 21.9 ± 3.4 | 22.0 ± 2.3 | 22.4 ± 3.3 | 22.5 ± 3.6 | 22.7 ± 3.7 | 21.8 ± 3.3 | 21.8 ± 2.3 | 22.2 ± 3.3 | 7.162 | <0.001 | 22.7 ± 3.7 | 22.8 ± 3.7 | 21.8 ± 3.3 | 21.8 ± 2.3 | 0.544 | 0.654 |
| Systolic pressure (mmHg) * | 112 ± 14 | 110 ± 12 | 109 ± 13 | 110 ± 11 | 110 ± 12 | 109 ± 10 | 107 ± 9 | 109 ± 11 | 107 ± 8 | 108 ± 10 | 3.142 | 0.002 | 113 ± 12 | 109 ± 10 | 110 ± 11 | 108 ± 11 | 0.842 | 0.475 |
| Diastolic pressure (mmHg) * | 67 ± 8 | 67 ± 11 | 63 ± 9 | 66 ± 7 | 65 ± 8 | 88 ± 7 | 86 ± 10 | 87 ± 9 | 86 ± 8 | 87 ± 8 | 30.874 | <0.001 | 67 ± 8 | 64 ± 8 | 64 ± 9 | 65 ± 8 | 0.334 | 0.800 |
| Indoors | Outdoors | |||
|---|---|---|---|---|
| Temperature (°C) | Humidity (%) | Temperature (°C) | Humidity (%) | |
| First study day | 20.7 | 59 | 22.0 | 64 |
| Second study day | 20.5 | 57 | 20.4 | 55 |
| Third study day | 20.5 | 63 | 19.8 | 61 |
| Average | 20.6 | 60 | 20.7 | 60 |
| WS Group 1 (n = 20) | WS Group 2 (n = 20) | WS Group 3 (n = 18) | NW Group (n = 18) | Total (n = 76) | F | p | |
|---|---|---|---|---|---|---|---|
| Water from food | 988 ± 253 | 870 ± 187 | 934 ± 210 | 884 ± 185 | 920 ± 212 | 1.264 | 0.293 |
| Water from breakfast | 79 ± 35 | 100 ± 40 | 82 ± 25 | 80 ± 26 | 85 ± 33 | 1.771 | 0.160 |
| Water from lunch | 463 ± 123 | 410 ± 99 | 448 ± 102 | 449 ± 101 | 442 ± 107 | 0.900 | 0.446 |
| Water from supper | 446 ± 130 | 361 ± 99 | 404 ± 122 | 355 ± 107 | 392 ± 119 | 2.568 | 0.055 |
| Water from stable food | 413 ± 146 | 367 ± 114 | 381 ± 111 | 352 ± 72 | 379 ± 115 | 1.001 | 0.398 |
| Water from dishes | 575 ± 167 | 503 ± 115 | 552 ± 137 | 532 ± 127 | 541 ± 138 | 0.965 | 0.414 |
| 24 h urinary biomarker | |||||||
| Urine volume | 939 ± 210 | 893 ± 187 | 934 ± 207 | 830 ± 136 | 900 ± 189 | 1.314 | 0.276 |
| Voids | 4 ± 1 | 4 ± 1 | 4 ± 1 | 4 ± 1 | 4 ± 1 | 0.949 | 0.422 |
| 24 h urine osmolality | 973 ± 101 | 985 ± 104 | 948 ± 104 | 997 ± 83 | 976 ± 98 | 0.840 | 0.476 |
| 24 h-Na (mmol/L) | 261 ± 35 | 247 ± 42 | 261 ± 33 | 267 ± 33 | 259 ± 36 | 1.015 | 0.391 |
| 24 h-K (mmol/L) | 43.10 ± 10.99 | 45.27 ± 13.63 | 40.68 ± 9.71 | 51.08 ± 12.83 | 44.99 ± 12.28 | 2.523 | 0.064 |
| 24 h-Cl (mmol/L) | 233 ± 30 | 213 ± 42 | 227 ± 31 | 223 ± 31 | 224 ± 34 | 1.165 | 0.329 |
| 24 h-Ca (mmol/L) | 5.11 ± 2.28 | 5.18 ± 1.71 | 4.80 ± 1.56 | 4.75 ± 1.07 | 4.97 ± 1.71 | 0.303 | 0.823 |
| 24 h-P (mmol/L) | 22.24 ± 6.26 | 26.99 ± 6.69 | 23.19 ± 5.79 | 25.42 ± 6.92 | 24.47 ± 6.58 | 2.194 | 0.096 |
| 24 h-Mg (mmol/L) | 4.38 ± 2.08 | 4.30 ± 1.74 | 5.04 ± 2.41 | 5.08 ± 2.14 | 4.68 ± 2.08 | 0.753 | 0.524 |
| 24 h-pH | 7.0 ± 0.4 | 6.9 ± 0.5 | 6.9 ± 0.3 | 7.1 ± 0.3 | 7.0 ± 0.4 | 1.735 | 0.167 |
| 24 h-USG | 1.023 ± 0.005 | 1.025 ± 0.004 | 1.023 ± 0.005 | 1.022 ± 0.004 | 1.023 ± 0.004 | 1.733 | 0.168 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Ma, G.; Du, S.; Liu, S.; Zhang, N. Effects of Water Restriction and Supplementation on Cognitive Performances and Mood among Young Adults in Baoding, China: A Randomized Controlled Trial (RCT). Nutrients 2021, 13, 3645. https://doi.org/10.3390/nu13103645
Zhang J, Ma G, Du S, Liu S, Zhang N. Effects of Water Restriction and Supplementation on Cognitive Performances and Mood among Young Adults in Baoding, China: A Randomized Controlled Trial (RCT). Nutrients. 2021; 13(10):3645. https://doi.org/10.3390/nu13103645
Chicago/Turabian StyleZhang, Jianfen, Guansheng Ma, Songming Du, Shufang Liu, and Na Zhang. 2021. "Effects of Water Restriction and Supplementation on Cognitive Performances and Mood among Young Adults in Baoding, China: A Randomized Controlled Trial (RCT)" Nutrients 13, no. 10: 3645. https://doi.org/10.3390/nu13103645