Effects of a 3-Week In-Hospital Body Weight Reduction Program on Cardiovascular Risk Factors, Muscle Performance, and Fatigue: A Retrospective Study in a Population of Obese Adults with or without Metabolic Syndrome

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Body Weight Reduction Program (BWRP)
2.3. Evaluation of Risk Factors
2.4. Stair Climbing Test
2.5. Fatigue Severity Scale
2.6. Statistical Analysis
3. Results
3.1. Total Population
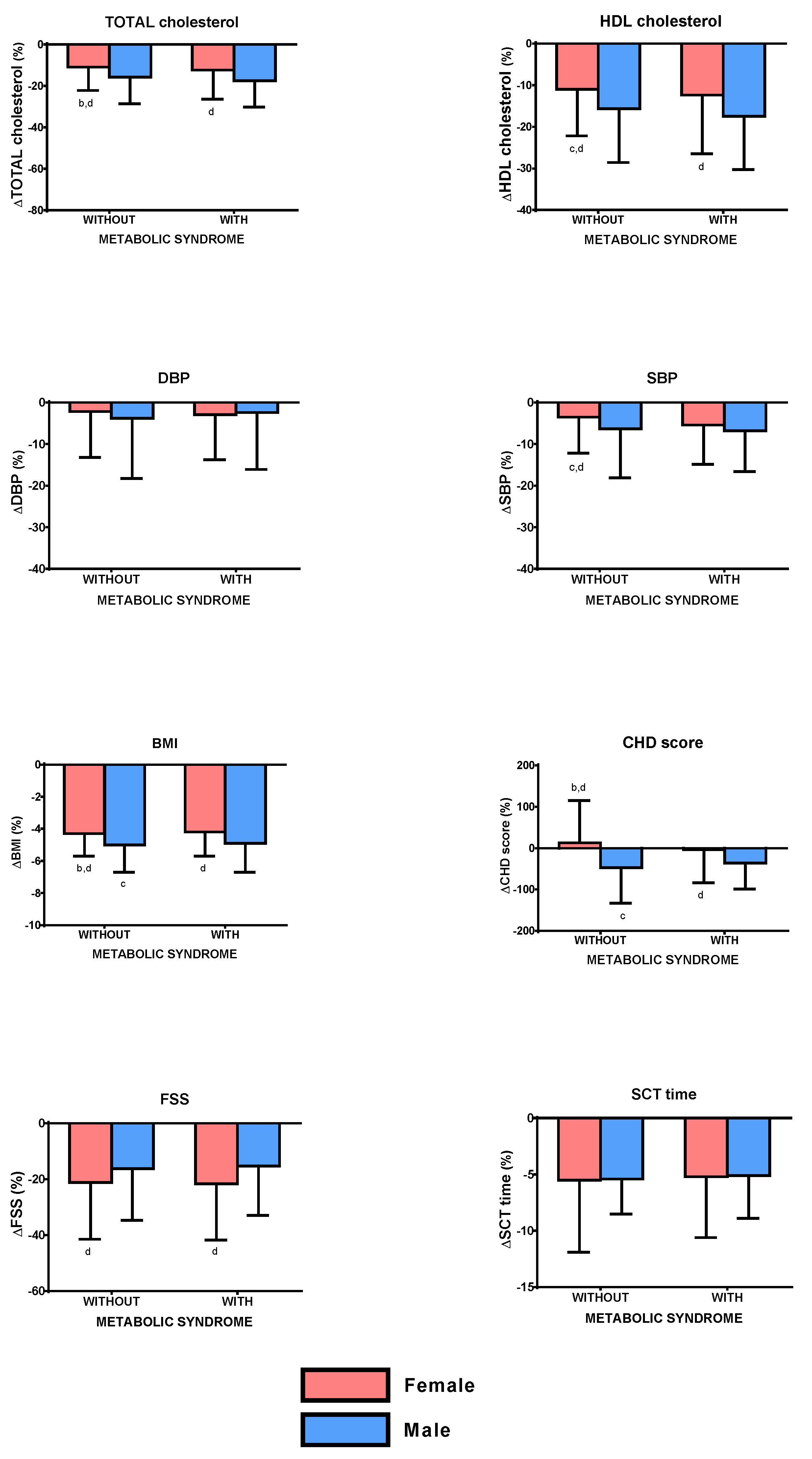
3.2. Subdivision for Sex: Females and Males
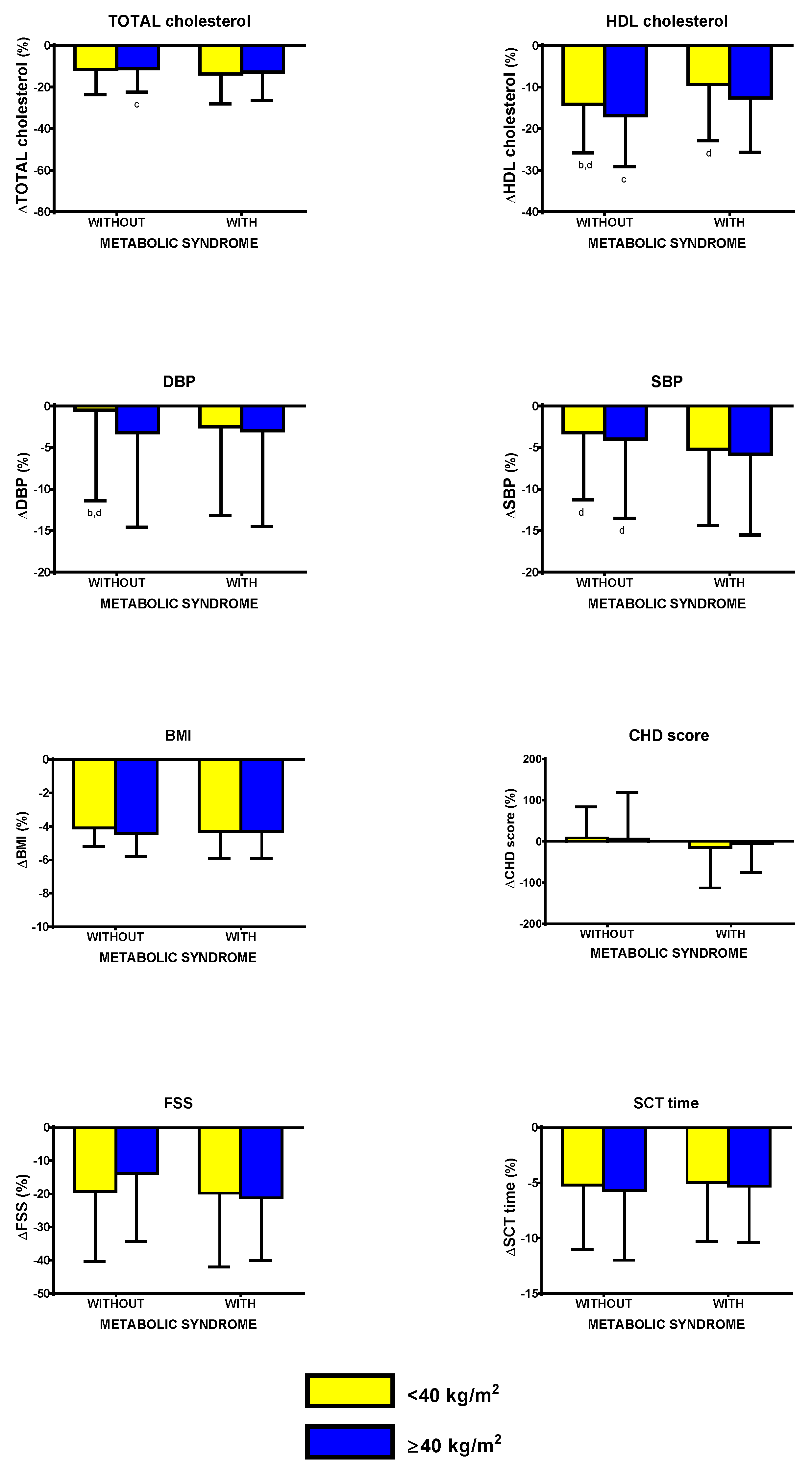
3.3. Subdivision for BMI: <40 and ≥40 kg/m2
3.4. Subdivision for Age: <65 and ≥65 yr
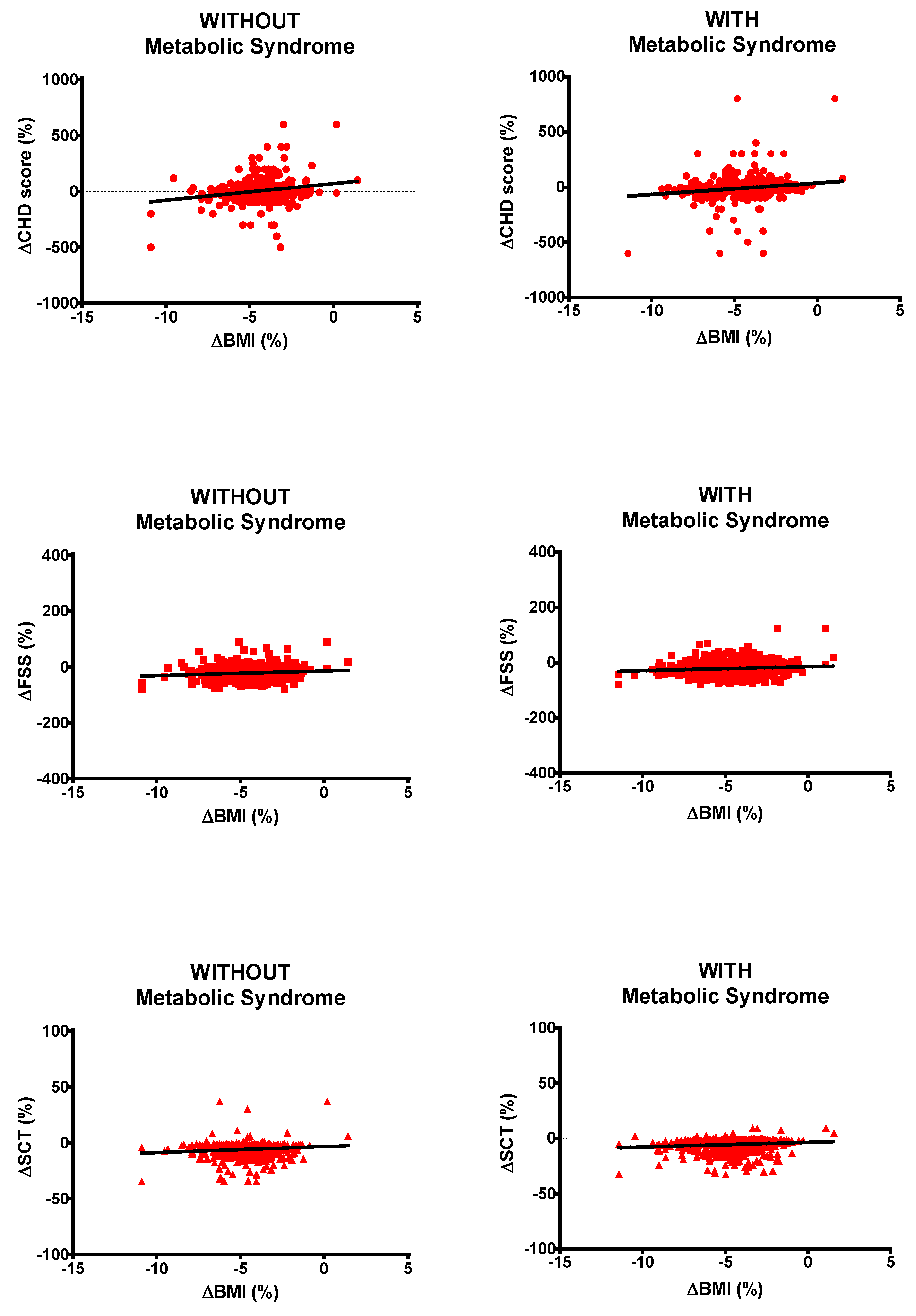
3.5. Regressions and Correlations
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef]
- Bartolomucci, A.; Bresciani, E.; Bulgarelli, I.; Rigamonti, A.E.; Pascucci, T.; Levi, A.; Possenti, R.; Torsello, A.; Locatelli, V.; Müller, E.E.; et al. Chronic intracerebroventricular injection of TLQP-21 prevents high fat diet induced weight gain in fast weight-gaining mice. Genes Nutr. 2009, 4, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Rigamonti, A.E.; Cella, S.G.; Bonomo, S.M.; Mancia, G.; Grassi, G.; Perotti, M.; Agosti, F.; Sartorio, A.; Muller, E.E.; Pincelli, A.I. Effect of somatostatin infusion on peptide YY secretion: Studies in the acute and recovery phase of anorexia nervosa and in obesity. Eur. J. Endocrinol. 2011, 165, 421–427. [Google Scholar] [CrossRef] [Green Version]
- De Gennaro-Colonna, V.; Rossoni, G.; Cocchi, D.; Rigamonti, A.E.; Berti, F.; Müller, E.E. Endocrine, metabolic and cardioprotective effects of hexarelin in obese Zucker rats. J. Endocrinol. 2000, 166, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Rigamonti, A.E.; Piscitelli, F.; Aveta, T.; Agosti, F.; De Col, A.; Bini, S.; Cella, S.G.; Di Marzo, V.; Sartorio, A. Anticipatory and consummatory effects of (hedonic) chocolate intake are associated with increased circulating levels of the orexigenic peptide ghrelin and endocannabinoids in obese adults. Food Nutr. Res. 2015, 59, 29678. [Google Scholar] [CrossRef] [Green Version]
- De Sousa, S.M.C.; Norman, R.; Ao, R.J.N. Metabolic syndrome, diet and exercise. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 37, 140–151. [Google Scholar] [CrossRef]
- Pritchett, A.M.; Foreyt, J.P.; Mann, D.L. Treatment of the metabolic syndrome: The impact of lifestyle modification. Curr. Atheroscler. Rep. 2005, 7, 95–102. [Google Scholar] [CrossRef]
- Rigamonti, A.E.; De Col, A.; Tamini, S.; Cicolini, S.; Caroli, D.; De Micheli, R.; Tringali, G.; Abbruzzese, L.; Marazzi, N.; Cella, S.; et al. Multidisciplinary Integrated Metabolic Rehabilitation in Elderly Obese Patients: Effects on Cardiovascular Risk Factors, Fatigue and Muscle Performance. Nutrients 2019, 11, 1240. [Google Scholar] [CrossRef] [Green Version]
- Rigamonti, A.E.; Tringali, G.; De Micheli, R.; De Col, A.; Tamini, S.; Saezza, A.; Cella, S.; Sartorio, A. Impact of a Three-Week in-Hospital Multidisciplinary Body Weight Reduction Program on Body Composition, Muscle Performance and Fatigue in a Pediatric Obese Population with or without Metabolic Syndrome. Nutrients 2020, 12, 208. [Google Scholar] [CrossRef] [Green Version]
- Sartorio, A.; Ottolini, S.; Agosti, F.; Massarini, M.; Lafortuna, C.L. Three-week integrated body weight reduction programme markedly improves performance and work capacity in severely obese patients. Eat. Weight. Disord. 2003, 8, 107–113. [Google Scholar] [CrossRef]
- Sartorio, A.; Lafortuna, C.L.; Marinone, P.G.; Tavani, A.; La Vecchia, C.; Bosetti, C. Short-term effects of two integrated, non-pharmacological body weight reduction programs on coronary heart disease risk factors in young obese patients. Diabetes Nutr. Metab. 2003, 16, 262–265. [Google Scholar] [PubMed]
- Sartorio, A.; Fontana, P.; Trecate, L.; Lafortuna, C.L. Short-term changes of fatigability and muscle performance in severe obese patients after an integrated body mass reduction program. Diabetes Nutr. Metab. 2003, 16, 88–93. [Google Scholar] [PubMed]
- Sartorio, A.; Lafortuna, C.L.; Vangeli, V.; Tavani, A.; Bosetti, C.; La Vecchia, C. Short-term changes of cardiovascular risk factors after a non-pharmacological body weight reduction program. Eur. J. Clin. Nutr. 2001, 55, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Lv, N.; Azar, K.M.; Rosas, L.G.; Wulfovich, S.; Xiao, L.; Ma, J. Behavioral lifestyle interventions for moderate and severe obesity: A systematic review. Prev. Med. 2017, 100, 180–193. [Google Scholar] [CrossRef] [PubMed]
- Bassi, N.; Karagodin, I.; Wang, S.; Vassallo, P.; Priyanath, A.; Massaro, E.; Stone, N.J. Lifestyle Modification for Metabolic Syndrome: A Systematic Review. Am. J. Med. 2014, 127, 1242.e1–1242.e10. [Google Scholar] [CrossRef]
- Dunkley, A.J.; Charles, K.; Gray, L.J.; Camosso-Stefinovic, J.; Davies, M.J.; Khunti, K. Effectiveness of interventions for reducing diabetes and cardiovascular disease risk in people with metabolic syndrome: Systematic review and mixed treatment comparison meta-analysis. Diabetes Obes. Metab. 2012, 14, 616–625. [Google Scholar] [CrossRef]
- Legato, M.J. Gender-specific aspects of obesity. Int. J. Fertil. Women’s Med. 1997, 42, 184–197. [Google Scholar]
- Williams, R.L.; Wood, L.G.; Collins, C.E.; Callister, R. Effectiveness of weight loss interventions—Is there a difference between men and women: A systematic review. Obes. Rev. 2014, 16, 171–186. [Google Scholar] [CrossRef]
- Fiorini, G.; Cerri, C.; Bini, S.; Rigamonti, A.E.; Perlini, S.; Marazzi, N.; Sartorio, A.; Cella, S. The burden of chronic noncommunicable diseases in undocumented migrants: A 1-year survey of drugs dispensation by a non–governmental organization in Italy. Public Health 2016, 141, 26–31. [Google Scholar] [CrossRef]
- Han, T.S.; Tajar, A.; Lean, M.E.J. Obesity and weight management in the elderly. Br. Med. Bull. 2011, 97, 169–196. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome-a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W.F.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershats, H.; Kannel, W.B. Prediction of coronary hearth disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartorio, A.; Proietti, M.; Marinone, P.G.; Agosti, F.; Adorni, F.; Lafortuna, C.L. Influence of gender, age and BMI on lower limb muscular power output in a large population of obese men and women. Int. J. Obes. Relat. Metab. Disord. 2003, 28, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Impellizzeri, F.M.; Agosti, F.; De Col, A.; Sartorio, A. Psychometric properties of the Fatigue Severity Scale in obese patients. Health Qual. Life Outcomes 2013, 11, 32. [Google Scholar] [CrossRef] [Green Version]
- Sartorio, A.; Narici, M.V.; Fumagalli, E.; Faglia, G.; Lafortuna, C.L. Aerobic and anaerobic performance before and after a short-term body mass reduction program in obese subjects. Diabetes Nutr. Metab. 2001, 14, 51–57. [Google Scholar]
- Sartorio, A.; Lafortuna, C.L.; Conte, G.; Faglia, G.; Narici, M.V. Changes in motor control and muscle performance after a short-term body mass reduction program in obese subjects. J. Endocrinol. Investig. 2001, 24, 393–398. [Google Scholar] [CrossRef]
- Hjollund, N.H.; Andersen, J.H.; Bech, P. Assessment of fatigue in chronic disease: A bibliographic study of fatigue measurement scales. Health Qual. Life Outcomes 2007, 5, 12. [Google Scholar] [CrossRef] [Green Version]
- Elbers, R.G.; Rietberg, M.B.; Van Wegen, E.; Verhoef, J.; Kramer, S.F.; Terwee, C.B.; Kwakkel, G. Self-report fatigue questionnaires in multiple sclerosis, Parkinson’s disease and stroke: A systematic review of measurement properties. Qual. Life Res. 2011, 21, 925–944. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, V.E. Weight loss is a critical factor to reduce inflammation. Clin. Nutr. ESPEN 2018, 28, 21–35. [Google Scholar] [CrossRef]
- Apostolopoulos, V.; De Courten, M.P.J.; Stojanovska, L.; Blatch, G.L.; Tangalakis, K.; De Courten, B. The complex immunological and inflammatory network of adipose tissue in obesity. Mol. Nutr. Food Res. 2015, 60, 43–57. [Google Scholar] [CrossRef]
- Nystoriak, M.A.; Bhatnagar, A. Cardiovascular Effects and Benefits of Exercise. Front. Cardiovasc. Med. 2018, 5, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saladini, F.; Palatini, P. Arterial Distensibility, Physical Activity, and the Metabolic Syndrome. Curr. Hypertens Rep. 2018, 20, 39. [Google Scholar] [CrossRef] [PubMed]
- Jovanovski, E.; Zurbau, A.; Vuksan, V. Carbohydrates and Endothelial Function: Is a Low-Carbohydrate Diet or a Low-Glycemic Index Diet Favourable for Vascular Health? Clin. Nutr. Res. 2015, 4, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyzos, S.A.; Margioris, A.N. Sarcopenic obesity. Hormones 2018, 17, 321–331. [Google Scholar] [CrossRef]
- Lim, W.; Hong, S.; Nelesen, R.; Dimsdale, J.E. The Association of Obesity, Cytokine Levels, and Depressive Symptoms With Diverse Measures of Fatigue in Healthy Subjects. Arch. Intern. Med. 2005, 165, 910. [Google Scholar] [CrossRef] [Green Version]
- Resnick, H.E.; Carter, E.A.; Aloia, M.; Phillips, B. Cross-Sectional Relationship of Reported Fatigue to Obesity, Diet, and Physical Activity: Results From the Third National Health and Nutrition Examination Survey. J. Clin. Sleep Med. 2006, 2, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Varni, J.W.; Limbers, C.A.; Bryant, W.P.; Wilson, D.P. The PedsQL Multidimensional Fatigue Scale in pediatric obesity: Feasibility, reliability and validity. Int. J. Pediatr. Obes. 2010, 5, 34–42. [Google Scholar] [CrossRef]
- Lee, Y.J.; Cho, W.J.; Kim, J.K.; Lee, D.C. Effects of Coenzyme Q10 on Arterial Stiffness, Metabolic Parameters, and Fatigue in Obese Subjects: A Double-Blind Randomized Controlled Study. J. Med. Food 2011, 14, 386–390. [Google Scholar] [CrossRef]
- Cordeiro, L.; Rabelo, P.; Moraes, M.; Teixeira-Coelho, F.; Coimbra, C.; Wanner, S.; Soares, D. Physical exercise-induced fatigue: The role of serotonergic and dopaminergic systems. Braz. J. Med Biol. Res. 2017, 50, e6432. [Google Scholar] [CrossRef]
- Foley, T.E.; Fleshner, M. Neuroplasticity of Dopamine Circuits After Exercise: Implications for Central Fatigue. Neuromol. Med. 2008, 10, 67–80. [Google Scholar] [CrossRef]
- Eime, R.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W. A systematic review of the psychological and social benefits of participation in sport for adults: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Ruiz, M.E.; Guarner-Lans, V.; Pérez-Torres, I.; Soto, M.E. Mechanisms Underlying Metabolic Syndrome-Related Sarcopenia and Possible Therapeutic Measures. Int. J. Mol. Sci. 2019, 20, 647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalinkovich, A.; Livshits, G. Sarcopenic obesity or obese sarcopenia: A cross talk between age-associated adipose tissue and skeletal muscle inflammation as a main mechanism of the pathogenesis. Ageing Res. Rev. 2017, 35, 200–221. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Obese Subjects | ||||||
|---|---|---|---|---|---|---|
| Parameter | Without Metabolic Syndrome | With Metabolic Syndrome | ||||
| Before | After | Δ (%) | Before | After | Δ (%) | |
| N. | 726 | - | - | 1196 | - | - |
| Age (yr) | 46.1 ± 15.3 a | - | - | 53.4 ± 12.6 | - | - |
| BMI (kg/m2) | 42.5 ± 5.3 a | 40.7 ± 5.1 | −4.4 ± 1.4 | 43.8 ± 6.6 | 41.9 ± 6.4 b | −4.3 ± 1.6 |
| TOT-CHOL (mg/dL) | 191.2 ± 35.5 a | 168.0 ± 31.1 b | −11.4 ± 11.4 a | 198.0 ± 37.9 | 170.3 ± 35.0 b | −13.1 ± 14.0 |
| HDL-CHOL (mg/dL) | 56.0 ± 12.2 a | 46.5 ± 10.4 b | −16.0 ± 12.2 a | 45.6 ± 11.4 | 39.8 ± 9.3 b | −11.6 ± 13.3 |
| Glucose (mg/dL) | 83.5 ± 11.9 a | - | - | 108.0 ± 36.9 | - | - |
| Triglycerides (mg/dL) | 99.9 ± 32.3 a | - | - | 159.4 ± 70.5 | - | - |
| DBP (mmHg) | 76.2 ± 7.9 a | 73.8 ± 6.4 b | −2.3±11.3 | 77.6 ± 7.7 | 74.8 ± 6.6 b | −2.8 ± 11.3 |
| SBP (mmHg) | 125.5 ± 13.8 a | 119.9 ± 9.0 b | −3.7 ± 9.0 a | 130.4 ± 13.6 | 122.2 ± 9.7 b | −5.6 ± 9.6 |
| CHD score | 3.1 ± 5.4 a | 3.3 ± 5.6 | 6.6 ± 102.3 a | 8.5 ± 4.8 | 7.9 ± 5.1 b | −7.7 ± 79.2 |
| FSS | 34.5 ± 12.7 a | 26.9 ± 11.5 b | −20.8 ± 20.2 | 38.3 ± 12.9 | 29.8 ± 11.8 b | −20.8 ± 19.9 |
| SCT (s) | 5.7 ± 1.8 a | 5.4 ± 1.8 b | −5.5 ± 6.1 | 6.4 ± 1.9 | 6.1 ± 1.9 b | −5.2 ± 5.2 |
| Female Obese Subjects | ||||
| Parameter | Without Metabolic Syndrome | With Metabolic Syndrome | ||
| Before | After | Before | After | |
| N. | 665 | - | 1035 | - |
| Age (yr) | 46.3 ± 15.3 a | - | 54.1 ± 12.2 | - |
| BMI (kg/m2) | 42.6 ± 5.3 a | 40.8 ± 5.1 b | 43.9 ± 6.6 | 42.1 ± 6.4 b |
| TOT-CHOL (mg/dL) | 191.9 ± 35.6 a | 169.5 ± 31.3 b | 198.6 ± 38.4 | 172.2 ± 35.4 b |
| HDL-CHOL (mg/dL) | 56.8 ± 12.1 a | 47.1 ± 10.3 b | 46.6 ± 11.4 | 40.4 ± 9.3 b |
| DBP (mmHg) | 76.0 ± 7.7 a | 73.8 ± 6.4 b | 77.5 ± 7.4 | 74.7 ± 6.5 b |
| SBP (mmHg) | 125.0 ± 13.4 a | 119.8 ± 8.9 b | 130.2 ± 13.5 | 122.3 ± 9.7 b |
| CHD score | 3.0 ± 5.6 a | 3.3 ± 5.8 b | 8.8 ± 4.9 | 8.4 ± 5.1 b |
| FSS | 34.9 ± 12.8 a | 27.1 ± 11.7 b | 39.2 ± 12.8 | 30.3 ± 12.0 b |
| SCT (s) | 5.7 ± 1.8 a | 5.4 ± 1.8 b | 6.5 ± 1.9 | 6.2 ± 1.9 b |
| MALE Obese Subjects | ||||
| Parameter | Without Metabolic Syndrome | With Metabolic Syndrome | ||
| Before | After | Before | After | |
| N. | 61 | - | 161 | - |
| Age (yr) | 44.1 ± 15.8 a | - | 48.7 ± 14.0 | - |
| BMI (kg/m2) | 41.9 ± 5.4 | 39.8 ± 5.2 b | 43.2 ± 6.5 | 41.0 ± 6.3 b |
| TOT-CHOL (mg/dL) | 183.4 ± 33.8 a | 152.0 ± 22.7 b | 193.9 ± 35.0 | 158.2 ± 29.5 b |
| HDL-CHOL (mg/dL) | 46.9 ± 10.2a | 40.4 ± 9.6 b | 39.5 ± 9.2 | 35.6 ± 8.0 b |
| DBP (mmHg) | 78.7 ± 9.7 | 74.7 ± 6.6 b | 78.0 ± 9.5 | 75.2 ± 7.0 b |
| SBP (mmHg) | 131.1 ± 17.2 | 121.3 ± 10.1 b | 131.8 ± 14.2 | 121.8 ± 9.5 b |
| CHD score | 4.3 ± 3.0 a | 2.9 ± 3.6 b | 6.3 ± 3.3 | 4.4 ± 3.7 b |
| FSS | 30.1 ± 11.3 | 24.9 ± 9.8 b | 32.4 ± 12.4 | 26.8 ± 10.3 b |
| SCT (s) | 5.5 ± 1.6 | 5.2 ± 1.5 b | 5.7 ± 1.7 | 5.4 ± 1.6 b |
| Obese Subjects with BMI < 40 kg/m2 | ||||
| Parameter | Without Metabolic Syndrome | With Metabolic Syndrome | ||
| Before | After | Before | After | |
| N. | 247 | - | 360 | - |
| Age (yr) | 47.0 ± 15.3 a | - | 53.6 ± 13.7 | - |
| BMI (kg/m2) | 37.4 ± 1.9 | 35.8 ± 1.9 b | 37.5 ± 1.9 | 35.9 ± 1.9 b |
| TOT-CHOL (mg/dL) | 193.1 ± 36.8 a | 169.2 ± 32.1 b | 199.4 ± 37.4 | 170.3 ± 35.0 b |
| HDL-CHOL (mg/dL) | 56.7 ± 11.6 a | 48.2 ± 10.0 b | 45.2 ± 10.9 | 40.4 ± 9.3 b |
| DBP (mmHg) | 74.2 ± 7.3 a | 73.3 ± 6.4 b | 76.2 ± 7.4 | 73.7 ± 6.1 b |
| SBP (mmHg) | 124.0 ± 12.7 a | 119.3 ± 9.1 b | 128.2 ± 12.7 | 120.8 ± 9.0 b |
| CHD score | 3.1 ± 5.4 a | 3.2 ± 5.5 | 8.3 ± 5.2 | 7.5 ± 5.8 b |
| FSS | 32.3 ± 11.9 a | 25.7 ± 11.0 b | 36.6 ± 12.8 | 28.5 ± 11.1 b |
| SCT (s) | 5.3 ± 1.6 a | 5.1 ± 1.6 b | 6.0 ± 1.9 | 5.7 ± 1.8 b |
| Obese Subjects with BMI ≥ 40 kg/m2 | ||||
| Parameter | Without Metabolic Syndrome | With Metabolic Syndrome | ||
| Before | After | Before | After | |
| N. | 479 | - | 836 | - |
| Age (yr) | 45.6 ± 15.3 a | - | 53.2 ± 12.1 | - |
| BMI (kg/m2) | 45.2 ± 4.6 a | 43.2 ± 4.4 b | 46.6 ± 6.0 | 44.5 ± 5.8 b |
| TOT-CHOL (mg/dL) | 198.3 ± 34.8 a | 167.4 ± 30.5 b | 197.4 ± 38.2 | 170.4 ± 35.0 b |
| HDL-CHOL (mg/dL) | 55.6 ± 12.6 a | 45.7 ± 10.5 b | 45.8 ± 11.6 | 39.5 ± 9.3 b |
| DBP (mmHg) | 77.2 ± 8.0 a | 74.1 ± 6.4 b | 78.2 ± 7.8 | 75.3 ± 6.7 b |
| SBP (mmHg) | 126.3 ± 14.4 a | 120.3 ± 8.9 b | 131.4 ± 13.8 | 122.8 ± 9.9 b |
| CHD score | 3.2 ± 5.5 a | 3.3 ± 5.6 | 8.5 ± 4.6 | 8.0 ± 4.9 b |
| FSS | 35.6 ± 13.0 a | 27.5 ± 11.8 b | 39.0 ± 12.9 | 30.4 ± 12.1 b |
| SCT (s) | 5.9 ± 1.9 a | 5.6 ± 1.8 b | 6.6 ± 1.9 | 6.2 ± 1.9 b |
| <65 yr old Obese Subjects | ||||
| Parameter | Without Metabolic Syndrome | With Metabolic Syndrome | ||
| Before | After | Before | After | |
| N. | 630 | - | 964 | - |
| Age (yr) | 42.4 ± 12.9 a | - | 49.5 ± 10.8 | - |
| BMI (kg/m2) | 42.6 ± 5.3 a | 40.7 ± 5.1 b | 44.2 ± 6.8 | 42.2 ± 6.5 b |
| TOT-CHOL (mg/dL) | 190.5 ± 35.6 a | 167.8 ± 31.0 b | 197.9 ± 38.0 | 170.9 ± 34.7 b |
| HDL-CHOL (mg/dL) | 55.1 ± 12.4 a | 46.2 ± 10.5 b | 45.1 ± 11.2 | 39.5 ± 9.2 b |
| DBP (mmHg) | 75.9 ± 7.7 a | 73.7 ± 6.5 b | 77.7 ± 7.6 | 74.8 ± 6.6 b |
| SBP (mmHg) | 124.0 ± 12.5 a | 119.4 ± 8.8 b | 129.9 ± 13.3 | 121.7 ± 9.4 b |
| CHD score | 2.3 ± 5.4 a | 2.5 ± 5.6 | 7.8 ± 5.0 | 7.1 ± 5.3 b |
| FSS | 33.2 ± 12.2 a | 25.4 ± 10.6 b | 37.4 ± 12.3 | 28.6 ± 11.2 b |
| SCT (s) | 5.5 ± 1.6 a | 5.2 ± 1.5 b | 6.2 ± 1.8 | 5.8 ± 1.7 b |
| ≥65 yr old Obese Subjects | ||||
| Parameter | Without Metabolic Syndrome | With Metabolic Syndrome | ||
| Before | After | Before | After | |
| N. | 96 | - | 232 | - |
| Age (yr) | 70.3 ± 4.1 | - | 69.5 ± 3.9 | - |
| BMI (kg/m2) | 42.0 ± 5.5 | 40.3 ± 5.3 b | 42.4 ± 5.7 | 40.8 ± 5.5 b |
| TOT-CHOL (mg/dL) | 196.2 ± 34.4 | 169.3 ± 31.8 b | 198.3 ± 37.8 | 168.0 ± 36.3 b |
| HDL-CHOL (mg/dL) | 61.8 ± 9.3 a | 49.1 ± 9.4 b | 47.9 ± 11.7 | 40.9 ± 9.8 b |
| DBP (mmHg) | 77.9 ± 9.0 | 74.6 ± 6.0 b | 77.2 ± 8.2 | 74.6 ± 6.6 b |
| SBP (mmHg) | 135.1 ± 17.8 | 123.6 ± 9.6b | 132.6 ± 14.6 | 124.4 ± 10.4 b |
| CHD score | 7.6 ± 2.4 a | 7.8 ± 2.6 | 10.9 ± 3.1 | 10.6 ± 3.3 |
| FSS | 43.4 ± 12.7 | 36.8 ± 12.7 b | 41.7 ± 13.5 | 35.0 ± 12.9 b |
| SCT (s) | 7.9 ± 2.1 | 7.6 ± 2.0 b | 7.7 ± 2.0 | 7.4 ± 1.9 b |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigamonti, A.E.; Cicolini, S.; Caroli, D.; De Col, A.; Scacchi, M.; Cella, S.G.; Sartorio, A. Effects of a 3-Week In-Hospital Body Weight Reduction Program on Cardiovascular Risk Factors, Muscle Performance, and Fatigue: A Retrospective Study in a Population of Obese Adults with or without Metabolic Syndrome. Nutrients 2020, 12, 1495. https://doi.org/10.3390/nu12051495
Rigamonti AE, Cicolini S, Caroli D, De Col A, Scacchi M, Cella SG, Sartorio A. Effects of a 3-Week In-Hospital Body Weight Reduction Program on Cardiovascular Risk Factors, Muscle Performance, and Fatigue: A Retrospective Study in a Population of Obese Adults with or without Metabolic Syndrome. Nutrients. 2020; 12(5):1495. https://doi.org/10.3390/nu12051495
Chicago/Turabian StyleRigamonti, Antonello E., Sabrina Cicolini, Diana Caroli, Alessandra De Col, Massimo Scacchi, Silvano G. Cella, and Alessandro Sartorio. 2020. "Effects of a 3-Week In-Hospital Body Weight Reduction Program on Cardiovascular Risk Factors, Muscle Performance, and Fatigue: A Retrospective Study in a Population of Obese Adults with or without Metabolic Syndrome" Nutrients 12, no. 5: 1495. https://doi.org/10.3390/nu12051495