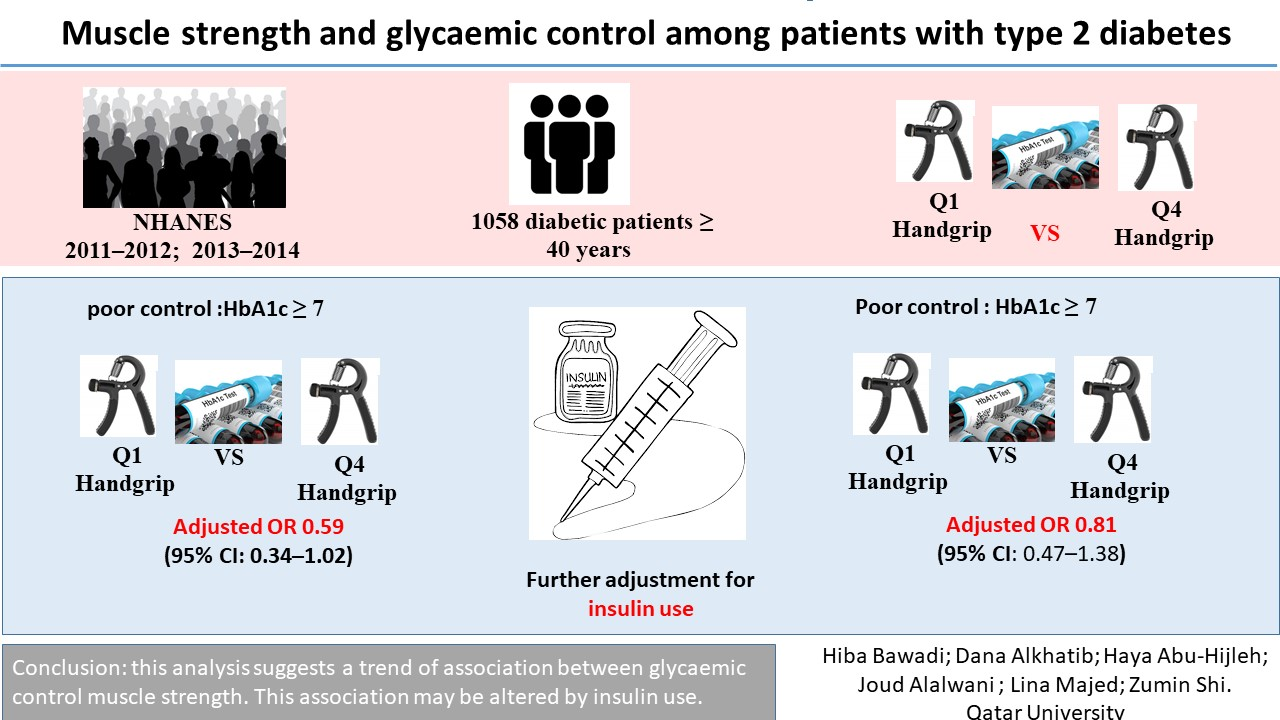
Muscle Strength and Glycaemic Control among Patients with Type 2 Diabetes

 , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Dependent Variable
Glycaemic Control
2.3. Independent Variables
Muscle Strength
2.4. Co-variates
2.4.1. Height and Body Weight
2.4.2. Sedentary Activity
2.4.3. Use of Insulin
2.4.4. Smoking Status
2.4.5. Alcohol Use
2.4.6. Participant Demographics
2.4.7. Income-to-poverty Ratio
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tabish, S.A. Is Diabetes Becoming the Biggest Epidemic of the Twenty-first Century? Int. J. Health Sci. 2007, 1. [Google Scholar]
- Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2014, 37, S81–S90. [CrossRef] [PubMed] [Green Version]
- American Diabetes Association Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2010, 34, S62–S69.
- Zimmet, P.Z. Diabetes and its drivers: The largest epidemic in human history? Clin. Diabetes Endocrinol. 2017, 3, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, M.; Li, J.; Li, Z.; Luo, W.; Dai, D.; Weaver, S.R.; Stauber, C.; Luo, R.; Fu, H. Mortality rates and the causes of death related to diabetes mellitus in Shanghai Songjiang District: An 11-year retrospective analysis of death certificates. BMC Endocr. Disord. 2015, 15, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stokes, A.; Preston, S.H. Deaths Attributable to Diabetes in the United States: Comparison of Data Sources and Estimation Approaches. PLoS ONE 2017, 12, e0170219. [Google Scholar] [CrossRef] [PubMed]
- Nickerson, H.; Dutta, S. Diabetic Complications: Current Challenges and Opportunities. J. Cardiovasc. Transl. Res. 2012, 5, 375–379. [Google Scholar] [CrossRef] [Green Version]
- Hill, J. Reducing the risk of complications associated with diabetes. Nurs. Stand. 2009, 23, 49–55. [Google Scholar] [CrossRef]
- Zhuo, X.; Zhang, P.; Hoerger, T.J. Lifetime Direct Medical Costs of Treating Type 2 Diabetes and Diabetic Complications. Am. J. Prev. Med. 2013, 45, 253–261. [Google Scholar] [CrossRef]
- Riddell, M.C.; Perkins, B.A. Exercise and Glucose Metabolism in Persons with Diabetes Mellitus: Perspectives on the Role for Continuous Glucose Monitoring. J. Diabetes Sci. Technol. 2009, 3, 914–923. [Google Scholar] [CrossRef]
- Lee, J.; Kim, D.; Kim, C. Resistance Training for Glycemic Control, Muscular Strength, and Lean Body Mass in Old Type 2 Diabetic Patients: A Meta-Analysis. Diabetes Ther. 2017, 8, 459–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayer, A.A.; Dennison, E.M.; Syddall, H.E.; Gilbody, H.J.; Phillips, D.I.W.; Cooper, C. Type 2 Diabetes, Muscle Strength, and Impaired Physical Function: The tip of the iceberg? Diabetes Care 2005, 28, 2541–2542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jurca, R.; LaMonte, M.J.; Barlow, C.E.; Kampert, J.B.; Church, T.S.; Blair, S.N. Association of Muscular Strength with Incidence of Metabolic Syndrome in Men. Med. Sci. Sports Exerc. 2005, 37, 1849–1855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrath, R.; Vincent, B.; Al Snih, S.; Markides, K.S.; Peterson, M.D. The Association between Muscle Weakness and Incident Diabetes in Older Mexican Americans. J. Am. Med Dir. Assoc. 2017, 18, 452.e7–452.e12. [Google Scholar] [CrossRef] [Green Version]
- Wander, P.; Boyko, E.J.; Leonetti, D.; McNeely, M.; Kahn, S.E.; Fujimoto, W. Greater hand-grip strength predicts a lower risk of developing type 2 diabetes over 10 years in leaner Japanese Americans. Diabetes Res. Clin. Pr. 2011, 92, 261–264. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Nelson, D.; Zhao, Y.; Cui, Z.L.; A Johnston, J. Relationship between muscle mass and muscle strength, and the impact of comorbidities: A population-based, cross-sectional study of older adults in the United States. BMC Geriatr. 2013, 13, 74. [Google Scholar] [CrossRef] [Green Version]
- Çetinus, E.; Buyukbese, M.A.; Üzel, M.; Ekerbiçer, H.; Karaoguz, A. Hand grip strength in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pr. 2005, 70, 278–286. [Google Scholar] [CrossRef]
- Bassey, E.J.; Harries, U.J. Normal values for handgrip strength in 920 men and women aged over 65 years, and longitudinal changes over 4 years in 620 survivors. Clin. Sci. 1993, 84, 331–337. [Google Scholar] [CrossRef]
- Chang, S.A. Smoking and Type 2 Diabetes Mellitus. Diabetes Metab. J. 2012, 36, 399–403. [Google Scholar] [CrossRef] [Green Version]
- Lassiter, T.L.; Ryde, I.T.; MacKillop, E.A.; Brown, K.K.; Levin, E.D.; Seidler, F.J.; A Slotkin, T. Exposure of Neonatal Rats to Parathion Elicits Sex-Selective Reprogramming of Metabolism and Alters the Response to a High-Fat Diet in Adulthood. Environ. Health Perspect. 2008, 116, 1456–1462. [Google Scholar] [CrossRef]
- Evangelista, L.; Heber, D.; Li, Z.; Bowerman, S.; Hamilton, M.A.; Fonarow, G.C. Reduced body weight and adiposity with a high-protein diet improves functional status, lipid profiles, glycemic control, and quality of life in patients with heart failure: A feasibility study. J. Cardiovasc. Nurs. 2009, 24, 207–215. [Google Scholar] [CrossRef] [Green Version]
- Association, A.D. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, W.J. What is sarcopenia? J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, 5–8. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics. National Health and Nutrition Examination Survey 2013–2014; Centers for Disease Control and Prevention, US Department of Health and Human Services: Hyattsville, MD, USA, 2013.
- Ogden, C.L.; Carroll, M.D.; Lawman, H.G.; Fryar, C.D.; Kruszon-Moran, D.; Kit, B.K.; Flegal, K.M. Trends in Obesity Prevalence Among Children and Adolescents in the United States, 1988–1994 Through 2013–2014. JAMA 2016, 315, 2292–2299. [Google Scholar] [CrossRef]
- Li, S.; Zhang, R.; Pan, G.; Zheng, L.; Li, C. Handgrip strength is associated with insulin resistance and glucose metabolism in adolescents: Evidence from National Health and Nutrition Examination Survey 2011 to 2014. Pediatr. Diabetes 2017, 19, 375–380. [Google Scholar] [CrossRef]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.; De Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; Newman, A.B. Decreased Muscle Strength and Quality in Older Adults With Type 2 Diabetes: The Health, Aging, and Body Composition Study. Diabetes 2006, 55, 1813–1818. [Google Scholar] [CrossRef] [Green Version]
- Gill, P.K.S.; Sandhu, R.; Dhillon, S.K.; Arora, A.K. Handgrip strength in patients with type 2 diabetes mellitus. Pak. J. Physiol. 2016, 12, 19–21. [Google Scholar]
- Kalyani, R.R.; Metter, E.J.; Egan, J.; Golden, S.H.; Ferrucci, L. Hyperglycemia Predicts Persistently Lower Muscle Strength with Aging. Diabetes Care 2014, 38, 82–90. [Google Scholar] [CrossRef] [Green Version]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.; Kuller, L.H.; Broudeau, R.; Kammerer, C.M.; De Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; et al. Accelerated Loss of Skeletal Muscle Strength in Older Adults With Type 2 Diabetes: The Health, Aging, and Body Composition Study. Diabetes Care 2007, 30, 1507–1512. [Google Scholar] [CrossRef] [Green Version]
- Marques-Vidal, P.; Vollenweider, P.; Waeber, G.; Jornayvaz, F.R. Grip strength is not associated with incident type 2 diabetes mellitus in healthy adults: The CoLaus study. Diabetes Res. Clin. Pr. 2017, 132, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Angst, F.; Drerup, S.; Werle, S.; Herren, D.; Simmen, B.R.; Goldhahn, J. Prediction of grip and key pinch strength in 978 healthy subjects. BMC Musculoskelet. Disord. 2010, 11, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Peolsson, A.; Massy-Westropp, N.; Desrosiers, J.; Bear-Lehman, J. Reference values for adult grip strength measured with a Jamar dynamometer: A descriptive meta-analysis. Physiother. 2006, 92, 11–15. [Google Scholar] [CrossRef]
- Brooks, N. Strength training improves muscle quality and insulin sensitivity in Hispanic older adults with type 2 diabetes. Int. J. Med Sci. 2007, 4, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Q1 | Q2 | Q3 | Q4 | p-Value | |
|---|---|---|---|---|---|
| N = 268 | N = 263 | N = 266 | N = 261 | ||
| Handgrip strength (kg) | 45.5 (13.4) | 58.3 (14.1) | 67.7 (15.9) | 81.8 (20.0) | < 0.001 |
| Age (years) | 65.6 (12.0) | 62.8 (11.4) | 62.2 (10.5) | 60.2 (9.8) | < 0.001 |
| Gender | 1.00 | ||||
| Men | 138 (51.5%) | 133 (50.6%) | 135 (50.8%) | 134 (51.3%) | |
| Women | 130 (48.5%) | 130 (49.4%) | 131 (49.2%) | 127 (48.7%) | |
| Race | < 0.001 | ||||
| NH White | 103 (38.4%) | 95 (36.1%) | 95 (35.7%) | 86 (33.0%) | |
| NH Black | 57 (21.3%) | 49 (18.6%) | 84 (31.6%) | 127 (48.7%) | |
| Mex. American | 41 (15.3%) | 43 (16.3%) | 38 (14.3%) | 20 (7.7%) | |
| Other race/ethnic | 67 (25.0%) | 76 (28.9%) | 49 (18.4%) | 28 (10.7%) | |
| Education | < 0.001 | ||||
| < 11 grade | 117 (43.8%) | 90 (34.2%) | 83 (31.3%) | 53 (20.3%) | |
| HS dipl. or GED | 58 (21.7%) | 51 (19.4%) | 72 (27.2%) | 62 (23.8%) | |
| Some college | 53 (19.9%) | 75 (28.5%) | 70 (26.4%) | 93 (35.6%) | |
| > college | 39 (14.6%) | 47 (17.9%) | 40 (15.1%) | 53 (20.3%) | |
| Smoking | 0.82 | ||||
| Never | 137 (51.1%) | 126 (47.9%) | 133 (50.0%) | 130 (49.8%) | |
| Former | 92 (34.3%) | 95 (36.1%) | 87 (32.7%) | 97 (37.2%) | |
| Current smoker | 39 (14.6%) | 42 (16.0%) | 46 (17.3%) | 34 (13.0%) | |
| Alcohol drinking | < 0.001 | ||||
| No | 85 (31.7%) | 71 (27.0%) | 77 (28.9%) | 73 (28.0%) | |
| Yes | 102 (38.1%) | 132 (50.2%) | 141 (53.0%) | 145 (55.6%) | |
| Missing | 81 (30.2%) | 60 (22.8%) | 48 (18.0%) | 43 (16.5%) | |
| BMI (kg/m2) | 30.7 (7.0) | 31.5 (7.3) | 32.7 (7.7) | 33.8 (6.8) | < 0.001 |
| Sedentary activity | 0.21 | ||||
| < 3 hrs | 41 (15.3%) | 58 (22.1%) | 47 (17.7%) | 51 (19.5%) | |
| 3–6 hrs | 77 (28.7%) | 89 (33.8%) | 85 (32.0%) | 79 (30.3%) | |
| 6+ hrs | 150 (56.0%) | 116 (44.1%) | 134 (50.4%) | 131 (50.2%) | |
| Income-to-poverty ratio | < 0.001 | ||||
| < 1.30 | 119 (47.6%) | 105 (43.6%) | 97 (39.8%) | 59 (24.1%) | |
| 1.3–3.5 | 83 (33.2%) | 96 (39.8%) | 92 (37.7%) | 104 (42.4%) | |
| > 3.5 | 48 (19.2%) | 40 (16.6%) | 55 (22.5%) | 82 (33.5%) | |
| HbA1c (%) | 7.5 (2.0) | 7.4 (1.7) | 7.6 (1.9) | 7.2 (1.7) | 0.078 |
| Poor glycaemic control | 130 (48.5%) | 132 (50.2%) | 141 (53.0%) | 107 (41.0%) | 0.040 |
| Use of insulin | 94 (35.1%) | 75 (28.5%) | 68 (25.6%) | 57 (21.8%) | 0.006 |
| Q1 | Q2 | Q3 | Q4 | p for Trend | |
|---|---|---|---|---|---|
| Model 1 | 1.00 | 0.99 (0.61-1.62) | 1.34 (0.76-2.34) | 0.73 (0.44-1.23) | 0.434 |
| Model 2 | 1.00 | 0.86 (0.45-1.62) | 1.07 (0.57-1.99) | 0.51 (0.27-0.99) | 0.073 |
| Model 3 | 1.00 | 1.09 (0.59-2.03) | 1.37 (0.70-2.69) | 0.67 (0.35-1.28) | 0.319 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bawadi, H.; Alkhatib, D.; Abu-Hijleh, H.; Alalwani, J.; Majed, L.; Shi, Z. Muscle Strength and Glycaemic Control among Patients with Type 2 Diabetes. Nutrients 2020, 12, 771. https://doi.org/10.3390/nu12030771
Bawadi H, Alkhatib D, Abu-Hijleh H, Alalwani J, Majed L, Shi Z. Muscle Strength and Glycaemic Control among Patients with Type 2 Diabetes. Nutrients. 2020; 12(3):771. https://doi.org/10.3390/nu12030771
Chicago/Turabian StyleBawadi, Hiba, Dana Alkhatib, Haya Abu-Hijleh, Joud Alalwani, Lina Majed, and Zumin Shi. 2020. "Muscle Strength and Glycaemic Control among Patients with Type 2 Diabetes" Nutrients 12, no. 3: 771. https://doi.org/10.3390/nu12030771