Fruit and Vegetable Consumption and Potential Moderators Associated with All-Cause Mortality in a Representative Sample of Spanish Older Adults

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
Study Sample
3. Measures
3.1. Fruit and Vegetable Consumption
3.2. Other Covariates
3.3. Mortality
3.4. Statistical Analysis
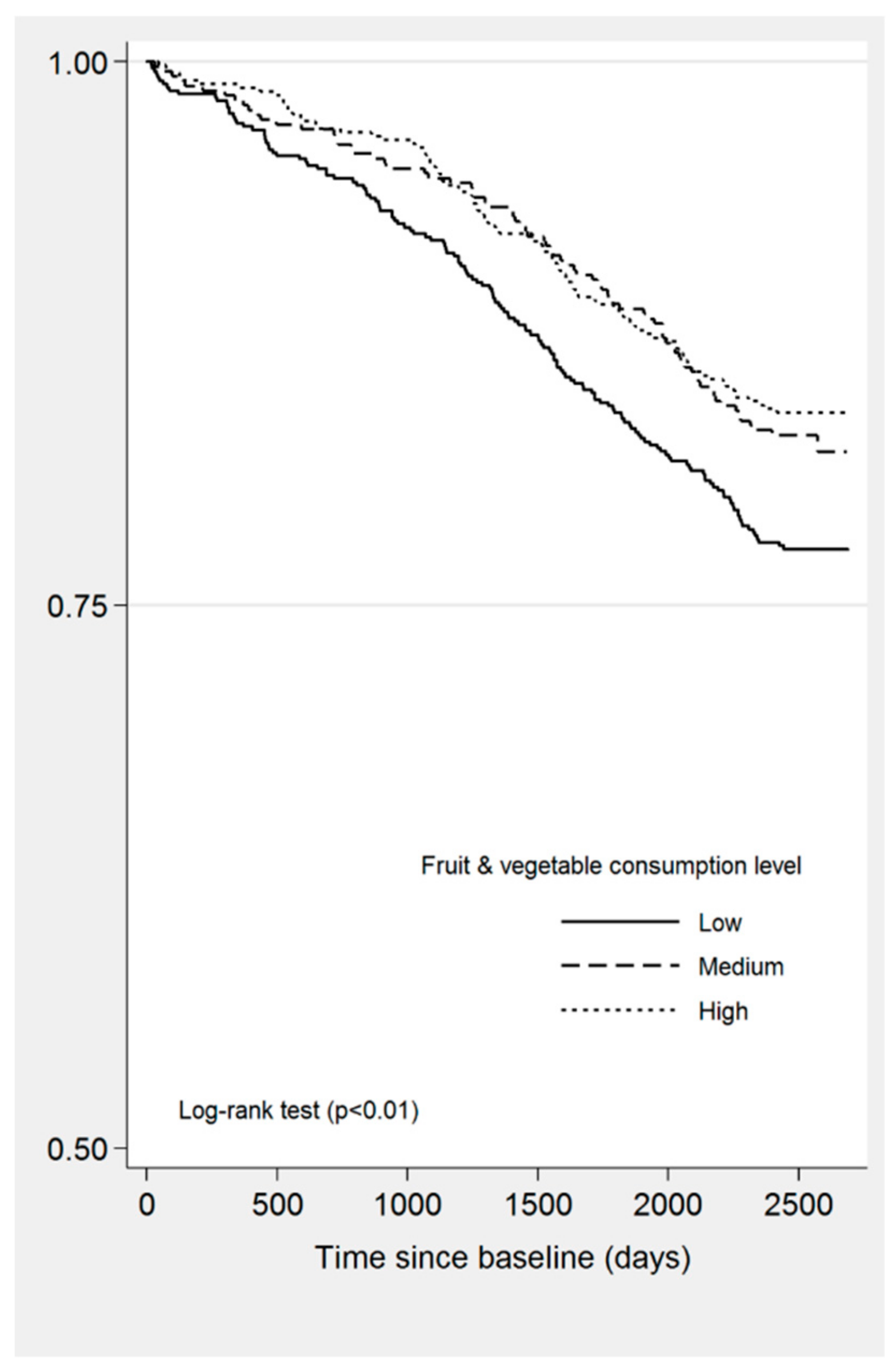
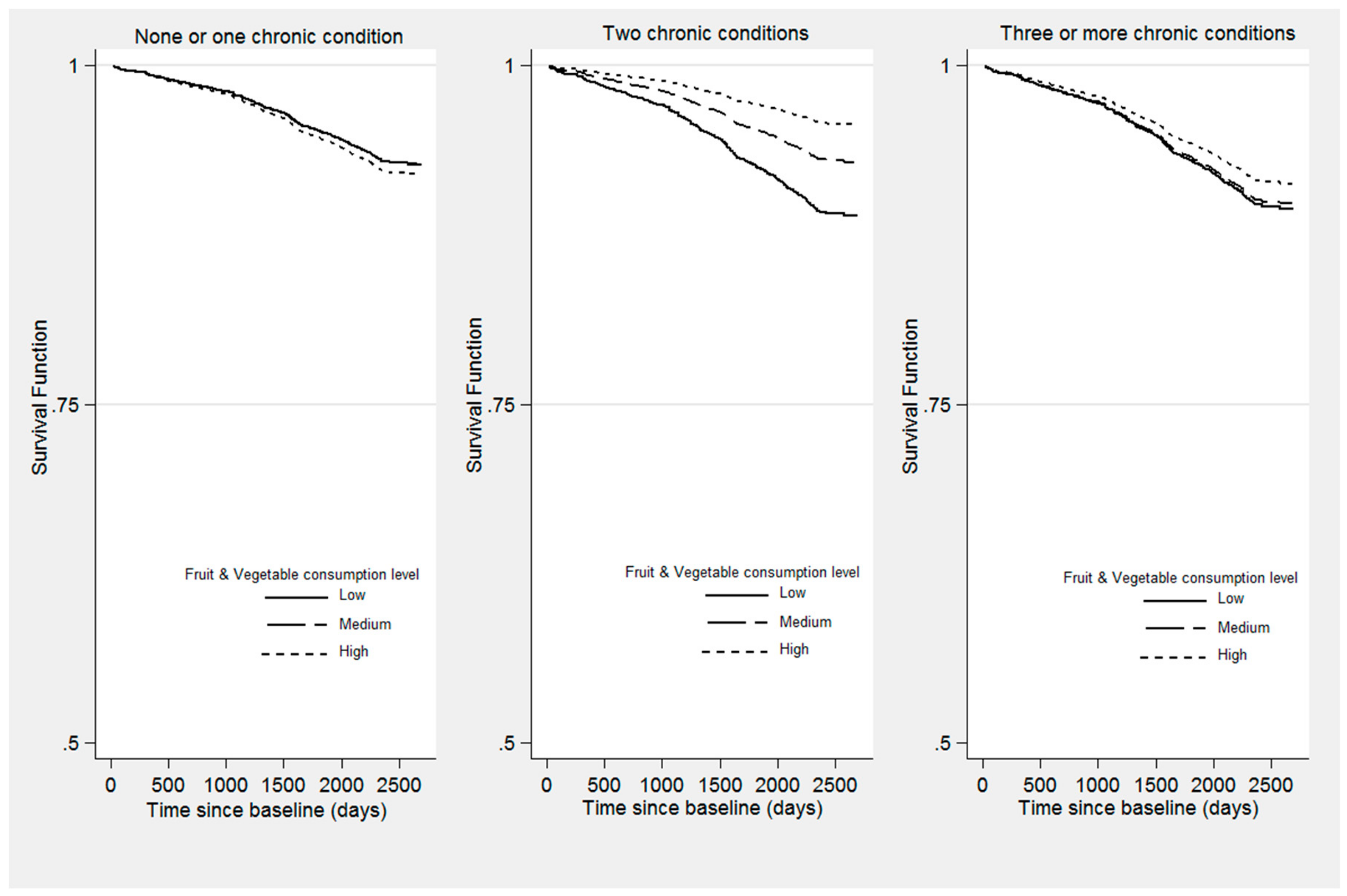
3.5. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Fulton, S.L.; McKinley, M.C.; Young, I.S.; Cardwell, C.R.; Woodside, J.V. The effect of increasing fruit and vegetable consumption on overall diet: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2016, 56, 802–816. [Google Scholar] [CrossRef] [PubMed]
- Mytton, O.T.; Nnoaham, K.; Eyles, H.; Scarborough, P.; Ni Mhurchu, C. Systematic review and meta-analysis of the effect of increased vegetable and fruit consumption on body weight and energy intake. BMC Public Health 2014, 14, 886. [Google Scholar]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—A systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Huang, J.; Wang, Y.; Zhang, D.; Qu, Y. Fruits and vegetables consumption and risk of stroke. Stroke 2014, 45, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Fan, Y.; Zhang, X.; Hou, W.; Tang, Z. Fruit and vegetable intake and risk of type 2 diabetes mellitus: Meta-analysis of prospective cohort studies. BMJ Open 2014, 4, e005497. [Google Scholar] [PubMed]
- Li, B.; Li, F.; Wang, L.; Zhang, D. Fruit and vegetables consumption and risk of hypertension: A meta-analysis. J. Clin. Hypertens. 2016, 18, 468–476. [Google Scholar]
- WHO, Promoting Fruit and Vegetable Consumption Around the World. Available online: https://www.who.int/dietphysicalactivity/fruit/en/index2.html (accessed on 5 June 2019).
- Bellavia, A.; Larsson, S.C.; Bottai, M.; Wolk, A.; Orsini, N. Fruit and vegetable consumption and all-cause mortality: A dose-response analysis. Am. J. Clin. Nutr. 2013, 98, 454–459. [Google Scholar] [PubMed]
- Buil-Cosiales, P.; Zazpe, I.; Toledo, E.; Corella, D.; Salas-Salvadó, J.; Diez-Espino, J.; Ros, E.; Navajas, J.F.C.; Santos-Lozano, J.M.; Arós, F.; et al. Fiber intake and all-cause mortality in the Prevención con Dieta Mediterránea (PREDIMED) study. Am. J. Clin. Nutr. 2014, 100, 1498–1507. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, g4490. [Google Scholar] [CrossRef]
- Miller, V.; Mente, A.; Dehghan, M.; Rangarajan, S.; Zhang, X.; Swaminathan, S.; Dagenais, G.; Gupta, R.; Mohan, V.; Lear, S.; et al. Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): A prospective cohort study. Lancet 2017, 390, 2037–2049. [Google Scholar] [CrossRef]
- Oyebode, O.; Gordon-Dseagu, V.; Walker, A.; Mindell, J.S. Fruit and vegetable consumption and all-cause, cancer and CVD mortality: Analysis of health survey for England data. J. Epidemiol. Community Health 2014, 68, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Sobue, T.; Otani, T.; Tsugane, S. Vegetables, fruit consumption and risk of lung cancer among middle-aged Japanese men and women: JPHC study. Cancer Causes Control 2004, 15, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Rajala, M. Nutrition and diet for healthy lifestyles in Europe: Science and policy implications. Public Health Nutr. 2001, 4, 339–340. [Google Scholar] [PubMed]
- World Cancer Research Fund; American Institute for Cancer Research. Diet Nutrition Physical Activity and Cancer: A Global Perspective; Continuous Update Project Expert Report 2018; World Cancer Research Fund/American Institute for Cancer Research: Washington, DC, USA, 2018. Available online: http://dietandcancerreport.org (accessed on 27 April 2019).
- WHO/FAO. Expert Report on Diet, Nutrition and the Prevention of Chronic Diseases; Technical Report Series 916; World Health Organisation: Geneva, Switzerland, 2003. [Google Scholar]
- Yngve, A.; Wolf, A.; Poortvliet, E.; Elmadfa, I.; Brug, J.; Ehrenblad, B.; Franchini, B.; Haraldsdóttir, J.; Krølner, R.; Maes, L.; et al. Fruit and vegetable intake in a sample of 11-year-old children in 9 European countries: The pro children cross-sectional survey. Ann. Nutr. Metab. 2005, 49, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Nicklett, E.J.; Kadell, A.R. Fruit and vegetable intake among older adults: A scoping review. Maturitas 2013, 75, 305–312. [Google Scholar] [PubMed] [Green Version]
- Amarya, S.; Singh, K.; Sabharwal, M. Changes during aging and their association with malnutrition. J. Clin. Gerontol. Geriatr. 2015, 6, 78–84. [Google Scholar] [Green Version]
- Tsai, A.C.; Chang, T.-L.; Chi, S.-H. Frequent consumption of vegetables predicts lower risk of depression in older Taiwanese—Results of a prospective population-based study. Public Health Nutr. 2012, 15, 1087–1092. [Google Scholar] [CrossRef]
- Loef, M.; Walach, H. Fruit, vegetables and prevention of cognitive decline or dementia: A systematic review of cohort studies. J. Nutr. Health Aging 2012, 16, 626–630. [Google Scholar] [CrossRef]
- Gopinath, B.; Russell, J.; Flood, V.M.; Burlutsky, G.; Mitchell, P. Adherence to dietary guidelines positively affects quality of life and functional status of older adults. J. Acad. Nutr. Diet. 2014, 114, 220–229. [Google Scholar] [CrossRef]
- García-Esquinas, E.; Rahi, B.; Peres, K.; Colpo, M.; Dartigues, J.-F.; Bandinelli, S.; Feart, C.; Rodríguez-Artalejo, F. Consumption of fruit and vegetables and risk of frailty: A dose-response analysis of 3 prospective cohorts of community-dwelling older adults. Am. J. Clin. Nutr. 2016, 104, 132–142. [Google Scholar] [CrossRef]
- Stefler, D.; Pikhart, H.; Kubinova, R.; Pajak, A.; Stepaniak, U.; Malyutina, S.; Simonova, G.; Peasey, A.; Marmot, M.G.; Bobak, M. Fruit and vegetable consumption and mortality in Eastern Europe: Longitudinal results from the health, alcohol and psychosocial factors in Eastern Europe study. Eur. J. Prev. Cardiol. 2016, 23, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, M.; Chatterji, S.; Koskinen, S.; Ayuso-Mateos, J.L.; Haro, J.M.; Frisoni, G.; Frattura, L.; Martinuzzi, A.; Tobiasz-Adamczyk, B.; Gmurek, M.; et al. Determinants of health and disability in ageing population: The courage in Europe project (collaborative research on ageing in Europe). Clin. Psychol. Psychother. 2014, 21, 193–198. [Google Scholar] [PubMed]
- Kowal, P.; Chatterji, S.; Naidoo, N.; Biritwum, R.; Fan, W.; Lopez Ridaura, R.; Maximova, T.; Arokiasamy, P.; Phaswana-Mafuya, N.; Williams, S.; et al. Data resource profile: The World Health Organization study on global AGEing and adult health (SAGE). Int. J. Epidemiol. 2012, 41, 1639–1649. [Google Scholar] [CrossRef] [PubMed]
- WHO. Process of Translation and Adaptation of Instruments. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 31 March 2019).
- Üstün, T.; Chatterji, S.; Mechbal, A.; Murray, C.; Groups, W.C. Quality assurance in surveys: Standards, guidelines and procedures. In Household Sample Surveys in Developing and Transtion Countries; United Nations: New York, NY, USA, 2005. [Google Scholar]
- Bull, F.C.; Maslin, T.S.; Armstrong, T. Global physical activity questionnaire (GPAQ): Nine country reliability and validity study. J. Phys. Act. Health 2009, 6, 790–804. [Google Scholar] [CrossRef]
- Olaya, B.; Moneta, M.V.; Doménech-Abella, J.; Miret, M.; Bayes, I.; Ayuso-Mateos, J.L.; Haro, J.M. Mobility difficulties, physical activity, and all-cause mortality risk in a nationally representative sample of older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 1272–1279. [Google Scholar] [CrossRef]
- Garin, N.; Koyanagi, A.; Chatterji, S.; Tyrovolas, S.; Olaya, B.; Leonardi, M.; Lara, E.; Koskinen, S.; Tobiasz-Adamczyk, B.; Ayuso-Mateos, J.L.; et al. Global multimorbidity patterns: A cross-sectional, population-based, multi-country study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 205–214. [Google Scholar] [PubMed]
- Basu, S.; Millett, C. Social epidemiology of hypertension in middle-income countries: Determinants of prevalence, diagnosis, treatment, and control in the WHO SAGE study. Hypertension 2013, 62, 18–26. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redón, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension. J. Hypertens. 2013, 31, 1281–1357. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization WHO. Global Database on Body Mass Index. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 2 May 2019).
- Rao, J.N.K.; Scott, A.J. On chi-squared tests for multiway contingency tables with cell proportions estimated from survey data. Ann. Stat. 1984, 12, 46–60. [Google Scholar] [CrossRef]
- Buil-Cosiales, P.; Martinez-Gonzalez, M.A.; Ruiz-Canela, M.; Díez-Espino, J.; García-Arellano, A.; Toledo, E. Consumption of fruit or fiber-fruit decreases the risk of cardiovascular disease in a Mediterranean young cohort. Nutrients 2017, 9, 295. [Google Scholar] [CrossRef]
- Hodgson, J.M.; Prince, R.L.; Woodman, R.J.; Bondonno, C.P.; Ivey, K.L.; Bondonno, N.; Rimm, E.B.; Ward, N.C.; Croft, K.D.; Lewis, J.R. Apple intake is inversely associated with all-cause and disease-specific mortality in elderly women. Br. J. Nutr. 2016, 115, 860–867. [Google Scholar] [CrossRef] [Green Version]
- Iimuro, S.; Yoshimura, Y.; Umegaki, H.; Sakurai, T.; Araki, A.; Ohashi, Y.; Iijima, K.; Ito, H. Japanese elderly diabetes intervention trial study group dietary pattern and mortality in Japanese elderly patients with type 2 diabetes mellitus: Does a vegetable- and fish-rich diet improve mortality? An explanatory study. Geriatr. Gerontol. Int. 2012, 12, 59–67. [Google Scholar] [CrossRef]
- Buil-Cosiales, P.; Toledo, E.; Salas-Salvadó, J.; Zazpe, I.; Farràs, M.; Basterra-Gortari, F.J.; Diez-Espino, J.; Estruch, R.; Corella, D.; Ros, E.; et al. Association between dietary fibre intake and fruit, vegetable or whole-grain consumption and the risk of CVD: Results from the PREvención con DIeta MEDiterránea (PREDIMED) trial. Br. J. Nutr. 2016, 116, 534–546. [Google Scholar] [CrossRef]
- Hung, H.-C.; Joshipura, K.J.; Jiang, R.; Hu, F.B.; Hunter, D.; Smith-Warner, S.A.; Colditz, G.A.; Rosner, B.; Spiegelman, D.; Willett, W.C. Fruit and vegetable intake and risk of major chronic disease. J. Natl. Cancer Inst. 2004, 96, 1577–1584. [Google Scholar] [CrossRef]
- Nunes, B.P.; Flores, T.R.; Mielke, G.I.; Thumé, E.; Facchini, L.A. Multimorbidity and mortality in older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2016, 67, 130–138. [Google Scholar] [CrossRef]
- Calderón-Larrañaga, A.; Poblador-Plou, B.; González-Rubio, F.; Gimeno-Feliu, L.A.; Abad-Díez, J.M.; Prados-Torres, A. Multimorbidity, polypharmacy, referrals, and adverse drug events: Are we doing things well? Br. J. Gen. Pract. 2012, 62, e821–e826. [Google Scholar] [CrossRef]
- De Mello, C.A.; Engstrom, E.M.; Alves, L.C. Health-related and socio-demographic factors associated with frailty in the elderly: A systematic literature review. Cad. Saude Publica 2014, 30, 1143–1168. [Google Scholar] [CrossRef]
- Hurst, J.R.; Dickhaus, J.; Maulik, P.K.; Miranda, J.J.; Pastakia, S.D.; Soriano, J.B.; Siddharthan, T.; Vedanthan, R.; GACD Multi-Morbidity Working Group. Global alliance for chronic disease researchers’ statement on multimorbidity. Lancet Glob. Health 2018, 6, e1270–e1271. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Lagiou, P. Healthy traditional Mediterranean diet: An expression of culture, history, and lifestyle. Nutr. Rev. 2009, 55, 383–389. [Google Scholar] [CrossRef]
- Bermejo, L.M.; Aparicio, A.; Andrés, P.; López-Sobaler, A.M.; Ortega, R.M. The influence of fruit and vegetable intake on the nutritional status and plasma homocysteine levels of institutionalised elderly people. Public Health Nutr. 2007, 10, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean diet and cardiovascular health: A critical review. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Barak, Y.; Fridman, D. Impact of Mediterranean diet on cancer: Focused literature review. Cancer Genom. Proteom. 2017, 14, 403–408. [Google Scholar]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis of observational studies. Cancer Med. 2015, 4, 1933–1947. [Google Scholar] [CrossRef]
- Samieri, C.; Grodstein, F.; Rosner, B.A.; Kang, J.H.; Cook, N.R.; Manson, J.E.; Buring, J.E.; Willett, W.C.; Okereke, O.I. Mediterranean diet and cognitive function in older age. Epidemiology 2013, 24, 490–499. [Google Scholar] [CrossRef]
- Anastasiou, C.A.; Yannakoulia, M.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Arampatzi, X.; Bougea, A.; Labropoulos, I.; Scarmeas, N. Mediterranean diet and cognitive health: Initial results from the Hellenic longitudinal investigation of ageing and diet. PLoS ONE 2017, 12, e0182048. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Critselis, E. Mediterranean diet and longevity. Eur. J. Cancer Prev. 2004, 13, 453–456. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.M.; Knüppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef]
- Schnabel, L.; Kesse-Guyot, E.; Allès, B.; Touvier, M.; Srour, B.; Hercberg, S.; Buscail, C.; Julia, C. Association between ultraprocessed food consumption and risk of mortality among middle-aged adults in France. JAMA Intern. Med. 2019, 179, 490–498. [Google Scholar] [CrossRef]
- Dauchet, L.; Montaye, M.; Ruidavets, J.-B.; Arveiler, D.; Kee, F.; Bingham, A.; Ferrières, J.; Haas, B.; Evans, A.; Ducimetière, P.; et al. Association between the frequency of fruit and vegetable consumption and cardiovascular disease in male smokers and non-smokers. Eur. J. Clin. Nutr. 2010, 64, 578–586. [Google Scholar] [CrossRef]
- Kesse, E.; Clavel-Chapelon, F.; Slimani, N.; van Liere, M. Do eating habits differ according to alcohol consumption? Results of a study of the French cohort of the European prospective investigation into cancer and nutrition (E3N-EPIC). Am. J. Clin. Nutr. 2001, 74, 322–327. [Google Scholar] [CrossRef]
- Sharma, S.P.; Chung, H.J.; Kim, H.J.; Hong, S.T. Paradoxical effects of fruit on obesity. Nutrients 2016, 8, 633. [Google Scholar] [CrossRef]
- Jezewska-Zychowicz, M.; Gębski, J.; Guzek, D.; Świątkowska, M.; Stangierska, D.; Plichta, M.; Wasilewska, M. The associations between dietary patterns and sedentary behaviors in Polish adults (LifeStyle study). Nutrients 2018, 10, 1004. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Kimiagar, M.; Mehrabi, Y.; Azadbakht, L.; Hu, F.B.; Willett, W.C. Fruit and vegetable intakes, C-reactive protein, and the metabolic syndrome. Am. J. Clin. Nutr. 2006, 84, 1489–1497. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Hecker, K.D.; Bonanome, A.; Coval, S.M.; Binkoski, A.E.; Hilpert, K.F.; Griel, A.E.; Etherton, T.D. Bioactive compounds in foods: Their role in the prevention of cardiovascular disease and cancer. Am. J. Med. 2002, 113 (Suppl. 9B), 71S–88S. [Google Scholar] [CrossRef]
- Vita, J.A. Polyphenols and cardiovascular disease: Effects on endothelial and platelet function. Am. J. Clin. Nutr. 2005, 81, 292S–297S. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Fruit & Vegetable Consumption | |||||
|---|---|---|---|---|---|
| Total Sample (n = 1699) | Low (n = 669, 39.6%) | Medium (n = 448, 26.1%) | High (n = 582, 34.3%) | p Value | |
| Death, n (%) | 322 (18.6) | 150 (21.9) | 78 (18.7) | 94 (14.7) | 0.019 |
| Age, mean (95%CI) | 74.80 (74.49–75.12) | 74.98 (74.46–75.5) | 75.06 (74.43–75.68) | 74.4 (73.57–75.24) | 0.476 |
| Females, n (%) | 956 (54.8) | 341 (49.7) | 266 (58.8) | 349 (57.6) | 0.013 |
| Cohabiting, n (%) | 935 (54.7) | 376 (54.4) | 254 (56.9) | 305 (53.4) | 0.653 |
| Educational level, n (%) | 0.023 | ||||
| No education/Primary school | 804 (46.3) | 343 (51.7) | 216 (47.5) | 245 (39) | - |
| Secondary school | 492 (30.1) | 181 (27) | 125 (30.6) | 186 (33.4) | - |
| High school/University | 403 (23.6) | 145 (21.3) | 107 (22) | 151 (27.6) | 0.791 |
| Ever smoked, n (%) | 620 (37.2) | 278 (41.8) | 150 (32.5) | 192 (35.5) | 0.008 |
| Obesity, n (%) | 606 (33.4) | 237 (33.8) | 156 (34.5) | 213 (32.1) | 0.803 |
| Alcohol consumption, n (%) | <0.001 | ||||
| Lifetime abstainer | 618 (36.5) | 218 (31.9) | 167 (38.7) | 233 (40.1) | - |
| Occasional drinker | 524 (31) | 197 (28.6) | 138 (30.4) | 189 (34.2) | - |
| Frequent drinker | 557 (32.5) | 254 (39.5) | 143 (30.9) | 160 (25.7) | - |
| Number CC, n (%) | 0.369 | ||||
| None or one | 780 (43.8) | 305 (43.9) | 197 (42.2) | 278 (44.9) | - |
| Two | 482 (29.7) | 188 (28.5) | 130 (28.6) | 164 (31.8) | - |
| Three or more | 437 (26.5) | 176 (27.6) | 121 (29.2) | 140 (23.3) | - |
| Level PA, n (%) | 0.011 | ||||
| High | 427 (25.2) | 151 (21.6) | 108 (21) | 168 (32.7) | - |
| Medium | 700 (41.6) | 268 (40.6) | 185 (45.1) | 247 (40.1) | - |
| Low | 572 (33.2) | 250 (37.8) | 155 (33.9) | 167 (27.2) | - |
| Unadjusted | Adjusted a | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Fruit & veg consumption | ||||
| Low (ref.) | - | - | - | - |
| Medium | 0.83 (0.61–1.13) | 0.802 | 1.0 (0.62–1.60) | 0.989 |
| High | 1.68 (1.3–2.18) | <0.001 | 1.11 (0.70–1.74) | 0.659 |
| Age | 1.12 (1.1–1.14) | <0.001 | 1.13 (1.1–15) | <0.001 |
| Gender | ||||
| Female (ref.) | - | - | - | - |
| Male | 1.96 (1.49–2.57) | <0.001 | 3.31 (2.21–4.99) | <0.001 |
| Marital status | ||||
| Not cohabiting (ref.) | - | - | - | - |
| Cohabiting | 0.84 (0.66–1.1) | 0.169 | 0.9 (0.66–1.24) | 0.523 |
| Educational level | ||||
| No education/Primary school | - | - | - | - |
| Secondary school | 0.57 (0.39–0.83) | 0.004 | 0.77 (0.54–1.11) | 0.168 |
| High school/University | 0.67 (0.49–0.92) | 0.013 | 1.0 (0.74–1.35) | 0.997 |
| Level PA | ||||
| High (ref.) | - | - | - | - |
| Medium | 1.45 (0.99–2.13) | 0.056 | 1.28 (0.84–1.93) | 0.246 |
| Low | 2.3 (1.59–3.32) | <0.001 | 1.61 (1.07–2.43) | 0.021 |
| Smoking status | - | - | - | |
| Never smoked | - | - | - | - |
| Ever smoked | 1.38 (1.07–1.78) | 0.013 | 1.01 (0.73–1.39) | 0.973 |
| Alcohol consumption | ||||
| Lifetime abstainer (ref.) | - | - | - | - |
| Occasional drinker | 1.13 (0.84–1.5) | 0.414 | 0.97 (0.69–1.36) | 0.87 |
| Frequent drinker | 0.93 (0.69–1.24) | 0.625 | 0.64 (0.46–0.91) | 0.012 |
| Obesity | ||||
| Non-obese (ref.) | - | - | - | - |
| Obese | 1.14 (0.82–1.57) | 0.43 | 1.11 (0.8–1.55) | 0.515 |
| Number CC | ||||
| None/one (ref.) | - | - | - | - |
| Two | 0.95 (0.67–1.37) | 0.802 | 1.56 (0.91–2.65) | 0.102 |
| Three or more | 1.68 (1.3–2.18) | <0.001 | 1.47 (0.99–2.18) | 0.056 |
| Fruit & veg × number CC | ||||
| Medium/two CC | - | - | 0.63 (0.31–1.28) | 0.199 |
| Medium/three+ CC | - | - | 0.97 (0.47–2.0) | 0.930 |
| High/two CC | - | - | 0.34 (0.18–0.65) | 0.001 |
| High/three+ CC | - | - | 0.74 (0.39–1.42) | 0.360 |
| None or One CC | Two CC | Three or More CC | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Level of Fruit & Vegetable Consumption | HR | 95%CI | p Value | HR | 95%CI | p Value | HR | 95%CI | p Value | |||
| Low (ref.) | - | - | - | - | - | - | - | - | - | - | - | - |
| Medium | 1.0 | 0.62 | 1.6 | 0.989 | 0.63 | 0.33 | 0.19 | 0.151 | 0.96 | 0.54 | 0.73 | 0.905 |
| High | 1.11 | 0.7 | 1.74 | 0.659 | 0.38 | 0.21 | 0.69 | 0.002 | 0.82 | 0.5 | 1.35 | 0.428 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olaya, B.; Essau, C.A.; Moneta, M.V.; Lara, E.; Miret, M.; Martín-María, N.; Moreno-Agostino, D.; Ayuso-Mateos, J.L.; Abduljabbar, A.S.; Haro, J.M. Fruit and Vegetable Consumption and Potential Moderators Associated with All-Cause Mortality in a Representative Sample of Spanish Older Adults. Nutrients 2019, 11, 1794. https://doi.org/10.3390/nu11081794
Olaya B, Essau CA, Moneta MV, Lara E, Miret M, Martín-María N, Moreno-Agostino D, Ayuso-Mateos JL, Abduljabbar AS, Haro JM. Fruit and Vegetable Consumption and Potential Moderators Associated with All-Cause Mortality in a Representative Sample of Spanish Older Adults. Nutrients. 2019; 11(8):1794. https://doi.org/10.3390/nu11081794
Chicago/Turabian StyleOlaya, Beatriz, Cecilia A. Essau, Maria Victoria Moneta, Elvira Lara, Marta Miret, Natalia Martín-María, Darío Moreno-Agostino, José Luis Ayuso-Mateos, Adel S. Abduljabbar, and Josep Maria Haro. 2019. "Fruit and Vegetable Consumption and Potential Moderators Associated with All-Cause Mortality in a Representative Sample of Spanish Older Adults" Nutrients 11, no. 8: 1794. https://doi.org/10.3390/nu11081794