High Prevalence of Hypovitaminosis D in Institutionalized Elderly Individuals is Associated with Summer in a Region with High Ultraviolet Radiation Levels
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
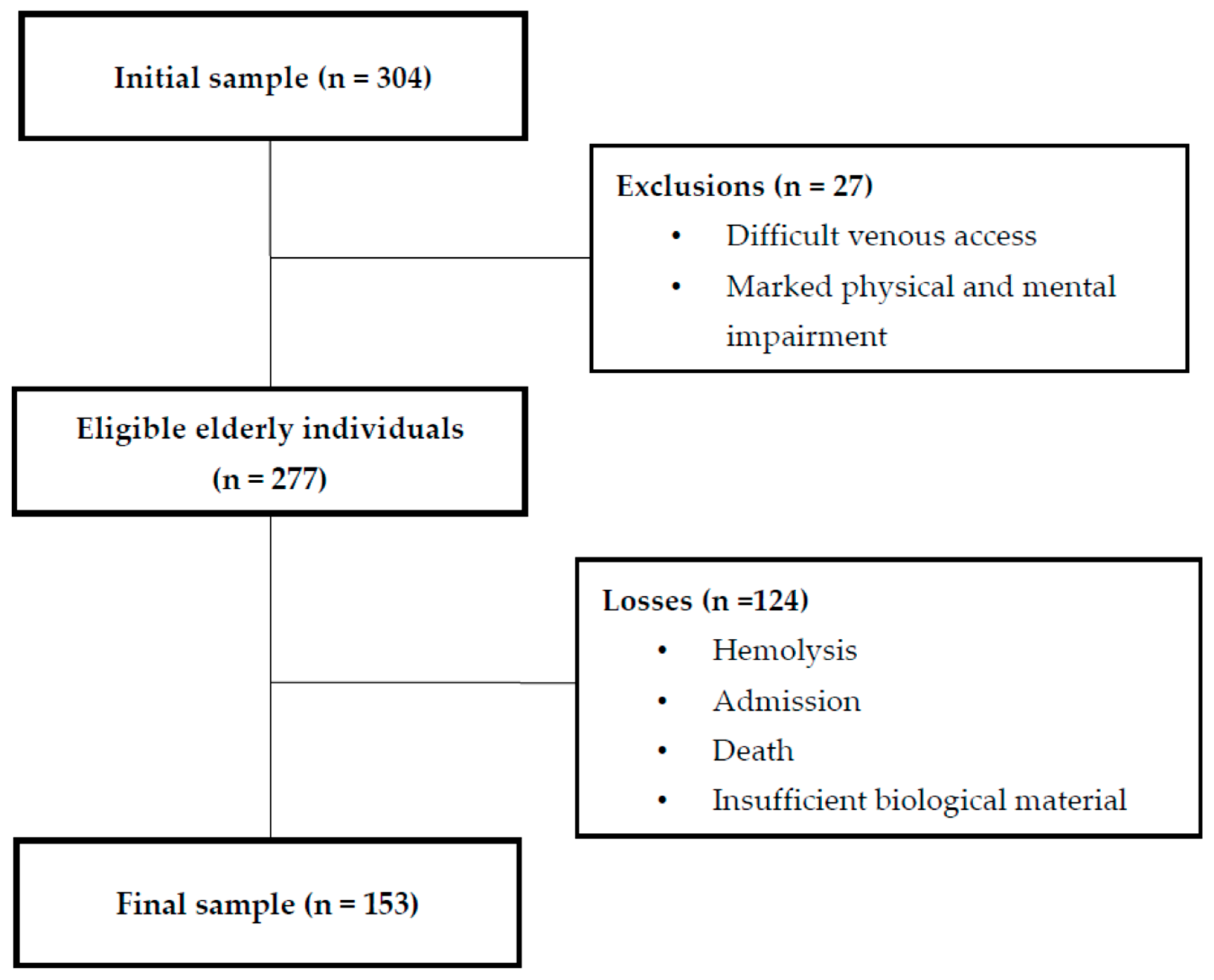
2.1. Study Population
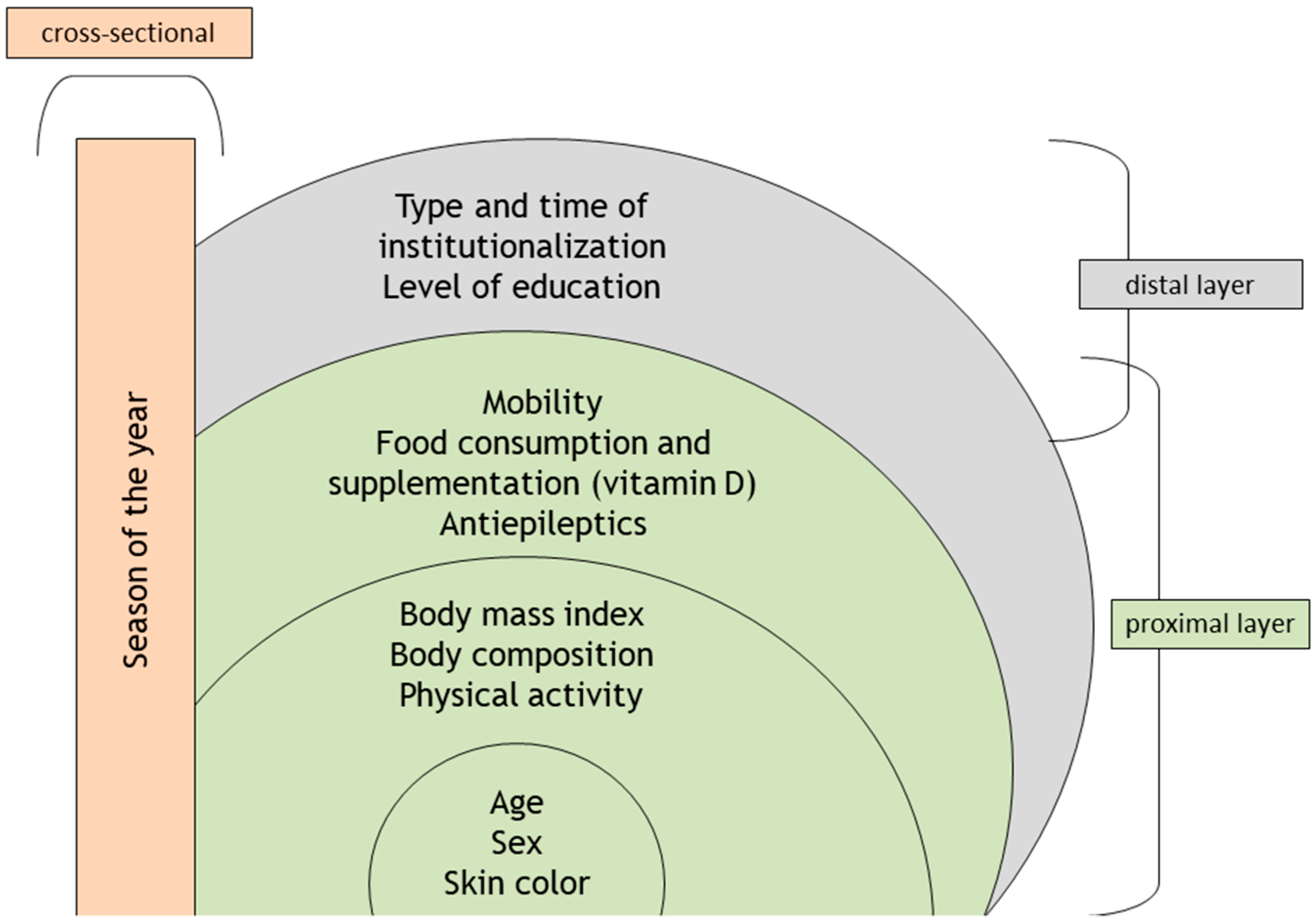
2.2. Theoretical Model of the Study
2.3. Analysis of 25(OH)D Serum Concentration
2.4. Dietary Intake
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- UNFPA. Ageing in the Twenty-First Century: A Celebration and A Challenge; UNFPA: New York, NY, USA, 2012; ISBN 9780897149815. [Google Scholar]
- BRASIL Sinopse Do Censo Demográfico. Available online: http://www.ibge.gov.br/home/estatistica/populacao/censo2010/sinopse/default_sinopse.shtm (accessed on 22 August 2017).
- Veldurthy, V.; Wei, R.; Oz, L.; Dhawan, P.; Jeon, Y.H.; Christakos, S. Vitamin D, calcium homeostasis and aging. Bone Res. 2016, 4, 16041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ter Borg, S.; Verlaan, S.; Hemsworth, J.; Mijnarends, D.M.; Schols, J.M.G.A.; Luiking, Y.C.; De Groot, L.C. Micronutrient intakes and potential inadequacies of community-dwelling older adults: A systematic review. Br. J. Nutr. 2015, 113, 1195–1206. [Google Scholar] [CrossRef] [PubMed]
- Berridge, M.J. Vitamin D deficiency accelerates ageing and age-related diseases: A novel hypothesis. J. Physiol. 2017, 595, 6825–6836. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Endocrine Society Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.E.S.; Maeda, S.S.; Batista, M.C.; Lazaretti-Castro, M.; Vasconcellos, L.S.; Madeira, M.; Soares, L.M.; Borba, V.Z.C.; Moreira, C.A. Posicionamento oficial da Sociedade Brasileira de Patologia Clínica/Medicina Laboratorial (SBPC/ML) e da Sociedade Brasileira de Endocrinologia e Metabologia (SBEM) sobre intervalos de referência da vitamina D [25(OH)D]. J. Bras. Patol. Med. Lab. 2017, 53, 377–381. [Google Scholar]
- Flicker, L. Vitamin D and the endocrinology of ageing. Curr. Opin. Endocr. Metab. Res. 2019, 5, 7–10. [Google Scholar] [CrossRef]
- Feng, X.; Guo, T.; Wang, Y.; Kang, D.; Che, X.; Zhang, H.; Cao, W.; Wang, P. The vitamin D status and its effects on life quality among the elderly in Jinan, China. Arch. Gerontol. Geriatr. 2016, 62, 26–29. [Google Scholar] [CrossRef]
- Salminen, M.; Saaristo, P.; Salonoja, M.; Vaapio, S.; Vahlberg, T.; Lamberg-Allardt, C.; Aarnio, P.; Kivelä, S.-L. Vitamin D status and physical function in older Finnish people: A one-year follow-up study. Arch. Gerontol. Geriatr. 2015, 61, 419–424. [Google Scholar] [CrossRef]
- Dawson-Hughes, B. Vitamin D and muscle function. J. Steroid Biochem. Mol. Biol. 2017, 173, 313–316. [Google Scholar] [CrossRef]
- Pilz, S.; Dobnig, H.; Tomaschitz, A.; Kienreich, K.; Meinitzer, A.; Friedl, C.; Wagner, D.; Piswanger-Sölkner, C.; März, W.; Fahrleitner-Pammer, A. Low 25-hydroxyvitamin D is associated with increased mortality in female nursing home residents. J. Clin. Endocrinol. Metab. 2012, 97, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Skaaby, T.; Husemoen, L.L.N.; Thuesen, B.H.; Pisinger, C.; Hannemann, A.; Jørgensen, T.; Linneberg, A. Longitudinal associations between lifestyle and vitamin D: A general population study with repeated vitamin D measurements. Endocrine 2016, 51, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.A.; Gordon, M.; Labranche, J.M.; Murray, T.M.; Vieth, R.; Shear, N.H. Seasonal prevalence of vitamin D deficiency in institutionalized older adults. J. Am. Geriatr. Soc. 1997, 45, 598–603. [Google Scholar] [CrossRef] [PubMed]
- Mosekilde, L. Vitamin D and the elderly. Clin. Endocrinol. 2005, 62, 265–281. [Google Scholar] [CrossRef] [PubMed]
- De Jongh, R.T.; Van Schoor, N.M.; Lips, P. Changes in vitamin D endocrinology during aging in adults. Mol. Cell. Endocrinol. 2017, 453, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Samefors, M.; Östgren, C.J.; Mölstad, S.; Lannering, C.; Midlöv, P.; Tengblad, A. Vitamin D deficiency in elderly people in Swedish nursing homes is associated with increased mortality. Eur. J. Endocrinol. 2014, 170, 667–675. [Google Scholar] [CrossRef] [Green Version]
- Saraiva, G.L.; Cendoroglo, M.S.; Ramos, L.R.; Araújo, L.M.Q.; Vieira, J.G.H.; Maeda, S.S.; Borba, V.Z.C.; Kunii, I.; Hayashi, L.F.; Lazaretti-Castro, M. Prevalência da deficiência, insuficiência de vitamina D e hiperparatiroidismo secundário em idosos institucionalizados e moradores na comunidade da cidade de São Paulo, Brasil. Arq. Bras. Endocrinol. Metabol. 2007, 51, 437–442. [Google Scholar] [CrossRef]
- Maeda, S.S.; Kunii, I.S.; Hayashi, L.F.; Lazaretti-Castro, M. Increases in summer serum 25-hydroxyvitamin D (25OHD) concentrations in elderly subjects in São Paulo, Brazil vary with age, gender and ethnicity. BMC Endocr. Disord. 2010, 10, 12. [Google Scholar] [CrossRef]
- Andersen, R.; Mølgaard, C.; Skovgaard, L.T.; Brot, C.; Cashman, K.D.; Chabros, E.; Charzewska, J.; Flynn, A.; Jakobsen, J.; Karkkainen, M.; et al. Teenage girls and elderly women living in northern Europe have low winter vitamin D status. Eur. J. Clin. Nutr. 2005, 59, 533–541. [Google Scholar] [CrossRef]
- Mowé, M.; Bohmer, T.; Haug, E. Serum calcidiol and calcitriol concentrations in elderly people: Variations with age, sex, season and disease. Clin. Nutr. 1996, 15, 201–206. [Google Scholar] [CrossRef]
- Pérez-Llamas, F.; López-Contreras, M.J.; Blanco, M.J.; López-Azorín, F.; Zamora, S.; Moreiras, O. Seemingly paradoxical seasonal influences on vitamin D status in nursing-home elderly people from a Mediterranean area. Nutrition 2008, 24, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Pereira Machado, R.S.; Santa Cruz Coelho, M.A. Risk of malnutrition among Brazilian institutionalized elderly: A study with the Mini Nutritional Assessment (MNA) questionnaire. J. Nutr. Health Aging 2011, 15, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, R. Micronutrient deficiencies in the elderly—Could ready meals be part of the solution? J. Nutr. Sci. 2017, 6, 4. [Google Scholar] [CrossRef]
- Brazil. The Statute of the Elderly, Law 10741. 2003. Available online: http:// www.planalto.gov.br/ccivil_03/leis/2003/l10.741.htm (accessed on 15 April 2017).
- Open Source Epidemiologic Statistics for Public Health. Available online: https://www.openepi.com (accessed on 22 January 2018).
- Sales, M.C.M.C.; de Oliveira, L.P.; de Araújo Cabral, N.L.; de Sousa, S.E.S.; das Graças Almeida, M.; Lemos, T.M.A.M.; de Oliveira Lyra, C.; de Lima, K.C.; Sena-Evangelista, K.C.M.; de Fatima Campos Pedrosa, L.; et al. Plasma zinc in institutionalized elderly individuals: Relation with immune and cardiometabolic biomarkers. J. Trace Elem. Med. Biol. 2018, 50, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Características étnico-raciais da população: Classificações e identidades, 2nd ed.; IBGE: Rio de Janeiro, Brazil, 2013; ISBN 978-85-240-4244-7.
- Chumlea, W.A.; Roche, A.F.; Mukherjee, D. Nutritional Assessment of the Elderly Through Anthropometry; Ross Laboratories: Columbus, OH, USA, 1987. [Google Scholar]
- Lipschitz, D.A. Screening for nutritional status in the elderly. Prim. Care 1994, 21, 55–67. [Google Scholar]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation; Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) fin. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Kennerfalk, A.; Ruigómez, A.; Wallander, M.-A.; Wilhelmsen, L.; Johansson, S. Geriatric Drug Therapy and Healthcare Utilization in the United Kingdom. Ann. Pharmacother. 2002, 36, 797–803. [Google Scholar] [CrossRef]
- Cincura, C.; Pontes-Neto, O.M.; Neville, I.S.; Mendes, H.F.; Menezes, D.F.; Mariano, D.C.; Pereira, I.F.; Teixeira, L.A.; Jesus, P.A.P.; de Queiroz, D.C.L.; et al. Validation of the National Institutes of Health Stroke Scale, Modified Rankin Scale and Barthel Index in Brazil: The Role of Cultural Adaptation and Structured Interviewing. Cerebrovasc. Dis. 2009, 27, 119–122. [Google Scholar] [CrossRef]
- De Oliveira Neto, L.; Agrícola, P.M.D.; de Andrade, F.L.J.P.; de Oliveira, L.P.; Lima, K.C.; de Oliveira Neto, L.; Agrícola, P.M.D.; de Andrade, F.L.J.P.; de Oliveira, L.P.; Lima, K.C. What is the impact of the European Consensus on the diagnosis and prevalence of sarcopenia among institutionalized elderly persons? Rev. Bras. Geriatr. Gerontol. 2017, 20, 754–761. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of adl: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Martínez de la Iglesia, J.; Dueñas Herrero, R.; Onís Vilches, M.C.; Aguado Taberné, C.; Albert Colomer, C.; Luque Luque, R. Spanish language adaptation and validation of the Pfeiffer’s questionnaire (SPMSQ) to detect cognitive deterioration in people over 65 years of age. Med. Clin. 2001, 117, 129–134. [Google Scholar]
- LAVAT Laboratório de Váriaveis Ambientais e Tropicais. Available online: http://www.crn.inpe.br/lavat/ (accessed on 8 May 2019).
- Nusser, S.M.; Carriquiry, A.L.; Dodd, K.W.; Fuller, W.A. A semiparametric transformation approach to estimating usual daily intake distributions. J. Am. Stat. Assoc. 1996, 91, 1440–1449. [Google Scholar] [CrossRef]
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Subcommittee on Interpretation and Uses of Dietary Reference Intakes; Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes: Applications in Dietary Assessment; National Academies Press: Washington, DC, USA, 2000; ISBN 978-0-309-07183-3. [Google Scholar]
- Van Dam, R.M.; Snijder, M.B.; Dekker, J.M.; Stehouwer, C.D.; Bouter, L.M.; Heine, R.J.; Lips, P. Potentially modifiable determinants of vitamin D status in an older population in the Netherlands: The Hoorn Study. Am. J. Clin. Nutr. 2007, 85, 755–761. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Solar UV Index: A Practical Guide. A Joint Recommendation of World Health Organization, World Meteorological Organization, United Nations Environment Programme and the International Commission on Non-Ionizing Radiation Protection; Library Cataloguing-in-Publication; WHO: Geneva, Switzerland, 2002; ISBN 92 4 159007 6.
- Lin, T.-C.; Liao, Y.-C. The impact of sunlight exposure on the health of older adults. J. Nurs. 2016, 63, 116–122. [Google Scholar]
- Okan, F.; Okan, S.; Zincir, H. Effect of Sunlight Exposure on Vitamin D Status of Individuals Living in a Nursing Home and Their Own Homes. J. Clin. Densitom. 2018. In Press. [Google Scholar] [CrossRef]
- Komar, L.; Nieves, J.; Cosman, F.; Rubin, A.; Shen, V.; Lindsay, R. Calcium Homeostasis of an Elderly Population upon Admission to a Nursing Home. J. Am. Geriatr. Soc. 1993, 41, 1057–1064. [Google Scholar] [CrossRef]
- Oliveira, B.S.; Zunzunegui, M.V.; Quinlan, J.; Batistuzzo de Medeiros, S.R.; Thomasini, R.L.; Guerra, R.O. Lifecourse Adversity and Telomere Length in Older Women from Northeast Brazil. Rejuvenation Res. 2018, 21, 294–303. [Google Scholar] [CrossRef]
- Jääskeläinen, T.; Itkonen, S.T.; Lundqvist, A.; Erkkola, M.; Koskela, T.; Lakkala, K.; Dowling, K.G.; Hull, G.L.; Kröger, H.; Karppinen, J.; et al. The positive impact of general vitamin D food fortification policy on vitamin D status in a representative adult Finnish population: Evidence from an 11-y follow-up based on standardized 25-hydroxyvitamin D data. Am. J. Clin. Nutr. 2017, 105, 1512–1520. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | n (%) | 95% CI |
|---|---|---|
| Sex | ||
| Male | 33 (21.6) | 3.30–15.00 |
| Female | 120 (78.4) | 3.30–71.90 |
| Skin color a | ||
| White | 70 (54.7) | 46.10–54.10 |
| Black | 25 (19.5) | 12.50–26.60 |
| Brown | 27 (21.1) | 14.10–28.90 |
| Other | 6 (4.7) | 1.60–8.60 |
| Marital status b | ||
| Single | 66 (52.0) | 42.50–60.60 |
| Widowed | 32 (25.2) | 18.10–33.10 |
| Married | 17 (13.4) | 7.90–19.70 |
| Separated/Divorced | 12 (9.4) | 3.70–17.30 |
| Level of education c | ||
| Illiterate | 43 (35.5) | 27.30–43.80 |
| Literate | 32 (26.4) | 18.20–34.70 |
| Elementary I (years 1–5) | 16 (13.2) | 6.60–19.00 |
| Elementary II (years 6–9) | 6 (5.0) | 1.70–9.10 |
| High School | 18 (14.9) | 8.30–21.50 |
| Higher Education | 6 (5.0) | 1.70–9.10 |
| Type of institution | ||
| Profit | 45 (29.4) | 22.20–37.20 |
| Nonprofit | 108 (70.6) | 62.80–77.80 |
| Time of institutionalization (mean) d | 29.38% | 24.72–34.04 |
| BMI (kg/m²) e | ||
| Thin | 55 (46.4) | 39.10–54.00 |
| Normal weight | 37 (31.1) | 23.90–39.50 |
| Excess weight | 27 (22.7) | 15.10–29.40 |
| Abdominal circumference f | ||
| Obese | 51 (40.5) | 31.80–50.00 |
| Non-obese | 75 (59.5) | 50.00–68.20 |
| Calf circumference g | ||
| Sign of lean mass loss | 88 (60.3) | 51.10–68.50 |
| No sign of lean mass loss | 58 (39.7) | 31.50–47.90 |
| Physical activity h | ||
| Inactive | 87 (70.2) | 67.80–81.50 |
| Active | 37 (29.8) | 18.50–32.20 |
| Mobility | ||
| Without mobility | 20 (13.1) | 7.80–19.00 |
| With mobility | 133 (86.9) | 81.00–92.20 |
| Sarcopenia g | 66 (45.2) | 46.60–63.00 |
| Cognition i | ||
| Preserved mental function | 13 (9.0) | 4.90–13.90 |
| Mild cognitive impairment | 9 (6.3) | 2.80–10.40 |
| Moderate cognitive impairment | 26 (18.1) | 11.80–25.00 |
| Severe cognitive impairment | 96 (66.7) | 58.40–74.30 |
| Multimorbidity b | 84 (66.1) | 57.50–74.00 |
| Polypharmacy j | 59 (38.6) | 34.80–50.70 |
| Use of antiepileptic medications | 27 (18.8) | 12.50–25.70 |
| Variables | Mean (SD) | 95% CI |
|---|---|---|
| Vitamin D intake (µg/day) | 2.8 (3.2) | 2.32–3.33 |
| Calcium intake (mg/day) | 997.9 (291.8) | 921.18–1074.64 |
| Serum 25(OH)D (ng/mL) a | 23.9 (16.6–31.0) | - |
| Local UV Index | ||
| Summer | 6.6 (0.5) | 6.45–6.66 |
| Spring | 6.6 (0.5) | 6.51–6.80 |
| Fall | 6.3 (0.4) | 6.48–6.99 |
| Vitamin D intake | ||
| Possibly inadequate | 146 (95.4) | 92.20–98.70 |
| Possibly adequate | 7 (4.6) | 1.30–7.80 |
| Calcium intake | ||
| Possibly inadequate | 122 (79.7) | 73.20–85.60 |
| Possibly adequate | 31 (20.3) | 14.40–26.80 |
| Vitamin D status b | ||
| Insufficient | 109 (71.2) | 64.70–78.40 |
| Sufficient | 44 (28.8) | 21.60–35.30 |
| Distribution by seasons | ||
| Summer | 92 (60.1) | 51.60–68.00 |
| Spring | 46 (30.1) | 22.90–37.90 |
| Fall | 15 (9.8) | 5.20–15.00 |
| Serum 25(OH)D (ng/mL) | ||||||
|---|---|---|---|---|---|---|
| Hypovitaminosis D (≤29) | Sufficient (30–60) | |||||
| n | % | n | % | PR a (95% CI) | p | |
| Sex | ||||||
| Male | 25 | 75.8 | 8 | 24.2 | 1.08 (0.86–1.36) | 0.518 |
| Female | 84 | 70.0 | 36 | 30.0 | ||
| Age | ||||||
| 75 years or older | 84 | 73.0 | 31 | 27.0 | 1.11 (0.86–1.43) | 0.392 |
| 60–74 years | 25 | 65.8 | 13 | 34.2 | ||
| Skin color | ||||||
| Non-white | 36 | 62.1 | 22 | 37.9 | 0.80 (0.63–1.02) | 0.063 |
| White | 54 | 77.1 | 16 | 22.9 | ||
| Type of institution | ||||||
| Nonprofit | 72 | 66.7 | 36 | 33.3 | 0.43 (0.18–1.03) | 0.053 |
| Profit | 37 | 82.2 | 8 | 17.8 | ||
| Body Mass Index | ||||||
| Non-normal weight | 83 | 72.3 | 31 | 27.2 | 0.63 (0.25–1.57) | 0.314 |
| Normal weight | 30 | 81.1 | 7 | 18.9 | ||
| Abdominal circumference | ||||||
| With abdominal fat | 39 | 76.5 | 12 | 23.5 | 0.85 (0.68–1.06) | 0.181 |
| Without abdominal fat | 49 | 65.3 | 26 | 34.7 | ||
| Calf circumference | ||||||
| Sign of muscle mass loss | 62 | 70.5 | 26 | 29.5 | 1.05 (0.86–1.29) | 0.628 |
| No sign of muscle mass loss | 43 | 74.1 | 15 | 25.9 | ||
| Physical activity | ||||||
| Inactive | 75 | 68.8 | 34 | 31.2 | 0.43 (0.16–1.12) | 0.078 |
| Active | 31 | 83.8 | 6 | 16.2 | ||
| Mobility | ||||||
| Yes | 17 | 85.0 | 3 | 15.0 | 1.23 (0.99–1.53) | 0.145 |
| No | 92 | 69.2 | 41 | 30.8 | ||
| Multimorbidity | ||||||
| Yes | 59 | 70.2 | 25 | 29.8 | 0.91 (0.77–1.23) | 0.828 |
| No | 31 | 72.1 | 12 | 27.9 | ||
| Falls | ||||||
| Yes | 4 | 80.0 | 1 | 20.0 | 1.12 (0.72–1.76) | 0.669 |
| None | 99 | 71.2 | 40 | 28.8 | ||
| Sarcopenia | ||||||
| Yes | 57 | 71.3 | 23 | 28.8 | 1.00 (0.81–1.23) | 0.996 |
| No | 47 | 71.2 | 19 | 28.8 | ||
| Cognition | ||||||
| Moderate to severe impairment | 89 | 73.0 | 33 | 27.0 | 1.33 (0.90–1.99) | 0.083 |
| Preserved to mild impairment | 12 | 54.5 | 10 | 45.5 | ||
| Depression | ||||||
| Depressed | 6 | 54.5 | 5 | 45.5 | 0.75 (0.13–1.30) | 0.198 |
| Non-depressed | 86 | 72.9 | 32 | 27.1 | ||
| Functional status | ||||||
| Reduced independence | 68 | 67.3 | 33 | 32.7 | 0.88 (0.71–1.08) | 0.251 |
| Independent | 36 | 76.6 | 11 | 23.4 | ||
| Seasons of the year | ||||||
| Other seasons | 38 | 62.3 | 23 | 37.7 | 0.49 (0.24–1.00) | 0.046 |
| Summer | 71 | 77.2 | 21 | 22.8 | ||
| Vitamin D intake | ||||||
| Possibly inadequate | 104 | 71.2 | 42 | 28.8 | 1.00 (0.62–1.61) | 0.991 |
| Possibly adequate | 5 | 71.4 | 2 | 28.6 | ||
| Dietary Calcium | ||||||
| Possibly inadequate | 117 | 95.9 | 5 | 4.1 | 1.02 (0.93–1.13) | 0.576 |
| Possibly adequate | 29 | 93.5 | 2 | 6.5 | ||
| Vitamin D supplementation | ||||||
| Yes | 87 | 70.2 | 37 | 29.8 | 1.05 (0.65–1.69) | 0.825 |
| No | 6 | 66.7 | 3 | 33.3 | ||
| Antiepileptic medications | ||||||
| Yes | 19 | 70.4 | 8 | 29.6 | 0.98 (0.75–1.28) | 0.882 |
| No | 84 | 71.8 | 33 | 28.2 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousa, S.E.S.; Sales, M.C.; Araújo, J.R.T.; Sena-Evangelista, K.C.M.; Lima, K.C.; Pedrosa, L.F.C. High Prevalence of Hypovitaminosis D in Institutionalized Elderly Individuals is Associated with Summer in a Region with High Ultraviolet Radiation Levels. Nutrients 2019, 11, 1516. https://doi.org/10.3390/nu11071516
Sousa SES, Sales MC, Araújo JRT, Sena-Evangelista KCM, Lima KC, Pedrosa LFC. High Prevalence of Hypovitaminosis D in Institutionalized Elderly Individuals is Associated with Summer in a Region with High Ultraviolet Radiation Levels. Nutrients. 2019; 11(7):1516. https://doi.org/10.3390/nu11071516
Chicago/Turabian StyleSousa, Sara Estéfani S., Márcia Cristina Sales, José Rodolfo T. Araújo, Karine C.M. Sena-Evangelista, Kenio C. Lima, and Lucia F.C. Pedrosa. 2019. "High Prevalence of Hypovitaminosis D in Institutionalized Elderly Individuals is Associated with Summer in a Region with High Ultraviolet Radiation Levels" Nutrients 11, no. 7: 1516. https://doi.org/10.3390/nu11071516