Fluid Restriction Decreases Solid Food Consumption Post-Exercise


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Preliminary Testing
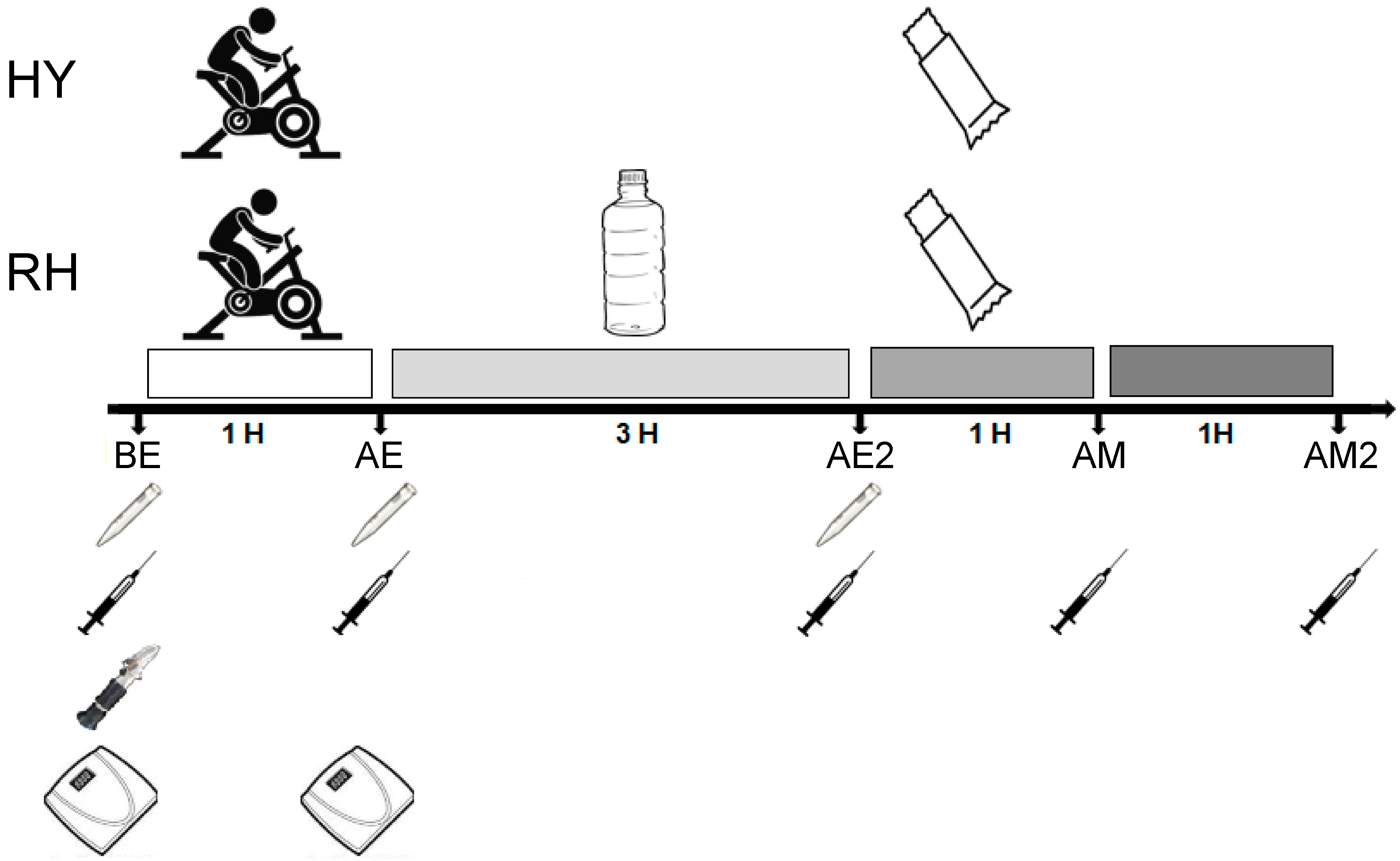
2.3. Experimental Trial
2.4. Measurements of Urine Specific Gravity (USG)
2.5. Hormone Measurements
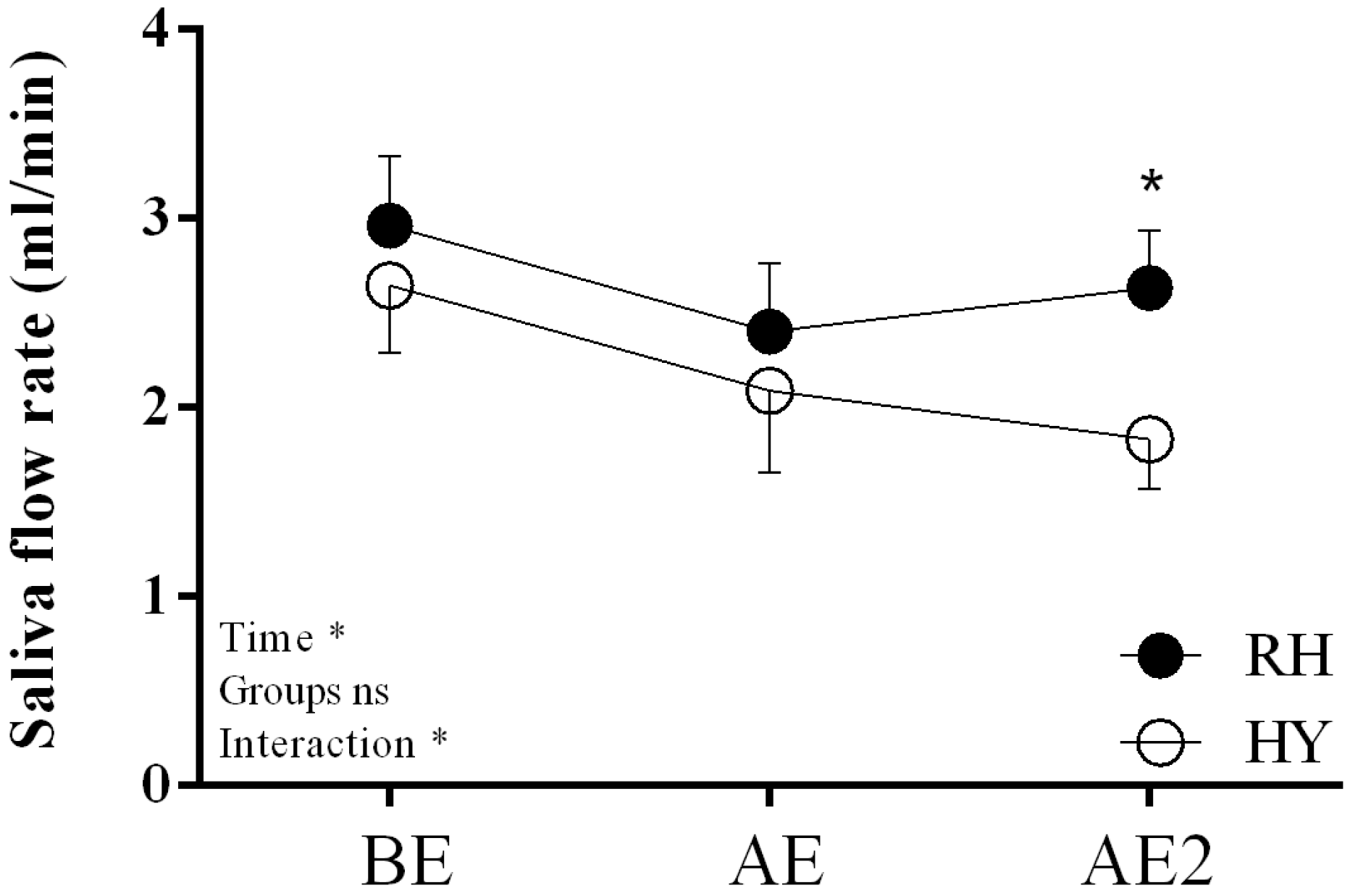
2.6. Saliva Measurements
2.7. Energy Intake
2.8. Statistical Analyses
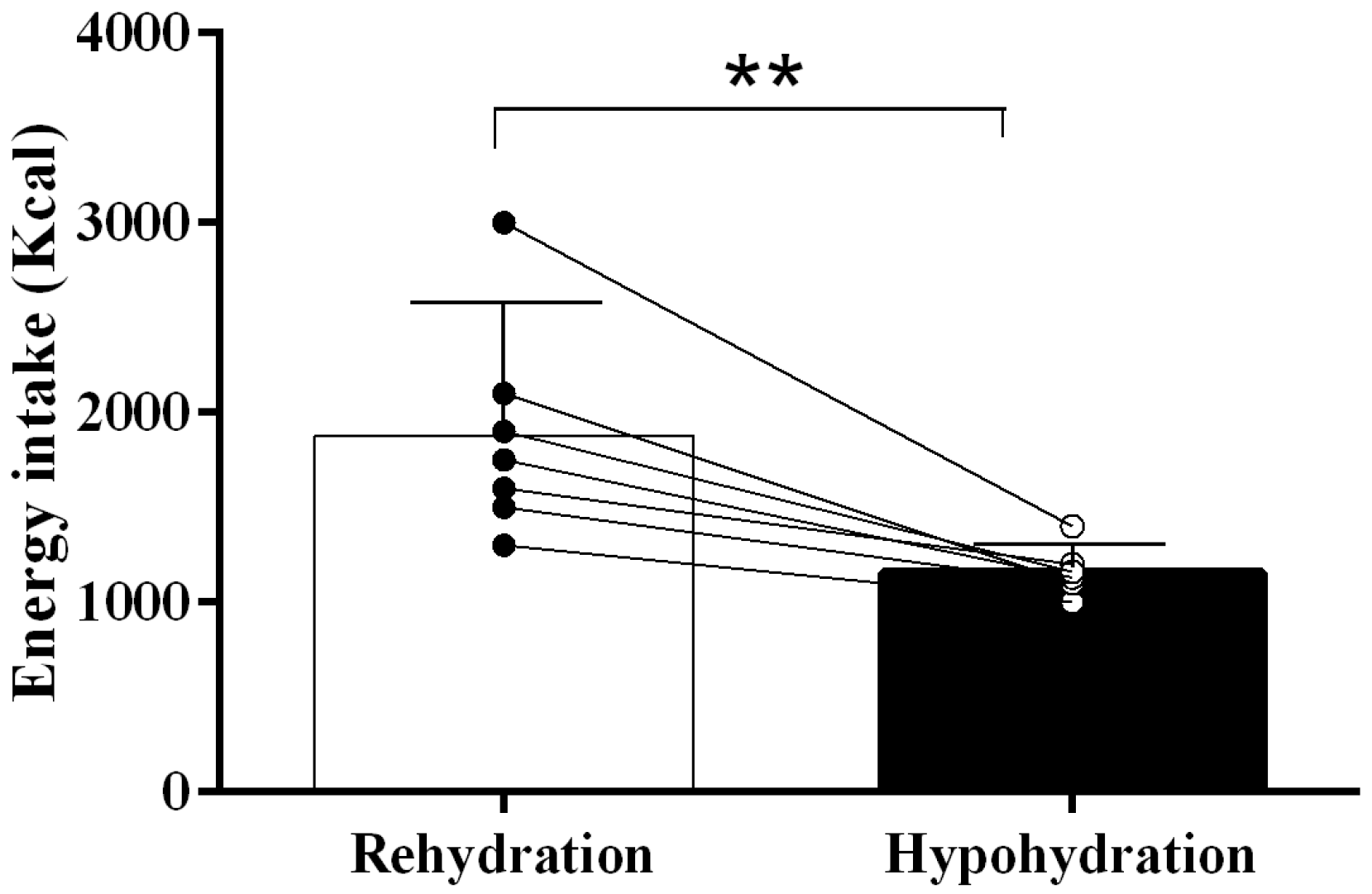
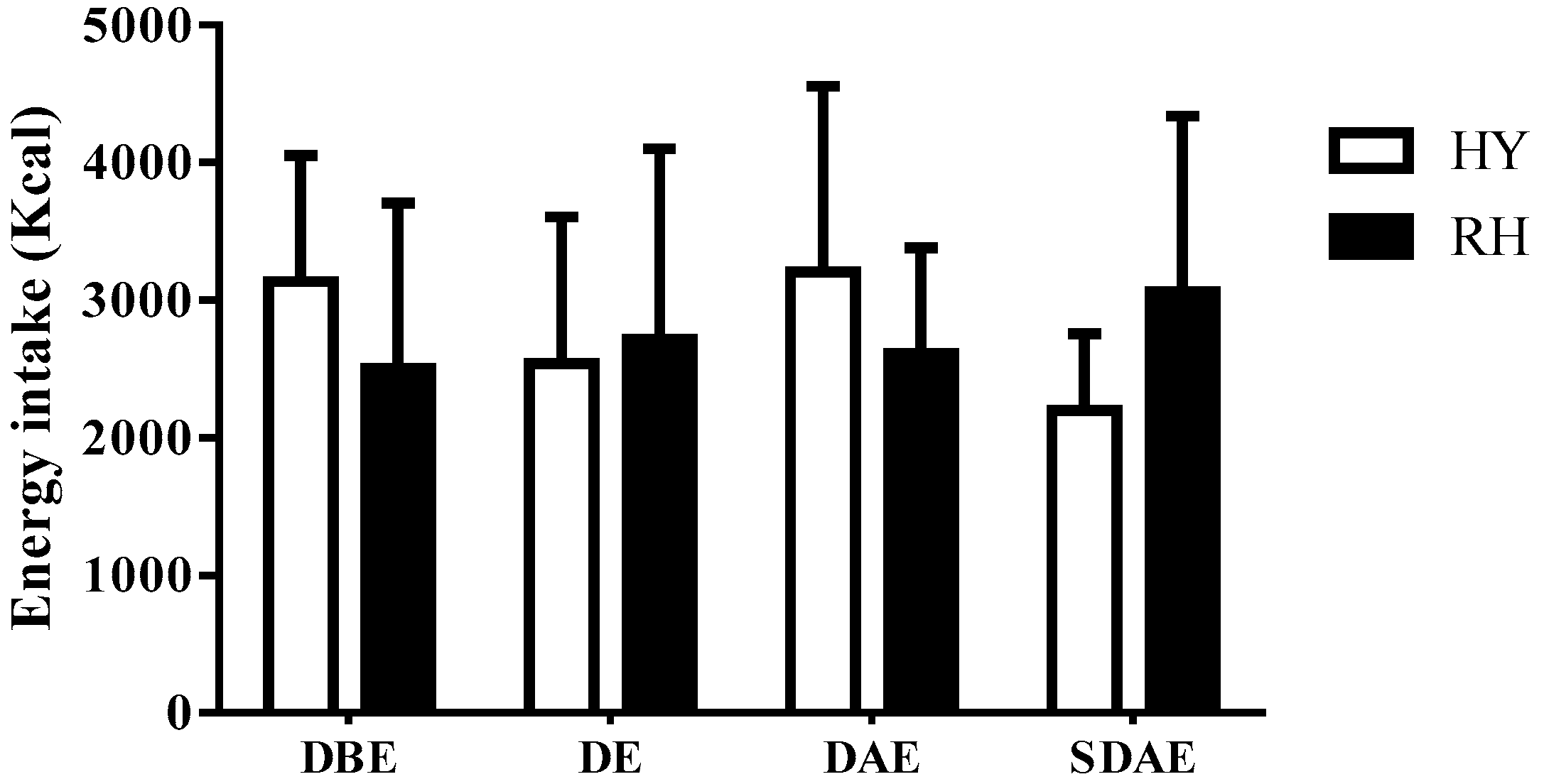
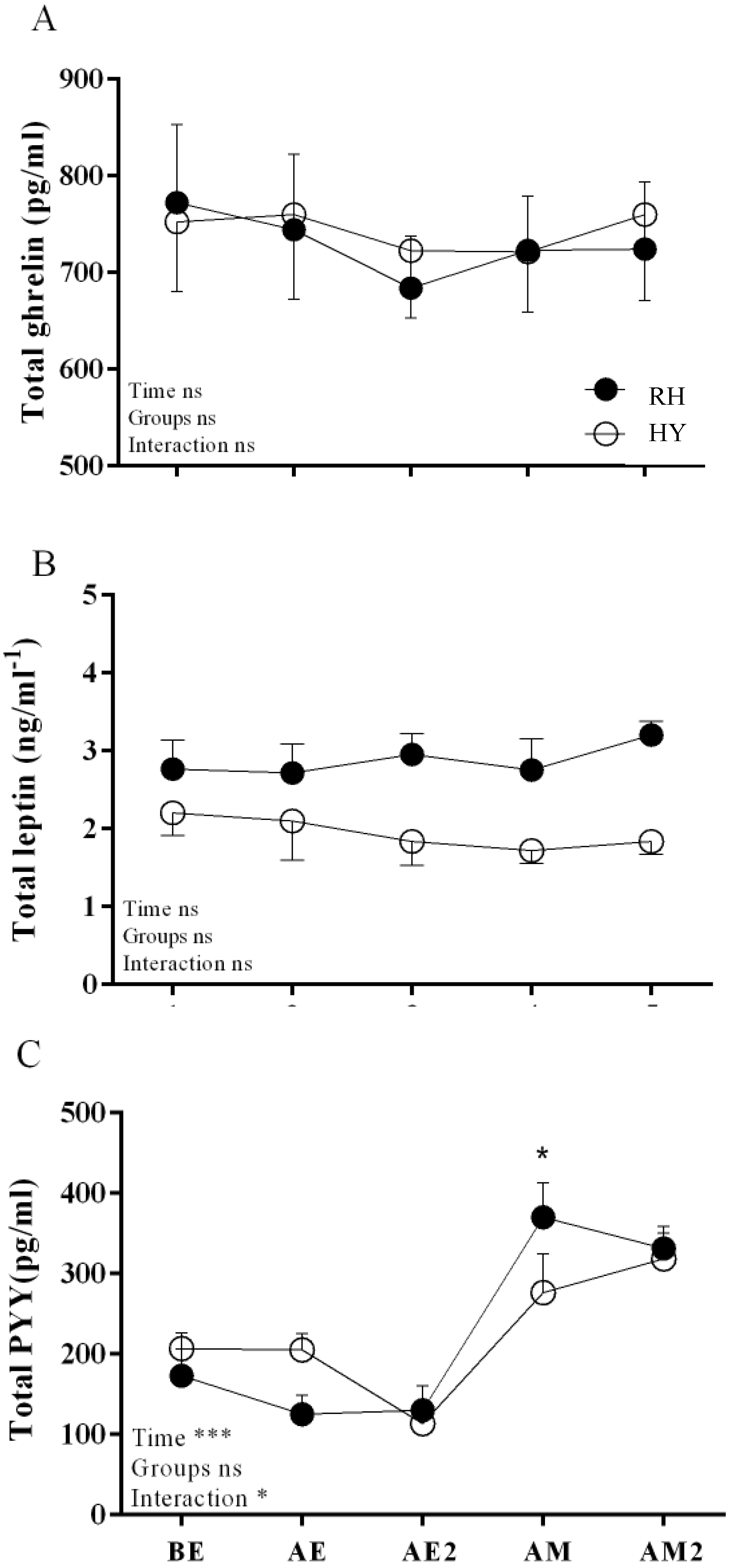
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wren, A.; Bloom, S. Gut hormones and appetite control. Gastroenterology 2007, 132, 2116–2130. [Google Scholar] [CrossRef]
- Farooqi, I.S.; Bullmore, E.; Keogh, J.; Gillard, J.; O’rahilly, S.; Fletcher, P.C. Leptin regulates striatal regions and human eating behavior. Science 2007, 317, 1355. [Google Scholar] [CrossRef] [PubMed]
- Watts, A.G. Dehydration-associated anorexia: Development and rapid reversal. Physiol. Behav. 1999, 65, 871–878. [Google Scholar] [CrossRef]
- Watts, A.G.; Boyle, C.N. The functional architecture of dehydration-anorexia. Physiol. Behav. 2010, 14, 472–477. [Google Scholar] [CrossRef]
- Engell, D. Interdependency of food and water intake in humans. Appetite 1988, 10, 133–141. [Google Scholar] [CrossRef]
- Shirreffs, S.M.; Merson, S.J.; Fraser, S.M.; Archer, D.T. The effects of fluid restriction on hydration status and subjective feelings in man. Br. J. Nutr. 2004, 91, 951–958. [Google Scholar] [CrossRef]
- Kelly, P.J.; Guelfi, K.J.; Wallman, K.E.; Fairchild, T.J. Mild dehydration does not reduce postexercise appetite or energy intake. Med. Sci. Sports Exerc. 2012, 44, 516–524. [Google Scholar] [CrossRef]
- Corney, R.A.; Sunderland, C.; James, L.J. The effect of hydration status on appetite and energy intake. J. Sports Sci. 2015, 33, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Brennan, I.M.; Feltrin, K.L.; Nair, N.S.; Hausken, T.; Little, T.J.; Gentilcore, D.; Wishart, J.M.; Jones, K.L.; Horowitz, M.; Feinle-Bisset, C. Effects of the phases of the menstrual cycle on gastric emptying, glycemia, plasma GLP-1 and insulin, and energy intake in healthy lean women. Am. J. Physiol. Gastrointest. Liver Physiol. 2009, 297, G602–G610. [Google Scholar] [CrossRef] [Green Version]
- Thompson, P.; Arena, R.; Riebe, D.; Pescatello, L. American College of Sports M. ACSM’s new preparticipation health screening recommendations from ACSM’s guidelines for exercise testing and prescription. Curr. Sports Med. Rep. 2013, 12, 215–217. [Google Scholar] [CrossRef]
- Shirreffs, S.M.; Taylor, A.J.; Leiper, J.B.; Maughan, R.J. Post-exercise rehydration in man: Effects of volume consumed and drink sodium content. Med. Sci. Sports Exerc. 1996, 28, 1260–1271. [Google Scholar] [CrossRef]
- American College of Sports Medicine; Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American College of Sports Medicine position stand. Exercise and fluid replacement. Med. Sci. Sports Exerc. 2007, 39, 377–390. [Google Scholar] [PubMed]
- Castro-Sepúlveda, M.; Astudillo, S.; Álvarez, C.; Zapata-Lamana, R.; Zbinden-Foncea, H.; Ramírez-Campillo, R.; Jorquera, C. [PREVALENCE OF DEHYDRATION BEFORE TRAINING IN PROFESIONAL CHILEAN SOCCER PLAYERS]. Nutr. Hosp. 2015, 1, 308–311. [Google Scholar]
- Miletic, I.; Schiffman, S.; Miletic, V.; Sattely-Miller, E. Salivary IgA secretion rate in young and elderly persons. Physiol. Behav. 1996, 60, 243–248. [Google Scholar] [CrossRef]
- Le Roux, C.; Batterham, R.; Aylwin, S.; Patterson, M.; Borg, C.; Wynne, K.; Kent, A.; Vincent, R.; Gardiner, J.; Ghatei, M. Attenuated peptide YY release in obese subjects is associated with reduced satiety. Endocrinology 2006, 147, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Walsh, N.P.; Montague, J.C.; Callow, N.; Rowlands, A.V. Saliva flow rate, total protein concentration and osmolality as potential markers of whole body hydration status during progressive acute dehydration in humans. Oral Biol. 2004, 49, 149–154. [Google Scholar] [CrossRef]
- Munoz, C.X.; Johnson, E.C.; Demartini, J.K.; Huggins, R.A.; Mckenzie, A.L.; Casa, D.J.; Maresh, C.M.; Armstrong, L.E. Assessment of hydration biomarkers including salivary osmolality during passive and active dehydration. Eur. J. Clin. Nutr. 2013, 67, 1257–1263. [Google Scholar] [CrossRef]
- Russ, M.J.; Ackerman, S.H. Salivation and depression: A role for appetitive factors. Appetite 1987, 8, 37–47. [Google Scholar] [CrossRef]
- Humphrey, S.P.; Williamson, R.T. A review of saliva: Normal composition, flow, and function. J. Prosthet. Dent. 2001, 85, 162–169. [Google Scholar] [CrossRef]
- Scalera, G. Taste preference and acceptance in thirsty and rehydrated [correction of dehydrated] rats. Physiol. Behav. 2000, 71, 457–468. [Google Scholar] [CrossRef]
- Corney, R.A.; Sunderland, C.; James, L.J. Immediate pre-meal water ingestion decreases voluntary food intake in lean young males. Eur. J. Nutr. 2016, 55, 815–819. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (%) | RH | HY | p-Value |
|---|---|---|---|
| CHO | 57 ± 08 | 55 ± 11 | 0.49 |
| Protein | 31 ± 07 | 32 ± 08 | 0.61 |
| Fat | 12 ± 04 | 13 ± 03 | 0.78 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Luco, C.; Díaz-Castro, F.; Jorquera, C.; Troncoso, R.; Zbinden-Foncea, H.; Johannsen, N.M.; Castro-Sepulveda, M. Fluid Restriction Decreases Solid Food Consumption Post-Exercise. Nutrients 2019, 11, 1209. https://doi.org/10.3390/nu11061209
Pérez-Luco C, Díaz-Castro F, Jorquera C, Troncoso R, Zbinden-Foncea H, Johannsen NM, Castro-Sepulveda M. Fluid Restriction Decreases Solid Food Consumption Post-Exercise. Nutrients. 2019; 11(6):1209. https://doi.org/10.3390/nu11061209
Chicago/Turabian StylePérez-Luco, Cristian, Francisco Díaz-Castro, Carlos Jorquera, Rodrigo Troncoso, Hermann Zbinden-Foncea, Neil M Johannsen, and Mauricio Castro-Sepulveda. 2019. "Fluid Restriction Decreases Solid Food Consumption Post-Exercise" Nutrients 11, no. 6: 1209. https://doi.org/10.3390/nu11061209