Micronutrients Deficiencies in 374 Severely Malnourished Anorexia Nervosa Inpatients

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients and Study Design
2.2. Ethical Aspects
2.3. Measures and Procedure
2.4. Statistical Analysis
3. Results
3.1. Patients Characteristics
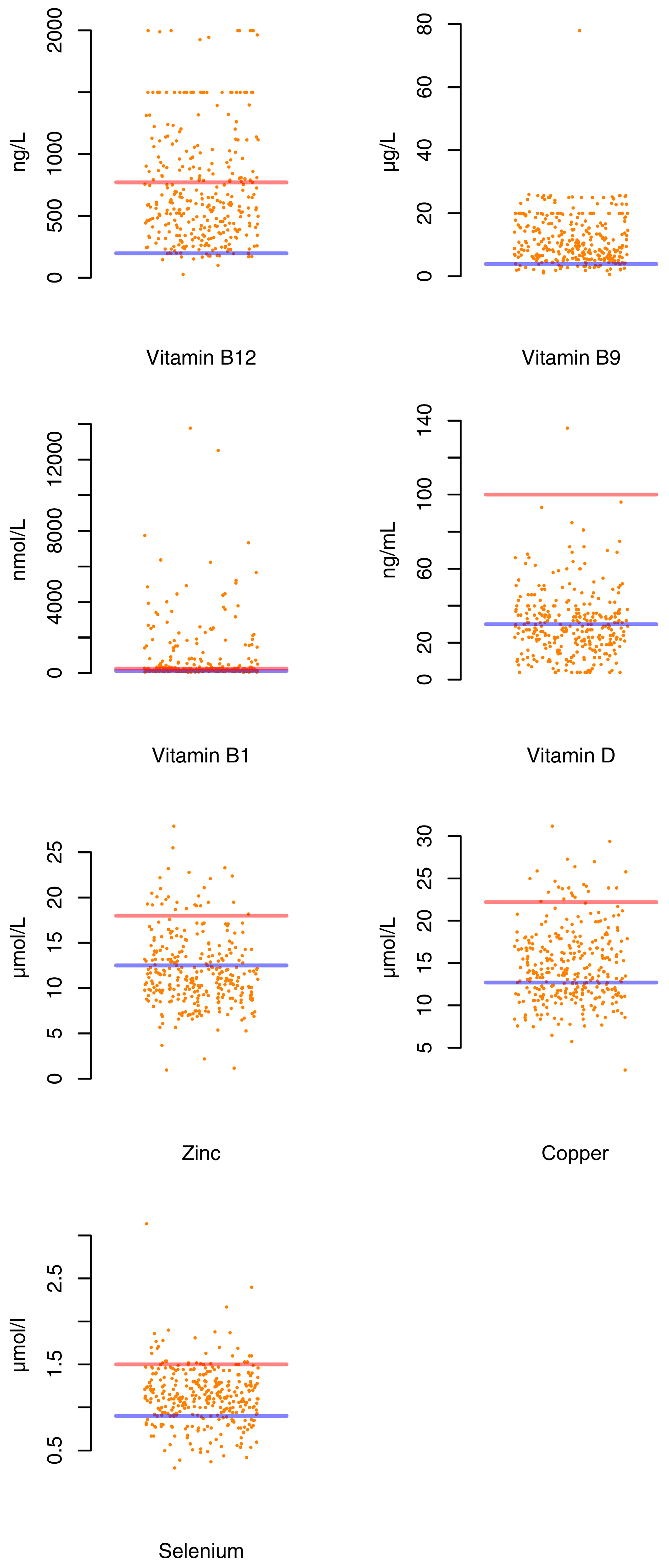
3.2. Prevalence of Micronutrients Deficiencies
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hudson, J.I.; Hiripi, E.; Pope, H.G.; Kessler, R.C. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar]
- Keski-Rahkonen, A.; Hoek, H.W.; Susser, E.S.; Linna, M.S.; Sihvola, E.; Raevuori, A.; Bulik, C.M.; Kaprio, J.; Rissanen, A. Epidemiology and course of anorexia nervosa in the community. Am. J. Psychiatry 2007, 164, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Huas, C.; Caille, A.; Godart, N.; Foulon, C.; Pham-Scottez, A.; Divac, S.; Dechartres, A.; Lavoisy, G.; Guelfi, J.D.; Rouillon, F.; et al. Factors predictive of ten-year mortality in severe anorexia nervosa patients. Acta Psychiatr. Scand. 2011, 123, 62–70. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Mental Disorders, 5th Edition (DSM-5); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Mattar, L.; Huas, C.; Duclos, J.; Apfel, A.; Godart, N. Relationship between malnutrition and depression or anxiety in Anorexia Nervosa: A critical review of the literature. J. Affect. Disord. 2011, 132, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Rizk, M.; Lalanne, C.; Berthoz, S.; Kern, L.; Godart, N. Problematic Exercise in Anorexia Nervosa: Testing Potential Risk Factors against Different Definitions. PLoS ONE 2015, 10, e0143352. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, F.C.; Ekbom, A.; Brandt, L.; Ekselius, L. Excess mortality, causes of death and prognostic factors in anorexia nervosa. Br. J. Psychiatry J. Ment. Sci. 2009, 194, 10–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, C.; Mehler, P.S. Medical complications of anorexia nervosa and their treatments: An update on some critical aspects. Eat. Weight Disord. 2015, 20, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Escudero, C.A.; Potts, J.E.; Lam, P.-Y.; De Souza, A.M.; Mugford, G.J.; Sandor, G.G.S. An Echocardiographic Study of Left Ventricular Size and Cardiac Function in Adolescent Females with Anorexia Nervosa. Eur. Eat. Disord. 2016, 24, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Hanachi, M.; Melchior, J.C.; Crenn, P. Hypertransaminasemia in severely malnourished adult anorexia nervosa patients: Risk factors and evolution under enteral nutrition. Clin. Nutr. Edinb. Scotl. 2013, 32, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Abraham, S.; Kellow, J.E. Do the digestive tract symptoms in eating disorder patients represent functional gastrointestinal disorders? BMC Gastroenterol. 2013, 13, 38. [Google Scholar] [CrossRef]
- De Filippo, E.; Marra, M.; Alfinito, F.; Di Guglielmo, M.L.; Majorano, P.; Cerciello, G.; De Caprio, C.; Contaldo, F.; Pasanisi, F. Hematological complications in anorexia nervosa. Eur. J. Clin. Nutr. 2016, 70, 1305–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baranowska, B.; Kochanowski, J. Neuroendocrine aspects of anorexia nervosa and bulimia nervosa. Neuro Endocrinol. Lett. 2018, 39, 172–178. [Google Scholar] [PubMed]
- Narayanan, V.; Gaudiani, J.L.; Mehler, P.S. Serum albumin levels may not correlate with weight status in severe anorexia nervosa. Eat. Disord. 2009, 17, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, D.; Sogni, P.; Hammel, P.; Melchior, J.C.; Angel, L.; Rozen, R.; Labarre, C.; Mignon, M.; Apfelbaum, M. Anorexia nervosa: Absence of sensitivity to nutritional protein markers. Study of 23 patients and comparison to a paired group with colonic Crohn’s disease. Annales de Medecine Interne 1989, 140, 86–90. [Google Scholar] [PubMed]
- Suzuki, H.; Asakawa, A.; Li, J.B.; Tsai, M.; Amitani, H.; Ohinata, K.; Michio, K.; Akio, I. Zinc as an appetite stimulator—The possible role of zinc in the progression of diseases such as cachexia and sarcopenia. Recent Pat. Food Nutr. Agric. 2011, 3, 226–231. [Google Scholar] [CrossRef]
- Franques, J.; Chiche, L.; Mathis, S. Sensory Neuronopathy Revealing Severe Vitamin B12 Deficiency in a Patient with Anorexia Nervosa: An Often-Forgotten Reversible Cause. Nutrients 2017, 9, 281. [Google Scholar] [CrossRef] [PubMed]
- Oudman, E.; Wijnia, J.W.; Oey, M.J.; van Dam, M.J.; Postma, A. Preventing Wernicke’s encephalopathy in anorexia nervosa: A systematic review. Psychiatry Clin. Neurosci. 2018, 72, 774–779. [Google Scholar] [CrossRef]
- Rio, A.; Whelan, K.; Goff, L.; Reidlinger, D.P.; Smeeton, N. Occurrence of refeeding syndrome in adults started on artificial nutrition support: Prospective cohort study. BMJ Open 2013, 3, e002173. [Google Scholar] [CrossRef]
- Haute Autorité de Santé. Prise en charge de l’anorexie mentale. Available online: https://www.has-sante.fr/portail/jcms/c_985715/fr/anorexie-mentale-prise-en-charge (accessed on 5 April 2019).
- National Institute of Health and Care Exellence (NICE). Eating Disorders: Recognition and Treatment. 2017. Available online: nice.org.uk/guidance/ng69 (accessed on 1 April 2019).
- Battle, D.E. Diagnostic and Statistical Manual of Mental Disorders (DSM). Codas 2013, 25, 191–192. [Google Scholar]
- Hadigan, C.M.; Anderson, E.J.; Miller, K.K.; Hubbard, J.L.; Herzog, D.B.; Klibanski, A.; Grinspoon, S.K. Assessment of macronutrient and micronutrient intake in women with anorexia nervosa. Int. J. Eat. Disord. 2000, 28, 284–292. [Google Scholar] [CrossRef]
- Chiurazzi, C.; Cioffi, I.; De Caprio, C.; De Filippo, E.; Marra, M.; Sammarco, R.; Di Guglielmo, M.L.; Contaldo, F.; Pasanisi, F. Adequacy of nutrient intake in women with restrictive anorexia nervosa. Nutrition 2017, 38, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Rautou, P.E.; Cazals-Hatem, D.; Moreau, R.; Francoz, C.; Feldmann, G.; Lebrec, D.; Ogier-Denis, É.; Bedossa, P.; Valla, D.; Durand, F. Acute liver cell damage in patients with anorexia nervosa: A possible role of starvation-induced hepatocyte autophagy. Gastroenterology 2008, 135, 840.e3–848.e3. [Google Scholar] [CrossRef] [PubMed]
- Tozzi, F.; Thornton, L.M.; Klump, K.L.; Fichter, M.M.; Halmi, K.A.; Kaplan, A.S.; Strober, M.; Woodside, D.B.; Crow, S.; Mitchell, J.; et al. Symptom fluctuation in eating disorders: Correlates of diagnostic crossover. Am. J. Psychiatry 2005, 162, 732–740. [Google Scholar] [CrossRef]
- Eddy, K.T.; Dorer, D.J.; Franko, D.L.; Tahilani, K.; Thompson-Brenner, H.; Herzog, D.B. Diagnostic crossover in anorexia nervosa and bulimia nervosa: Implications for DSM-V. Am. J. Psychiatry 2008, 165, 245–250. [Google Scholar] [CrossRef]
- Castro, J.; Deulofeu, R.; Gila, A.; Puig, J.; Toro, J. Persistence of nutritional deficiencies after short-term weight recovery in adolescents with anorexia nervosa. Int. J. Eat. Disord. 2004, 35, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, C.L.; Gritzner, S. How does zinc supplementation benefit anorexia nervosa? Eat. Weight Disord. 2006, 11, e109–e111. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, C.L.; Goldner, E.M.; Bakan, R. Controlled trial of zinc supplementation in anorexia nervosa. Int. J. Eat. Disord. 1994, 15, 251–255. [Google Scholar] [PubMed]
- Su, J.C.; Birmingham, C.L. Zinc supplementation in the treatment of anorexia nervosa. Eat. Weight Disord. 2002, 7, 20–22. [Google Scholar] [CrossRef]
- Achamrah, N.; Coëffier, M.; Rimbert, A.; Charles, J.; Folope, V.; Petit, A.; Déchelotte, P.; Grigioni, S. Micronutrient Status in 153 Patients with Anorexia Nervosa. Nutrients 2017, 9, 225. [Google Scholar] [CrossRef]
- Mohee, K.; Kucharska-Pietura, K.; Karthigeyan, A.; Naqvi, A. Diagnostic and treatment dilemmas of persistent chronic hypokalaemia in a patient with anorexia nervosa: A case report. J. Med. Case Rep. 2014, 8, 294. [Google Scholar] [CrossRef]
- Davidson, A.; Anisman, P.C.; Eshaghpour, E. Heart failure secondary to hypomagnesemia in anorexia nervosa. Pediatr. Cardiol. 1992, 13, 241–242. [Google Scholar] [CrossRef]
- Ewan, S.-L.; Moynihan, P.C. Cardiac arrest: First presentation of anorexia nervosa. BMJ Case Rep. 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, H.; Kanda, F.; Matsushita, T.; Chihara, K.; Itoh, K. White muscle disease in humans: Myopathy caused by selenium deficiency in anorexia nervosa under long term total parenteral nutrition. J. Neurol. Neurosurg. Psychiatry 1999, 67, 829–830. [Google Scholar] [CrossRef] [PubMed]
- Agnello, E.; Malfi, G.; Costantino, A.M.; Massarenti, P.; Pugliese, M.; Fortunati, N.; Catalano, M.G.; Palmo, A. Tumour necrosis factor alpha and oxidative stress as maintaining factors in the evolution of anorexia nervosa. Eat. Weight Disord. 2012, 17, e194–e199. [Google Scholar] [CrossRef] [PubMed]
- Solmi, M.; Veronese, N.; Luchini, C.; Manzato, E.; Sergi, G.; Favaro, A.; Santonastaso, P.; Correll, C.U. Oxidative Stress and Antioxidant Levels in Patients with Anorexia Nervosa after Oral Re-alimentation: A Systematic Review and Exploratory Meta-analysis. Eur. Eat. Disord. 2016, 24, 101–105. [Google Scholar] [CrossRef]
- Chandrakumar, A.; Bhardwaj, A.; Jong, G.W. Review of thiamine deficiency disorders: Wernicke encephalopathy and Korsakoff psychosis. J. Basic Clin. Physiol. Pharmacol. 2018. [Google Scholar] [CrossRef]
- Tang, L.; Alsulaim, H.A.; Canner, J.K.; Prokopowicz, G.P.; Steele, K.E. Prevalence and predictors of postoperative thiamine deficiency after vertical sleeve gastrectomy. Surg. Obes. Relat. Dis. 2018, 14, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Aasheim, E.T. Wernicke encephalopathy after bariatric surgery: A systematic review. Ann. Surg. 2008, 248, 714–720. [Google Scholar]
- Winston, A.P.; Jamieson, C.P.; Madira, W.; Gatward, N.M.; Palmer, R.L. Prevalence of thiamin deficiency in anorexia nervosa. Int. J. Eat. Disord. 2000, 28, 451–454. [Google Scholar] [CrossRef]
- Matak, P.; Zumerle, S.; Mastrogiannaki, M.; Balkhi, S.E.; Delga, S.; Mathieu, J.R.R.; Canonne-Hergaux, F.; Poupon, J.; Sharp, P.A.; Vaulont, S.; et al. Copper Deficiency Leads to Anemia, Duodenal Hypoxia, Upregulation of HIF-2α and Altered Expression of Iron Absorption Genes in Mice. PLoS ONE 2013, 8, e59538. [Google Scholar] [CrossRef]
- Khera, D.; Sharma, B.; Singh, K. Copper deficiency as a cause of neutropenia in a case of coeliac disease. BMJ Case Rep. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, D.M. Copper, iron, and selenium dietary deficiencies negatively impact skeletal integrity: A review. Exp. Biol. Med. 2016, 241, 1316–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatti, D.; Ghoch, M.E.; Viapiana, O.; Ruocco, A.; Chignola, E.; Rossini, M.; Giollo, A.; Idolazzi, L.; Adami, S.; Dalle Grave, R. Strong relationship between vitamin D status and bone mineral density in anorexia nervosa. Bone 2015, 78, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Tasegian, A.; Curcio, F.; Dalla Ragione, L.; Rossetti, F.; Cataldi, S.; Codini, M.; Ambesi-Impiombato, F.S.; Beccari, T.; Albi, E. Hypovitaminosis D3, Leukopenia, and Human Serotonin Transporter Polymorphism in Anorexia Nervosa and Bulimia Nervosa. Mediat. Inflamm. 2016, 2016, 8046479. [Google Scholar] [CrossRef] [PubMed]
- Divasta, A.D.; Feldman, H.A.; Brown, J.N.; Giancaterino, C.; Holick, M.F.; Gordon, C.M. Bioavailability of vitamin D in malnourished adolescents with anorexia nervosa. J. Clin. Endocrinol. Metab. 2011, 96, 2575–2580. [Google Scholar] [CrossRef] [PubMed]
- Giollo, A.; Idolazzi, L.; Caimmi, C.; Fassio, A.; Bertoldo, F.; Dalle Grave, R.; El Ghoch, M.; Calugi, S.; Bazzani, P.V.; Viapiana, O.; et al. Vitamin D levels strongly influence bone mineral density and bone turnover markers during weight gain in female patients with anorexia nervosa. Int. J. Eat. Disord. 2017, 50, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Misra, M. Long-term skeletal effects of eating disorders with onset in adolescence. Ann. N. Y. Acad. Sci. 2008, 1135, 212–218. [Google Scholar] [CrossRef]
- Corbetta, F.; Tremolizzo, L.; Conti, E.; Ferrarese, C.; Neri, F.; Bomba, M.; Nacinovich, R. Paradoxical increase of plasma vitamin B12 and folates with disease severity in anorexia nervosa. Int. J. Eat. Disord. 2015, 48, 317–322. [Google Scholar] [CrossRef]
- Hercberg, S.; Preziosi, P.; Galan, P.; Deheeger, M.; Papoz, L.; Dupin, H. Dietary intake of a representative sample of the population of Val-de-Marne; III. Mineral and vitamin intake. Rev. Epidemiol. Sante Publique 1991, 39, 245–261. [Google Scholar]
- Arnaud, J.; Bertrais, S.; Roussel, A.M.; Arnault, N.; Ruffieux, D.; Favier, A.; Berthelin, S.; Estaquio, C.; Galan, P.; Czernichow, S.; et al. Serum selenium determinants in French adults: The SU.VI.M.AX study. Br. J. Nutr. 2006, 95, 313–320. [Google Scholar] [CrossRef]
- Anorexie Mentale: Prise en Charge. Available online: http://www.has-sante.fr/portail/jcms/c_985715/fr/anorexie-mentale-prise-en-charge (accessed on 5 April 2019).
- National Institute of Health and Care Exellence. Eating Disorders: Recognition and Treatment; National Institute of Health and Care Exellence: London, UK, 2017. [Google Scholar]


{kind=link}
| Clinical and Biological Parameters | N | AN-BP | AN-R | P |
|---|---|---|---|---|
| Patients (n, %) | 374 | 121 (32%) | 253 (68%) | |
| Gender | 360 (96.3%) Women | 117 (96.7%) | 243 (96%) | NS |
| 14 (3.7%) Men | 4 (3.3%) | 10 (4.1%) | NS | |
| Age (year) | 31.3 ± 12.9 | 29,41 (23.73, 37.09) | 26,22 (19.98, 38.29) | 0.029 |
| Weight (kg) | 33.7 ± 5.9 | 34.40 (30.00, 39.10) | 32,40 (29.60, 36.80) | 0.048 |
| Height (m) | 1.6 ± 0.07 | 1.64 (1.60, 1.68) | 1.62 (1.59, 1.68) | NS |
| BMI (18.5–24.9 kg/m2) | 12.5 ± 1.7 | 12.80 (11.25, 14.20) | 12.30 (11.30, 13.50) | NS |
| Fat Mass (g) | 3098 ± 1744 | 2715.00 (2236.75, 4073.73) | 2505.60 (2165.75, 3381.02) | NS |
| Fat Mass (%) | 9702 ± 4057 | 8.60 (7.75, 12.45) | 8.50 (7.40, 9.43) | NS |
| Disease duration (year) | 9.4 ± 9.2 | 10.00 (5.00, 16.00) | 4.50 (2.00, 12.00) | <0.001 |
| Albumin (38–52 g/L) | 37 ± 6.8 | 38.00 (32.00, 42.00) | 37.75 (34.00, 41.00) | NS |
| CRP (<5 mg/L) | 4 ± 14.5 | 0.71 (0.50, 1.20) | 0.70 (0.50, 1.45) | NS |
| TSH (0.55–4.78 mUI/L) | 1.9 ± 1.5 | 1.35 (0.90, 2.23) | 1.62 (1.14, 2.35) | NS |
| Ca (2.12–2.52 mmol/L) | 2.2 ± 0.17 | 2.25 (2.17, 2.38) | 2.22 (2.14, 2.30) | NS |
| Ph (0.8–1.45 mmol/L) | 1.2 ± 1.6 | 1.15 (0.94, 1.27) | 1.15 (0.98, 1.31) | NS |
| AST (15–37 UI/L) | 60.4 ± 116.3 | 28.00 (21.00, 38.00) | 29.00 (21.00, 54.00) | NS |
| ALT (12–78 UI/L) | 109 ± 232.8 | 36.00 (26.25, 65.75) | 51.00 (30.00, 103.50) | 0.001 |
| GGT (5–55 UI/L) | 63.1 ± 135.6 | 29.00 (18.00, 56.50) | 34.00 (20.00, 59.00) | NS |
| ALP (46–116 UI/L) | 90.2 ± 105.3 | 70.00 (52.75, 95.50) | 70.00 (53.00, 94.00) | NS |
| BNP (<100 ng/L) | 47.3 ± 68.4 | 20.00 (9.00, 46.00) | 31.00 (15.00, 52.75) | 0.021 |
| LVEF (>50%) | 64.87 ± 7708 | 65.00 (57.00, 67.00) | 66.00 (61.00, 71.00) | 0.009 |
| Deficiencies Number | % of Patients |
|---|---|
| None deficiency | 7.2% |
| One deficiency | 28.3% |
| Two deficiency | 33.2% |
| Three deficiency | 18.8% |
| Four and more deficiency | 12.6% |
| Micronutrients | AN-BP | AN-R | p |
|---|---|---|---|
| Zinc (12.5–18 micromol/L) | 11.10 (9.05, 13.20) | 11.45 (9.50, 14.07) | NS |
| Copper (12.7–22.2 micromol/L) | 15.25 (11.75, 17.70) | 13.50 (11.30, 16.72) | 0.022 |
| Selenium (0.9–1.5 micromol/L) | 1.02 (0.83, 1.21) | 1.18 (1.00, 1.38) | <0.001 |
| Vitamin B12 (197–77 1ng/L) | 516.00 (337.00, 804.00) | 608.50 (394.25, 976.75) | 0.036 |
| Vitamin B9 (>3.90 microg/L) | 9.32 (6.18, 14.70) | 10.66 (6.19, 17.55) | NS |
| Vitamin D (30–100 ng/mL) | 26.00 (15.75, 35.25) | 29.00 (20.75, 36.25) | NS |
| Vitamin B1 (126–250 nmol/L) | 188.50 (150.00, 334.25) | 195.00 (148.00, 457.00) | NS |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanachi, M.; Dicembre, M.; Rives-Lange, C.; Ropers, J.; Bemer, P.; Zazzo, J.-F.; Poupon, J.; Dauvergne, A.; Melchior, J.-C. Micronutrients Deficiencies in 374 Severely Malnourished Anorexia Nervosa Inpatients. Nutrients 2019, 11, 792. https://doi.org/10.3390/nu11040792
Hanachi M, Dicembre M, Rives-Lange C, Ropers J, Bemer P, Zazzo J-F, Poupon J, Dauvergne A, Melchior J-C. Micronutrients Deficiencies in 374 Severely Malnourished Anorexia Nervosa Inpatients. Nutrients. 2019; 11(4):792. https://doi.org/10.3390/nu11040792
Chicago/Turabian StyleHanachi, Mouna, Marika Dicembre, Claire Rives-Lange, Jacques Ropers, Pauline Bemer, Jean-Fabien Zazzo, Joël Poupon, Agnès Dauvergne, and Jean-Claude Melchior. 2019. "Micronutrients Deficiencies in 374 Severely Malnourished Anorexia Nervosa Inpatients" Nutrients 11, no. 4: 792. https://doi.org/10.3390/nu11040792