Bone Mineral Metabolism Status, Quality of Life, and Muscle Strength in Older People

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Procedures
2.2.1. Questionnaires
2.2.2. Physical Performance Measures
2.2.3. Biochemical Blood Analysis
2.3. Statistical Analyses
3. Results
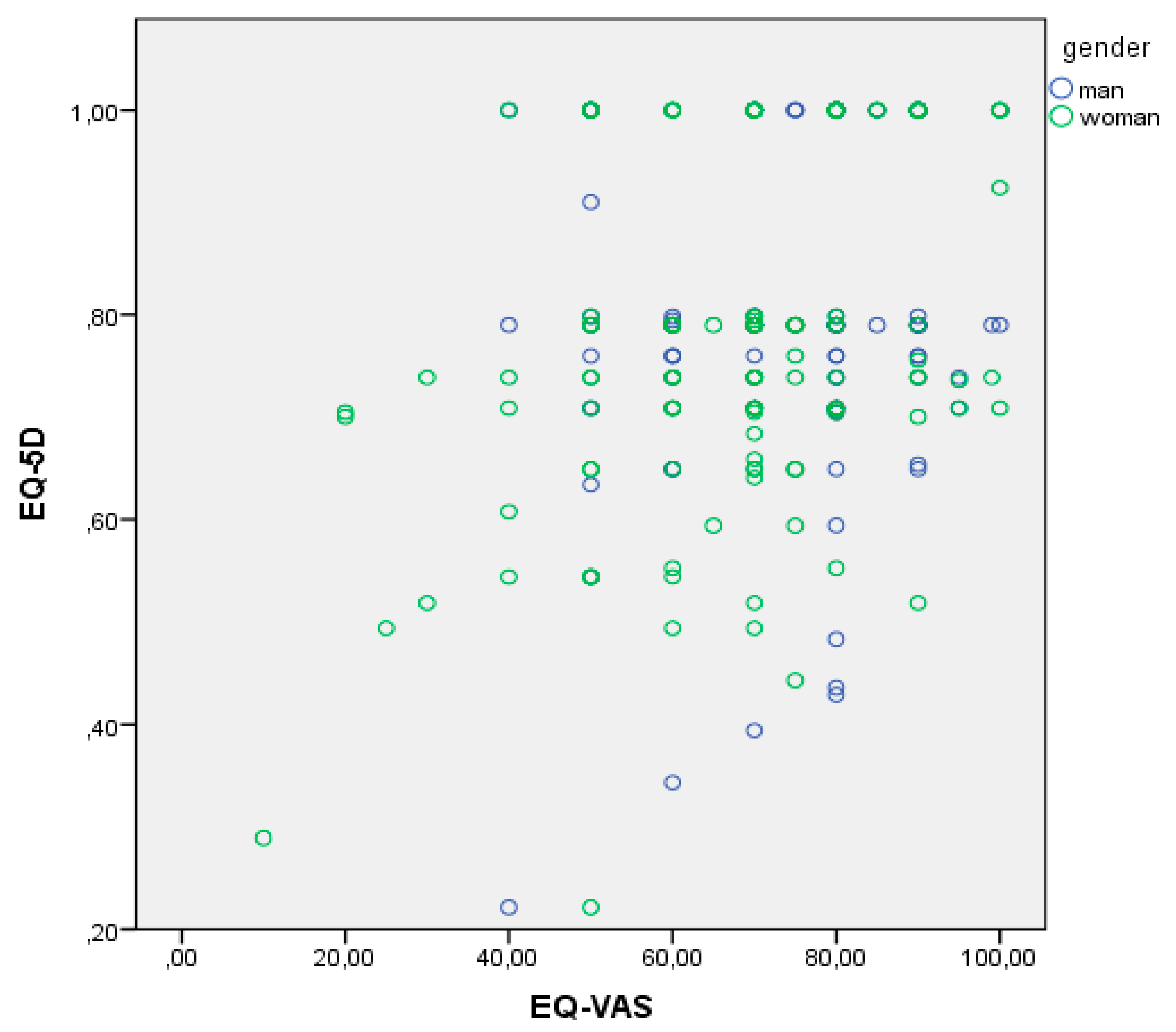
Associations between EQ-5D, Hand Grip, and MNA and Mineral Metabolism Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Alb | Albumin |
| BMI | Body mass index |
| Ca2+ | Calcium |
| CGR | Clinical group risk |
| CKD | Chronic kidney disease |
| 1,25(OH)2D3 | 1, 25-dihydroxyvitamin D3 |
| EQ-5D | EuroQoL-5 dimensions |
| EQ-VAS | EQ-5D-visual analogue scale |
| FGF23 | Fibroblast growth factor-23 |
| 25 (OH)D3 | 25-hydroxyvitamin D3 |
| IOM | Institute of Medicine |
| iPTH | Intact parathyroid hormone |
| MMSE | Mini Mental State Examination |
| MNA | Mini Nutritional Assessment |
| PASE | Physical Activity Scale for the Elderly |
| QoL | Quality of life |
| SD | Standard deviation |
| VDRs | Vitamin D receptors |
References
- Holick, M.F. Vitamin D: A D-lightful solution for health. J. Investig. Med. 2011, 59, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D. Calcium and Vitamin D. Novartis Found. Symp. 2007, 282, 123–142. [Google Scholar] [PubMed]
- Lips, P. Vitamin D physiology. Prog. Biophys. Mol. Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Mendes, J.; Santos, A.; Borges, N.; Afonso, C.; Moreira, P.; Padrão, P.; Negrão, R.; Amaral, T.F. Vitamin D status and functional parameters: A cross-sectional study in an older population. PLoS ONE 2018, 13, e0201840. [Google Scholar] [CrossRef] [PubMed]
- Kaur, J.; Ferguson, S.L.; Freitas, E.; Miller, R.; Bemben, D.; Knehans, A.; Bemben, M. Association of vitamin d status with chronic disease risk factors and cognitive dysfunction in 50–70 year old adults. Nutrients 2019, 11, 141. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G. Vitamin D: Past, present and future perspectives in the prevention of chronic diseases. Eur. J. Clin. Nutr. 2018, 79, 1221–1225. [Google Scholar] [CrossRef] [PubMed]
- Sondarwa, K.; Buttar, R.S.; Hensley, V.; Melamed, M.L. Vitamin D and Cardiovascular Disease. In Contemporary Endocrinology; Humana Press Inc.: Totowa, NJ, USA, 2018; pp. 151–164. [Google Scholar]
- Tejwani, V.; Qian, Q. Calcium regulation and bone mineral metabolism in elderly patients with chronic kidney disease. Nutrients 2013, 29, 1913–1936. [Google Scholar] [CrossRef] [PubMed]
- Bahlas, S.; Mushtaq Ahmed, M. Calcium and vitamin D nutrition and bone disease of the elderly. Life Sci. J. 2014, 11, 362–369. [Google Scholar]
- Timpini, A.; Pini, L.; Tantucci, C.; Cossi, S.; Grassi, V. Vitamin D and health status in elderly. Intern. Emerg. Med. 2011, 6, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016. Lancet 2017, 16, 1211–1259. [Google Scholar] [CrossRef]
- Seene, T.; Kaasik, P. Role of exercise therapy in prevention of decline in aging muscle function: Glucocorticoid myopathy and unloading. J. Aging Res. 2012, 2012, 172492. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.W.; Chen, W.L.; Lin, F.G.; Fang, W.H.; Yen, M.Y.; Hsieh, C.C.; Kao, T.W. Frailty and its impact on health-related quality of life: A cross-sectional study on elder community-dwelling preventive health service users. PLoS ONE 2012, 7, e38079. [Google Scholar] [CrossRef] [PubMed]
- Rabin, R.; Oemar, M.; Oppe, M.; Janssen, B.; Herdman, M. EQ-5D-5L user guide. In Basic Information How to Use EQ-5D-5L Instrument; EuroQol Research Foundation: Rotterdam, The Netherlands, 2015; p. 28. [Google Scholar]
- Logan, S.L.; Gottlieb, B.H.; Maitl, S.B.; Meegan, D.; Spriet, L.L. The physical activity scale for the elderly (PASE) questionnaire; Does it predict physical health? Int. J. Environ. Res. Public Health 2013, 10, 3967–3986. [Google Scholar] [CrossRef] [PubMed]
- Secher, M.; Soto, M.E.; Villars, H.; Van Kan, G.A.; Vellas, B. The Mini Nutritional Assessment (MNA) after 20 years of research and clinical practice. Rev. Clin. Gerontol. 2008, 23, 388–396. [Google Scholar] [CrossRef]
- Liu, C.J.; Marie, D.; Fredrick, A.; Bertram, J.; Utley, K.; Fess, E.E. Predicting hand function in older adults: Evaluations of grip strength, arm curl strength, and manual dexterity. Aging Clin. Exp. Res. 2017, 29, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Massy-Westropp, N.M.; Gill, T.K.; Taylor, A.W.; Bohannon, R.W.; Hill, C.L. Hand Grip Strength: Age and gender stratified normative data in a population-based study. BMC Res. Notes 2011, 4, 127. [Google Scholar] [CrossRef] [PubMed]
- Alley, D.E.; Shardell, M.D.; Peters, K.W.; McLean, R.R.; Dam, T.T.L.; Kenny, A.M.; Fragala, M.S.; Harris, T.B.; Kiel, D.P.; Guralnik, J.M.; et al. Grip strength cutpoints for the identification of clinically relevant weakness. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Mata-Granados, J.M.; Luque de Castro, M.D.; Quesada Gomez, J.M. Inappropriate serum levels of retinol, α-tocopherol, 25 hydroxyvitamin D3 and 24,25 dihydroxyvitamin D3 levels in healthy Spanish adults: Simultaneous assessment by HPLC. Clin. Biochem. 2008, 41, 676–680. [Google Scholar] [CrossRef] [PubMed]
- Navarro Valverde, C.; Quesada Gómez, J.M. Deficiencia de vitamina D en España: ¿Realidad o mito? Rev. Osteoporos. Metab. Miner. 2014, 6, 5–10. [Google Scholar] [CrossRef]
- González-Molero, I.; Morcillo, S.; Valdés, S.; Pérez-Valero, V.; Botas, P.; Delgado, E.; Hernández, D.; Olveira, G.; Rojo, G.; Gutierrez-Repiso, C.; et al. Vitamin D deficiency in Spain: A population-based cohort study. Eur. J. Clin. Nutr. 2011, 62, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Glendenning, P. Measuring vitamin D. Aust. Prescr. 2015, 38, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Sobocki, P.; Ekman, M.; Ågren, H.; Krakau, I.; Runeson, B.; Mårtensson, B.; Jönsson, B. Health-related quality of life measured with EQ-5D in patients treated for depression in primary care. Value Health 2007, 10, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, G.; Garin, O.; Pardo, Y.; Vilagut, G.; Pont, À.; Suárez, M.; Neira, M.; Rajmil, L.; Gorostiza, I.; Ramallo-Fariña, Y.; et al. Validity of the EQ–5D–5L and reference norms for the Spanish population. Qual. Life Res. 2018, 27, 2337–2348. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.S.; Ekwaru, J.P.; Ohinmaa, A.; Griener, G.; Veugelers, P.J. Vitamin D and health-related quality of life in a community sample of older Canadians. Qual. Life Res. 2014, 23, 2569–2575. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed]
- Signorello, L.B.; McLaughlin, J.K.; Lipworth, L.; Friis, S.; Sørensen, H.T.; Blot, W.J. Confounding by indication in epidemiologic studies of commonly used analgesics. Am. J. Ther. 2002, 9, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Delgado-Rodríguez, M.; Alonso, A.; Schlatter, J.; Lahortiga, F.; Serra-Majem, L.; Martínez-González, M.A. Association of the Mediterranean dietary pattern with the incidence of depression: The Seguimiento Universidad de Navarra/University of Navarra follow-up (SUN) cohort. Arch. Gen. Psychiatry 2009, 66, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, J.A.; Edmondson, D.; Wasson, L.T.; Falzon, L.; Homma, K.; Ezeokoli, N.; Li, P.; Davidson, K.W. Vitamin D supplementation for depressive symptoms: A systematic review and meta-analysis of randomized controlled trials. Psychosom. Med. 2014, 76, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Kimball, S.M.; Mirhosseini, N.; Rucklidge, J. Database analysis of depression and anxiety in a community sample—Response to a micronutrient intervention. Nutrients 2018, 10, 152. [Google Scholar] [CrossRef] [PubMed]
- Garcion, E.; Wion-Barbot, N.; Montero-Menei, C.N.; Berger, F.; Wion, D. New clues about vitamin D functions in the nervous system. Trends Endocrinol. Metab. 2002, 13, 100–105. [Google Scholar] [CrossRef]
- Obradovic, D.; Gronemeyer, H.; Lutz, B.; Rein, T. Cross-talk of vitamin D and glucocorticoids in hippocampal cells. J. Neurochem. 2006, 96, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Puchacz, E.; Stumpf, W.E.; Stachowiak, E.K.; Stachowiak, M.K. Vitamin D increases expression of the tyrosine hydroxylase gene in adrenal medullary cells. Mol. Brain Res. 1996, 36, 193–196. [Google Scholar] [CrossRef]
- Cass, W.A.; Smith, M.P.; Peters, L.E. Calcitriol protects against the dopamine- and serotonin-depleting effects of neurotoxic doses of methamphetamine. Proc. Ann. N. Y. Acad. Sci. 2006, 1074, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Byers, A.L.; Yaffe, K.; Covinsky, K.E.; Friedman, M.B.; Bruce, M.L. High occurrence of mood and anxiety disorders among older adults: The National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2010, 67, 489–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gum, A.M.; King-Kallimanis, B.; Kohn, R. Prevalence of mood, anxiety, and substance-abuse disorders for older Americans in the national comorbidity survey-replication. Am. J. Geriatr. Psychiatry 2009, 17, 769–781. [Google Scholar] [CrossRef] [PubMed]
- Bertone-Johnson, E.R. Vitamin D and the occurrence of depression: Causal association or circumstantial evidence? Nutr. Rev. 2009, 67, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Divo, M.J.; Martinez, C.H.; Mannino, D.M. Ageing and the epidemiology of multimorbidity. Eur. Respir. J. 2014, 44, 1055–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spedding, S. Vitamin D and depression: A systematic review and meta-analysis comparing studies with and without biological flaws. Nutrients 2014, 6, 1501–1518. [Google Scholar] [CrossRef] [PubMed]
- Uemura, K.; Doi, T.; Lee, S.; Shimada, H. Sarcopenia and Low Serum Albumin Level Synergistically Increase the Risk of Incident Disability in Older Adults. J. Am. Med. Dir. Assoc. 2019, 20, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Romero, L.; Garry, P.J. Serum albumin is associated with skeletal muscle in elderly men and women. Am. J. Clin. Nutr. 1996, 64, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Schalk, B.W.M.; Deeg, D.J.H.; Penninx, B.W.J.H.; Bouter, L.M.; Visser, M. Serum albumin and muscle strength: A longitudinal study in older men and women. J. Am. Geriatr. Soc. 2005, 53, 1331–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Peolsson, A.; Massy-Westropp, N.; Desrosiers, J.; Bear-Lehman, J. Reference values for adult grip strength measured with a Jamar dynamometer: A descriptive meta-analysis. Physiotherapy 2006, 92, 11–15. [Google Scholar] [CrossRef]
- Schubert, L.; DeLuca, H.F. Hypophosphatemia is responsible for skeletal muscle weakness of vitamin D deficiency. Arch. Biochem. Biophys. 2010, 500, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Lips, P.; Hosking, D.; Lippuner, K.; Norquist, J.M.; Wehren, L.; Maalouf, G.; Ragi-Eis, S.; Chandler, J. The prevalence of vitamin D inadequacy amongst women with osteoporosis: An international epidemiological investigation. J. Intern. Med. 2006, 260, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, X.; Gu, Y.; Liu, M.; Chi, V.T.Q.; Zhang, Q.; Liu, L.; Meng, G.; Yao, Z.; Wu, H.; et al. Vitamin D is related to handgrip strength in adult men aged 50 years and over: A population study from the TCLSIH cohort study. Clin. Endocrinol. 2019, 90, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Kitsu, T.; Kabasawa, K.; Ito, Y.; Kitamura, K.; Watanabe, Y.; Tanaka, J.; Nakamura, K.; Narita, I. Low serum 25-hydroxyvitamin D is associated with low grip strength in an older Japanese population. J. Bone Miner. Metab. 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, G.S.; Welsh, P.W.; Papacosta, O.P.; Lennon, L.; Whincup, P.H.; Sattar, N. Elevated parathyroid hormone, but not vitamin D deficiency, is associated with increased risk of heart failure in older men with and without cardiovascular disease. Circ. Heart Fail. 2014, 7, 732–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moe, S.M. Disorders Involving Calcium, Phosphorus, and Magnesium. Prim. Care Clin. Off. Pract. 2008, 35, 215–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bischoff-Ferrari, H.A.; Dietrich, T.; Orav, E.J.; Dawson-Hughes, B. Positive association between 25-hydroxy vitamin D levels and bone mineral density: A population-based study of younger and older adults. Am. J. Med. 2004, 116, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.S.; Rodríguez, M.; Felsenfeld, A.J. Serum calcium and bone: Effect of PTH, phosphate, vitamin D and uremia. Nefrologia 2014, 34, 658–669. [Google Scholar] [PubMed]


{kind=link}
| Characteristics | Men n = 129 | Women n = 144 | p-Value |
|---|---|---|---|
| Age, mean (SD) | 76.14 (7.32) | 75.40 (7.04) | 0.394 |
| BMI (SD) | 27.62 (3.77) | 27.80 (4.23) | 0.728 |
| Total drugs used, mean (SD) | 3.88 (2.83) | 4.11 (3.01) | 0.522 |
| Falls (SD) | 0.07 (0.26) | 0.26 (0.52) | <0.001 |
| Hospital admissions (SD) | 0.10 (0.29) | 0.09 (0.28) | 0.770 |
| CRG (% pluripathologic or chronic diseases) | 34.10 | 29.90 | 0.268 |
| EQ-5D (SD) | 0.83 (0.16) | 0.79 (0.16) | 0.058 |
| EQ-5D, problems with mobility (%) | 26.6 | 31.3 | 0.237 |
| EQ-5D, problems with self-care (%) | 3.1 | 9.7 | 0.024 |
| EQ-5D, problems with usual activities (%) | 7.8 | 14.6 | 0.058 |
| EQ-5D, problems with pain and discomfort (%) | 39.8 | 51.4 | 0.037 |
| EQ-5D, problems with depression or anxiety (%) | 25.0 | 39.6 | 0.009 |
| EQ-5D, any problem (%) | 61.7 | 70.8 | 0.072 |
| EQ-VAS, mean (SD) | 74.64 (14.03) | 68.63 (17.30) | 0.002 |
| VAS, mean (SD) | 2.51 (2.53) | 2.97 (2.51) | 0.131 |
| PASE (SD) | 329.68 (199.82) | 331.13 (196.59) | 0.646 |
| Hand grip, mean (SD) | 45.21 (26.23) | 30.47 (16.22) | <0.001 |
| MNA, mean (SD) | 27.06 (2.60) | 26.74 (2.97) | 0.350 |
| Vitamin D, mean (SD) | 19.83 (7.43) | 20.19 (3.00) | 0.796 |
| PTH (SD) | 64.32 (27.47) | 67.51 (29.77) | 0.369 |
| Ca2+ (SD) | 9.40 (0.30) | 9.52 (0.37) | 0.007 |
| Phosphorus (SD) | 3.06 (0.43) | 3.42 (0.49) | <0.001 |
| Creatinine (SD) | 1.04 (0.23) | 0.82 (0.19) | <0.001 |
| Albumin (SD) | 4.45 (0.25) | 4.39 (0.25) | 0.044 |
| Variables | Age | BMI | Number of Drugs | Number of Falls | Number of Hospitalizations | PASE | Hand Grip | EQ-5D | EQ-VAS | MNA | Vitamin D | Ca2+ | phosphorus | Alb | iPTH |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 1 | −0.047 | −0.006 | 0.016 | 0.016 | 0.003 | −0.255 | −0.159 | −0.137 | −0.138 | −0.143 | −0.025 | −0.092 | −0.301 | 0.249 |
| − | 0.444 | 0.920 | 0.792 | 0.792 | 0.967 | <0.001 | 0.009 | 0.023 | 0.023 | 0.019 | 0.678 | 0.132 | <0.001 | <0.001 | |
| BMI | 1 | 0.096 | 0.010 | −0.041 | −0.115 | 0.082 | −0.108 | −0.062 | 0.060 | 0.059 | 0.026 | −0.026 | 0.063 | −0.012 | |
| − | 0.115 | 0.871 | 0.507 | 0.050 | 0.178 | 0.076 | 0.310 | 0.327 | 0.338 | 0.672 | 0.677 | 0.302 | 0.845 | ||
| Number of Drugs | 1 | 0.020 | 0.032 | −0.182 | −0.116 | −0.327 | −0.356 | −0.019 | 0.070 | 0.058 | 0.102 | −0.027 | 0.020 | ||
| − | 0.747 | 0.606 | 0.003 | 0.056 | <0.001 | <0.001 | 0.753 | 0.253 | 0.347 | 0.094 | 0.661 | 0.748 | |||
| Number of Falls | 1 | 0.157 | −0.075 | −0.081 | −0.039 | −0.109 | −0.005 | 0.057 | 0.056 | 0.129 | −0.049 | 0.051 | |||
| − | 0.011 | 0.221 | 0.189 | 0.529 | 0.075 | 0.929 | 0.356 | 0.363 | 0.036 | 0.431 | 0.418 | ||||
| Number of Hospitalizations | 1 | 0.054 | 0.072 | −0.027 | −0.027 | −0.004 | 0.079 | 0.021 | 0.107 | −0.005 | −0.096 | ||||
| − | 0.378 | 0.242 | 0.666 | 0.657 | 0.945 | 0.205 | 0.733 | 0.086 | 0.936 | 0.123 | |||||
| PASE | 1 | −0.107 | 0.397 | 0.221 | −0.225 | −0.017 | −0.044 | −0.024 | 0.062 | 0.006 | |||||
| − | 0.078 | <0.001 | <0.001 | <0.001 | 0.777 | 0.470 | 0.697 | 0.310 | 0.925 | ||||||
| Hand Grip | 1 | 0.107 | 0.119 | 0.371 | 0.001 | −0.014 | −0.217 | 0.212 | 0.138 | ||||||
| − | 0.078 | 0.050 | <0.001 | 1 | 0.817 | <0.001 | <0.001 | 0.024 | |||||||
| EQ-5D | 1 | 0.309 | 0.026 | 0.002 | −0.072 | −0.045 | 0.018 | −0.007 | |||||||
| − | <0.001 | 0.672 | 0.975 | 0.237 | 0.467 | 0.769 | 0.910 | ||||||||
| EQ-VAS | 1 | 0.096 | 0.006 | 0.009 | −0.160 | 0.134 | −0.046 | ||||||||
| − | 0.115 | 0.927 | 0.887 | 0.008 | 0.028 | 0.459 | |||||||||
| MNA | 1 | 0.038 | −0.108 | −0.080 | 0.058 | 0.035 | |||||||||
| − | 0.537 | 0.077 | 0.191 | 0.347 | 0.567 | ||||||||||
| Vitamin D | 1 | 0.023 | 0.123 | 0.056 | −0.196 | ||||||||||
| − | 0.704 | 0.044 | 0.360 | 0.001 | |||||||||||
| Ca2+ | 1 | 0.052 | 0.471 | −0.035 | |||||||||||
| − | 0.393 | <0.001 | 0.575 | ||||||||||||
| phosphorus | 1 | −0.007 | −0.090 | ||||||||||||
| − | 0.910 | 0.144 | |||||||||||||
| Alb | 1 | −0.209 | |||||||||||||
| − | 0.001 | ||||||||||||||
| iPTH | 1 | ||||||||||||||
| − |
| Measurements | Vitamin D | Ca2+ | phosphorus | Alb | iPTH | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | |
| EQ-5D * | |||||||||||||||
| Mobility | 0.964 | 0.933–0.995 | 0.024 | 0.918 | 0.859–0.981 | 0.011 | 0.768 | 0.627–0.942 | 0.011 | 0.835 | 0.727–0.959 | 0.010 | 0.990 | 0.981–1.000 | 0.044 |
| Self-care | 0.943 | 0.875–1.016 | 0.125 | 0.805 | 0.739–1.013 | 0.072 | 0.647 | 0.398–1.051 | 0.078 | 0.734 | 0.526–1.025 | 0.069 | 0.985 | 0.964–1.006 | 0.158 |
| Usual activities | 0.924 | 0.866–0.987 | 0.019 | 0.845 | 0.743–0.962 | 0.011 | 0.598 | 0.401–0.893 | 0.012 | 0.698 | 0.530–0.917 | 0.010 | 0.979 | 0.960–0.997 | 0.025 |
| Pain and discomfort | 0.983 | 0.958–1.009 | 0.206 | 0.946 | 0.894–1.000 | 0.050 | 0.833 | 0.702–0.989 | 0.037 | 0.894 | 0.796–1.005 | 0.060 | 0.991 | 0.983–0.999 | 0.034 |
| Depression or anxiety | 0.959 | 0.930–0.990 | 0.009 | 0.912 | 0.856–0.972 | 0.005 | 0.739 | 0.606–0.901 | 0.003 | 0.825 | 0.722–0.943 | 0.005 | 0.988 | 0.979–0.998 | 0.014 |
| Any problem | 0.974 | 0.948–1.000 | 0.049 | 0.926 | 0.875–0.981 | 0.009 | 0.779 | 0.655–0.927 | 0.005 | 0.852 | 0.756–0.960 | 0.008 | 0.990 | 0.982–0.998 | 0.014 |
| EQ-VAS | 1.036 | 0.994–1.080 | 0.095 | 1.046 | 0.967–1.132 | 0.262 | 1.142 | 0.897–1.453 | 0.281 | 1.112 | 0.942–1.313 | 0.211 | 1.005 | 0.993–1.016 | 0.149 |
| Hand grip | 1.035 | 1.010–1.060 | 0.006 | 1.087 | 1.028–1.150 | 0.003 | 1.263 | 1.078–1.480 | 0.004 | 1.206 | 1.070–1.358 | 0.002 | 1.004 | 0.997–1.011 | 0.309 |
| MNA | 1.008 | 0.966–1.051 | 0.727 | 1.010 | 0.925–1.102 | 0.829 | 1.038 | 0.793–1.360 | 0.784 | 1.019 | 0.842–1.220 | 0.843 | 1.002 | 0.989–1.015 | 0.755 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verde, Z.; Giaquinta, A.; Moreno Sainz, C.; Díaz Ondina, M.; Fernández Araque, A. Bone Mineral Metabolism Status, Quality of Life, and Muscle Strength in Older People. Nutrients 2019, 11, 2748. https://doi.org/10.3390/nu11112748
Verde Z, Giaquinta A, Moreno Sainz C, Díaz Ondina M, Fernández Araque A. Bone Mineral Metabolism Status, Quality of Life, and Muscle Strength in Older People. Nutrients. 2019; 11(11):2748. https://doi.org/10.3390/nu11112748
Chicago/Turabian StyleVerde, Zoraida, Andrea Giaquinta, Carmelo Moreno Sainz, Marta Díaz Ondina, and Ana Fernández Araque. 2019. "Bone Mineral Metabolism Status, Quality of Life, and Muscle Strength in Older People" Nutrients 11, no. 11: 2748. https://doi.org/10.3390/nu11112748