Association between Hydration Status and Body Composition in Healthy Adolescents from Spain

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
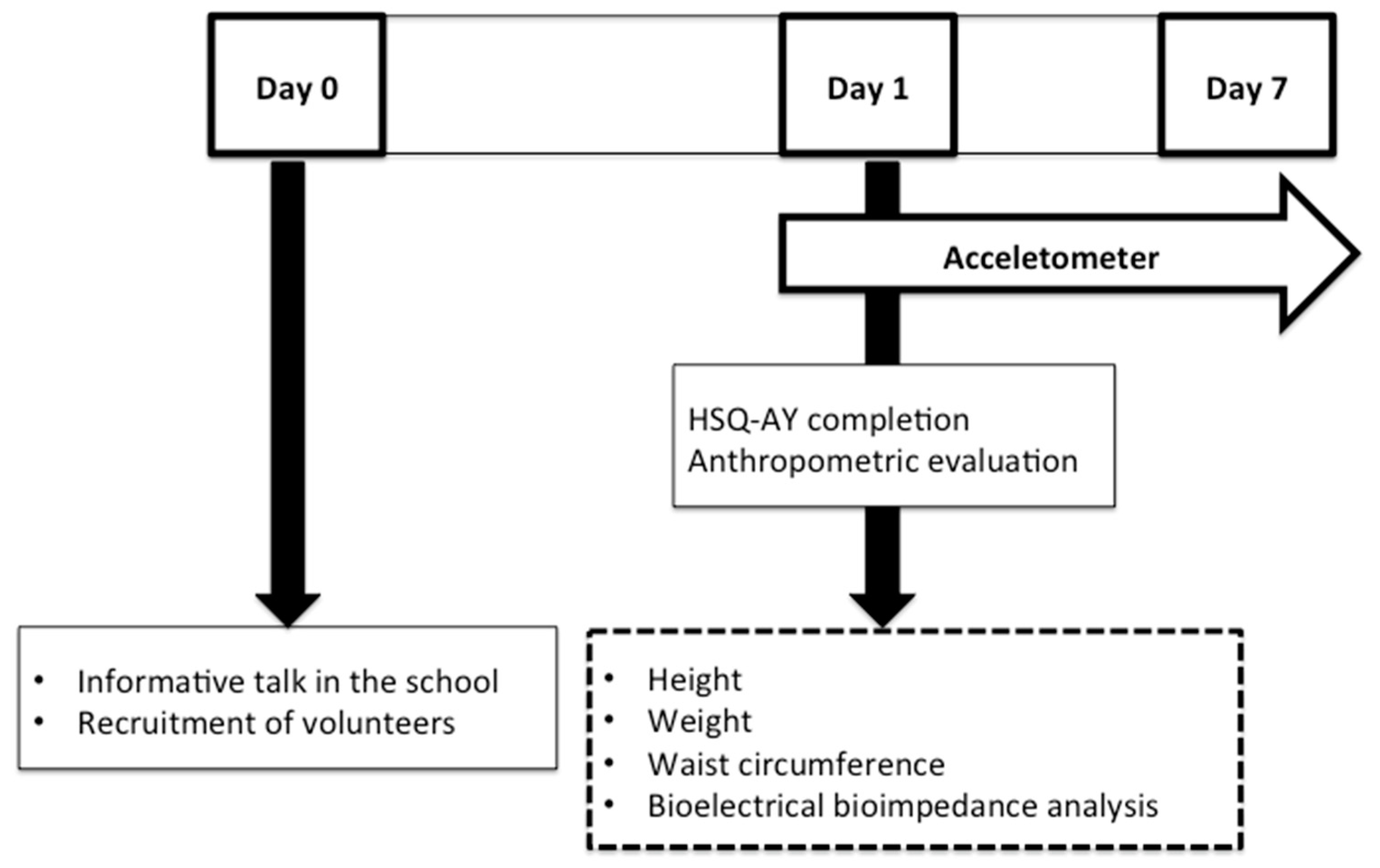
2.1. Study Protocol
2.2. Statistical Analysis
3. Results
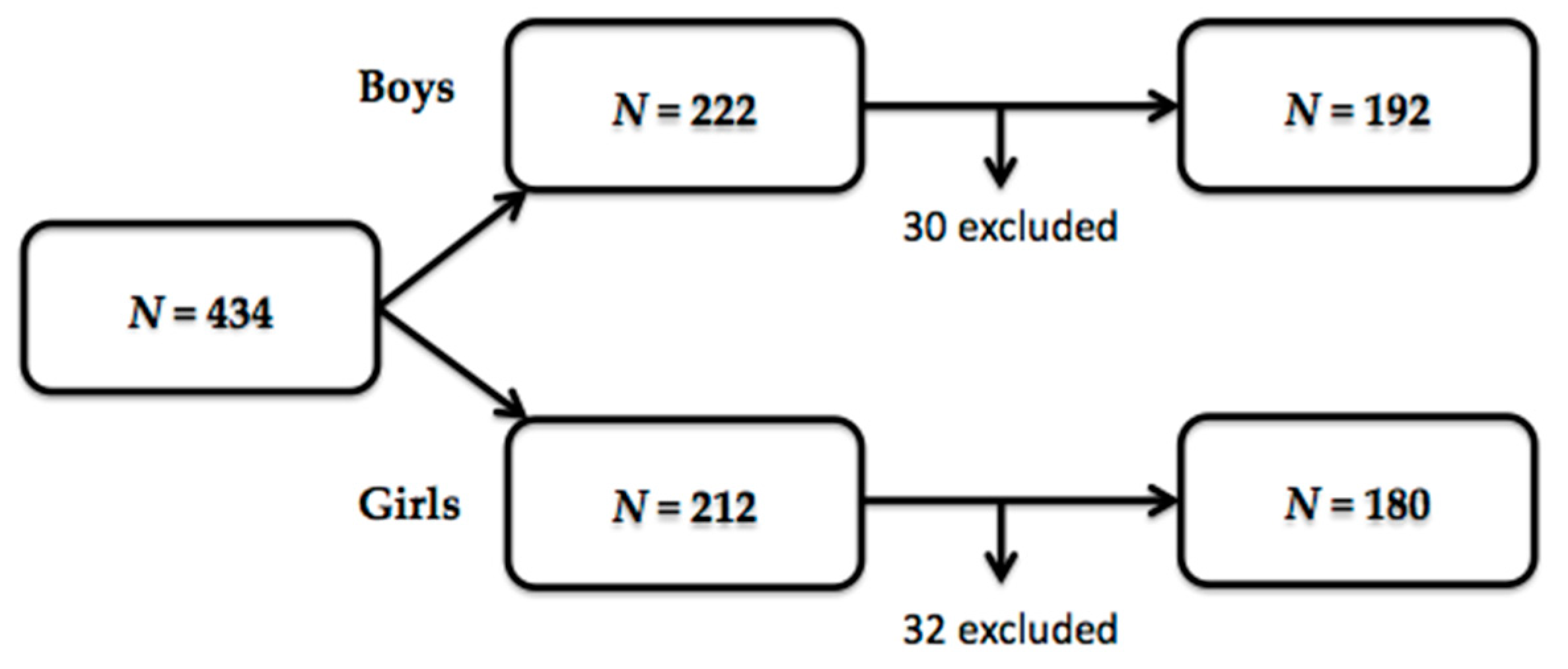
3.1. Sample Characteristics
3.2. Hydration Status and Body Composition
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization. Obesity and Overweight. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 22 July 2019).
- Ministerio de Sanidad, Consumo y Bienestar Social. Encuesta Nacional de Salud. España 2017. Available online: http://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2017.htm (accessed on 17 June 2019).
- Barton, M. Childhood obesity: A life-long health risk. Acta Pharm. Sin. 2012, 33, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Bridger, T. Childhood obesity and cardiovascular disease. Paediatr. Child Heal. 2009, 14, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Pulgaron, E.R.; Delamater, A.M. Obesity and type 2 diabetes in children: Epidemiology and treatment. Curr. Diabetes Rep. 2014, 14, 508. [Google Scholar] [CrossRef] [PubMed]
- Buttitta, M.; Iliescu, C.; Rousseau, A.; Guerrien, A. Quality of life in overweight and obese children and adolescents: A literature review. Qual. Life Res. 2014, 23, 1117–1139. [Google Scholar] [CrossRef] [PubMed]
- Lakerveld, J.; Mackenbach, J. The Upstream Determinants of Adult Obesity. Obes. Facts 2017, 10, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Marti, A.; Martinez-González, M.A.; Martinez, J.A. Interaction between genes and lifestyle factors on obesity. Proc. Nutr. Soc. 2008, 67, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ang, Y.N.; Wee, B.S.; Poh, B.K.; Ismail, M.N. Multifactorial influences of childhood obesity. Curr. Obes. Rep. 2013, 2, 10–22. [Google Scholar] [CrossRef]
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. Pharm. Econ. 2015, 33, 673–689. [Google Scholar] [CrossRef]
- Riebl, S.K.; Davy, B.M. The Hydration Equation: Update on Water Balance and Cognitive Performance. ACSM Health Fit. J. 2013, 17, 21–28. [Google Scholar]
- Stookey, J.D. Drinking Water and Weight Management. Nutr. Today 2010, 45, 7–12. [Google Scholar] [CrossRef]
- Muckelbauer, R.; Sarganas, G.; Grüneis, A.; Müller-Nordhorn, J. Association between water consumption and body weight outcomes: A systematic review. Am. J. Clin. Nutr. 2013, 98, 282–299. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.; Ravi, N.; Plegue, M.A.; Sonneville, K.R.; Davis, M.M. Inadequate Hydration, BMI, and Obesity Among US Adults: NHANES 2009–2012. Ann. Fam. Med. 2016, 14, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Thornton, S.N. Increased Hydration Can Be Associated with Weight Loss. Front. Nutr. 2016, 3, 1678. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Malik, V.S.; Hao, T.; Willett, W.C.; Mozaffarian, D.; Hu, F.B. Changes in water and beverage intake and long-term weight changes: Results from three prospective cohort studies. Int. J. Obes. 2013, 37, 1378–1385. [Google Scholar] [CrossRef] [PubMed]
- Daniels, M.C.; Popkin, B.M. Impact of water intake on energy intake and weight status: A systematic review. Nutr. Rev. 2010, 68, 505–521. [Google Scholar] [CrossRef] [PubMed]
- Muckelbauer, R.; Barbosa, C.L.; Mittag, T.; Burkhardt, K.; Mikelaishvili, N.; Müller-Nordhorn, J. Association between water consumption and body weight outcomes in children and adolescents: A systematic review. Obesity 2014, 22, 2462–2475. [Google Scholar]
- Milla-Tobarra, M.; García-Hermoso, A.; Lahoz-García, N.; Notario-Pacheco, B.; La Cruz, L.L.-D.; Pozuelo-Carrascosa, D.P.; García-Meseguer, M.J.; Martínez-Vizcaíno, V. The association between water intake, body composition and cardiometabolic factors among children—The Cuenca study. Nutr. Hosp. 2016, 33, 19–26. [Google Scholar] [CrossRef]
- Laja García, A.I.; Moráis-Moreno, C.; Samaniego-Vaesken, M.; Puga, A.M.; Partearroyo, T.; Varela-Moreiras, G. Influence of Water Intake and Balance on Body Composition in Healthy Young Adults from Spain. Nutrients 2019, 11, 1923. [Google Scholar] [CrossRef]
- Lappalainen, R.; Mennen, L.; Van Weert, L.; Mykkänen, H. Drinking water with a meal: A simple method of coping with feelings of hunger, satiety and desire to eat. Eur. J. Clin. Nutr. 1993, 47, 815–819. [Google Scholar]
- Van Walleghen, E.L.; Orr, J.S.; Gentile, C.L.; Davy, B.M. Pre-meal water consumption reduces meal energy intake in older but not younger subjects. Obesity 2007, 15, 93–99. [Google Scholar] [CrossRef]
- Dennis, E.A.; Dengo, A.L.; Comber, D.L.; Flack, K.D.; Savla, J.; Davy, K.P.; Davy, B.M. Water consumption increases weight loss during a hypocaloric diet intervention in middle-aged and older adults. Obesity 2010, 18, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Boschmann, M.; Steiniger, J.; Franke, G.; Birkenfeld, A.L.; Luft, F.C.; Jordan, J. Water Drinking Induces Thermogenesis through Osmosensitive Mechanisms. J. Clin. Endocrinol. Metab. 2007, 92, 3334–3337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubnov-Raz, G.; Constantini, N.W.; Yariv, H.; Nice, S.; Shapira, N. Influence of water drinking on resting energy expenditure in overweight children. Int. J. Obes. 2011, 35, 1295–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, J.M.W.; Ebbeling, C.B.; Robinson, L.; Feldman, H.A.; Ludwig, D.S. Effects of Advice to Drink 8 Cups of Water per Day in Adolescents with Overweight or Obesity: A Randomized Clinical Trial. JAMA Pediatrics 2017, 171, e170012. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Barclay, D.V.; Nielsen, S.J. Water and Food Consumption Patterns of U.S. Adults from 1999 to 2001. Obes. Res. 2005, 13, 2146–2152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stookey, J.D.; Constant, F.; Popkin, B.M.; Gardner, C.D. Drinking Water Is Associated with Weight Loss in Overweight Dieting Women Independent of Diet and Activity. Obesity 2008, 16, 2481–2488. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Graubard, B.I. Contributors of water intake in US children and adolescents: Associations with dietary and meal characteristics—National Health and Nutrition Examination Survey 2005–2006. Am. J. Clin. Nutr. 2010, 92, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Nissensohn, M.; Sánchez-Villegas, A.; Ortega, R.M.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Varela-Moreiras, G.; Serra-Majem, L. Beverage Consumption Habits and Association with Total Water and Energy Intakes in the Spanish Population: Findings of the ANIBES Study. Nutrients 2016, 8, 232. [Google Scholar] [CrossRef]
- European Food Safety Agency (EFSA). Scientific Opinion on Dietary Reference Values for water. EFSA J. 2010, 8, 1459. [Google Scholar]
- Jéquier, E.; Constant, F. Water as an Essential Nutrient: The Physiological Basis of Hydration. Eur. J. Clin. Nutr. 2010, 64, 115–123. [Google Scholar] [CrossRef]
- Popkin, B.M.; D’Anci, K.E.; Rosenberg, I.H. Water, hydration, and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Shirreffs, S.M. Markers of hydration status. Eur. J. Clin. Nutr. 2003, 57, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Perrier, E.; Rondeau, P.; Poupin, M.; Le Bellego, L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I.; Vergne, S.; Klein, A. Relation between urinary hydration biomarkers and total fluid intake in healthy adults. Eur. J. Clin. Nutr. 2013, 67, 939–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, L.E. Assessing Hydration Status: The Elusive Gold Standard. J. Am. Coll. Nutr. 2007, 26, 575–584. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Johnson, E.C.; Muñoz, C.X.; Swokla, B.; Le Bellego, L.; Jimenez, L.; Casa, D.J.; Maresh, C.M. Hydration Biomarkers and Dietary Fluid Consumption of Women. J. Acad. Nutr. Diet. 2012, 112, 1056–1061. [Google Scholar] [CrossRef]
- Perrier, E.; Vergne, S.; Klein, A.; Poupin, M.; Rondeau, P.; Le Bellego, L. Hydration biomarkers in free-living adults with different levels of habitual fluid consumption. Br. J. Nutr. 2013, 109, 1678–1687. [Google Scholar] [CrossRef]
- Laja, G.A.; Samaniego, V.M.; Partearroyo, T.; Varela, M.G. Validated questionnaire to assess the hydration status in a healthy adult Spanish population: A cross sectional study. Nutr. Hosp. 2019, 36, 875. [Google Scholar]
- Laja García, A.I.; Samaniego-Vaesken, M.D.L.; Partearroyo, T.; Varela-Moreiras, G. Adaptation and Validation of the Hydration Status Questionnaire in a Spanish Adolescent-Young Population: A Cross Sectional Study. Nutrients 2019, 11, 565. [Google Scholar] [CrossRef]
- Plasqui, G.; Bonomi, A.G.; Westerterp, K.R. Daily physical activity assessment with accelerometers: New insights and validation studies. Obes. Rev. 2013, 14, 451–462. [Google Scholar] [CrossRef]
- Marfell-Jones, M.J.; Stewart, A.D.; De Ridder, J.H. International Standards for Anthropometric Assessment; International Standards for Anthropometric Assessment (ISAK): Wellington, New Zealand, 2011. [Google Scholar]
- Khosla, T.; Lowe, C.R. Indices of obesity derived from body weight and height. J. Epidemiol. Community Heal. 1967, 21, 122–128. [Google Scholar] [CrossRef]
- Fernández, C.; Lorenzo, H.; Vrotsou, K.; Aresti, U.; Rica, I.; Sánchez, E. Estudio de crecimiento de Bilbao. Curvas y tablas de crecimiento (Estudio transversal). Instituto de Investigación Sobre Crecimiento y Desarrollo. Fundación Faustino Orbegozo Eizaguirre. 2011 Edition. Available online: https://www.fundacionorbegozo.com/wp-content/uploads/pdf/tPC.pdf (accessed on 5 July 2019).
- Kushner, R.F.; Schoeller, D.A. Estimation of total body water by bioelectrical impedance analysis. Am. J. Clin. Nutr. 1986, 44, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Matias, C.N.; Júdice, P.B.; Santos, D.A.; Magalhães, J.P.; Minderico, C.S.; Fields, D.A.; Sardinha, L.B.; Silva, A.M. Suitability of Bioelectrical Based Methods to Assess Water Compartments in Recreational and Elite Athletes. J. Am. Coll. Nutr. 2016, 35, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Segal, K.R.; Burastero, S.; Chun, A.; Coronel, P.; Pierson, R.N.; Wang, J. Estimation of extracellular and total body water by multiple-frequency bioelectrical-impedance measurement. Am. J. Clin. Nutr. 1991, 54, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Matias, C.N.; Santos, D.A.; Júdice, P.B.; Magalhães, J.P.; Minderico, C.S.; Fields, D.A.; Lukaski, H.C.; Sardinha, L.B.; Silva, A.M. Estimation of total body water and extracellular water with bioimpedance in athletes: A need for athlete-specific prediction models. Clin. Nutr. 2016, 35, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Yanovski, S.Z.; Hubbard, V.S.; Heymsfield, S.B.; Lukaski, H.C. Bioelectrical impedance analysis in body composition measurement: National institutes of health technology assessment conference statement. Am. J. Clin. Nutr. 1996, 64, 524–532. [Google Scholar]
- Bray, G.A.; Heisel, W.E.; Afshin, A.; Jensen, M.D.; Dietz, W.H.; Long, M.; Kushner, R.F.; Daniels, S.R.; Wadden, T.A.; Tsai, A.G.; et al. The Science of Obesity Management: An Endocrine Society Scientific Statement. Endocr. Rev. 2018, 39, 79–132. [Google Scholar] [CrossRef] [Green Version]
- Maughan, R.J. Impact of mild dehydration on wellness and on exercise performance. Eur. J. Clin. Nutr. 2003, 57, 19–23. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, N.; Du, S.; He, H.; Xu, Y.; Cai, H.; Guo, X.; Ma, G. The Effects of Hydration Status on Cognitive Performances among Young Adults in Hebei, China: A Randomized Controlled Trial (RCT). Int. J. Environ. Res. Public Heal. 2018, 15, 1477. [Google Scholar] [CrossRef]
- Stookey, J. Another look at: Fuel+ O2→CO2+ H2O. Developing a water-oriented perspective. Med. Hypotheses 1999, 52, 285–290. [Google Scholar]
- Keller, U.; Szinnai, G.; Bilz, S.; Berneis, K. Effects of changes in hydration on protein, glucose and lipid metabolism in man: Impact on health. Eur. J. Clin. Nutr. 2003, 57, 69–74. [Google Scholar] [CrossRef]
- Stahl, A.; Kroke, A.; Bolzenius, K.; Manz, F. Relation between hydration status in children and their dietary profile—Results from the DONALD study. Eur. J. Clin. Nutr. 2007, 61, 1386–1392. [Google Scholar] [CrossRef] [PubMed]
- Molina, T. Desarrollo puberal normal: Pubertad precoz. Pediatría Atención Primaria 2009, 11, 127–142. [Google Scholar] [Green Version]
- Nutrient Requirements in Relation to Body Size and Body Function. Nutr. Rev. 1952, 10, 42–45. [CrossRef]
- Puga, A.; Partearroyo, T.; Varela-Moreiras, G. Hydration status, drug interactions, and determinants in a Spanish elderly population: A pilot study. J. Physiol. Biochem. 2018, 74, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine of the National Academies. Water. Dietary Reference Intakes for Water, Sodium, Chloride, Potassium and Sulfate; National Academy Press: Washington, DC, USA, 2005. [Google Scholar]
- Institute of Medicine (US) Committee on Military Nutrition Research. Fluid Replacement and Heat Stress; National Academy Press: Washington, DC, USA, 1994. [Google Scholar]
- Ritz, P.; Vol, S.; Berrut, G.; Tack, I.; Arnaud, M.; Tichet, J. Influence of gender and body composition on hydration and body water spaces. Clin. Nutr. 2008, 27, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Ferry, M. Strategies for Ensuring Good Hydration in the Elderly. Nutr. Rev. 2005, 63, 22–29. [Google Scholar] [CrossRef]
- Iglesias, C.R.; Villarino, A.M.; Martínez, J.A.; Cabrerizo, L.; Gargallo, M.; Lorenzo, H. Importance of water in the hydration of the Spanish population: FESNAD 2010 document. Nutr. Hosp. 2011, 26, 27–36. [Google Scholar]
- Iglesia, I.; Guelinckx, I.; De Miguel-Etayo, P.M.; González-Gil, E.M.; Salas-Salvadó, J.; Kavouras, S.A.; Gandy, J.; Martinez, H.; Bardosono, S.; Abdollahi, M.; et al. Total fluid intake of children and adolescents: Cross-sectional surveys in 13 countries worldwide. Eur. J. Nutr. 2015, 54, 57–67. [Google Scholar] [CrossRef]
- Fenández-Alvira, J.M.; Iglesia, I.; Ferreira-Pêgo, C.; Babio, N.; Salas-Salvadó, J.; Moreno, L.A. Fluid intake in Spanish children and adolescents; a cross-sectional study. Nutr. Hosp. 2014, 29, 1163–1170. [Google Scholar]
- Ferreira-Pêgo, C.; Guelinckx, I.; Moreno, L.A.; Kavouras, S.A.; Gandy, J.; Martinez, H.; Bardosono, S.; Abdollahi, M.; Nasseri, E.; Jarosz, A.; et al. Total fluid intake and its determinants: Cross-sectional surveys among adults in 13 countries worldwide. Eur. J. Nutr. 2015, 54, 35–43. [Google Scholar] [CrossRef]
- Gandy, J.; Martinez, H.; Guelinckx, I.; Aznar, L.A.M.; Bardosono, S.; Salas-Salvadó, J.; Kavouras, S.A. Relevance of Assessment Methods for Fluid Intake. Ann. Nutr. Metab. 2016, 68, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food patterns of Spanish schoolchildren and adolescents: The enKid Study. Public Heal. Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Anthropometric Variables | Boys (n = 192) | Girls (n = 180) | p Values |
|---|---|---|---|
| Age | 13.0 (12.0−14.0) | 13.0 (12.0–14.0) | 0.427 |
| Weight (Kg) | 49.0 (43.4−59.0) | 51.0 (45.4−54.8) | 0.507 |
| Height (cm) | 160.2 (154.2−166.3) | 160.1 (155.1−164.5) | 0.536 |
| BMI (Kg/m2) | 18.8 (17.5−21.3) | 19.4 (17.8−21.2) | 0.201 |
| WC (cm) | 66.0 (63.0− 70.9) | 63.5 (60.1−66.6) | 0.000 |
| TBW (%) | 56.2 (52.8−60.0) | 53.2 (50.2−56.2) | 0.000 |
| TBW (L) | 28.1 (24.5−32.3) | 27.1 (24.7−29.2) | 0.005 |
| FBM (%) | 24.6 (20.0−29.4) | 29.6 (26.2−33.9) | 0.000 |
| FBM (Kg) | 12.0 (9.3−16.1) | 15.3 (12.0−18.6) | 0.000 |
| LBM (Kg) | 37.5 (32.5−42.9.) | 35.5 (32.7−38.6) | 0.001 |
| DLBM (Kg) | 9.5 (8.1−10.9) | 8.6 (7.8−9.4) | 0.000 |
| Boys (n = 192) | Girls (n = 180) | p Values | |
|---|---|---|---|
| Drinking water (mL/day) | 1650.0 | 1400.0 | |
| (1000.0–2000.0) | (1000.0–2000.0) | 0.089 | |
| Water from beverages (mL/day) | 2339.1 | 2086.6 | |
| (1779.0–2890.2) | (1575.7–2769.7) | 0.067 | |
| Water from food (mL/day) | 383.5 | 413.5 | |
| (257.8–544.4) | (265.7–596.4) | 0.227 | |
| Water intake (mL/day) | 2648.8 | 2509.5 | |
| (2217.4–3352.7) | (1923.9–3315.9) | 0.153 | |
| Total water loss (mL/day) | 3734.7 | 3172.7 | |
| (3183.6–4327.4) | (2746.1–3785.3) | 0.000 | |
| Water balance (mL/day) | −979.3 | −661.0 | |
| (−1748.8 to −308.1) | (−1329.2 to 160.1) | 0.002 | |
| Drinking water /weight (mL/Kg) | 32.2 | 28.4 | |
| (21.7–42.6) | (19.1–41.2) | 0.122 | |
| Water from beverages/weight (mL/ Kg) | 46.3 | 41.8 | |
| (35.1–61.1) | (30.9–56.0) | 0.051 | |
| Water from food/weigh (mL/Kg) | 7.6 | 8.1 | |
| (4.7–11.4) | (5.4–12.6) | 0.369 | |
| Water intake/weight (mL/Kg) | 53.9 | 50.7 | |
| (42.6–70.4) | (38.6–66.1) | 0.135 |
| Drinking Water (mL/day) | Water from Beverages (mL/day) | Water from Food (mL/day) | Water Intake (mL/day) | Water Balance (mL/day) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| r | p Values | r | p Values | r | p Values | r | p Values | r | p Values | |
| Weight (Kg) | 0.051 | 0.485 | 0.026 | 0.718 | −0.141 | 0.050 | 0.021 | 0.777 | −0.060 | 0.406 |
| BMI (Kg/m2) | −0.048 | 0.512 | −0.093 | 0.197 | −0.187 | 0.009 | −0.099 | 0.171 | −0.206 | 0.004 |
| BMI p (Kg/m2) | −0.085 | 0.242 | −0.091 | 0.209 | −0.120 | 0.098 | −0.076 | 0.294 | −0.225 | 0.002 |
| WC (cm) | −0.088 | 0.225 | −0.085 | 0.241 | −0.091 | 0.211 | −0.073 | 0.317 | −0.183 | 0.011 |
| TBW (%) | 0.115 | 0.113 | 0.187 | 0.009 | 0.118 | 0.104 | 0.174 | 0.016 | 0.158 | 0.029 |
| TBW (L) | 0.131 | 0.070 | 0.139 | 0.055 | −0.117 | 0.107 | 0.119 | 0.099 | 0.035 | 0.632 |
| FBM (%) | −0.124 | 0.088 | −0.195 | 0.007 | −0.116 | 0.109 | −0.182 | 0.011 | −0.167 | 0.021 |
| FBM (Kg) | −0.043 | 0.555 | −0.100 | 0.167 | −0.147 | 0.042 | −0.094 | 0.195 | −0.104 | 0.152 |
| LBM (Kg) | 0.111 | 0.125 | 0.120 | 0.098 | −0.122 | 0.092 | 0.101 | 0.162 | 0.038 | 0.601 |
| DLBM (Kg) | 0.129 | 0.075 | 0.136 | 0.060 | −0.110 | 0.127 | 0.118 | 0.104 | 0.037 | 0.607 |
| Drinking Water (mL/day) | Water from Beverages (mL/day) | Water from Food (mL/day) | Water Intake (mL/day) | Water Balance (mL/day) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| r | p Values | r | p Values | r | p Values | r | p Values | r | p Values | |
| Weight (Kg) | 0.039 | 0.606 | 0.013 | 0.868 | 0.094 | 0.212 | 0.025 | 0741 | 0.023 | 0.762 |
| BMI (Kg/m2) | 0.020 | 0792 | −0.045 | 0.553 | −0.041 | 0.584 | −0.059 | 0.431 | −0.025 | 0.737 |
| BMI p (Kg/m2) | −0.081 | 0282 | −0.173 | 0.020 | −0.094 | 0.211 | −0.180 | 0.015 | −0.180 | 0.016 |
| WC (cm) | 0.034 | 0.653 | 0.006 | 0.934 | 0.009 | 0.904 | −0.003 | 0.968 | −0.119 | 0.112 |
| TBW (%) | −0.061 | 0.413 | −0.023 | 0.762 | 0.051 | 0.498 | 0.013 | 0.860 | −0.049 | 0.517 |
| TBW (L) | 0.007 | 0.927 | −0.003 | 0.973 | 0.139 | 0.062 | 0.029 | 0.702 | −0.016 | 0.836 |
| FBM (%) | 0.077 | 0.304 | 0.020 | 0.786 | −0.032 | 0.672 | −0.007 | 0.925 | 0.045 | 0.546 |
| FBM (Kg) | 0.079 | 0.292 | 0.028 | 0.707 | 0.012 | 0.877 | 0.010 | 0.890 | 0.047 | 0.533 |
| LBM (Kg) | −0.013 | 0.862 | −0.020 | 0.792 | 0.127 | 0.088 | 0.010 | 0.898 | −0.018 | 0.809 |
| DLBM (Kg) | −0.034 | 0.648 | −0.038 | 0.611 | 0.110 | 0.140 | −0.012 | 0.875 | 0.010 | 0.893 |
| Drinking Water/Weight (mL/day/Kg) | Water from Beverages/Weight (mL/day/Kg) | Water from Food/Weight (mL/day/Kg) | Water Intake/Weight (mL/day/Kg) | |||||
|---|---|---|---|---|---|---|---|---|
| r | p Values | r | p Values | r | p Values | r | p Values | |
| BMI (Kg/m2) | −0.388 | 0.000 | −0.497 | 0.000 | −0.440 | 0.000 | −0.548 | 0.000 |
| BMI p (Kg/m2) | −0.320 | 0.000 | −0.368 | 0.000 | −0.299 | 0.000 | −0.395 | 0.000 |
| WC (cm) | −0.390 | 0.000 | −0.447 | 0.000 | −0.328 | 0.000 | −0.476 | 0.000 |
| TBW (%) | 0.250 | 0.000 | 0.332 | 0.000 | 0.213 | 0.003 | 0.342 | 0.000 |
| TBW (L) | −0.239 | 0.001 | −0.319 | 0.000 | −0.395 | 0.000 | −0.379 | 0.000 |
| FBM (%) | −0.243 | 0.001 | −0.321 | 0.000 | −0.200 | 0.006 | −0.329 | 0.000 |
| FBM (Kg) | −0.340 | 0.000 | −0.454 | 0.000 | −0.367 | 0.000 | −0.488 | 0.000 |
| LBM (Kg) | −0.255 | 0.000 | −0.332 | 0.000 | −0.394 | 0.000 | −0.389 | 0.000 |
| DLBM (Kg) | −0.235 | 0.001 | −0.314 | 0.000 | −0.386 | 0.000 | −0.372 | 0.000 |
| Drinking Water/Weight (mL/day/Kg) | Water from Beverages/Weight (mL/day/Kg) | Water from Food/Weight (mL/day/Kg) | Water Intake/Weight (mL/day/Kg) | |||||
|---|---|---|---|---|---|---|---|---|
| r | p Values | r | p Values | r | p Values | r | p Values | |
| BMI (Kg/m2) | −0.254 | 0.000 | −0.348 | 0.000 | −0.273 | 0.000 | −0.376 | 0.000 |
| BMI p (Kg/m2) | −0.281 | 0.000 | −0.386 | 0.000 | −0.271 | 0.000 | −0.400 | 0.000 |
| WC (cm) | −0.178 | 0.017 | −0.233 | 0.002 | −0.181 | 0.015 | −0.253 | 0.001 |
| TBW (%) | 0.125 | 0.096 | 0.197 | 0.008 | 0.214 | 0.004 | 0.237 | 0.001 |
| TBW (L) | −0.247 | 0.001 | −0.294 | 0.000 | −0.099 | 0.184 | −0.274 | 0.000 |
| FBM (%) | −0.117 | 0.116 | −0.207 | 0.005 | −0.198 | 0.008 | −0.242 | 0.001 |
| FBM (Kg) | −0.181 | 0.015 | −0.270 | 0.000 | −0.216 | 0.004 | −0.300 | 0.000 |
| LBM (Kg) | −0.275 | 0.000 | −0.318 | 0.000 | −0.118 | 0.116 | −0.299 | 0.000 |
| DLBM (Kg) | −0.296 | 0.000 | −0.336 | 0.000 | −0.135 | 0.071 | −0.319 | 0.000 |
| Underweight (N = 10) | Normal Weight (N = 149) | Overweight/Obesity (N = 33) | |
|---|---|---|---|
| Drinking water (mL/day) | 1575.0 | 1650.0 | 1600.0 |
| (1187.5–2392.5) | (1000.0–2050.0) | (1000.0–1890.0) | |
| Water from beverages (mL/day) | 2390.7 | 2063.1 | |
| (1717.3–2892.8) | (1869.8–2924.7) | (1455.7–2566.5) | |
| Water from food (mL/day) | 531.0 | 382.7 | 321.0 |
| (399.2–707.2) | (253.2–525.2) | (230.6–518.6) | |
| Water intake (mL/day) | 2315.5 | 2690.6 | 2584.8 |
| (2103.6–3473.9) | (2273.8–3455.9) | (2040.0–3112.5) | |
| Water balance (mL/day) | −931.1ab | −946.5a | −1522.1b |
| (−1219.7 to −308.1) | (−1584.9 to −274.4) | (−2085.1 to −734.2) | |
| Drinking water/ body weight (mL/Kg) | 39.3c | 35.4c | 23.2d |
| (30.5–70.1) | (22.8–44.2) | (15.8–28.4) | |
| Water from beverages/body weight (mL/Kg) | 50.6e | 48.6e | 31.1f |
| (39.4–84.4) | (38.2–62.2) | (23.1–40.8) | |
| Water from food/body weight (mL/Kg) | 14.1g | 8.1h | 5.0i |
| (9.8–19.7) | (5.1–11.4) | (3.5–9.2) | |
| Water intake/body weight (mL/Kg) | 64.7j | 55.7j | 40.2k |
| (52.1–101.3) | (45.9–75.5) | (30.0–50.7) |
| Underweight (N = 11) | Normal Weight (N = 151) | Overweight/Obesity (N = 18) | |
|---|---|---|---|
| Drinking water (mL/day) | 1800.0 | 1400.0 | 1550.0 |
| (1320.0–2000.0) | (1000.0–2000.0) | (950.0–1985.0) | |
| Water from beverages (mL/day) | 2651.0 | 2065.6 | 1898.6 |
| (1979.5–3373.0) | (1571.0–2771.3) | (1265.9–2531.8) | |
| Water from food (mL/day) | 488.5 | 400.8 | 400.4 |
| (387.1–729.1) | (262.4–601.0) | (203.5–494.1) | |
| Water intake (mL/day) | 3219.7 | 2490.8 | 2551.4 |
| (2498.7–3913.1) | (1912.2–3393.4) | (1807.0–2921.8) | |
| Water balance (mL/day) | −540.3 | −664.1 | −933.3 |
| (−578.8 to −984.5) | (−1350.6–196.7) | (−1583.8 to −457.8) | |
| Drinking water/ body weight (mL/Kg) | 46.5a | 28.1b | 23.1b |
| (37.9–58.6) | (19.0–41.1) | (16.6–29.9) | |
| Water from beverages/body weight (mL/Kg) | 67.4c | 42.1d | 29.7e |
| (53.9–86.5) | (31.8–55.4) | (19.5–39.2) | |
| Water from food/body weight (mL/Kg) | 14.8f | 8.1fg | 5.8g |
| (10.6–15.9) | (5.4–11.7) | (3.1–8.1) | |
| Water intake/body weight (mL/Kg) | 82.4h | 52.1i | 38.6j |
| (67.5–104.4) | (39.4–65.7) | (26.5–46.5) |
| Percentiles | Distribution of Water Balance (mL) | |||
|---|---|---|---|---|
| < p 25 (N = 58) | p 25–p50 (N = 50) | p 50–p75 (N = 47) | > p 75 (N = 37) | |
| Weight (Kg) | 50.1 | 47.3 | 51.0 | 46.6 |
| (44.4–61.8) | (42.4–56.7) | (45.6–60.1) | (42.0–55.8) | |
| BMI (Kg/m2) | 19.9a | 18.6ab | 19.2a | 18.0b |
| (17.9–22.6) | (17.6–21.0) | (18.0–21.4) | (16.6–19.6) | |
| FBM (%) | 27.5c | 22.9cd | 25.0cd | 21.5d |
| (21.9–32.5) | (19.3–28.6) | (21.5–29.4) | (18.8–26.8) | |
| FBM (Kg) | 13.2 | 10.6 | 12.9 | 10.4 |
| (10.0–18.7) | (8.1–14.5) | (10.5–16.1) | (8.7–15.5) | |
| WC (Cm) | 68.0e | 64.8ef | 67.4e | 63.8f |
| (63.9–74.0) | (62.4–69.0) | (63.9–72.2) | (61.0–67.0) | |
| LBM (Kg) | 37.3 | 36.1 | 39.7 | 36.7 |
| (32.3–44.4) | (32.4–40.9) | (33.2–42.8) | (30.8–45.4) | |
| DLBM (kg) | 9.3 | 9.3 | 9.9 | 9.3 |
| (7.9–11.2) | (8.0–10.4) | (8.4–10.8) | (7.8–11.6) | |
| TBW (%) | 54.2 | 58.1 | 55.9 | 58.2 |
| (50.6–58.7) | (53.6–60.7) | (53.1–58.7) | (54.8–60.9) | |
| Percentiles | Distribution of Water Intake/Body Weight (mL/Kg) | |||
|---|---|---|---|---|
| < p 25 | p 25–p50 | p 50–p75 | > p 75 | |
| (N = 42) | (N = 51) | (N = 46) | (N = 53) | |
| Weight (Kg) | 59.8a | 52.3a | 46.8b | 43.8b |
| (49.0–66.8) | (46.6–60.1) | (43.0–51.5) | (37.5–48.4) | |
| BMI (Kg/m2) | 21.4c | 20.1cd | 18.5de | 17.4e |
| (19.5–24.3) | (18.3–21.6) | (17.7–19.9) | (16.6–18.5) | |
| FBM (%) | 28.6f | 24.3fg | 24.4g | 21.9g |
| (24.7–32.9) | (21.4–29.4) | (19.6–29.0) | (19.6–27.7) | |
| FBM (Kg) | 16.9h | 13.3hi | 11.8ij | 9.4j |
| (11.5–21.6) | (10.0–15.8) | (8.8–14.7) | (8.1–11.1) | |
| WC (Cm) | 72.5k | 68.0l | 64.6lm | 63.8m |
| (65.0–80.1) | (64.0–71.8) | (61.5–68.3) | (60.8–66.0) | |
| LBM (Kg) | 40.9n | 41.3n | 35.7o | 33.5o |
| (36.9–46.6) | (34.6–45.1) | (31.5–39.4) | (28.1–38.6) | |
| DLBM (kg) | 10.3p | 10.4p | 8.9q | 8.4q |
| (9.3–11.8) | (8.6–11.5) | (7.9–10.0) | (6.9–9.8) | |
| TBW (%) | 53.2r | 56.3rs | 56.4s | 58.9s |
| (50.1–56.4) | (53.3–58.7) | (53.6–60.3) | (54.5–60.6) | |
| Percentiles | Distribution of Water Intake/Body Weight (mL/Kg) | |||
|---|---|---|---|---|
| < p 25 | p 25–p50 | p 50–p75 | > p 75 | |
| (N = 51) | (N = 43) | (N = 47) | (N = 39) | |
| Weight (Kg) | 53.2a | 50.9a | 52.0a | 45.4b |
| (48.1–58.0) | (45.5–54.1) | (47.4–54.8) | (40.2–49.7) | |
| BMI (Kg/m2) | 20.9c | 19.6cd | 19.2de | 17.7e |
| (19.2–23.1) | (17.8–21.4) | (18.0–21.0) | (16.9–19.9) | |
| FBM (%) | 31.4f | 31.3f | 29.6fg | 27.5g |
| (28.0–35.5) | (27.2–35.6) | (25.0–33.9) | (24.9–29.6) | |
| FBM (Kg) | 16.5h | 15.8h | 15.1h | 12.0i |
| (13.3–21.0) | (13.6–20.5) | (12.0–18.6) | (9.9–16.0) | |
| WC (Cm) | 65.9j | 63.5jk | 63.2jk | 60.5k |
| (61.5–68.0) | (60.8–66.5) | (62.0–66.6) | (57.8–64.0) | |
| LBM (Kg) | 37.1l | 35.1lm | 36.7l | 32.9m |
| (35.1–39.7) | (32.7–38.4) | (33.2–38.9) | (30.0–36.3) | |
| DLBM (kg) | 9.0n | 8.6no | 8.7n | 8.0o |
| (8.3–9.7) | (7.8–9.4) | (7.9–9.3) | (7.2–8.5) | |
| TBW (%) | 52.4p | 52.5p | 53.4pq | 55.5q |
| (49.3–54.5) | (49.0–55.1) | (50.2–56.6) | (53.1–57.5) | |
| Variable | B | SEM | β | 95%CI | p Value |
|---|---|---|---|---|---|
| Waist circumference (cm) | −0.244 | 0.225 | −0.070 | −0.688 to 0.199 | 0.279 |
| Fat body mass (%) | −1.042 | 0.195 | −0.284 | −1.426 to −0.658 | 0.000 |
| Dry lean body mass (Kg) | −3.841 | 0.850 | 0.274 | −5.513 to −2.170 | 0.000 |
| Constant | 136.735 | 10.946 | 115.209 to 158.260 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laja García, A.I.; Moráis-Moreno, C.; Samaniego-Vaesken, M.d.L.; Puga, A.M.; Varela-Moreiras, G.; Partearroyo, T. Association between Hydration Status and Body Composition in Healthy Adolescents from Spain. Nutrients 2019, 11, 2692. https://doi.org/10.3390/nu11112692
Laja García AI, Moráis-Moreno C, Samaniego-Vaesken MdL, Puga AM, Varela-Moreiras G, Partearroyo T. Association between Hydration Status and Body Composition in Healthy Adolescents from Spain. Nutrients. 2019; 11(11):2692. https://doi.org/10.3390/nu11112692
Chicago/Turabian StyleLaja García, Ana Isabel, Carmen Moráis-Moreno, Mª de Lourdes Samaniego-Vaesken, Ana M. Puga, Gregorio Varela-Moreiras, and Teresa Partearroyo. 2019. "Association between Hydration Status and Body Composition in Healthy Adolescents from Spain" Nutrients 11, no. 11: 2692. https://doi.org/10.3390/nu11112692