Prevalence of Anemia in Children from Latin America and the Caribbean and Effectiveness of Nutritional Interventions: Systematic Review and Meta–Analysis



Abstract
:1. Introduction
2. Materials and Methods
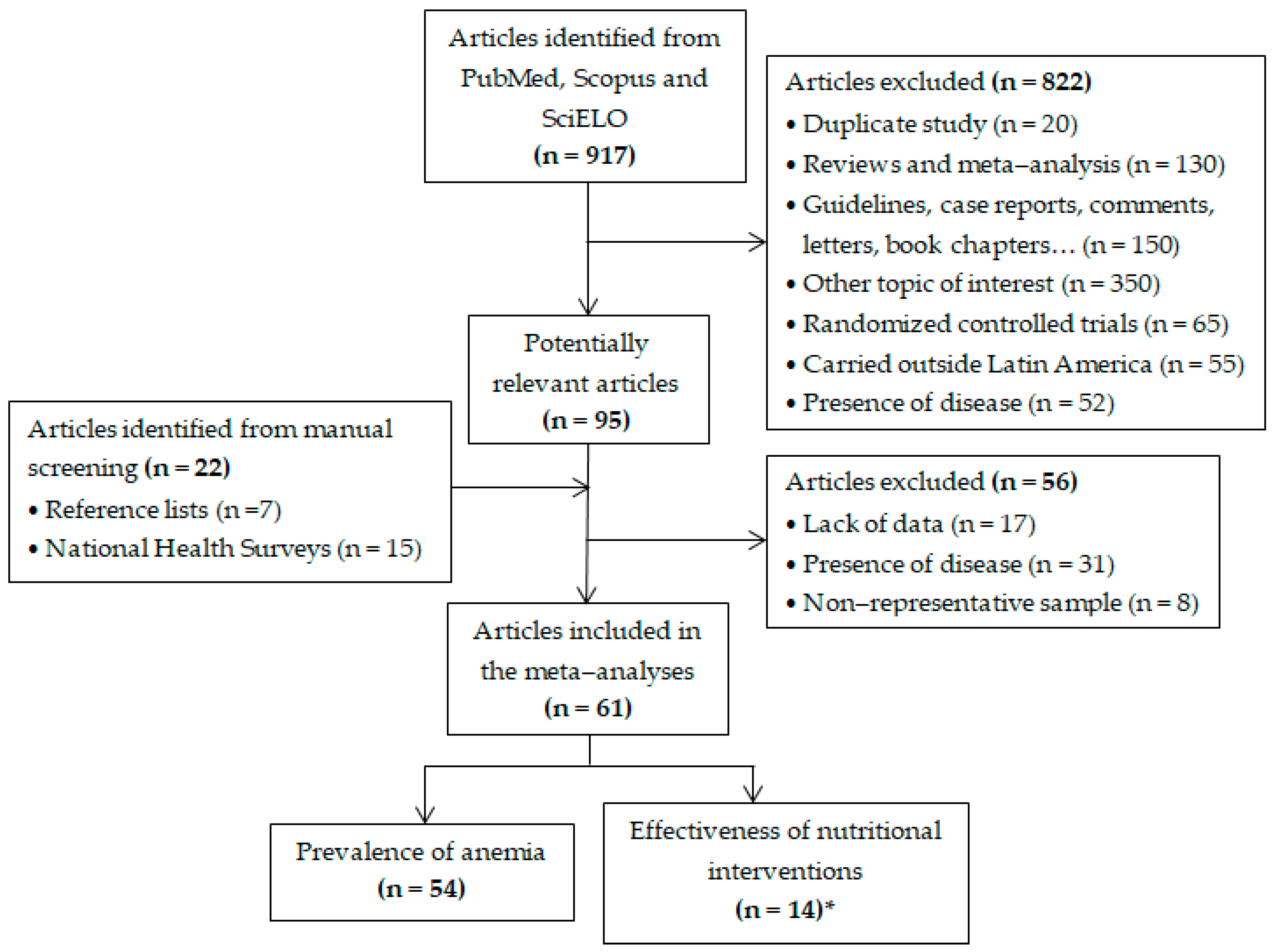
2.1. Literature Search
2.2. Data Extraction and Quality Assessment
2.3. Data Analysis
3. Results
3.1. Study Characteristics
3.2. Prevalence of Anemia in Children
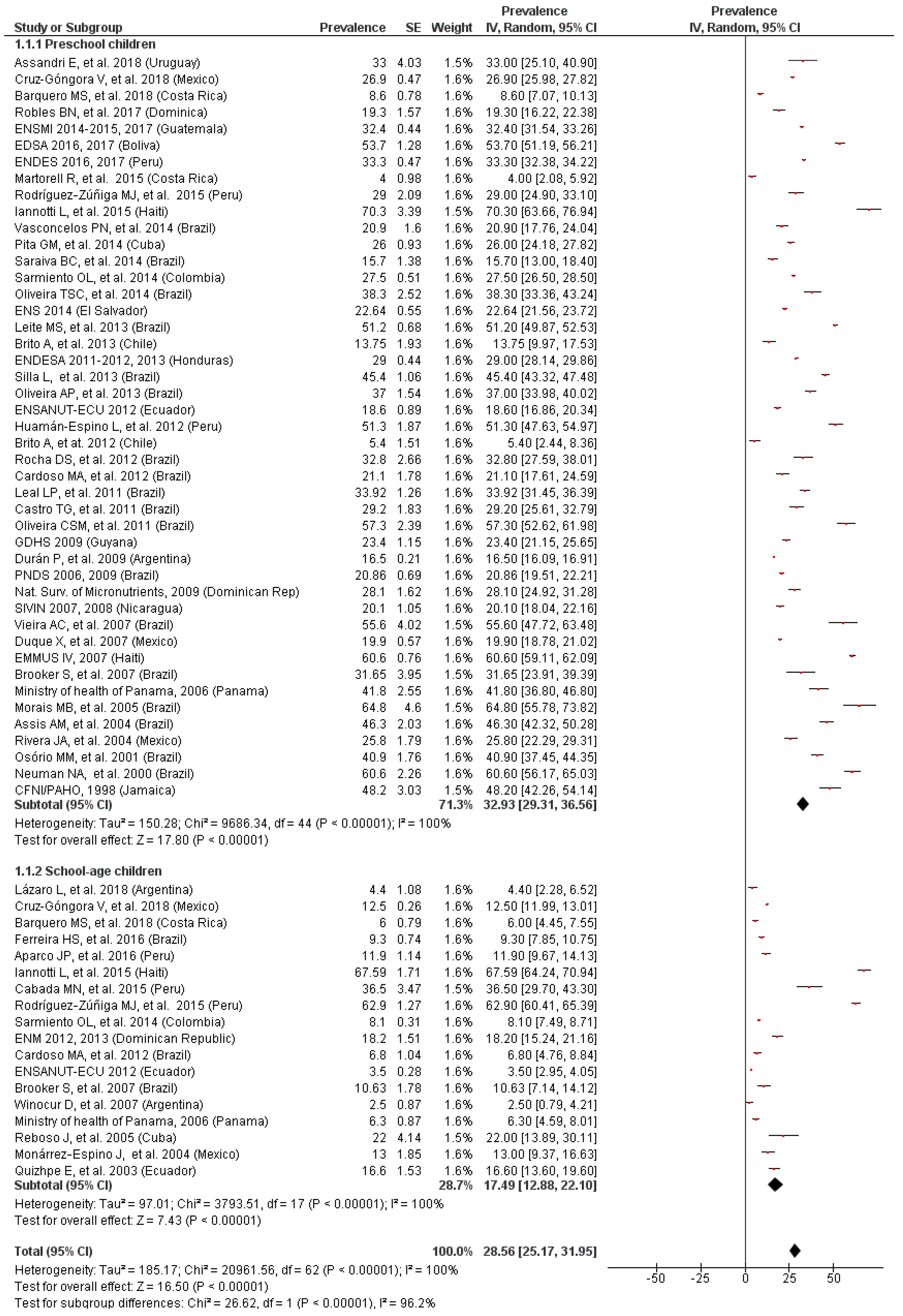
3.3. Prevalence of Anemia by Age
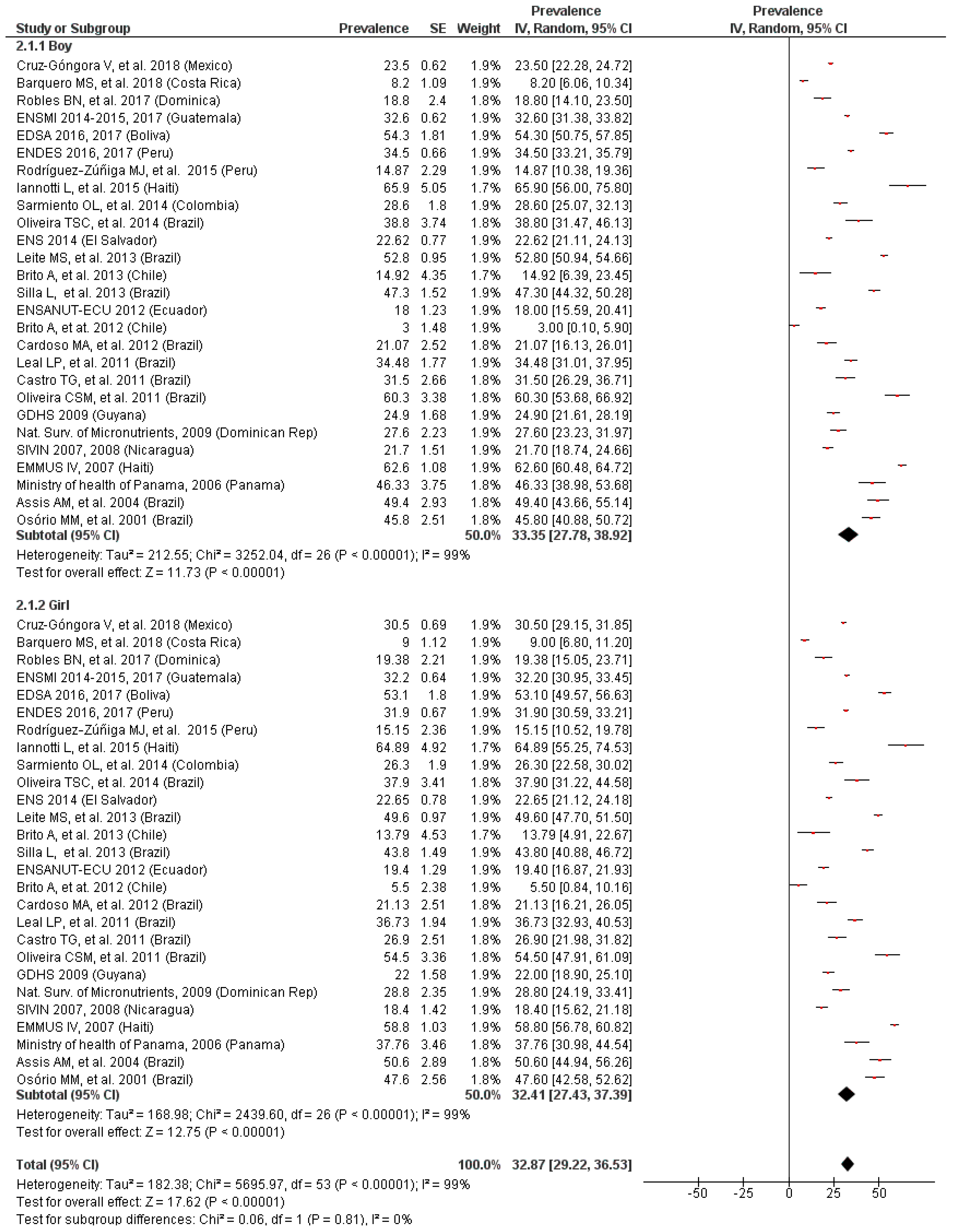
3.4. Prevalence of Anemia by Gender
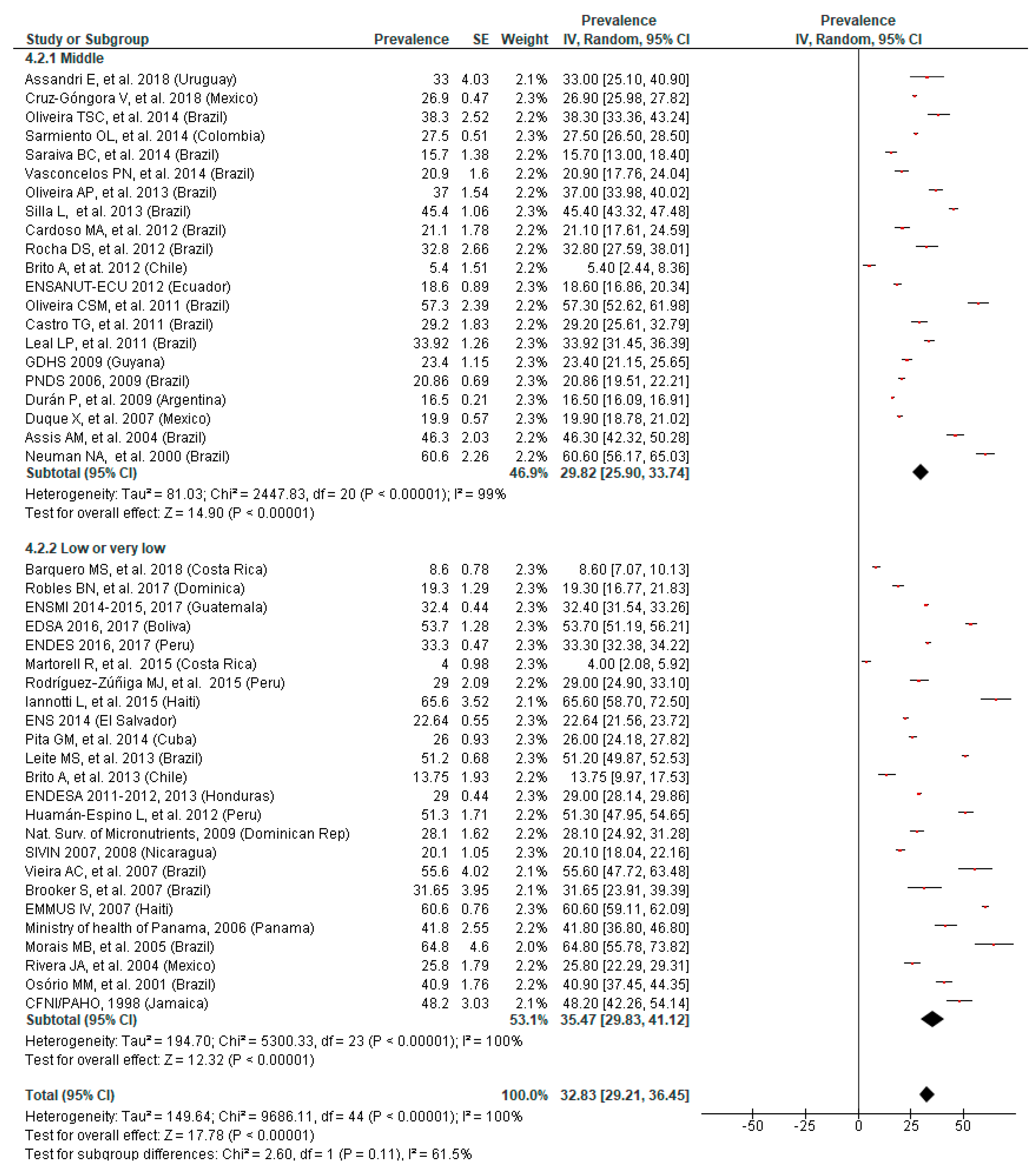
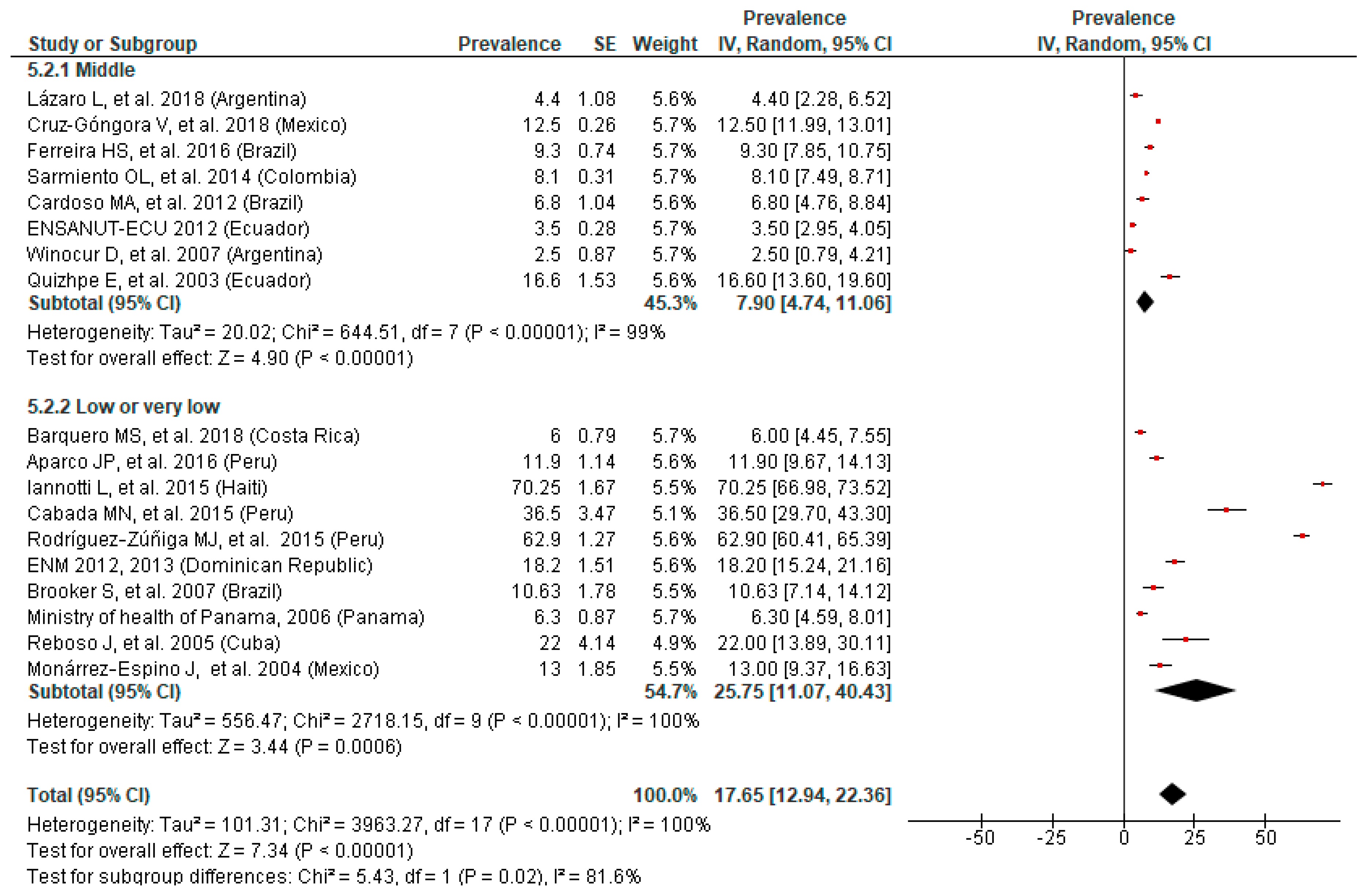
3.5. Prevalence of Anemia by SES
3.6. Prevalence of Anemia by Area of Residence
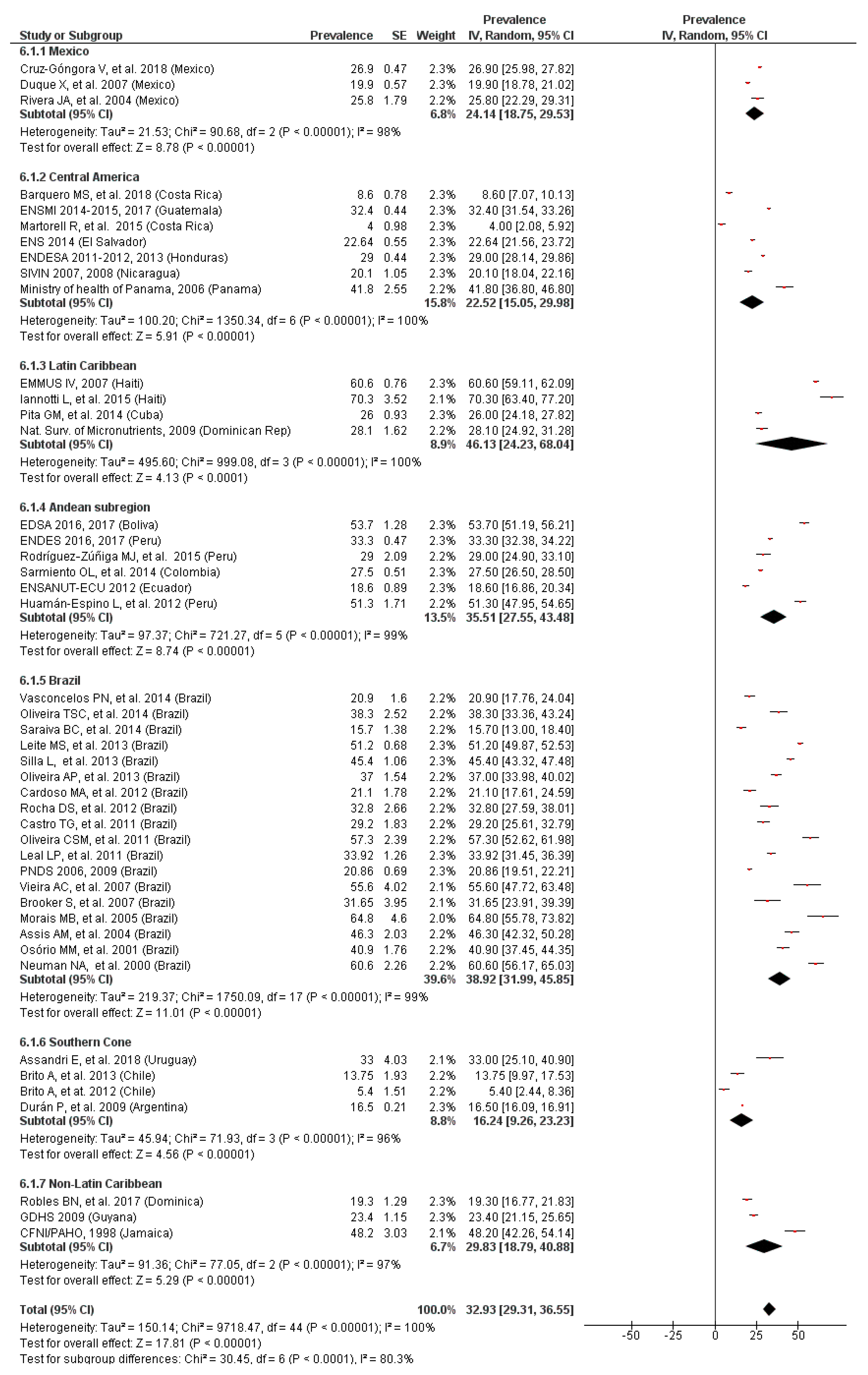
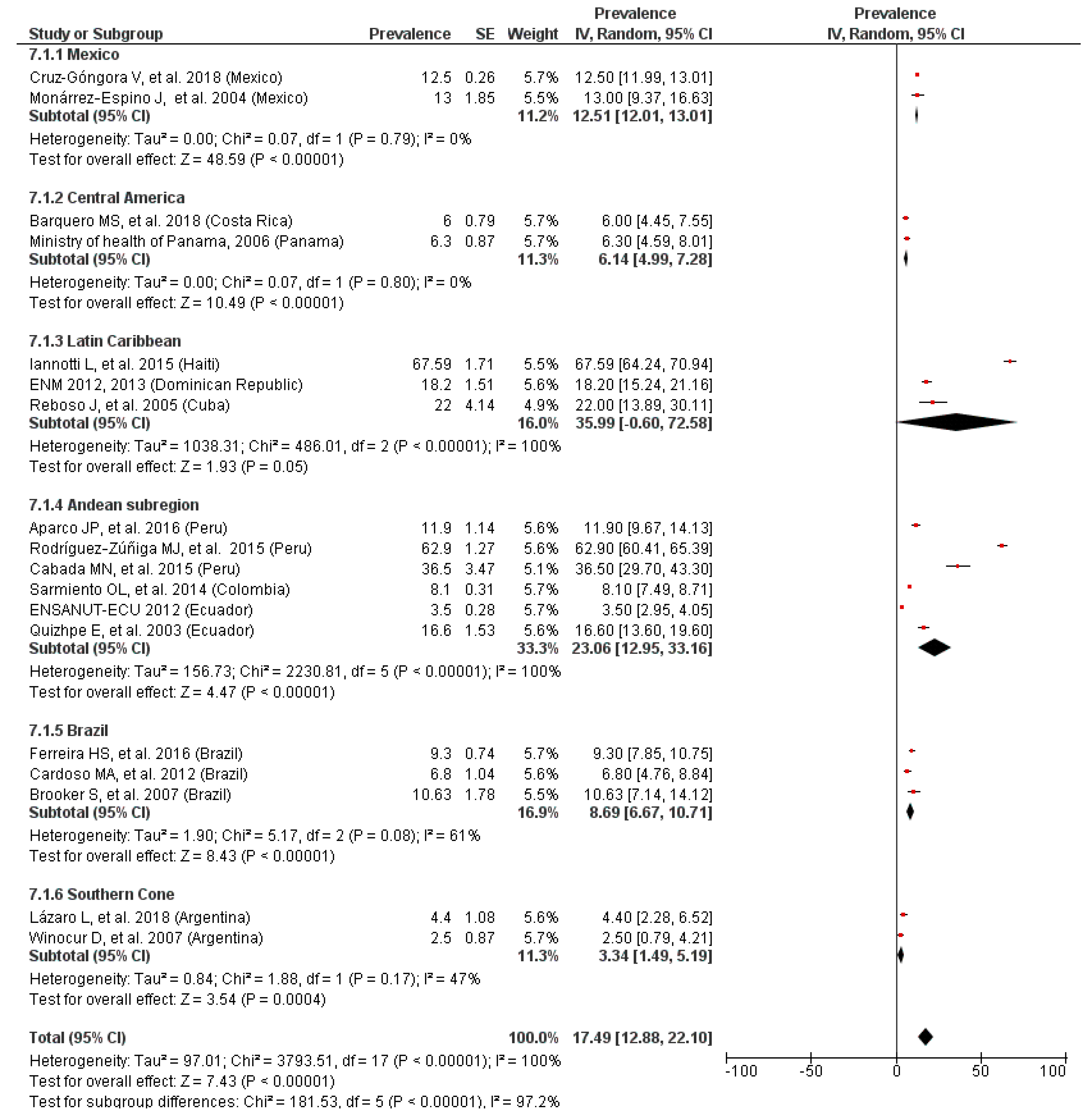
3.7. Prevalence of Anemia by LAC Region
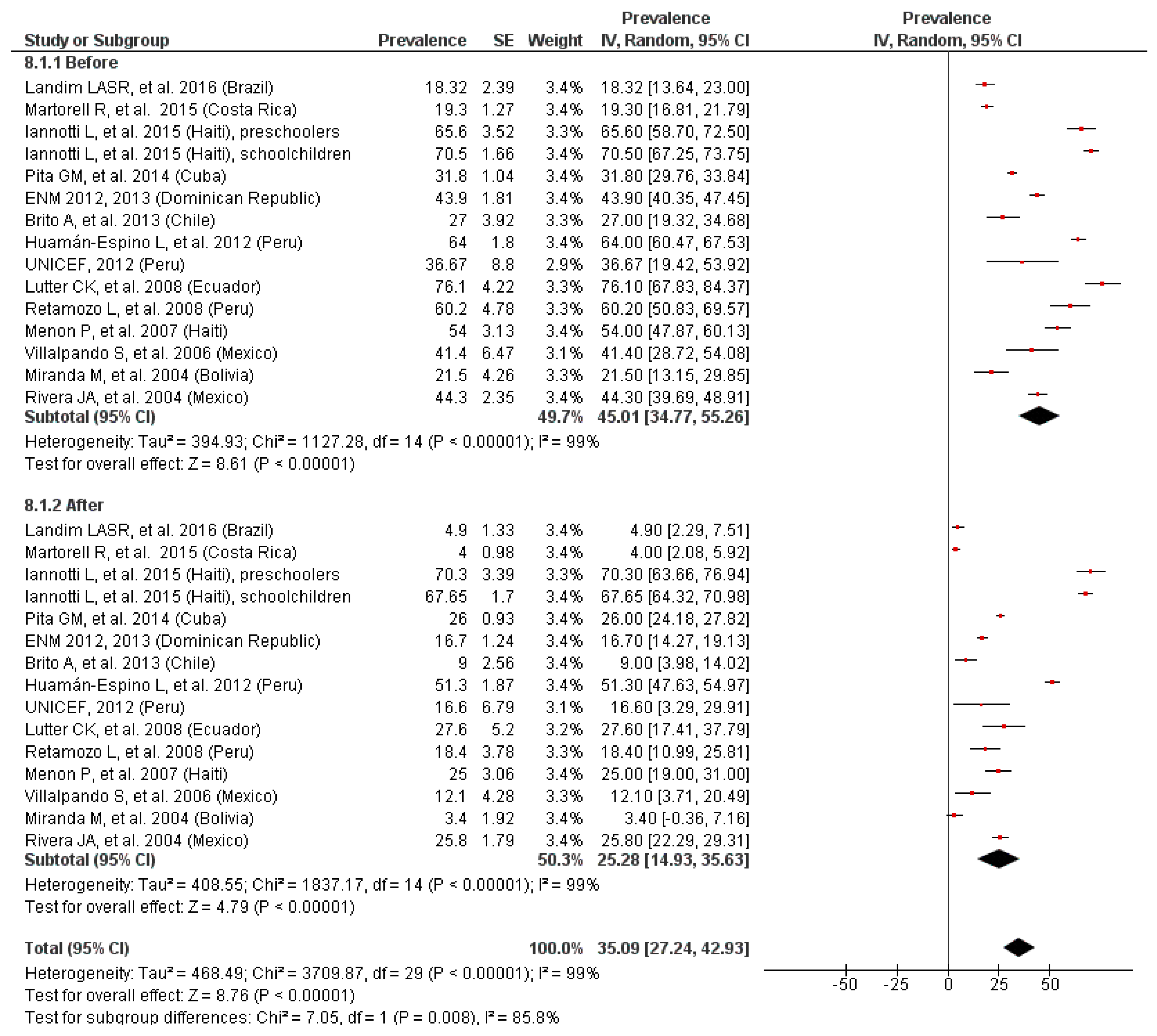
3.8. Effectiveness of Iron Supplementation Programs
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- De Benoist, B.; McLean, E.; Egli, I.; Cogswell, M. Worldwide Prevalence of Anaemia 1993–2005: WHO Global Database on Anaemia; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- World Health Organization. Nutritional Anaemias: Tools for Effective Prevention; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Pan American Health Organization. Anemia in Latin America and the Caribbean, 2009; PAHO: Washington, DC, USA, 2010. [Google Scholar]
- Best, C.; Neufingerl, N.; van Geel, L.; van den Briel, T.; Osendarp, S. The nutritional status of school-aged children: Why should we care? Food Nutr. Bull. 2014, 31, 400–417. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.; de Sanctis, V.; Kalra, S. Anemia and growth. Indian J. Endocrinol. Metab. 2014, 18, 1–5. [Google Scholar] [CrossRef]
- Lozoff, B.; Corapci, F.; Burden, M.J.; Kaciroti, N.; Angulo-Barroso, R.; Sazawal, S.; Black, M. Preschool-aged children with iron deficiency anemia show altered affect and behavior. J. Nutr. 2007, 137, 683–689. [Google Scholar] [CrossRef]
- Balarajan, Y.; Ramakrishnan, U.; Özaltin, E.; Shankar, A.H.; Subramanian, S.V. Anaemia in low-income and middle-income countries. Lancet 2011, 378, 2123–2135. [Google Scholar] [CrossRef]
- Zavaleta, N.; Astete-Robilliard, L. Effect of anemia on child development: Long-term consequences. Rev. Peru. Med. Exp. Salud Publica 2017, 34, 716–722. [Google Scholar] [CrossRef]
- Galicia, L.; Grajeda, R.; de Romaña, D.L. Nutrition situation in Latin America and the Caribbean: Current scenario, past trends, and data gaps. Pan Am. J. Public Health 2016, 40, 104–113. [Google Scholar]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 November 2018).
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Noel Robles, B.; James, A.B.; Macri, R.; Xiong, M.; Jafri, S.; Vitale, A.; Beata, V.; Faheem, S.; McIntyre-Francis, R. Prevalence of anemia in preschool aged children living in Dominica. J. Pediatr. Care 2017, 3, 12. [Google Scholar] [CrossRef]
- UNICEF; PAHO; Ministry of Health of Panama. Situation of Deficiency of Iron and Anemia; UNICEF; PAHO; Ministry of Health of Panama: Panama, Republic of Panama, 2006.
- National Institute of Statistics and Informatics. Demographic and Family Health Survey (ENDES 2016); National Institute of Statistics and Informatics: Lima, Peru, 2016.
- Freire, W.B.; Ramírez-Luzuriaga, M.J.; Belmont, P.; Mendieta, M.J.; Silva-Jaramillo, M.K.; Romero, N.; Sáenz, K.; Piñeiros, P.; Gómez, L.F.; Monge, R. Vol. I: National Survey of Health and Nutrition (ENSANUT-ECU 2012); Ministry of Public Health, National Institute of Statistics and Census: Quito, Ecuador, 2014.
- Cayemites, M.; Placide, M.F.; Mariko, S.; Barrère, B.; Sévère, B.; Alexandre, C. Enquête Mortalité, Morbidité et Utilisation des Services (EMMUS-IV) 2005–2006; Ministère de la Santé Publique et de la Population, Institut Haïtien de l’Enfance et Macro International Inc.: Calverton, MD, USA, 2007. [Google Scholar]
- Ministry of Health; Brazilian Center for Analysis and Planning. National Survey on Demography and Health of Women and Children (PNDS 2006): Dimensions of Reproduction and Child Health; Ministry of Health: Brasilia, Brazil, 2009.
- Ministry of Health (Honduras), National Institute of Statistics and ICF International. National Survey of Demography and Health (ENDESA 2011–2012); Ministry of Health: Tegucigalpa, Honduras, 2012.
- Ministry of Health [Guyana], Bureau of Statistics and ICF Macro. Guyana Demographic and Health Survey 2009; Ministry of Health: Georgetown, Guyana, 2010.
- WHO Global Database on Anaemia: Vitamin and Mineral Nutrition Information System [Nicaragua]. Available online: https://www.who.int/vmnis/anaemia/data/database/countries/nic_ida.pdf?ua=1 (accessed on 26 February 2010).
- Ministry of Public Health and Social Assistance; Statistics National Institute; ICF International. VI National Survey of Maternal and Child Health (ENSMI 2014–2015); Ministry of Public Health and Social Assistance: Guatemala City, Guatemala, 2017.
- Salvadoran Demographic Association; ICC; CDC. National Survey of Family Health (FESAL 2008); Salvadoran Demographic Association: San Salvador, Republic of El Salvador, 2009. [Google Scholar]
- Ministry of Public Health and Social Assistance. National Micronutrient Survey; Dominican Republic: Santo Domingo, Dominican Republic, 2014.
- Ministry of Education [Dominican Republic]; INABIE; UNICEF; PMA; PNUD. National Micronutrient Survey in the School Population of the Dominican Republic (ENM 2012); Dominican Republic: Santo Domingo, Dominican Republic, 2013.
- Ministry of Health (Bolivia); Statistics National Institute. Demography and Health Survey (EDSA 2016); Ministry of Health: La Paz, Bolivia, 2017.
- Sarmiento, O.L.; Parra, D.C.; González, S.A.; González-Casanova, I.; Forero, A.Y.; Garcia, J. The dual burden of malnutrition in Colombia. Am. J. Clin. Nutr. 2014, 100, 1628S–1635S. [Google Scholar] [CrossRef] [PubMed]
- Leite, M.S.; Cardoso, A.M.; Coimbra, C.E., Jr.; Welch, J.R.; Gugelmin, S.A.; Lira, P.C.; Horta, B.L.; Santos, R.V.; Escobar, A.L. Prevalence of anemia and associated factors among indigenous children in Brazil: Results from the First National Survey of Indigenous People’s Health and Nutrition. Nutr. J. 2013, 12, 69. [Google Scholar] [CrossRef] [PubMed]
- Durán, P.; Mangialavori, G.; Biglieri, A.; Kogan, L.; Abeyá Gilardon, E. Nutrition status in Argentinean children 6 to 72 months old. Results from the National Nutrition and Health Survey (ENNyS). Arch. Argent Pediatr. 2009, 107, 397–404. [Google Scholar]
- De la Cruz-Góngora, V.; Villalpando, S.; Shamah-Levy, T. Prevalence of anemia and consumption of iron-rich food groups in Mexican children and adolescents: Ensanut MC 2016. Salud Publica Mex 2018, 60, 291–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duque, X.; Flores-Hernández, S.; Flores-Huerta, S.; Méndez-Ramírez, I.; Muñoz, S.; Turnbull, B.; Martínez-Andrade, G.; Ramos, R.I.; González-Unzaga, M.; Mendoza, M.E.; et al. Prevalence of anemia and deficiency of iron, folic acid, and zinc in children younger than 2 years of age who use the health services provided by the Mexican Social Security Institute. BMC Public Health 2007, 7, 345. [Google Scholar] [CrossRef] [PubMed]
- Winocur, D.; Ceriani Cernadas, J.M.; Imach, E.; Otasso, J.C.; Morales, P.; Gards, A. Prevalence of iron deficiency anemia in a group of pre-school and school children, living in conditions of poverty. Medicina (B. Aires) 2004, 64, 481–486. [Google Scholar] [PubMed]
- Lázaro Cuesta, L.; Rearte, A.; Rodríguez, S.; Niglia, M.; Scipioni, H.; Rodríguez, D.; Salinas, R.; Sosa, C.; Rasse, S. Anthropometric and biochemical assessment of nutritional status and dietary intake in school children aged 6-14 years, Province of Buenos Aires, Argentina. Arch. Argent. Pediatr. 2018, 116, e34–e46. [Google Scholar] [PubMed]
- Leal, L.P.; Batista Filho, M.; Cabral de Lira, P.I.; Natal Figueiroa, J.; Osório, M.M. Prevalence of anemia and associated factors in children aged 6–59 months in Pernambuco, Northeastern Brazil. Rev. Saude Publica 2011, 45, 457–466. [Google Scholar] [CrossRef]
- Cardoso, M.A.; Scopel, K.K.; Muniz, P.T.; Villamor, E.; Ferreira, M.U. Underlying factors associated with anemia in amazonian children: A population-based, cross-sectional study. PLoS ONE 2012, 7, e36341. [Google Scholar] [CrossRef]
- Rocha, D.S.; Capanema, F.D.; Pereira Netto, M.; Franceschini, S.C.; Lamounier, J.A. Prevalence and risk factors of anemia in children attending daycare centers in Belo Horizonte–MG. Rev. Bras. Epidemiol. 2012, 15, 675–684. [Google Scholar] [CrossRef]
- De Oliveira, A.P.; Pascoal, M.N.; dos Santos, L.C.; Pereira, S.C.; Justino, L.E.; Petarli, G.B.; Kitoko, P.M. The prevalence of anemia and its association with socio-demographic and anthropometric aspects in children living in Vitória, State of Espírito Santo, Brazil. Ciênc. Saude Colet. 2013, 18, 3273–3280. [Google Scholar]
- Silla, L.M.; Zelmanowicz, A.; Mito, I.; Michalowski, M.; Hellwing, T.; Shilling, M.A.; Friedrisch, J.R.; Bittar, C.M.; Albrecht, C.A.; Scapinello, E.; et al. High prevalence of anemia in children and adult women in an urban population in southern Brazil. PLoS ONE 2013, 8, e68805. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, T.S.C.; da Silva, M.C.; Santos, J.N.; Rocha, D.S.; Alves, C.R.L.; Capanema, F.D.; Lamounier, J.A. Anemia entre pré-escolares-um problema de saúde pública em Belo Horizonte, Brasil. Ciênc. Saude Colet. 2014, 19, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, B.C.; Soares, M.C.; Santos, L.C.; Pereira, S.C.; Horta, P.M. Iron deficiency and anemia are associated with low retinol levels in children aged 1 to 5 years. J. Pediatr. 2014, 90, 593–599. [Google Scholar] [CrossRef] [Green Version]
- Vasconcelos, P.N.; Cavalcanti, D.S.; Leal, L.P.; Osório, M.M.; Batista Filho, M. Time trends in anemia and associated factors in two age groups (6–23 and 24–59 months) in Pernambuco State, Brazil, 1997–2006. Cad. Saude Publica 2014, 30, 1777–1787. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Ferreira, H.; de Assunção Bezerra, M.K.; Lopes De Assunção, M.; Egito de Menezes, R.C. Prevalence of and factors associated with anemia in school children from Maceió, northeastern Brazil. BMC Public Health 2016, 16, 380. [Google Scholar] [CrossRef] [Green Version]
- Neuman, N.A.; Tanaka, O.Y.; Szarfarc, S.C.; Guimarães, P.R.; Victora, C.G. Prevalence and risk factors for in Southern Brazil. Rev. Saude Publica 2000, 34, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Osório, M.M.; Lira, P.I.; Batista-Filho, M.; Ashworth, A. Prevalence of anemia in children 6–59 months old in the state of Pernambuco, Brazil. Rev. Panam. Salud Pública 2001, 10, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Assis, A.M.; Barreto, M.L.; Gomes, G.S.; Prado, M.S.; dos Santos, N.S.; Santos, L.M.; Sampaio, L.R.; Ribeiro, R.C.; de Oliveira, L.P.; de Oliveira, V.A. Childhood anemia prevalence and associated factors in Salvador, Bahia, Brazil. Cad. Saude Publica 2004, 20, 1633–1641. [Google Scholar] [CrossRef] [PubMed]
- Morais, M.B.; Alves, G.M.; Fagundes-Neto, U. Nutritional status of Terena indian children from Mato Grosso do Sul, Brazil: Follow up of weight and height and current prevalence of anemia. J. Pediatr. 2005, 81, 383–389. [Google Scholar] [CrossRef]
- Brooker, S.; Jardim-Botelho, A.; Quinnell, R.J.; Geiger, S.M.; Caldas, I.R.; Fleming, F.; Hotez, P.J.; Correa-Oliveira, R.; Rodrigues, L.C.; Bethony, J.M. Age-related changes in hookworm infection, anaemia and iron deficiency in an area of high Necator americanus hookworm transmission in south-eastern Brazil. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 146–154. [Google Scholar] [CrossRef]
- Vieira, A.C.; Diniz, A.S.; Cabral, P.C.; Oliveira, R.S.; Lóla, M.M.F.; Silva, S.M.; Kolsteren, P. Nutritional assessment of iron status and anemia in children under 5 years old at public daycare centers. J. Pediatr. 2007, 83, 370–376. [Google Scholar] [CrossRef]
- Oliveira, C.S.M.; Cardoso, M.A.; Araújo, T.S.; Muniz, P.T. Anemia em crianças de 6 a 59 meses e fatores associados no Município de Jordão, Estado do Acre, Brasil. Cad. Saude Publica 2011, 27, 1008–1020. [Google Scholar] [CrossRef] [Green Version]
- De Castro, T.G.; Silva-Nunes, M.; Conde, W.L.; Muniz, P.T.; Cardoso, M.A. Anemia and iron defi ciency among schoolchildren in the Western Brazilian Amazon: Prevalence and associated factors. Cad. Saude Publica 2011, 27, 131–142. [Google Scholar] [PubMed]
- Brito, A.; Hertrampf, E.; Olivares, M. Low prevalence of anemia in children aged 19 to 72 months in Chile. Food Nutr. Bull. 2012, 33, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Brito, A.; Olivares, M.; Pizarro, T.; Rodríguez, L.; Hertrampf, E. Chilean Complementary Feeding Program reduces anemia and improves iron status in children aged 11 to 18 months. Food Nutr. Bull. 2013, 34, 378–385. [Google Scholar] [CrossRef]
- Martorell, R.; Ascencio, M.; Tacsan, L.; Alfaro, T.; Young, M.F.; Addo, O.Y.; Dary, O.; Flores-Ayala, R. Effectiveness evaluation of the food fortification program of Costa Rica: Impact on anemia prevalence and hemoglobin concentrations in women and children. Am. J. Clin. Nutr. 2015, 101, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Barquero, M.S.; Mora, A.M.; Santamaría-Ulloa, C.; Marín Arias, L.; Granados Zamora, M.; Reyes Lizano, L. Nutritional Deficiencies and Anemia in Preschool Children of Costa Rica in 2014–2016. 2018. Available online: https://revistas.ucr.ac.cr/index.php/psm/article/view/32447 (accessed on 10 December 2018).
- Pita, G.M.; Jiménez, S.; Basabe, B.; García, R.G.; Macías, C.; Selva, L.; Hernández, C.; Cruz, M.; Herrera, R.; O’Farrill, R.; et al. Anemia in children under five years old in Eastern Cuba, 2005–2011. MEDICC Rev. 2014, 16, 16–23. [Google Scholar]
- Reboso Pérez, J.; Cabrera Núñez, E.; Rodríguez, G.P.; Jiménez Acosta, S. Anemia por deficiencia de hierro en niños de 6 a 24 meses y de 6 a 12 años de edad. Revista Cubana de Salud Pública 2005, 31, 306–312. [Google Scholar]
- Quizhpe, E.; San Sebastián, M.; Hurtig, A.K.; Llamas, A. Prevalence of anemia in schoolchildren in the Amazon area of Ecuador. Rev. Panam. Salud Pública 2003, 13, 355–361. [Google Scholar] [CrossRef]
- Assandri, E.; Skapino, E.; da Rosa, D.; Alemán, A.; Acuña, A.M. Anemia, nutritional status and intestinal parasites in children from vulnerable homes of Montevideo. Arch. Pediatr. Urug. 2018, 89, 86–98. [Google Scholar]
- Ministry of Education [Jamaica]; Ministry of Health [Jamaica]; PAHO. Micronutrient Study Report: An Assessment of the Vitamin A, E, Betacarotene, and Iron Status in Jamaica; PAHO: Kingston, Jamaica, 1998. [Google Scholar]
- Iannotti, L.L.; Delnatus, J.R.; Odom, A.R.; Eaton, J.C.; Griggs, J.J.; Brown, S.; Wolff, P.B. Determinants of anemia and hemoglobin concentration in haitian school-aged children. Am. J. Trop. Med. Hyg. 2015, 93, 1092–1098. [Google Scholar] [CrossRef]
- Rivera, J.A.; Sotres-alvarez, D.; Habicht, J.P.; Shamah, T.; Villalpando, S. Impact of the Mexican program for education, health, and nutrition (Progresa) on rates of growth and anemia in infants and young children a randomized effectiveness study. JAMA 2004, 291, 2563–2570. [Google Scholar] [CrossRef] [PubMed]
- Monárrez-Espino, J.; Martínez, H.; Martínez, V.; Greiner, T. Nutritional status of indigenous children at boarding schools in northern Mexico. Eur. J. Clin. Nutr. 2004, 58, 532–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabada, M.M.; Goodrich, M.R.; Graham, B.; Villanueva-Meyer, P.G.; Deichsel, E.L.; Lopez, M.; Arque, E.; Clinton White, A., Jr. Prevalence of intestinal helminths, anemia, and malnutrition in Paucartambo, Peru. Rev. Panam. Salud Publica 2015, 37, 69–75. [Google Scholar] [PubMed]
- Aparco, J.P.; Bautista-Olórtegui, W.; Astete-Robilliard, L.; Pillaca, J. Assessment of the nutritional status, physical activity, and eating habits of schoolchildren in Cercado de Lima. Rev. Peru. Med. Exp. Salud Publica 2016, 33, 633–639. [Google Scholar] [CrossRef]
- Huamán-Espino, L.; Aparco, J.P.; Nuñez-Robles, E.; Gonzáles, E.; Pillaca, J.; Mayta-Tristán, P. Consumo de suplementos con multimicronutrientes Chispitas* y anemia en niños de 6 a 35 meses: Estudio transversal en el contexto de una intervención poblacional en Apurímac, Perú. Rev. Peru. Med. Exp. Salud Publica 2012, 29, 314–323. [Google Scholar] [CrossRef] [PubMed]
- RODRÍGUEZ-ZÚÑIGA, M.J. Obesidad, sobrepeso y anemia en niños de una zona rural de lima, Perú. MEDICINA (Buenos Aires) 2015, 75, 379–383. [Google Scholar]
- Lutter, C.K.; Rodriguez, A.; Fuenmayor, G.; Avila, L.; Sempertegui, F.; Escobar, J. Growth and micronutrient status in children receiving a fortified complementary food. J. Nutr. 2008, 138, 379–388. [Google Scholar] [CrossRef]
- UNICEF. ADIÓS ANEMIA: A Local Strategy for the Reduction of Childhood Anemia in Peri-Urban Areas; UNICEF: Lima, Peru, 2012. [Google Scholar]
- PMA; PRONAA. Educational Intervention in Prevention of Anemia and Malnutrition in Pachacutec—Peru; PMA; PRONAA: Lima, Peru, 2008. [Google Scholar]
- Miranda, M.; Olivares, M.; Brito, A.; Pizarro, F. Reducing iron deficiency anemia in Bolivian school children: Calcium and iron combined versus iron supplementation alone. Nutrition 2014, 30, 771–775. [Google Scholar] [CrossRef]
- Menon, P.; Ruel, M.T.; Loechl, C.U.; Arimond, M.; Habicht, J.P.; Pelto, G.; Michaud, L. Micronutrient Sprinkles Reduce Anemia among 9-to 24-Mo-Old Children When Delivered through an Integrated Health and Nutrition Program in Rural Haiti. J. Nutr. 2007, 137, 1023–1030. [Google Scholar] [CrossRef]
- Landim, L.A.; Pessoa, M.L.; Brandão, A.C.; Morgano, M.A.; Mota Araújo, M.A.; Rocha, M.M.; Arêas, J.A.; Moreira-Araújo, R.S. Impact of the two different iron fortified cookies on treatment of anemia in preschool children in Brazil. Nutr. Hosp. 2016, 33, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Villalpando, S.; Shamah, T.; Rivera, J.A.; Lara, Y.; Monterrubio, E. Fortifying milk with ferrous gluconate and zinc oxide in a public nutrition program reduced the prevalence of anemia in toddlers. J. Nutr. 2006, 136, 2633–2637. [Google Scholar] [CrossRef]
- Kliegman, R.M.; Stanton, B.F.; Geme, J.W.; Schor, N.F. Nelson. Textbook of Pediatrics, 20th ed.; Elsevier: Barcelona, Spain, 2016; pp. 68–88. [Google Scholar]
- Meinzen-Derr, J.K.; Guerrero, M.L.; Altaye, M.; Ortega-Gallegos, H.; Ruiz-Palacios, G.M.; Morrow, A.L. Risk of infant anemia is associated with exclusive breast-feeding and maternal anemia in a mexican cohort. J. Nutr. 2006, 136, 452–458. [Google Scholar] [CrossRef]
- Wang, F.; Liu, H.; Wan, Y.; Li, J.; Chen, Y.; Zheng, J.; Huang, T.; Li, D. Prolonged exclusive breastfeeding duration is positively associated with risk of anemia in infants aged 12 months. J. Nutr. 2016, 146, 1707–1713. [Google Scholar] [CrossRef] [PubMed]
- Nriagu, J.O. Encyclopedia of Environmental Health; Elsevier: Michigan, MI, USA, 2011; pp. 601–610. [Google Scholar]
- Joo, E.Y.; Kim, K.Y.; Kim, D.H.; Lee, J.E.; Kim, S.K. Iron deficiency anemia in infants and toddlers. Blood Res. 2016, 51, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Kaciroti, N.; Walter, T. Iron deficiency in infancy: Applying a physiologic framework for prediction. Am. J. Clin. Nutr. 2006, 84, 1412–1421. [Google Scholar] [CrossRef]
- Diouf, S.; Folquet, M.; Mbofung, K.; Ndiaye, O.; Brou, K.; Dupont, C.; N’dri, D.; Vuillerod, M.; Azaïs-Braesco, V.; Tetanye, E. Prevalence and determinants of anemia in young children in French-speaking Africa. Role of iron deficiency. Arch. Pédiatr. 2015, 22, 1188–1197. [Google Scholar] [CrossRef] [PubMed]
- Wieringa, F.T.; Berger, J.; Dijkhuizen, M.A.; Hidayat, A.; Ninh, N.X.; Utomo, B.; Wasantwisut, E.; Winichagoon, P. Sex differences in prevalence of anaemia and iron deficiency in infancy in a large multi-country trial in South-East Asia. Br. J. Nutr. 2018, 98, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Ncogo, P.; Romay-Barja, M.; Benito, A.; Aparicio, P.; Nseng, G.; Berzosa, P.; Santana-Morales, M.A.; Riloha, M.; Valladares, B.; Herrador, Z. Prevalence of anemia and associated factors in children living in urban and rural settings from Bata District, Equatorial Guinea, 2013. PLoS ONE 2017, 12, e0176613. [Google Scholar] [CrossRef]
- Barría, P.; Amigo, H. Nutritional transition: A review of the Latin American profile. Arch. Latinoam. Nutr. 2006, 56, 3–11. [Google Scholar]
- Albala, C.; Vio, F.; Kain, J.; Uauy, R. Nutrition transition in Latin America: The case of Chile. Nutr. Rev. 2009, 59, 170–176. [Google Scholar] [CrossRef]
- Bermudez, O.I.; Tucker, K.L. Trends in dietary patterns of Latin American populations. Cad. Saude Publica 2003, 19, S87–S99. [Google Scholar] [CrossRef] [PubMed]
- Mujica-Coopman, M.F.; Brito, A.; López de Romaña, D.; Ríos-Castillo, I.; Coris, H.; Olivares, M. Prevalence of anemia in Latin America and the Caribbean. Food Nutr. Bull. 2015, 36, S119–S128. [Google Scholar] [CrossRef] [PubMed]
- Cembranel, F.; Corso, A.C.T.; González-Chica, D.A. Inadequacies in the treatment of iron deficiency anemia among children registered in the national program of iron supplementation in Florianopolis, Santa Catarina, Brazil. Texto Contexto Enferm. 2017, 26, e06310015. [Google Scholar] [CrossRef]
- Cembranel, F.; Corso, A.C.T.; González-Chica, D.A. Coverage and adequacy of ferrous sulfate supplementation in the prevention of anemia among children treated at health centers of Florianopolis, Santa Catarina. Rev. Paul. Pediatr. 2013, 31, 315–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health [Panama]; National Commission of Micronutrients. National Plan “Prevention and Control of Micronutrient Deficiencies” 2008–2015; Ministry of Health: Panama, Republic of Panama, 2008.
- WHO: Geneva, Switzerland. World Health Statistics 2010. Available online: http://www.who.int/iris/handle/10665/44292 (accessed on 2 December 2018).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | SES | Study Design | Sample Size (n) | Anemic Children (n) | Anemia | Quality of Studies | |
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | ||||||||
| CFNI/PAHO_Jamaica [59] | 1998 | Jamaica | Low | Cross–sectional | 272 | 131 | 48.20 | 42.26–54.14 | Fair |
| Neuman NA, et al. [43] | 2000 | Brazil | Middle | Cross–sectional | 468 | 284 | 60.60 | 56.17–65.03 | Good |
| Osório MM, et al. [44] | 2001 | Brazil | Very low | Cross–sectional | 777 | 318 | 40.90 | 37.44–44.36 | Good |
| Rivera JA, et al. [61] | 2004 | Mexico | Low | Cross–sectional | 595 | 154 | 25.80 | 22.28–29.32 | Good |
| Assis AM, et al. [45] | 2004 | Brazil | Middle | Cross–sectional | 603 | 279 | 46.30 | 42.32–50.28 | Good |
| Morais MB, et al. [46] | 2005 | Brazil | Very low | Cross–sectional | 108 | 70 | 64.80 | 55.79–73.81 | Fair |
| Ministry of health of Panama [14] | 2006 | Panama | Very low | National Survey | 373 | 156 | 41.80 | 36.79–46.81 | Fair |
| Brooker S, et al. [47] | 2007 | Brazil | Very low | Cross–sectional | 139 | 44 | 31.65 | 23.92–39.38 | Fair |
| EMMUS IV [17] | 2007 | Haiti | Low | National Survey | 4142 | 2599 | 60.60 | 59.11–62.09 | Fair |
| Duque X, et al. [31] | 2007 | Mexico | Middle | Cross–sectional * | 4957 | 986 | 19.90 | 18.79–21.01 | Good |
| Vieira AC, et al. [48] | 2007 | Brazil | Very low | Cross–sectional | 153 | 85 | 55.60 | 47.73–63.47 | Fair |
| SIVIN 2007 [21] | 2008 | Nicaragua | Very low | National Survey | 1466 | 295 | 20.10 | 18.05–22.15 | Good |
| PNDS 2006 [18] | 2009 | Brazil | Middle | National Survey | 3455 | 721 | 20.86 | 19.51–22.21 | Good |
| Durán P, et al. [29] | 2009 | Argentina | Middle | Cross–sectional * | 30,514 | 5035 | 16.50 | 16.08–16.92 | Good |
| GDSH 2009 [20] | 2009 | Guyana | Middle | National Survey | 1349 | 316 | 23.40 | 21.14–25.66 | Good |
| Oliveira CSM, et al. [49] | 2011 | Brazil | Middle | Cross–sectional | 429 | 246 | 57.30 | 52.62–61.98 | Good |
| Castro TG, et al. [50] | 2011 | Brazil | Middle | Cross–sectional | 617 | 180 | 29.20 | 25.61–32.79 | Good |
| Leal LP, et al. [34] | 2011 | Brazil | Middle | Cross–sectional | 1403 | 476 | 33.92 | 31.44–36.40 | Good |
| Cardoso MA, et al. [35] | 2012 | Brazil | Middle | Cross–sectional | 526 | 111 | 21.10 | 17.61–24.59 | Good |
| Rocha DS, et al. [36] | 2012 | Brazil | Middle | Cross–sectional | 312 | 102 | 32.80 | 27.59–38.01 | Good |
| Brito A, et al. [51] | 2012 | Chile | Middle | Cross–sectional | 224 | 12 | 5.40 | 2.44–8.36 | Fair |
| Huamán–Espino L, et al. [65] | 2012 | Peru | Very low | Cross–sectional | 714 | 366 | 51.30 | 47.63–54.97 | Good |
| ENSANUT-ECU 2012 [16] | 2012 | Ecuador | Middle | National Survey | 1913 | 356 | 18.60 | 16.86–20.34 | Fair |
| Oliveira AP, et al. [37] | 2013 | Brazil | Middle | Cross–sectional | 980 | 363 | 37.00 | 33.98–40.02 | Good |
| Silla L, et al. [38] | 2013 | Brazil | Middle | Cross–sectional | 2186 | 992 | 45.40 | 43.31–47.49 | Good |
| ENDESA 2011-2012 [19] | 2013 | Honduras | Very low | National Survey | 10,681 | 3097 | 29.00 | 28.14–29.86 | Good |
| Brito A, et al. [52] | 2013 | Chile | Very low | Cross–sectional | 320 | 44 | 13.75 | 9.98–17.52 | Good |
| Leite MS, et al. [28] | 2013 | Brazil | Very low | Cross–sectional * | 5397 | 2763 | 51.20 | 49.87–52.53 | Good |
| National Micronutrients Survey [24] | 2014 | Dominican Republic | Low | National Survey | 772 | 217 | 28.10 | 24.93–31.27 | Fair |
| ENS 2014 [23] | 2014 | El Salvador | Very low | National Survey | 5862 | 1327 | 22.64 | 21.57–23.71 | Good |
| Oliveira TSC, et al. [39] | 2014 | Brazil | Middle | Cross–sectional | 373 | 143 | 38.30 | 33.37–43.23 | Good |
| Sarmiento OL, et al. [27] | 2014 | Colombia | Middle | Cross–sectional * | 7725 | 2124 | 27.50 | 26.50–28.50 | Good |
| Saraiva BC, et al. [40] | 2014 | Brazil | Middle | Cross–sectional | 692 | 109 | 15.70 | 12.99–18.41 | Good |
| Pita GM, et al. [55] | 2014 | Cuba | Low | Cross–sectional | 2204 | 573 | 26.00 | 24.17–27.83 | Good |
| Vasconcelos PN, et al. [41] | 2014 | Brazil | Middle | Cross–sectional | 646 | 135 | 20.90 | 17.76–24.04 | Fair |
| Iannotti L, et al. [60] | 2015 | Haiti | Low | Cross–sectional | 182 | 128 | 70.30 | 63.66–76.94 | Good |
| Rodríguez–Zúñiga MJ, et al. [66] | 2015 | Peru | Low | Cross–sectional | 473 | 137 | 29.00 | 24.91–33.09 | Good |
| Martorell R, et al. [53] | 2015 | Costa Rica | Very low | Cross–sectional | 403 | 16 | 4.00 | 2.09–5.91 | Fair |
| ENDES 2016 [15] | 2017 | Peru | Low | National Survey | 10,060 | 3350 | 33.30 | 32.38–34.22 | Good |
| EDSA 2016 [26] | 2017 | Boliva | Low | National Survey | 1526 | 819 | 53.70 | 51.20–56.20 | Fair |
| ENSMI 2014-2015 [22] | 2017 | Guatemala | Low | National Survey | 11,164 | 3617 | 32.40 | 31.53–33.27 | Good |
| Robles BN, et al. [13] | 2017 | Dominica | Very low | Retrospective | 635 | 123 | 19.30 | 16.23–22.37 | Good |
| Barquero MS, et al. [54] | 2018 | Costa Rica | Very low | Cross–sectional | 1291 | 111 | 8.60 | 7.07–10.13 | Fair |
| Cruz-Góngora V, et al. [30] | 2018 | Mexico | Middle | Cross–sectional * | 9094 | 2446 | 26.90 | 25.99–27.81 | Good |
| Assandri E, et al. [58] | 2018 | Uruguay | Middle | Cross–sectional | 136 | 45 | 33.00 | 25.10–40.90 | Fair |
| Author | Year | Country | SES | Study Design | Sample Size (n) | Anemic Children (n) | Anemia | Quality of Studies | |
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | ||||||||
| Quizhpe E, et al. [57] | 2003 | Ecuador | Middle | Cross–sectional | 592 | 98 | 16.60 | 13.60–19.60 | Good |
| Monárrez–Espino J, et al. [62] | 2004 | Mexico | Very low | Cross–sectional | 331 | 43 | 13.00 | 9.38–16.62 | Fair |
| Reboso J, et al. [56] | 2005 | Cuba | Low | Cross–sectional | 100 | 22 | 22.00 | 13.88–30.12 | Fair |
| Ministry of health of Panama [14] | 2006 | Panama | Very low | National Survey | 788 | 50 | 6.30 | 4.60–8.00 | Fair |
| Winocur D, et al. [32] | 2007 | Argentina | Middle | Cross–sectional | 323 | 8 | 2.50 | 0.80–4.20 | Good |
| Brooker S, et al. [47] | 2007 | Brazil | Very low | Cross–sectional | 301 | 32 | 10.63 | 7.15–14.11 | Fair |
| ENSANUT-ECU 2012 [16] | 2012 | Ecuador | Middle | National Survey | 4443 | 156 | 3.50 | 2.96–4.04 | Fair |
| Cardoso MA, et al. [35] | 2012 | Brazil | Middle | Cross–sectional | 585 | 40 | 6.80 | 4.76–8.84 | Good |
| ENM 2012 [25] | 2013 | Dominican Republic | Low | National Survey | 654 | 119 | 18.20 | 15.24–21.16 | Fair |
| Sarmiento OL, et al. [27] | 2014 | Colombia | Middle | Cross–sectional * | 7906 | 640 | 8.10 | 7.50–8.70 | Good |
| Rodríguez–Zúñiga MJ, et al. [66] | 2015 | Peru | Low | Cross–sectional | 1.438 | 905 | 62.90 | 60.40–65.40 | Good |
| Cabada MN, et al. [63] | 2015 | Peru | Very low | Cross–sectional | 192 | 70 | 36.50 | 29.69–43.31 | Fair |
| Iannotti L, et al. [60] | 2015 | Haiti | Low | Cross–sectional | 753 | 509 | 67.59 | 64.25–70.93 | Good |
| Aparco JP, et al. [64] | 2016 | Peru | Low | Cross–sectional | 808 | 96 | 11.90 | 9.67–14.13 | Fair |
| Ferreira HS, et al. [42] | 2016 | Brazil | Middle | Cross–sectional | 1547 | 144 | 9.30 | 7.85–10.75 | Good |
| Barquero MS, et al. [54] | 2018 | Costa Rica | Very low | Cross–sectional | 912 | 55 | 6.00 | 4.46–7.54 | Fair |
| Cruz-Góngora V, et al. [30] | 2018 | Mexico | Middle | Cross–sectional * | 15,993 | 1999 | 12.50 | 11.99–13.01 | Good |
| Lázaro L, et al. [33] | 2018 | Argentina | Middle | Cross–sectional | 362 | 16 | 4.40 | 2.29–6.51 | Fair |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iglesias Vázquez, L.; Valera, E.; Villalobos, M.; Tous, M.; Arija, V. Prevalence of Anemia in Children from Latin America and the Caribbean and Effectiveness of Nutritional Interventions: Systematic Review and Meta–Analysis. Nutrients 2019, 11, 183. https://doi.org/10.3390/nu11010183
Iglesias Vázquez L, Valera E, Villalobos M, Tous M, Arija V. Prevalence of Anemia in Children from Latin America and the Caribbean and Effectiveness of Nutritional Interventions: Systematic Review and Meta–Analysis. Nutrients. 2019; 11(1):183. https://doi.org/10.3390/nu11010183
Chicago/Turabian StyleIglesias Vázquez, Lucía, Edith Valera, Marcela Villalobos, Mónica Tous, and Victoria Arija. 2019. "Prevalence of Anemia in Children from Latin America and the Caribbean and Effectiveness of Nutritional Interventions: Systematic Review and Meta–Analysis" Nutrients 11, no. 1: 183. https://doi.org/10.3390/nu11010183